Familial Hemiplegic Migraine with an ATP1A4 Mutation: Clinical Spectrum and Carbamazepine Efficacy

 ,
,  ,
,  ,
,  and
and 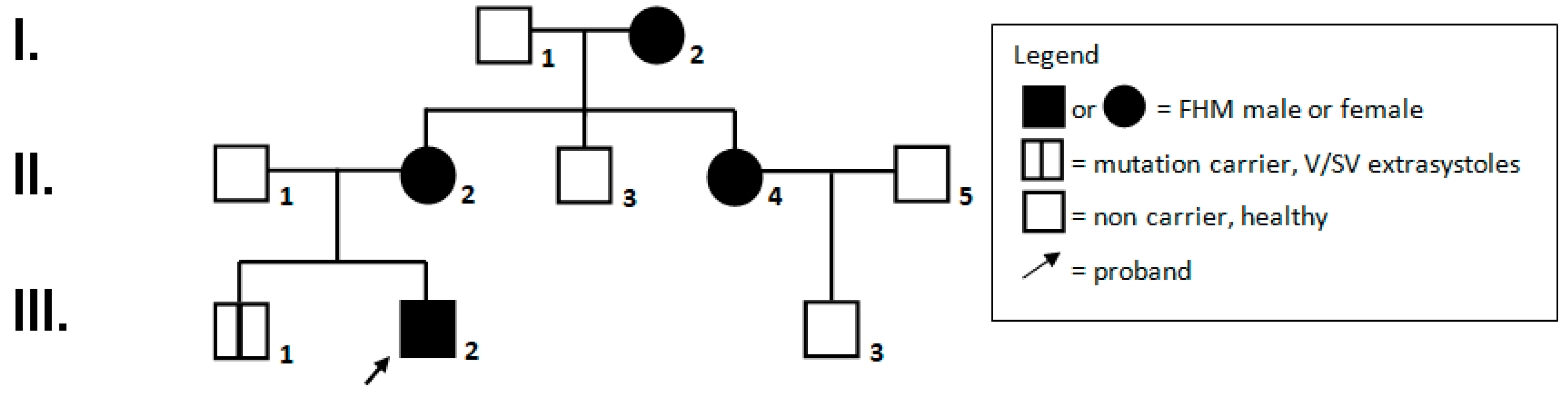{kind=link}
Abstract
1. Introduction
2. Family Report (See Figure 1, Family Pedigree)
2.1. I,2: Female, Aged 78 Years
2.2. II,2: Female, 52 Years of Age
2.3. II,4: Female, 48 Years of Age
2.4. III,1: Male, 19 Years of Age
2.5. III,2: Male Proband, 16 Years of Age
2.6. III,3: Male, Age of 12 Years
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Russell, M.B.; Ducros, A. Sporadic and familial hemiplegic migraine: Pathophysiological mechanisms, clinical characteristics, diagnosis, and management. Lancet Neurol. 2011, 10, 457–470. [Google Scholar] [CrossRef]
- Palumbo, P.; Palumbo, O.; Operto, F.F.; Castellana, S.; Di Muro, E.; Leone, M.P.; Biagini, T.; Pastorino, G.; Mazza, T.; Carella, M.; et al. Familial hemiplegic migraine: A new gene in an italian family. Arch. Clin. Med. Case Rep. 2019, 3, 534–543. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society. The international classification of headache disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Roth, C.; Freilinger, T.; Kirovski, G.; Dunkel, J.; Shah, Y.; Wilken, B.; Rautenstrauß, B.; Ferbert, A. Clinical spectrum in three families with familial hemiplegic migraine type 2 including a novel mutation in the ATP1A2 gene. Cephalalgia 2014, 34, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Schubert, V.; Auffenberg, E.; Biskup, S.; Jurkat-Rott, K.; Freilinger, T. Two novel families with hemiplegic migraine caused by recurrent SCN1A mutation p.F1499L. Cephalalgia 2018, 38, 1503–1508. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, K.; Depienne, C.; Le Fort, D.; Riant, F.; Chaine, P.; Trouillard, O.; Gaudric, A.; Morris, M.A.; Leguern, E.; Tournier-Lasserve, E.; et al. Elicited repetitive daily blindness: A new phenotype associated with hemiplegic migraine and SCN1A mutations. Neurology 2009, 72, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Weller, C.M.; Leen, W.G.; Neville, B.G.; Duncan, J.S.; de Vries, B.; Geilenkirchen, M.A.; Haan, J.; Kamsteeg, E.J.; Ferrari, M.D.; van den Maagdenberg, A.M.; et al. A novel SLC2A1 mutation linking hemiplegic migraine with alternating hemiplegia of childhood. Cephalalgia 2015, 35, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Van Paesschen, W.; Stalmans, I.; Horita, S.; Yamada, H.; Bergmans, B.A.; Legius, E.; Riant, F.; De Jonghe, P.; Li, Y.; et al. Defective membrane expression of the Na(+)-HCO(3)(-) cotransporter NBCe1 is associated with familial migraine. Proc. Natl. Acad. Sci. USA 2020, 107, 15963–15968. [Google Scholar] [CrossRef] [PubMed]
