Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy





Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
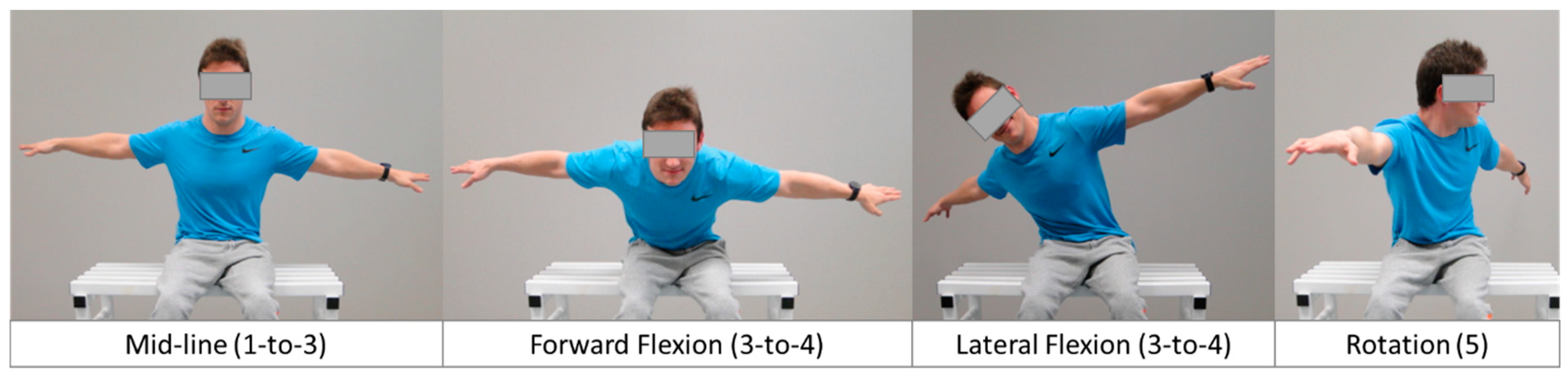
2.3. BISFed TFS
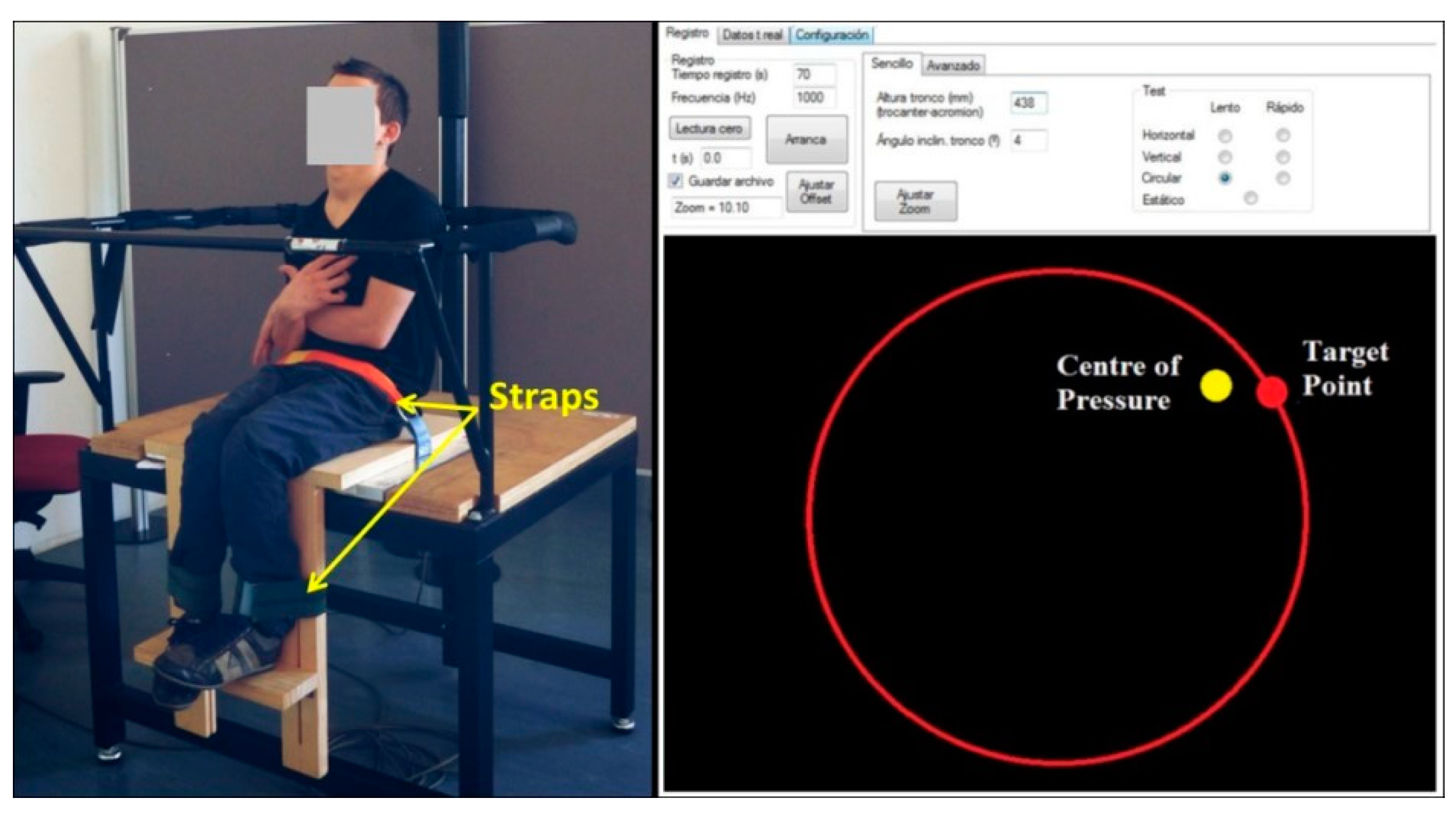
2.4. Posturographic Test Battery
Posturography Data Reduction
2.5. Statistical Analysis
2.5.1. Inter-Rater Reliability
2.5.2. Validity
2.5.3. Sensitivity
3. Results
3.1. Inter-Rater Reliability
3.2. Concurrent Validity between BISFed TFS and Posturography
3.3. Sensitivity of the BISFed TFS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Boccia International Sports Federation (BISFed). Boccia Classification Rules, Fourth Edition. Available online: http://www.bisfed.com/wp-content/uploads/2018/12/Boccia-Classification-Rules-4th-Edition-October-2018.pdf (accessed on 22 February 2020).
- Tweedy, S.M.; Vanlandewijck, Y.C. International Paralympic Committee position stand--background and scientific principles of classification in Paralympic sport. Br. J. Sports Med. 2009, 45, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Szopa, A.; Domagalska-Szopa, M. Postural stability in children with hemiplegia estimated for three postural conditions: Standing, sitting and kneeling. Res. Dev. Disabil. 2015, 39, 67–75. [Google Scholar] [CrossRef]
- Huang, P.-C.; Pan, P.-J.; Ou, Y.-C.; Yu, Y.-C.; Tsai, Y.-S. Motion analysis of throwing Boccia balls in children with cerebral palsy. Res. Dev. Disabil. 2014, 35, 393–399. [Google Scholar] [CrossRef]
- Miyake, Y.; Kobayashi, R.; Kelepecz, D.; Nakajima, M. Core exercises elevate trunk stability to facilitate skilled motor behavior of the upper extremities. J. Bodyw. Mov. Ther. 2013, 17, 259–265. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Barbado, D.; Barbado, L.C.; Elvira, J.; Van Dieën, J.; Vera-Garcia, F.J. Sports-related testing protocols are required to reveal trunk stability adaptations in high-level athletes. Gait Posture 2016, 49, 90–96. [Google Scholar] [CrossRef]
