Factors Modifying the Amount of Neuroanatomical Overlap between Languages in Bilinguals—A Systematic Review of Neurosurgical Language Mapping Studies


Abstract
1. Introduction
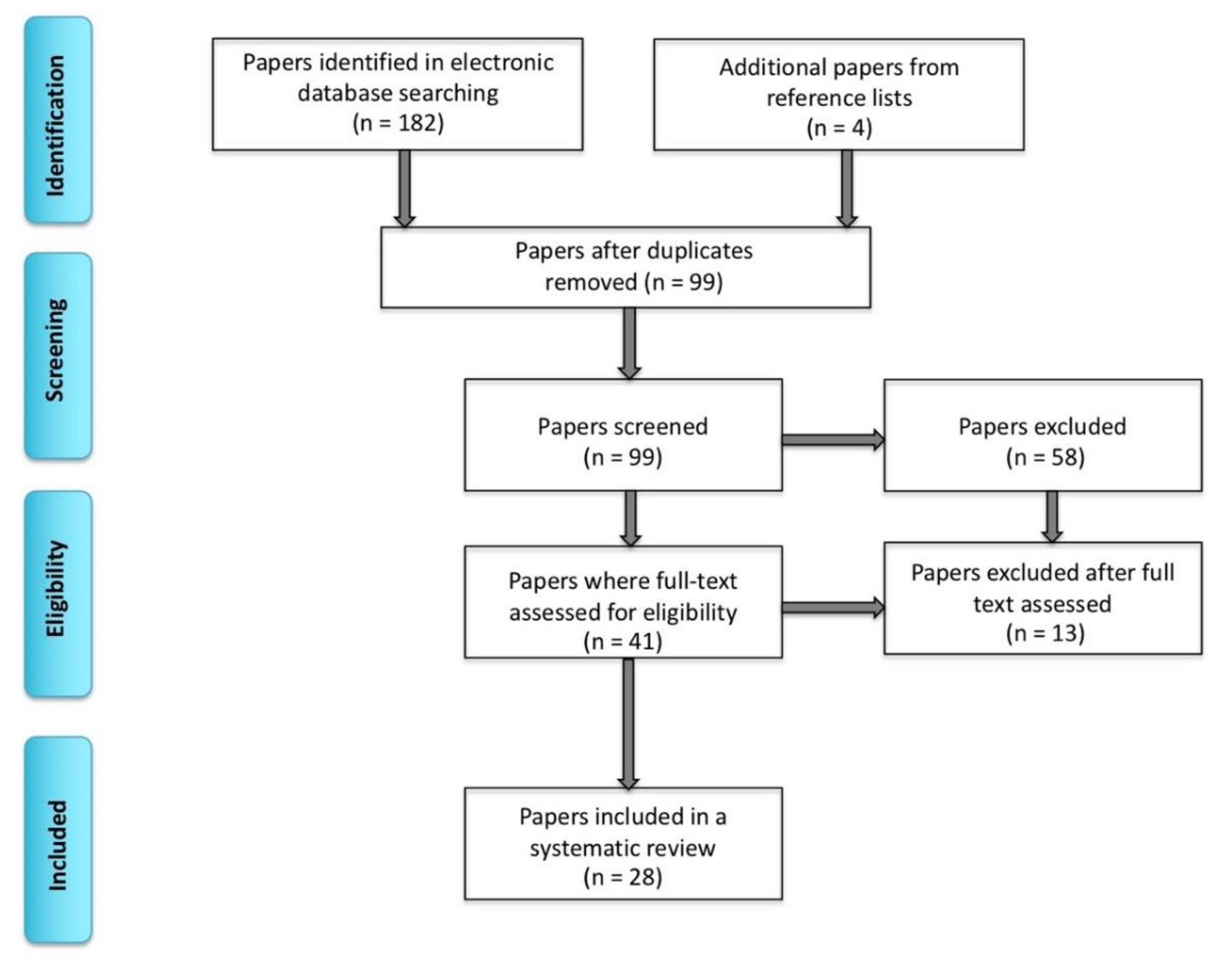
2. Materials and Methods
3. Results
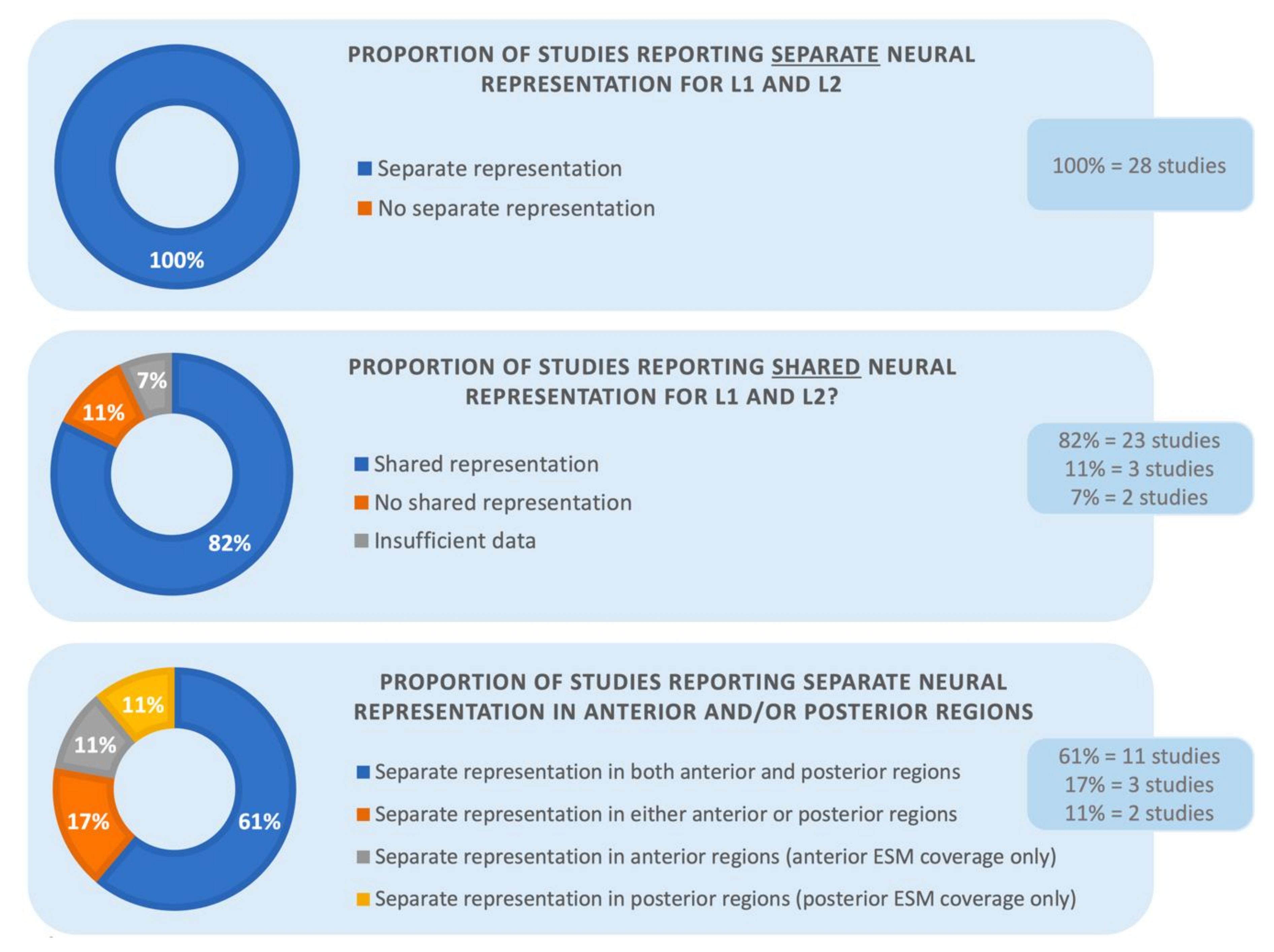
3.1. Distinct Versus Overlapping Representations of L1 and L2
3.2. Regional Specificity of Language Overlap
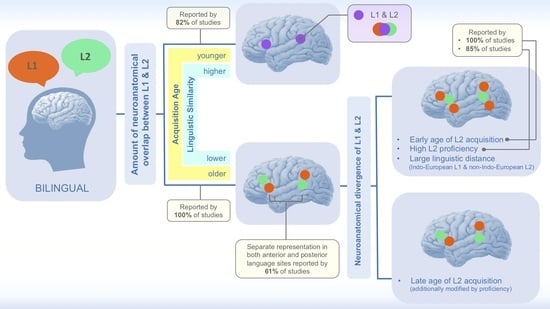
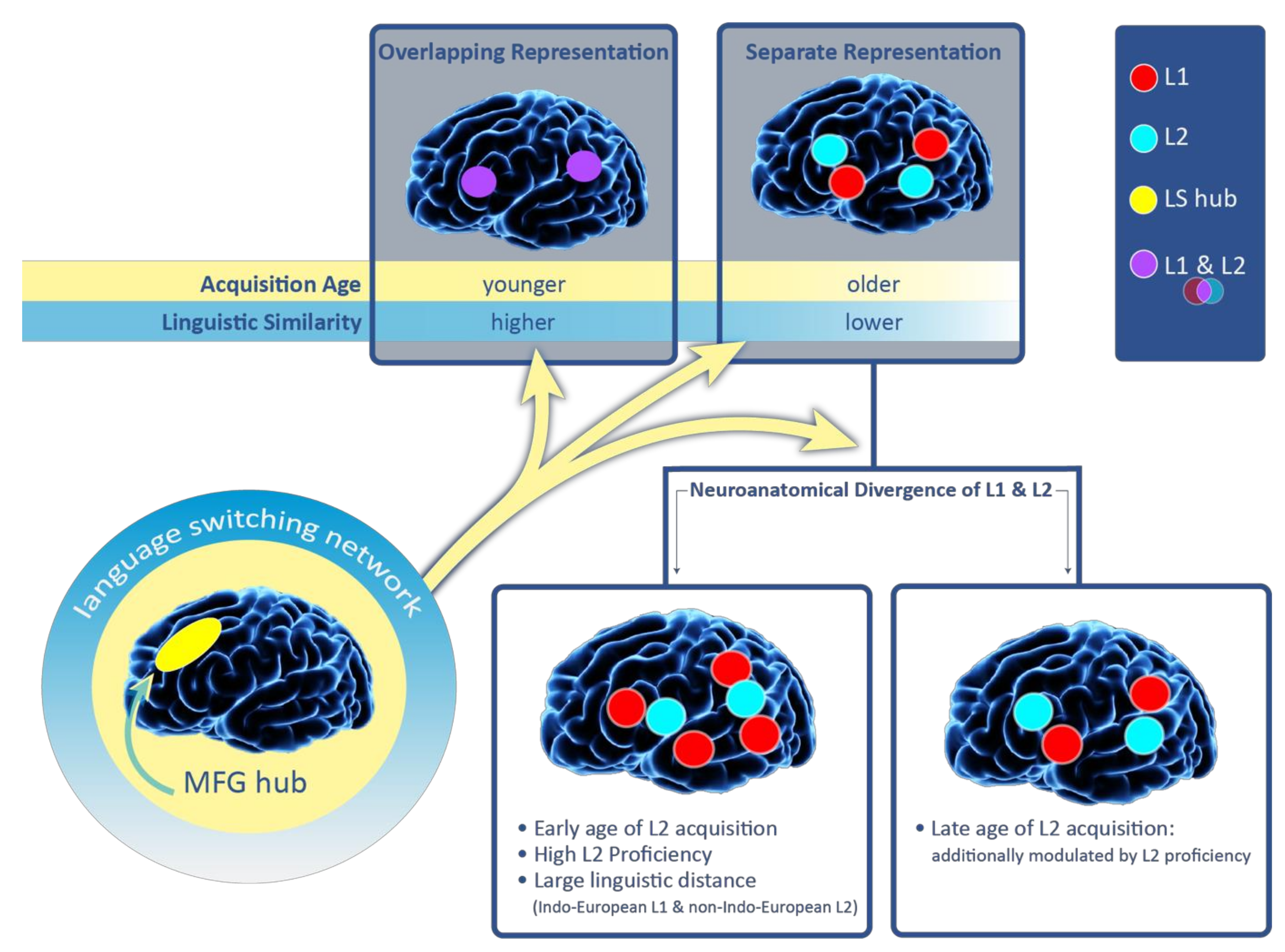
3.3. Factors Modifying the Amount of Overlap between L1 and L2
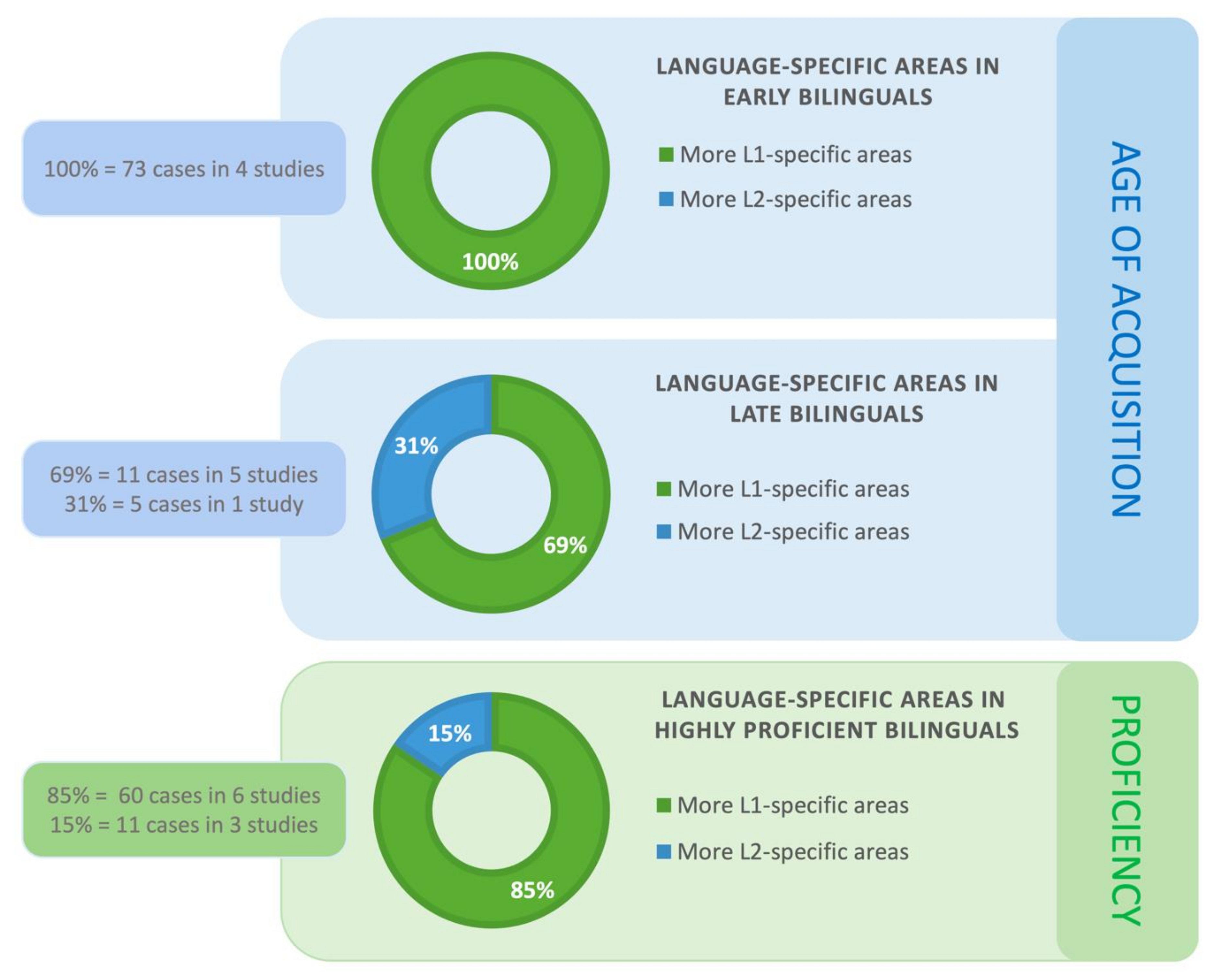
3.3.1. Age of Acquisition
3.3.2. Proficiency
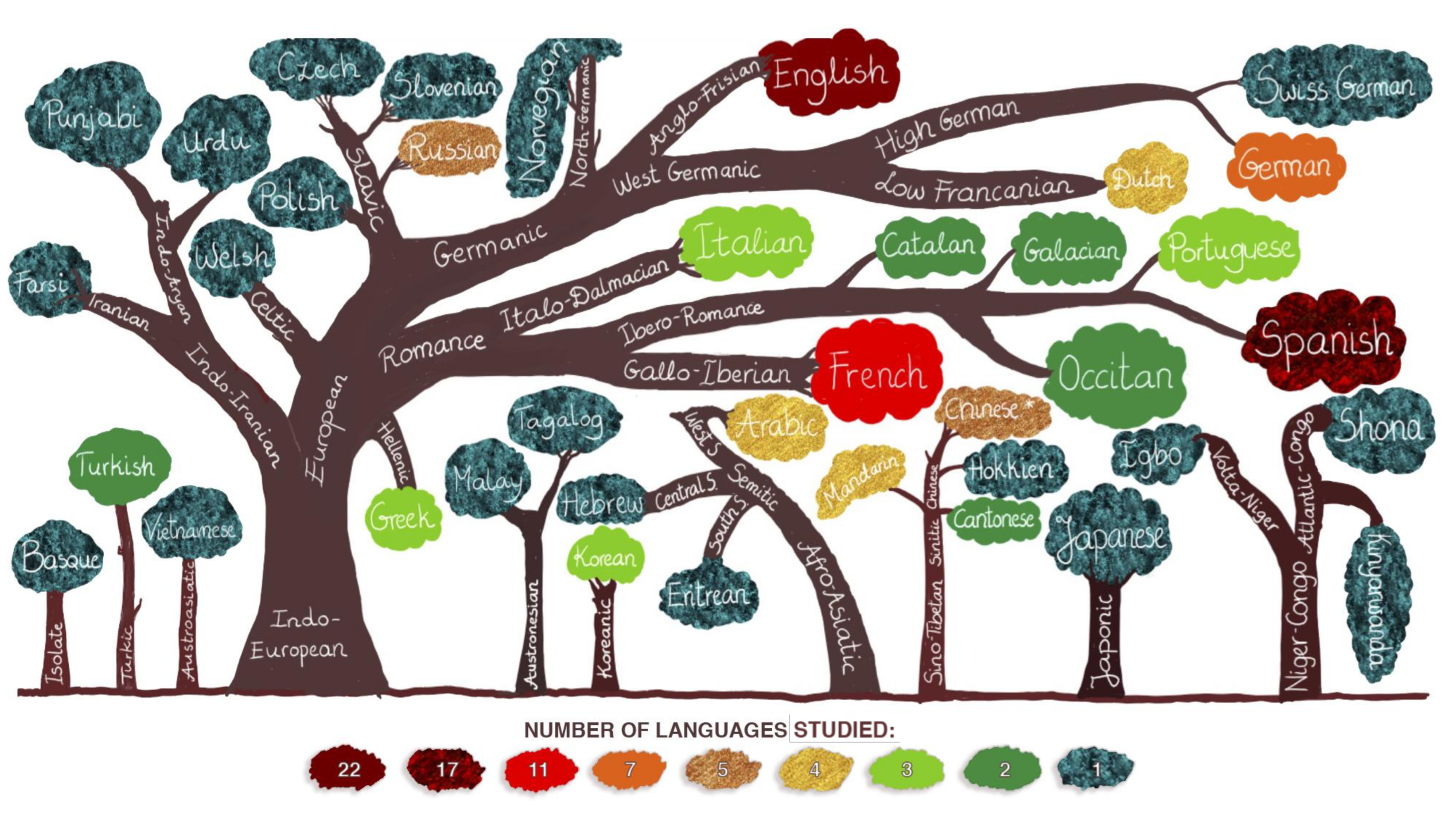
3.3.3. The Linguistic Distance between Languages
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimers
Appendix A. Draft Pubmed Search
- bilingual AND clinical language mapping
- bilingualism AND clinical language mapping
- multilingual AND clinical language mapping
- multilingualism AND clinical language mapping
- bilingual AND fMRI AND brain tumor
- bilingualism AND fMRI AND brain tumor
- bilingual AND fMRI AND epilepsy
- bilingualism AND fMRI AND epilepsy
- bilingual AND fMRI AND arteriovenous malformation
- bilingualism AND fMRI AND arteriovenous malformation
- multilingual AND fMRI AND brain tumor
- multilingualism AND fMRI AND brain tumor
- multilingual AND fMRI AND epilepsy
- multilingualism AND fMRI AND epilepsy
- multilingual AND fMRI AND arteriovenous malformation
- multilingualism AND fMRI AND arteriovenous malformation
- bilingual AND Wada
- bilingualism AND Wada
- multilingual AND Wada
- multilingualism AND Wada
- bilingual AND awake surgery
- bilingualism AND awake surgery
- multilingual AND awake surgery
- multilingualism AND awake surgery
- bilingual AND direct electrical stimulation
- bilingualism AND direct electrical stimulation
- multilingual AND direct electrical stimulation
- multilingualism AND direct electrical stimulation
- bilingual AND bilingual AND electrocorticography
- bilingualism AND electrocorticography
- multilingual AND electrocorticography
- multilingualism AND electrocorticography
- bilingualism AND direct electrical stimulation
- multilingual AND direct electrical stimulation