- Kovermann, P.; Hessel, M.; Kortzak, D.; Jen, J.C.; Koch, J.; Fahlke, C.; Freilinger, T. Impaired K(+) binding to glial glutamate transporter EAAT1 in migraine. Sci. Rep. 2017, 24, 13913. [Google Scholar] [CrossRef] [PubMed]
- Lafrenière, R.G.; Rouleau, G.A. Identification of Novel Genes Involved in Migraine. Headache 2012, 52 (Suppl. 2), 107–110. [Google Scholar] [CrossRef]
- Dale, R.C.; Gardiner, A.; Branson, J.A.; Houlden, H. Benefit of carbamazepine in a patient with hemiplegic migraine associated with PRRT2 mutation. Dev. Med. Child. Neurol. 2014, 56, 910. [Google Scholar] [CrossRef] [PubMed]
- Suzuki-Muromoto, S.; Kosaki, R.; Kosaki, K.; Kubota, M. Familial hemiplegic migraine with a PRRT2 mutation: Phenotypic variations and carbamazepine efficacy. Brain Dev. 2020, 42, 293–297. [Google Scholar] [CrossRef]
- Jimenez, T.; Sánchez, G.; Wertheimer, E.V.; Blanco, G. Activity of the Na,K-ATPase alpha4 Isoform Is important for membrane potential, intracellular Ca2+, and pH to maintain motility in rat spermatozoa. Reproduction 2010, 139, 835–845. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coppola, G.; Pastorino, G.M.G.; Vetri, L.; D’Onofrio, F.; Operto, F.F. Familial Hemiplegic Migraine with an ATP1A4 Mutation: Clinical Spectrum and Carbamazepine Efficacy. Brain Sci. 2020, 10, 372. https://doi.org/10.3390/brainsci10060372
Coppola G, Pastorino GMG, Vetri L, D’Onofrio F, Operto FF. Familial Hemiplegic Migraine with an ATP1A4 Mutation: Clinical Spectrum and Carbamazepine Efficacy. Brain Sciences. 2020; 10(6):372. https://doi.org/10.3390/brainsci10060372
Chicago/Turabian StyleCoppola, Giangennaro, Grazia Maria Giovanna Pastorino, Luigi Vetri, Floriana D’Onofrio, and Francesca Felicia Operto. 2020. "Familial Hemiplegic Migraine with an ATP1A4 Mutation: Clinical Spectrum and Carbamazepine Efficacy" Brain Sciences 10, no. 6: 372. https://doi.org/10.3390/brainsci10060372
APA StyleCoppola, G., Pastorino, G. M. G., Vetri, L., D’Onofrio, F., & Operto, F. F. (2020). Familial Hemiplegic Migraine with an ATP1A4 Mutation: Clinical Spectrum and Carbamazepine Efficacy. Brain Sciences, 10(6), 372. https://doi.org/10.3390/brainsci10060372