- Barbado, D.; Reina, R.; Roldán, A.; McCulloch, K.; Campayo-Piernas, M.; Vera-Garcia, F.J. How much trunk control is affected in adults with moderate-to-severe cerebral palsy? J. Biomech. 2019, 82, 368–374. [Google Scholar] [CrossRef]
- Lin, D.; Seol, H.; Nussbaum, M.A.; Madigan, M.L. Reliability of COP-based postural sway measures and age-related differences. Gait Posture 2008, 28, 337–342. [Google Scholar] [CrossRef]
- Borg, F.G.; Laxåback, G. Entropy of balance - some recent results. J. Neuroeng. Rehabilitation 2010, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Van Dieën, J.; Koppes, L.L.J.; Twisk, J. Postural sway parameters in seated balancing; their reliability and relationship with balancing performance. Gait Posture 2010, 31, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Hancock, G.R.; Butler, M.S.; Fischman, M.G. On the Problem of Two-Dimensional Error Scores: Measures and Analyses of Accuracy, Bias, and Consistency. J. Mot. Behav. 1995, 27, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Witz, K.; Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences. J. Educ. Stat. 1990, 15, 84. [Google Scholar] [CrossRef]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: San Diego, CA, USA, 1985. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Hillsdale, IL, USA, 1988. [Google Scholar]
- Hopkins, W.G.; Marshall, S.; Batterham, A.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Zeng, N.; Wang, N. Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS implementations. In NESUG Proceedings: Health Care and Life Sciences; SAS Institute Inc.: Baltimore, MA, USA, 2010; Volume 19, pp. 67–76. [Google Scholar]
- International Paralympic Committee. IPC´s Athletes Classification Code. Available online: https://www.paralympic.org/sites/default/files/document/170704160235698_2015_12_17%2BClassification%2BCode_FINAL2_0.pdf (accessed on 17 November 2019).