- multilingualism AND direct electrical stimulation
- bilingual AND EEG AND brain tumor
- bilingualism AND EEG AND brain tumor
- bilingual AND EEG AND epilepsy
- bilingualism AND EEG AND epilepsy
- bilingual AND EEG AND arteriovenous malformation
- bilingualism AND EEG AND arteriovenous malformation
- multilingual AND EEG AND brain tumor
- multilingualism AND EEG AND brain tumor
- multilingual AND EEG AND epilepsy
- multilingualism AND EEG AND epilepsy
- multilingual AND EEG AND arteriovenous malformation
- multilingualism AND EEG AND arteriovenous malformation
- bilingual AND MEG AND tumor
- bilingualism AND MEG AND tumor
- bilingual AND MEG AND epilepsy
- bilingualism AND MEG AND epilepsy
- bilingual AND MEG AND arteriovenous malformation
- bilingualism AND MEG AND arteriovenous malformation
- multilingual AND MEG AND tumor
- multilingualism AND MEG AND tumor
- multilingual AND MEG AND epilepsy
- multilingualism AND MEG AND epilepsy
- multilingual AND MEG AND arteriovenous malformation
- multilingualism AND MEG AND arteriovenous malformation
- bilingual AND TMS AND tumor
- bilingualism AND TMSAND tumor
- bilingual AND TMSAND epilepsy
- bilingualism AND TMS AND epilepsy
- bilingual AND TMS AND arteriovenous malformation
- bilingualism AND TMS AND arteriovenous malformation
- multilingual AND TMS AND tumor
- multilingualism AND TMS AND tumor
- multilingual AND TMS AND epilepsy
- multilingualism AND TMS AND epilepsy
- multilingual AND TMS AND arteriovenous malformation
- multilingualism AND TMS AND arteriovenous malformation.
References
- Grosjean, F. Bilingual: Life and Reality; Harvard University Press: Cambridge, MA, USA, 2010. [Google Scholar]
- Fernández-Coello, A.; Havas, V.; Juncadella, M.; Sierpowska, J.; Rodríguez-Fornells, A.; Gabarrós, A. Age of language acquisition and cortical language organization in multilingual patients undergoing awake brain mapping. J. Neurosurg. 2017, 126, 1912–1923. [Google Scholar] [CrossRef] [PubMed]
