Tractography Alterations in the Arcuate and Uncinate Fasciculi in Post-Stroke Aphasia

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Case
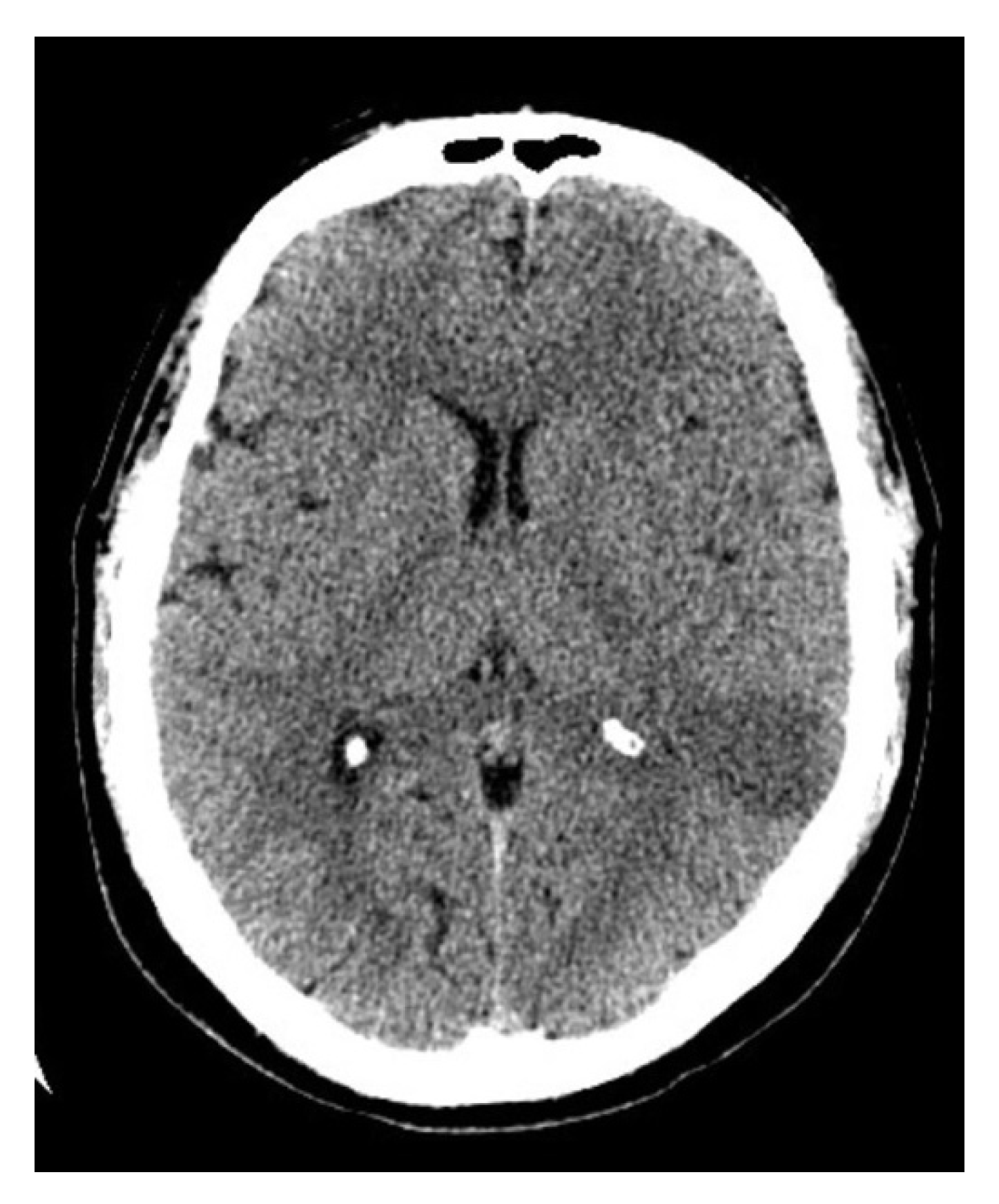
2.1. Case History
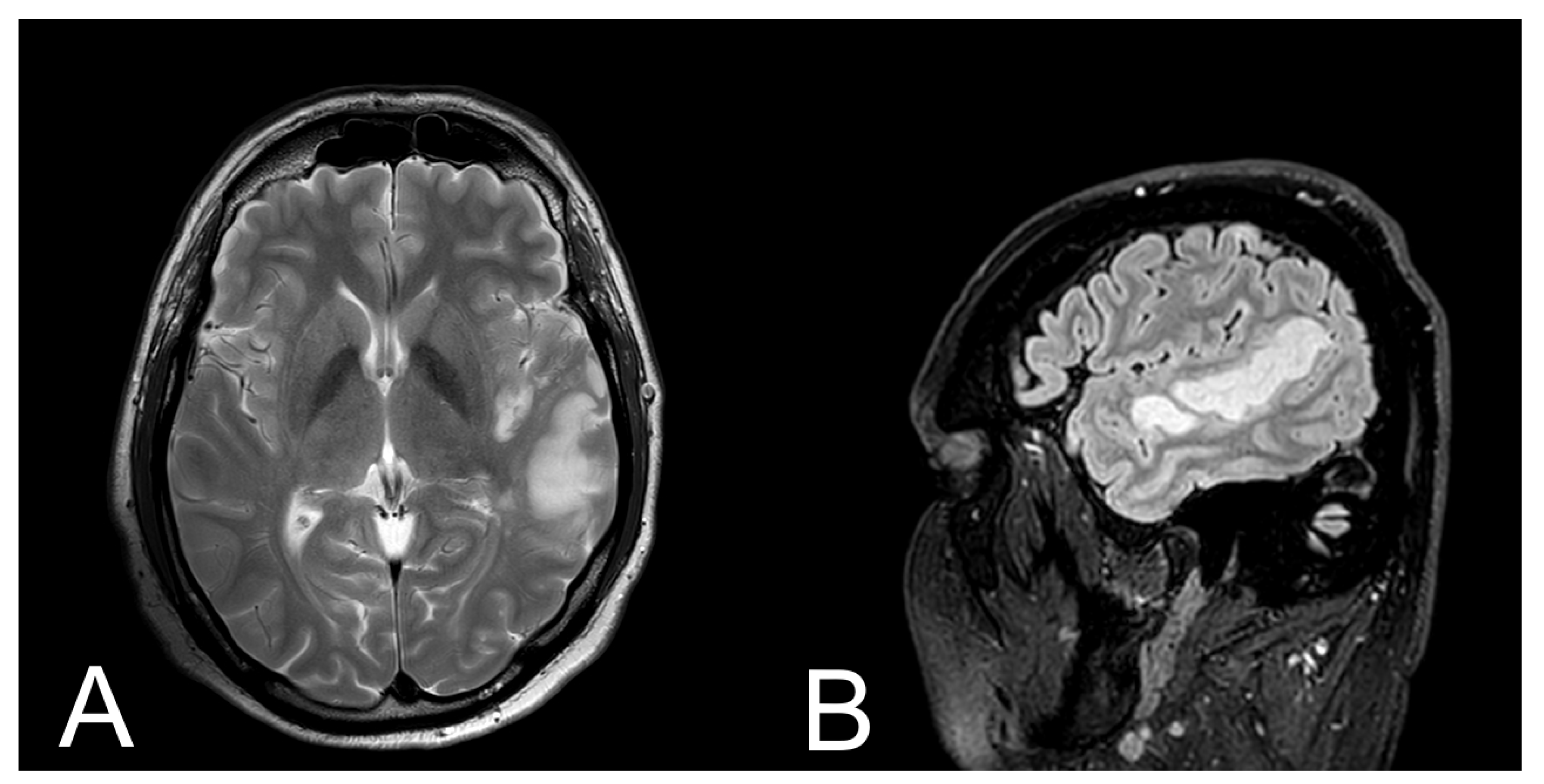
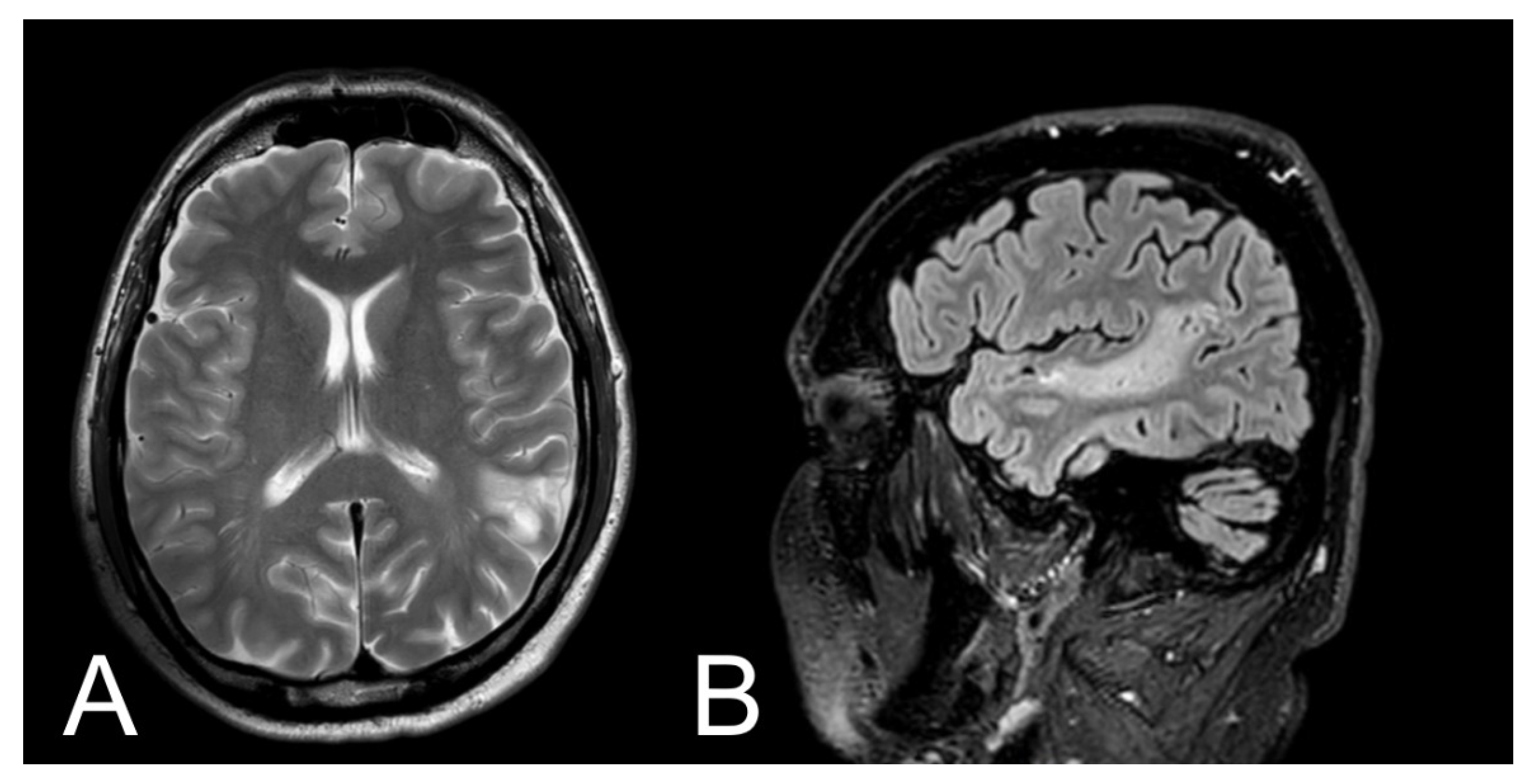
2.2. Results of Tests
2.3. Treatment
2.4. Outcome after Treatment
2.5. MRI Protocol
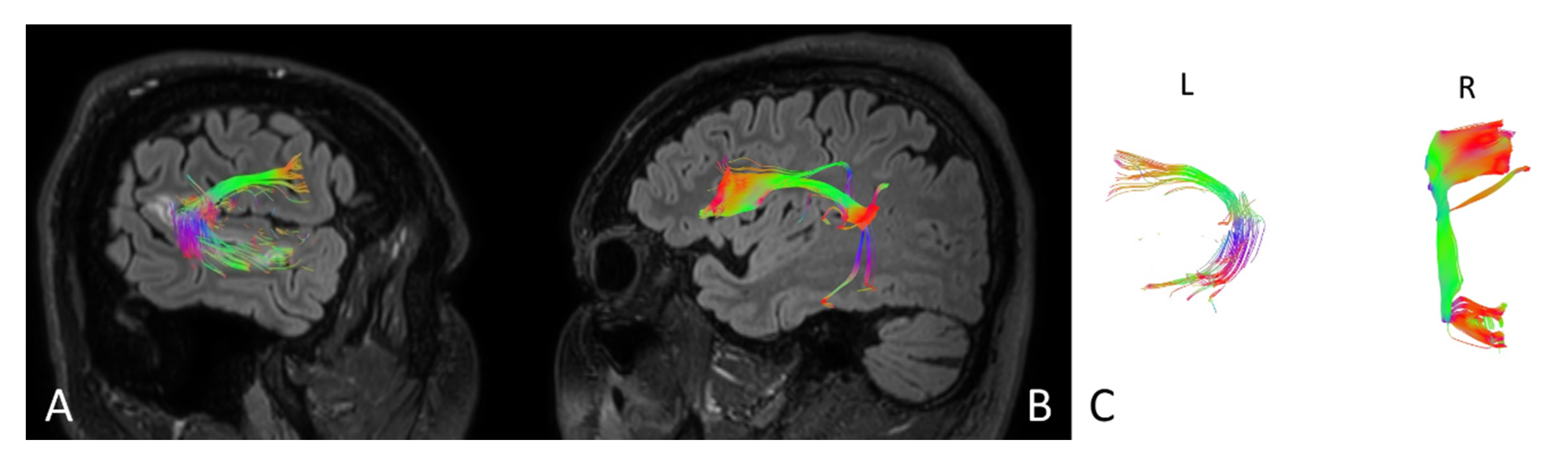
2.6. Fiber Tracking Protocol
2.7. tDCS Protocol
2.8. Outcome at Discharge
2.9. Outcome at Follow Up
3. Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Bolognini, N.; Russo, C.; Edwards, D.J. The sensory side of post-stroke motor rehabilitation. Restor. Neurol. Neurosci. 2016, 34, 571–586. [Google Scholar] [CrossRef] [PubMed]
- Berthier, M.L. Poststroke aphasia: Epidemiology, pathophysiology and treatment. Drugs Aging 2005, 22, 163–182. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Lyden, P.; Brady, M. Aphasia and dysarthria in acute stroke: Recovery and functional outcome. Int. J. Stroke 2015, 10, 400–406. [Google Scholar] [CrossRef]
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018. [Google Scholar] [CrossRef]
- Menon, B.K. Neuroimaging in Acute Stroke. Contin. (Minneap. Minn.) 2020, 26, 287–309. [Google Scholar] [CrossRef]
- Taea, W.-S.; Hama, B.-J.; Pyuna, S.-B.; Kang, S.H.; Kim, B.J. Current clinical applications of diffusion-tensor imaging in neurological disorders. J. Clin. Neurol. 2008, 14, 129–140. [Google Scholar] [CrossRef]
- Denier, C.; Chassin, O.; Vandendries, C.; Bayon De La Tour, L.; Cauquil, C.; Sarov, M.; Adams, D.; Flamand-Roze, C. Thrombolysis in stroke patients with isolated aphasia. Cerebrovasc. Dis. 2016, 41, 163–169. [Google Scholar] [CrossRef]