- Pham, H.P.; Eidem, A.; Hansen, G.; Nyquist, A.; Vik, T.; Sæther, R. Validity and Responsiveness of the Trunk Impairment Scale and Trunk Control Measurement Scale in Young Individuals with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2016, 36, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Santos, P.B.R.; Vigario, P.; Mainenti, M.R.M.; Ferreira, A.S.; Lemos, T. Seated limits-of-stability of athletes with disabilities with regard to competitive levels and sport classification. Scand. J. Med. Sci. Sports 2017, 27, 2019–2026. [Google Scholar] [CrossRef]
- Roldan, A.; Sabido, R.; Barbado, D.; Caballero, C.; Reina, R. Manual Dexterity and Intralimb Coordination Assessment to Distinguish Different Levels of Impairment in Boccia Players with Cerebral Palsy. Front. Neurol. 2017, 8, 582. [Google Scholar] [CrossRef]
- Chruscikowski, E.; Fry, N.R.D.; Noble, J.J.; Gough, M.; Shortland, A.P. Selective motor control correlates with gait abnormality in children with cerebral palsy. Gait Posture 2017, 52, 107–109. [Google Scholar] [CrossRef]
- Pavão, S.L.; Santos, A.N.; Oliveira, A.B.; Rocha, N.A.C.F. Postural control during sit-to-stand movement and its relationship with upright position in children with hemiplegic spastic cerebral palsy and in typically developing children. Braz. J. Phys. Ther. 2015, 19, 18–25. [Google Scholar] [CrossRef]
- Reina, R.; Domínguez-Díez, M.; Urban, T.; Roldan, A. Throwing distance constraints regarding kinematics and accuracy in high-level boccia players. Sci. Sports 2018, 33, 299–306. [Google Scholar] [CrossRef]
- Mason, B.S.; Van Der Woude, L.H.V.; Goosey-Tolfrey, V.L. The Ergonomics of Wheelchair Configuration for Optimal Performance in the Wheelchair Court Sports. Sports Med. 2012, 43, 23–38. [Google Scholar] [CrossRef]
- Ben Kibler, W.; Press, J.; Sciascia, A. The role of core stability in athletic function. Sports Med. 2006, 36, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Hyde, A.; Hogarth, L.; Sayers, M.G.; Beckman, E.; Connick, M.J.; Tweedy, S.; Burkett, B. The Impact of an Assistive Pole, Seat Configuration, and Strength in Paralympic Seated Throwing. Int. J. Sports Physiol. Perform. 2017, 12, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Connick, M.J.; Beckman, E.; Vanlandewijck, Y.C.; A Malone, L.; Blomqvist, S.; Tweedy, S.M. Cluster analysis of novel isometric strength measures produces a valid and evidence-based classification structure for wheelchair track racing. Br. J. Sports Med. 2017, 52, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Altmann, V.; Groen, B.; Hart, A.L.; Vanlandewijck, Y.C.; Keijsers, N.L.W. Classifying trunk strength impairment according to the activity limitation caused in wheelchair rugby performance. Scand. J. Med. Sci. Sports 2017, 28, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Ozinga, S.J.; Koop, M.M.; Linder, S.M.; Machado, A.G.; Dey, T.; Alberts, J.L. Three-dimensional evaluation of postural stability in Parkinson’s disease with mobile technology. Neurorehabilit. 2017, 41, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Barbado, D.; Irles-Vidal, B.; Prat-Luri, A.; García-Vaquero, M.P.; Vera-Garcia, F.J. Training intensity quantification of core stability exercises based on a smartphone accelerometer. PLoS ONE 2018, 13, e0208262. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Variables | BC1 n = 13 | BC2 n = 23 | Overall n = 36 |
|---|---|---|---|
| Age (year) | 39.00 ± 13.20 | 34.50 ± 14.14 | 36.33 ± 13.69 |
| Body Mass (kg) | 53.65 ± 10.96 | 51.56 ± 11.89 | 52.02 ± 11.04 |