- Ojemann, G.A.; Whitaker, H.A. The bilingual brain. Arch. Neurol. 1978, 35, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Bello, L.; Acerbi, F.; Giussani, C.; Baratta, P.; Taccone, P.; Songa, V. Technique application. Neurosurgery 2006, 58, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Cao, F.; Tao, R.; Liu, L.; Perfetti, C.A.; Booth, J.R. High proficiency in a second language is characterized by greater involvement of the first language network: Evidence from Chinese learners of English. J. Cogn. Neurosci. 2013, 25, 1649–1663. [Google Scholar] [CrossRef]
- Cargnelutti, E.; Tomasino, B.; Fabbro, F. Language brain representation in bilinguals with different age of appropriation and proficiency of the second language: A meta-analysis of functional imaging studies. Front. Hum. Neurosci. 2019, 13, 154. [Google Scholar] [CrossRef]
- Gao, H.; Bai, H.M.; Han, L.X.; Li, T.D.; Wang, G.L.; Wang, W.M. Brain cancer surgery in the language areas of Mandarin-Cantonese bilinguals. J. Cancer Res. Ther. 2015, 11, 415–419. [Google Scholar] [CrossRef]
- Kim, S.Y.; Qi, T.; Feng, X.; Ding, G.; Liu, L.; Cao, F. How does language distance between L1 and L2 affect the L2 brain network? An fMRI study of Korean-Chinese-English trilinguals. Neuroimage 2016, 129, 25–39. [Google Scholar] [CrossRef]
- Lucas, T.H.; McKhann, G.M.; Ojemann, G.A. Functional separation of languages in the bilingual brain: A comparison of electrical stimulation language mapping in 25 bilingual patients and 117 monolingual control patients. J. Neurosurg. 2004, 101, 449–457. [Google Scholar] [CrossRef]
- Perani, D.; Abutalebi, J.; Paulesu, E.; Brambati, S.; Scifo, P.; Cappa, S.F.; Fazio, F. The role of age of acquisition and language usage in early, high-proficient bilinguals: An fMRI study during verbal fluency. Hum. Brain Mapp. 2003, 19, 170–182. [Google Scholar] [CrossRef]
- Hernandez, A.E. The Bilingual Brain; Oxford University Press: Oxford, UK, 2013; ISBN 0199828113. [Google Scholar]
- Hull, R.; Vaid, J. Bilingual language lateralization: A meta-analytic tale of two hemispheres. Neuropsychologia 2007, 45, 1987–2008. [Google Scholar] [CrossRef]
- Perani, D.; Paulesu, E.; Galles, N.S.; Dupoux, E.; Dehaene, S.; Bettinardi, V.; Cappa, S.F.; Fazio, F.; Mehler, J. The bilingual brain. Proficiency and age of acquisition of the second language. Brain 1998, 121, 1841–1852. [Google Scholar] [CrossRef] [PubMed]