- Moura, L.M.; Luccas, R.; De Paiva, J.P.Q.; Amaro, E.; Leemans, A.; Leite, C.D.C.; Otaduy, M.C.G.; Conforto, A.B. Diffusion tensor imaging biomarkers to predict motor outcomes in stroke: A narrative review. Front. Neurol. 2019, 10, 445. [Google Scholar] [CrossRef]
- Puig, J.; Blasco, G.; Daunis-I-Estadella, J.; Thomalla, G.; Castellanos, M.; Figueras, J.; Remollo, S.; Van Eendenburg, C.; Sánchez-González, J.; Serena, J.; et al. Decreased corticospinal tract fractional anisotropy predicts long-term motor outcome after stroke. Stroke 2013, 44, 2016–2018. [Google Scholar] [CrossRef]
- Maeshima, S.; Osawa, A.; Nishio, D.; Hirano, Y.; Kigawa, H.; Takeda, H. Diffusion tensor MR imaging of the pyramidal tract can predict the need for orthosis in hemiplegic patients with hemorrhagic stroke. Neurol. Sci. 2013, 34, 1765–1770. [Google Scholar] [CrossRef] [PubMed]
- Kieronska, S.; Słoniewski, P. The usefulness and limitations of diffusion tensor imaging—A review study. Eur. J. Transl. Clin. Med. 2020, 2, 43–51. [Google Scholar] [CrossRef]
- Elsner, B.; Kugler, J.; Pohl, M.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving aphasia in adults with aphasia after stroke. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Polanowska, K.; Seniów, J. Influence of transcranial direct current stimulation on cognitive functioning of patients with brain injury. Neurol. I Neurochir. Pol. 2010, 44, 580–590. [Google Scholar] [CrossRef]
- Fridriksson, J.; Rorden, C.; Elm, J.; Sen, S.; George, M.S.; Bonilha, L. transcranial direct current stimulation vs sham stimulation to treat aphasia after stroke: A randomized clinical trial. JAMA Neurol. 2018, 75, 1470–1476. [Google Scholar] [CrossRef]