| Trunk Height (cm) | 43.50 ± 2.12 | 54.67 ± 7.36 | 52.64 ± 8.02 |
| Impairment type (muscle tone) | |||
| Spasticity | 7 (53.85) | 13 (56.52) | 20 (55.56) |
| Athetosis/Dystonia | 1 (7.69) | 4 (17.39) | 5 (13.89) |
| Mixed (spastic/athetoid) | 5 (38.46) | 6 (26.09) | 11 (30.56) |
| Sex | |||
| Male, n (%) | 6 (46.15) | 14 (60.87) | 20 (55.56) |
| Female, n (%) | 7 (53.85) | 9 (39.13) | 16 (44.44) |
| Competition Level | |||
| Regional, n (%) | 9 (69.23) | 10 (43.48) | 19 (52.78) |
| National, n (%) | 3 (23.08) | 11 (47.83) | 14 (38.89) |
| International, n (%) | 1 (7.69) | 2 (8.69) | 3 (8.33) |
| GMFCS (level), median (range) | 4 (4–4) | 4 (2–4) | 4 (2–4) |
| Level II, n (%) | -- | 6 (26.09) | 6 (16.67) |
| Level III, n (%) | -- | 5 (21.74) | 5 (13.89) |
| Level IV, n (%) | 13 (100) | 12 (52.17) | 25 (69.44) |
| Demographic Variables | Classifier/Tester #1 | Classifier/Tester #2 |
|---|---|---|
| Age (year) | 48 | 39 |
| Sex | Female | Male |
| Background | Physiotherapist | Sports Sciences PhD |
| BISFed Classification Level | Level 3 | Level 3 |
| Classification Experience in Boccia | ||
| International (year) | 12 | 6 |
| National (year) | 22 | 16 |
| Experience in other Paralympic sports | Cerebral Palsy Football | Cerebral Palsy Football |
| World Para Athletics | World Para Athletics | |
| Para Equestrian | Wheelchair Slalom |
| BISFed TFS | SNVF | SVF | DML | DAP | DC | Comp. Static | Comp. Dynamic | |
|---|---|---|---|---|---|---|---|---|
| BISFed TFS | -- | −0.23 | −0.31 | −0.38 * | −0.35 | −0.46 * | −0.27 | −0.51 ** |
| SNVF | 0.85 ** | 0.46 ** | 0.53 ** | 0.40 * | 0.97 ** | 0.61 ** | ||
| SVF | 0.39 * | 0.54 ** | 0.36 | 0.95 ** | 0.58 ** | |||
| DML | 0.90 ** | 0.73 ** | 0.45 ** | 0.94 ** | ||||
| DAP | 0.79 ** | 0.56 ** | 0.96 ** | |||||
| DC | 0.40 * | 0.92 ** | ||||||
| Comp. Static | 0.63 ** | |||||||
| Comp. Dynamic |
| Variable | NBC1 + NBC2 = N | BC1 (Mean ± SD) | BC2 (Mean ± SD) | F | p | dg |
|---|---|---|---|---|---|---|
| BISFed TFS (unitless) | 13 + 23 = 36 | 2.2 ± 1.1 | 2.3 ± 1.1 | 0.02 | 0.892 | 0.05 |
| SNVF (mm) | 13 + 23 = 36 | 7.9 ± 6.8 | 3.4 ± 2.0 | 8.93 | 0.005 | 1.01 |
| SVF (mm) | 13 + 23 = 36 | 6.2 ± 4.9 | 2.7 ± 2.3 | 8.43 | 0.006 | 0.99 |
| DML (mm) | 12 + 22 = 34 | 8.3 ± 4.7 | 7.9 ± 4.3 | 0.06 | 0.811 | 0.09 |
| DAP (mm) | 12 + 20 = 32 | 8.8 ± 4.3 | 7.5 ± 3.8 | 0.81 | 0.374 | 0.32 |
| DC (mm) | 11 + 15 = 26 | 11.7 ± 4.4 | 8.6 ± 4.5 | 2.96 | 0.098 | 0.67 |
| Composite Static (mm) | 13 + 23 = 36 | 7.0 ± 5.7 | 3.0 ± 1.8 | 9.62 | 0.004 | 1.06 |
| Composite Dynamic (mm) | 11 + 15 = 26 | 9.4 ± 4.1 | 7.3 ± 3.4 | 1.97 | 0.173 | 0.55 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roldan, A.; Barbado, D.; Vera-Garcia, F.J.; Sarabia, J.M.; Reina, R. Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy. Brain Sci. 2020, 10, 130. https://doi.org/10.3390/brainsci10030130
Roldan A, Barbado D, Vera-Garcia FJ, Sarabia JM, Reina R. Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy. Brain Sciences. 2020; 10(3):130. https://doi.org/10.3390/brainsci10030130
Chicago/Turabian StyleRoldan, Alba, David Barbado, Francisco J. Vera-Garcia, José M. Sarabia, and Raul Reina. 2020. "Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy" Brain Sciences 10, no. 3: 130. https://doi.org/10.3390/brainsci10030130
APA StyleRoldan, A., Barbado, D., Vera-Garcia, F. J., Sarabia, J. M., & Reina, R. (2020). Inter-Rater Reliability, Concurrent Validity and Sensitivity of Current Methods to Assess Trunk Function in Boccia Players with Cerebral Palsy. Brain Sciences, 10(3), 130. https://doi.org/10.3390/brainsci10030130