- Tu, L.; Wang, J.; Abutalebi, J.; Jiang, B.; Pan, X.; Li, M.; Gao, W.; Yang, Y.; Liang, B.; Lu, Z.; et al. Language exposure induced neuroplasticity in the bilingual brain: A follow-up fMRI study. Cortex 2015, 64, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Morgan-Short, K.; Steinhauer, K.; Sanz, C.; Ullman, M.T. Explicit and implicit second language training differentially affect the achievement of native-like brain activation patterns. J. Cogn. Neurosci. 2012, 24, 933–947. [Google Scholar] [CrossRef] [PubMed]
- Kochunov, P.; Fox, P.; Lancaster, J.; Tan, L.H.; Amunts, K.; Zilles, K.; Mazziotta, J.; Gao, J.H. Localized morphological brain differences between English-speaking Caucasians and Chinese-speaking Asians: New evidence of anatomical plasticity. Neuroreport 2003, 14, 961–964. [Google Scholar] [CrossRef]
- Emmorey, K.; Giezen, M.R.; Gollan, T.H. Psycholinguistic, cognitive, and neural implications of bimodal bilingualism. Bilingualism 2016, 19, 223–242. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 6. [Google Scholar] [CrossRef]
- Pouratian, N.; Bookheimer, S.; O’Farrell, A.; Sicotte, N.; Cannestra, A.; Beckerf, D.; Toga, A. Optical imaging of bilingual cortical representations. Neuroimage 2000, 93, 676–681. [Google Scholar] [CrossRef]
- Połczyńska, M.M.; Japardi, K.; Bookheimer, S.Y. Lateralizing language function with pre-operative functional magnetic resonance imaging in early proficient bilingual patients. Brain Lang. 2017, 170, 1–11. [Google Scholar] [CrossRef]
- Cheung, M.C.; Chan, A.S.; Sze, S.L. Increased theta coherence during Chinese reading. Int. J. Psychophysiol. 2009, 74, 132–138. [Google Scholar] [CrossRef]
- Roux, F.E.; Lubrano, V.; Lauwers-Cances, V.; Trémoulet, M.; Mascott, C.R.; Démonet, J.F. Intra-operative mapping of cortical areas involved in reading in mono- and bilingual patients. Brain 2004, 127, 1796–1810. [Google Scholar] [CrossRef]
- Walker, J.A.; Quiñones-Hinojosa, A.; Berger, M.S.; Grossman, R.G. Intraoperative speech mapping in 17 bilingual patients undergoing resection of a mass lesion. Neurosurgery 2004, 54, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Centeno, M.; Koepp, M.J.; Vollmar, C.; Stretton, J.; Sidhu, M.; Michallef, C.; Symms, M.R.; Thompson, P.J.; Duncan, J.S. Language dominance assessment in a bilingual population: Validity of fMRI in the second language. Epilepsia 2014, 55, 1504–1511. [Google Scholar] [CrossRef] [PubMed]