- Monti, A.; Ferrucci, R.; Fumagalli, M.; Mameli, F.; Cogiamanian, F.; Ardolino, G.; Priori, A. Transcranial direct current stimulation (tDCS) and language. J. Neurol. Neurosurg. Psychiatry 2013, 84, 832–842. [Google Scholar] [CrossRef]
- Enderby, P.M.; Wood, V.A.; Wade, D.T.; Hewer, R.L. The frenchay aphasia screening test: A short, simple test for aphasia appropriate for non-specialists. Disabil. Rehabil. 1986, 8, 166–170. [Google Scholar] [CrossRef]
- del Toro, C.M.; Bislick, L.P.; Comer, M.; Velozo, C.; Romero, S.; Rothi, L.J.G.; Kendall, D.L. Development of a short form of the boston naming test for individuals with aphasia. J. SpeechLang. Hear. Res. 2011, 54, 1089–1100. [Google Scholar] [CrossRef]
- Vollmar, C.; Muircheartaigh, J.O.; Barker, G.J.; Symms, M.R.; Thompson, P.; Kumari, V.; Duncan, J.S.; Richardson, M.P.; Koepp, M.J. NeuroImage identical, but not the same: Intra-site and inter-site reproducibility of fractional anisotropy measures on two 3. 0 T scanners. NeuroImage 2010, 51, 1384–1394. [Google Scholar] [CrossRef]
- Andica, C.; Kamagata, K.; Hayashi, T.; Hagiwara, A.; Uchida, W.; Saito, Y. Scan—rescan and inter-vendor reproducibility of neurite orientation dispersion and density imaging metrics. Neuroradiology 2019, 62, 483–494. [Google Scholar] [CrossRef]
- Sebastian, R.; Tsapkini, K.; Tippett, D.C. Transcranial direct current stimulation in post stroke aphasia and primary progressive Aphasia: Current knowledge and future clinical applications. NeuroRehabilitation 2017, 39, 141–152. [Google Scholar] [CrossRef]