- Roux, F.E.; Trétmoulet, M. Organization of language areas in bilingual patients: A cortical stimulation study. J. Neurosurg. 2002, 97, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Sierpowska, J.; Fernandez-Coello, A.; Gomez-Andres, A.; Camins, À.; Castañer, S.; Juncadella, M.; Gabarrós, A.; Rodríguez-Fornells, A. Involvement of the middle frontal gyrus in language switching as revealed by electrical stimulation mapping and functional magnetic resonance imaging in bilingual brain tumor patients. Cortex 2018, 99, 78–92. [Google Scholar] [CrossRef] [PubMed]
- Rapport, R.L.; Tan, C.T.; Whitaker, H.A. Language function and dysfunction among Chinese and English speaking polyglots: Cortical stimulation, Wada Testing, and clinical studies. Brain Lang. 1983, 18, 342–366. [Google Scholar] [CrossRef]
- Borius, P.Y.; Giussani, C.; Draper, L.; Roux, F.E. Sentence translation in proficient bilinguals: A direct electrostimulation brain mapping. Cortex 2012, 48, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Cervenka, M.C.; Boatman-Reich, D.F.; Ward, J.; Franaszczuk, P.J.; Crone, N.E. Language mapping in multilingual patients: Electrocorticography and cortical stimulation during naming. Front. Hum. Neurosci. 2011, 5, 13. [Google Scholar] [CrossRef]
- Sierpowska, J.; Gabarrós, A.; Ripollés, P.; Juncadella, M.; Castañer, S.; Camins, Á.; Plans, G.; Rodríguez-Fornells, A. Intraoperative electrical stimulation of language switching in two bilingual patients. Neuropsychologia 2013, 51, 2882–2892. [Google Scholar] [CrossRef]
- Kho, K.H.; Duffau, H.; Gatignol, P.; Leijten, F.S.S.; Ramsey, N.F.; van Rijen, P.C.; Rutten, G.J.M. Involuntary language switching in two bilingual patients during the Wada test and intraoperative electrocortical stimulation. Brain Lang. 2007, 101, 31–37. [Google Scholar] [CrossRef]
- Bilotta, F.; Stazi, E.; Delfini, R.; Rosa, G. Language testing during awake “anesthesia” in a bilingual patient with brain lesion adjacent to Wernicke’s area. Anesth. Analg. 2011, 112, 938–939. [Google Scholar] [CrossRef]