- Seghier, M.L.; Lazeyras, F.; Zimine, S.; Saudan-Frei, S.; Safran, A.B.; Hüppi, P.S. Visual recovery after perinatal stroke evidenced by functional and diffusion MRI: Case report. BMC Neurol. 2005, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Furlanis, G.; Ridolfi, M.; Polverino, P.; Menichelli, A.; Caruso, P.; Naccarato, M.; Sartori, A.; Torelli, L.; Pesavento, V.; Manganotti, P. Early recovery of aphasia through thrombolysis: The significance of spontaneous speech. J. Stroke Cerebrovasc. Dis. 2018, 27, 1937–1948. [Google Scholar] [CrossRef]
- Kierońska, S.; Sokal, P.; Dura, M.; Jabłońska, M.; Rudaś, M.; Jabłońska, R. Tractography-based analysis of morphological and anatomical characteristics of the uncinate fasciculus in human brains. Brain Sci. 2020, 10, 709. [Google Scholar] [CrossRef] [PubMed]
- Armitage, P.A.; Bastin, M.E.; Marshal, I.; Wardlaw, J.M.; Cannon, J. Diffusion anisotropy measurements in ischaemic stroke of the human brain. Magn. Reson. Mater. Phys. Biol. Med. 1998, 6, 28–36. [Google Scholar] [CrossRef]
- Maniega, S.M.; Bastin, M.E.; Armitage, P.A.; Farrall, A.J.; Carpenter, T.K.; Hand, P.J.; Cvoro, V.; Rivers, C.S.; Wardlaw, J.M. Temporal evolution of water diffusion parameters is different in grey and white matter in human ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1714–1718. [Google Scholar] [CrossRef] [PubMed]
- Ozsunar, Y.; Grant, P.E.; Huisman, T.A.G.M.; Schaefer, P.W.; Wu, O.; Sorensen, A.G.; Koroshetz, W.J.; Gonzalez, R.G. Evolution of water diffusion and anisotropy in hyperacute stroke: Significant correlation between fractional anisotropy and T2. Am. J. Neuroradiol. 2004, 25, 699–705. [Google Scholar]
- García, A.O.; Brambati, S.M.; Brisebois, A.; Désilets-Barnabé, M.; Houzé, B.; Bedetti, C.; Rochon, E.; Leonard, C.; Desautels, A.; Marcotte, K. predicting early post-stroke aphasia outcome from initial aphasia severity. Front. Neurol. 2020, 11, 120. [Google Scholar] [CrossRef] [PubMed]
- Provenzale, J.M.; Mukundan, S.; Barboriak, D.P. Diffusion-weighted and perfusion mr imaging for brain tumor characterization and assessment of treatment response. Radiology 2006, 239, 632–649. [Google Scholar] [CrossRef]
- Puig, J.; Blasco, G.; Schlaug, G.; Stinear, C.M.; Daunis-i-Estadella, P.; Biarnes, C.; Figueras, J.; Serena, J.; Hernández-Pérez, M.; Alberich-Bayarri, A.; et al. Diffusion tensor imaging as a prognostic biomarker for motor recovery and rehabilitation after stroke. Neuroradiology 2017, 59, 343–351. [Google Scholar] [CrossRef]
- Gonzalez-Aquines, A.; Moreno-Andrade, T.; Gongora-Rivera, F.; Cordero-Perez, A.C.; Ortiz-Jiménez, X.; Cavazos-Luna, O.; Garza-Villareal, E.; Campos-Coy, M.; Elizondo-Riojas, G. The role of tractography in ischemic stroke: A review of the literature. Med. Univ. 2019, 20, 161–165. [Google Scholar] [CrossRef]
- Szmuda, T.; Kierońska, S.; Ali, S.; Słoniewski, P.; Pacholski, M.; Dzierżanowski, J.; Sabisz, A.; Szurowska, E. Tractography-guided surgery of brain tumors: What is the best method to outline the corticospinal tract? Folia Morphol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Szmuda, T.; Rogowska, M.; Słoniewski, P.; Abuhaimed, A.; Szmuda, M.; Springer, J. Frontal aslant tract projections to the inferior frontal gyrus. Folia Morphol. 2017, 76, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Catani, M. The arcuate fasciculus and the disconnection theme in language and aphasia: History and current state. Cortex 2008, 44, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Breier, J.I.; Hasan, K.M.; Zhang, W.; Men, D.; Papanicolaou, A.C. Language dysfunction after stroke and damage to white matter tracts evaluated using diffusion tensor imaging. Am. J. Neuroradiol. 2008, 29, 483–487. [Google Scholar] [CrossRef]