- Połczyńska, M.M.; Benjamin, C.F.A.; Japardi, K.; Frew, A.; Bookheimer, S.Y. Language system organization in a quadrilingual with a brain tumor: Implications for understanding of the language network. Neuropsychologia 2016, 86, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Kin, H.; Ishikawa, E.; Takano, S.; Ayuzawa, S.; Matsushita, A.; Muragaki, Y.; Aiyama, H.; Sakamoto, N.; Yamamoto, T.; Matsumura, A. Language areas involving the inferior temporal cortex on intraoperative mapping in a bilingual patient with glioblastoma. Neurol. Med. Chir. 2013, 53, 256–258. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Serafini, S.; Gururangan, S.; Friedman, A.; Haglund, M. Identification of distinct and overlapping cortical areas for bilingual naming and reading using cortical stimulation: Case report. J. Neurosurg. Pediatr. 2008, 1, 247–254. [Google Scholar] [CrossRef] [PubMed]
- O’Grady, C.; Omisade, A.; Sadler, R.M. Language lateralization of a bilingual person with epilepsy using a combination of fMRI and neuropsychological assessment findings. Neurocase 2016, 22, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Gomeztortosa, E.; Martin, E.M.; Gaviria, M.; Charbel, F.; Ausman, J.I. Selective deficit of one language in a bilingual patient following surgery in the left perisylvian area. Brain Lang. 1995, 48, 320–325. [Google Scholar] [CrossRef]
- Berthier, M.L.; Starkstein, S.E.; Lylyk, P.; Leiguarda, R. Differential recovery of languages in a bilingual patient: A case study using selective amytal test. Brain Lang. 1990, 38, 449–453. [Google Scholar] [CrossRef]
- Lubrano, V.; Prod’homme, K.; Démonet, J.F.; Köpke, B. Language monitoring in multilingual patients undergoing awake craniotomy: A case study of a German-English-French trilingual patient with a WHO grade II glioma. J. Neurolinguistics 2012, 25, 567–578. [Google Scholar] [CrossRef]
- Navarro, V.; Delmaire, C.; Chauviré, V.; Habert, M.O.; Footnick, R.; Lehéricy, S.; Baulac, M.; Pallier, C.; Cohen, L. “What is it?” A functional MRI and SPECT study of ictal speech in a second language. Epilepsy Behav. 2009, 14, 396–399. [Google Scholar] [CrossRef]