- Kim, S.H.; Jang, S.H. Prediction of aphasia outcome using diffusion tensor tractography for arcuate fasciculus in stroke. Am. J. Neuroradiol. 2013, 34, 785–790. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, D.G.; You, H.; Son, S.M.; Cho, Y.W.; Chang, M.C.; Lee, J.; Jang, S.H. The clinical application of the arcuate fasciculus for stroke patients with aphasia: A diffusion tensor tractography study. NeuroRehabilitation 2011, 29, 305–310. [Google Scholar] [CrossRef]
- Oishi, K.; Faria, A.; Hsu, J.; Tippett, D. The critical role of the right uncinate fasciculus in emotional empathy. Ann. Neurol. 2015, 77, 68–74. [Google Scholar] [CrossRef]
- Matsuo, K.; Mizuno, T.; Yamada, K. Cerebral white matter damage in frontotemporal dementia assessed by diffusion tensor tractography. Neuroradiology 2008. [Google Scholar] [CrossRef]
- Heiss, W.D.; Kidwell, C.S. Imaging for prediction of functional outcome and assessment of recovery in ischemic stroke. Stroke 2014, 45, 1195–1201. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef]
- Ogretmen, B. tDCS in post-stroke aphasia recovery. Physiol. Behav. 2019, 176, 139–148. [Google Scholar] [CrossRef]
- Shah-Basak, P.P.; Norise, C.; Garcia, G.; Torres, J.; Faseyitan, O.; Hamilton, R.H. Individualized treatment with transcranial direct current stimulation in patients with chronic non-fluent aphasia due to stroke. Front. Hum. Neurosci. 2015, 9, 201. [Google Scholar] [CrossRef] [PubMed]
- You, D.S.; Kim, D.Y.; Chun, M.H.; Jung, S.E.; Park, S.J. Cathodal transcranial direct current stimulation of the right Wernicke’s area improves comprehension in subacute stroke patients. Brain Lang. 2011, 119, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Alber, R.; Moser, H.; Gall, C.; Sabel, B.A. Combined transcranial direct current stimulation and vision restoration training in subacute stroke rehabilitation: A pilot study. PM&R 2017, 9, 787–794. [Google Scholar] [CrossRef]
- Fridriksson, J.; Guo, D.; Fillmore, P.; Holland, A.; Rorden, C. Damage to the anterior arcuate fasciculus predicts non-fluent speech production in aphasia. Brain 2013, 136, 3451–3460. [Google Scholar] [CrossRef] [PubMed]
- Krajewska, M. Plastyczność ośrodkowego układu nerwowego a modele i mechanizmy poprawy sprawności językowych po udarze niedokrwiennym mózgu. Logop. Lodz. 2018, 2, 77–92. [Google Scholar] [CrossRef][Green Version]
- Keci, A.; Tani, K.; Xhema, J. Role of rehabilitation in neural plasticity. Open Access Maced. J. Med Sci. 2019, 7, 1540–1547. [Google Scholar] [CrossRef]
- Pellegrino, G.; Arcara, G.; Di, G.; Cristina, P.; Maran, M.; Weis, L.; Piccione, F.; Roman, H. Transcranial direct current stimulation over the sensory-motor regions inhibits gamma synchrony. Hum. Brain Mapp. 2019, 40, 2736–2746. [Google Scholar] [CrossRef]
- Turolla, A.; Venneri, A.; Farina, D.; Cagnin, A.; Cheung, V.C.K. Rehabilitation induced neural plasticity after acquired brain injury. Hindawi Neural Plast. 2018, 2018. [Google Scholar] [CrossRef]
- Mukherjee, P. Diffusion tensor imaging and fiber tractography in acute stroke. Neuroimaging Clin. North Am. 2005, 15, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.M.; Eriksson, D.K.; Brandt, T.H.; Schneck, S.M.; Lucanie, J.M.; Burchfield, A.S.; Charney, S.; Quillen, I.A.; de Riesthal, M.; Kirshner, H.S.; et al. Patterns of recovery from aphasia in the first 2 weeks after stroke. J. SpeechLang. Hear. Res. 2019, 62, 723–732. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Admission | 3 Month Follow-Up | |||