- Wang, X.; Wang, Y.Y.; Jiang, T.; Wang, Y.Z.; Wu, C.X. Direct evidence of the left caudate’s role in bilingual control: An intra-operative electrical stimulation study. Neurocase 2013, 19, 462–469. [Google Scholar] [CrossRef]
- Berken, J.A.; Chai, X.; Chen, J.K.; Gracco, V.L.; Klein, D. Effects of early and late bilingualism on resting-state functional connectivity. J. Neurosci. 2016, 36, 1165–1172. [Google Scholar] [CrossRef]
- Abutalebi, J.; Green, D.W. Control mechanisms in bilingual language production: Neural evidence from language switching studies. Lang. Cogn. Process. 2008, 23, 557–582. [Google Scholar] [CrossRef]
- Green, D.W.; Abutalebi, J. Language control in bilinguals: The adaptive control hypothesis. J. Cogn. Psychol. 2013, 25, 515–530. [Google Scholar] [CrossRef] [PubMed]
- Council of Europe. The Common European Framework of Reference for Languages. Europe 2001. [Google Scholar] [CrossRef]
- Lewis, M.P.; Simons, G.F.; Fennig, C.D. Ethnologue: Languages of the World, 21st ed.; SIL International: Dallas, TX, USA; Available online: https://www.ethnologue.com/ (accessed on 1 March 2019).
- Kroll, J.F.; Dussias, P.E.; Bice, K.; Perrotti, L. Bilingualism, mind, and brain. Annu. Rev. Linguist. 2015, 1, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Abutalebi, J.; Zinszer, B.; Yan, X.; Shu, H.; Peng, D.; Ding, G. Second language experience modulates functional brain network for the native language production in bimodal bilinguals. Neuroimage 2012, 62, 1367–1375. [Google Scholar] [CrossRef]
- Meschyan, G.; Hernandez, A.E. Impact of language proficiency and orthographic transparency on bilingual word reading: An fMRI investigation. Neuroimage 2006, 29, 1135–1140. [Google Scholar] [CrossRef]
- de Bruin, A. Not all bilinguals are the same: A call for more detailed assessments and descriptions of bilingual experiences. Behav. Sci. 2019, 9, 33. [Google Scholar] [CrossRef]
- Dziubalska-Kołaczyk, K.; Wrembel, M. Natural growth theory of acquisition (NGTA): Evidence from (mor)phonotactics. In Theoretical and Practical Perspectives on English Pronunciation Teaching and Research; Springer: Amsterdam, The Netherlands, in press.