|---|---|---|---|---|
| Parameters | Left side | Right side | Left side | Right side |
| Number of fibers | 148 | 183 | 155 | 152 |
| Volume of tract [mm2] | 13305 | 16440 | 14400 | 16338 |
| Length of tract [mm] | 88.5 | 98.3 | 87.5 | 97.1 |
| FA | 0.675 | 0.895 | 0.705 | 0.880 |
| Admission | 3 Month Follow-Up | |||
|---|---|---|---|---|
| Parameters | Left side | Right side | Left side | Right side |
| Number of fibres | 160 | 205 | 185 | 208 |
| Volume of tract [mm2] | 1125 | 18440 | 1280 | 18559 |
| Length of tract [mm] | 75.5 | 88.0 | 86.4 | 89.0 |
| FA | 0.715 | 0.885 | 0.785 | 0.880 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kierońska, S.; Świtońska, M.; Meder, G.; Piotrowska, M.; Sokal, P. Tractography Alterations in the Arcuate and Uncinate Fasciculi in Post-Stroke Aphasia. Brain Sci. 2021, 11, 53. https://doi.org/10.3390/brainsci11010053
Kierońska S, Świtońska M, Meder G, Piotrowska M, Sokal P. Tractography Alterations in the Arcuate and Uncinate Fasciculi in Post-Stroke Aphasia. Brain Sciences. 2021; 11(1):53. https://doi.org/10.3390/brainsci11010053
Chicago/Turabian StyleKierońska, Sara, Milena Świtońska, Grzegorz Meder, Magdalena Piotrowska, and Paweł Sokal. 2021. "Tractography Alterations in the Arcuate and Uncinate Fasciculi in Post-Stroke Aphasia" Brain Sciences 11, no. 1: 53. https://doi.org/10.3390/brainsci11010053
APA StyleKierońska, S., Świtońska, M., Meder, G., Piotrowska, M., & Sokal, P. (2021). Tractography Alterations in the Arcuate and Uncinate Fasciculi in Post-Stroke Aphasia. Brain Sciences, 11(1), 53. https://doi.org/10.3390/brainsci11010053