- Mieszkowska, K.; Łuniewska, M.; Kołak, J.; Kacprzak, A.; Wodniecka, Z.; Haman, E. Home language will not take care of itself: Vocabulary knowledge in trilingual children in the United Kingdom. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef]
- Chou, N.; Serafini, S.; Muh, C.R. Cortical language areas and plasticity in pediatric patients with epilepsy: A review. Pediatr. Neurol. 2018, 78, 3–12. [Google Scholar] [CrossRef]
- Lee, D.J.; Pouratian, N.; Bookheimer, S.Y.; Martin, N.A. Factors predicting language lateralization in patients with perisylvian vascular malformations: Clinical article. J. Neurosurg. 2010, 113, 723–730. [Google Scholar] [CrossRef]
- Batouli, S.A.H.; Hasani, N.; Gheisari, S.; Behzad, E.; Oghabian, M.A. Evaluation of the factors influencing brain language laterality in presurgical planning. Phys. Med. 2016, 32, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, C.F.; Walshaw, P.D.; Hale, K.; Gaillard, W.D.; Baxter, L.C.; Berl, M.M.; Polczynska, M.; Noble, S.; Alkawadri, R.; Hirsch, L.J.; et al. Presurgical language fMRI: Mapping of six critical regions. Hum. Brain Mapp. 2017, 38, 4239–4255. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.E.; Li, P. Age of acquisition: Its neural and computational mechanisms. Psychol. Bull. 2007, 133, 638–650. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Swanson, S.J.; Sabsevitz, D.S.; Hammeke, T.A.; Winstanley, F.S.; Possing, E.T.; Binder, J.R. Functional MRI and Wada studies in patients with interhemispheric dissociation of language functions. Epilepsy Behav. 2008, 13, 350–356. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Połczyńska, M.M.; Benjamin, C.F.A.; Moseley, B.D.; Walshaw, P.; Eliashiv, D.; Vigil, C.; Jones, M.; Bookheimer, S.Y. Role of the Wada test and functional magnetic resonance imaging in preoperative mapping of language and memory: Two atypical cases. Neurocase 2015, 21, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Rofes, A.; Spena, G.; Miozzo, A.; Fontanella, M.M.; Miceli, G. Advantages and disadvantages of intraoperative language tasks in awake surgery: A three-task approach for prefrontal tumors. J. Neurosurg. Sci. 2015, 59, 337–349. [Google Scholar] [PubMed]
- Gaillard, W.D.; Balsamo, L.; Xu, B.; McKinney, C.; Papero, P.H.; Weinstein, S.; Conry, J.; Pearl, P.L.; Sachs, B.; Sato, S.; et al. fMRI language task panel improves determination of language dominance. Neurology 2004, 63, 1403–1408. [Google Scholar] [CrossRef]
- Benjamin, C.F.; Dhingra, I.; Li, A.X.; Blumenfeld, H.; Alkawadri, R.; Bickel, S.; Helmstaedter, C.; Meletti, S.; Bronen, R.A.; Warfield, S.K.; et al. Presurgical language fMRI: Technical practices in epilepsy surgical planning. Hum. Brain Mapp. 2018, 39, 4032–4042. [Google Scholar] [CrossRef]
- Hamberger, M.J. Cortical language mapping in epilepsy: A critical review. Neuropsychol. Rev. 2007, 17, 477–489. [Google Scholar] [CrossRef]
- Bolger, D.J.; Perfetti, C.A.; Schneider, W. Cross-cultural effect on the brain revisited: Universal structures plus writing system variation. Hum. Brain Mapp. 2005, 25, 92–104. [Google Scholar] [CrossRef]
- Jeong, H.; Sugiura, M.; Sassa, Y.; Haji, T.; Usui, N.; Taira, M.; Horie, K.; Sato, S.; Kawashima, R. Effect of syntactic similarity on cortical activation during second language processing: A comparison of English and Japanese among native Korean trilinguals. Hum. Brain Mapp. 2007, 23, 194–204. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | No. of Patients | Etiology | Lesion Location | Age | Handedness | Gender | Aphasia | Onset Age | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tumor | Epilepsy | AVM | Aneur | LH | RH | n-L | Ant | Post | N/A | Right | Left | Mixed | Male | Female | Yes | No | ||||
| Połczyńska et al., 2017 [20] | 25 | 17 | 5 | 3 | 17 | 8 | 14 | 11 | 15–83 | 22 | 3 | 14 | 11 | 15 | 10 | N/A | ||||
| Lucas et al., 2004 [9] | 22 | 22 | 21 | 1 | 22 | 18–53 | 18 | 2 | 2 | 5 | 17 | 22 | N/A | |||||||
| Cheung et al., 2009 [21] | 21 | 21 | 13 | 8 | 21 | 14–48 | 21 | 9 | 12 | N/A | N/A | 1 to 47 | ||||||||
| Roux et al., 2004 [22] | 19 | 19 | 14 | 5 | 19 | 13–76 | 18 | 1 | N/A * | N/A * | 19 | N/A | ||||||||
| Walker et al., 2004 [23] | 17 | 17 | 17 | 9 | 8 | 15–57 | 14 | 3 | 11 | 6 | N/A | N/A | N/A | |||||||
| Centeno et al., 2014 *** [24] | 16 | 16 | 9 | 4 | 3 | 16 | 24–50 | 14 | 2 | 13 | 3 | N/A | N/A | >1 to 27 | ||||||
| Roux & Trémoulet, 2002 [25] | 12 | 12 | 12 | 7 | 5 | 30–74 | 12 | 8 | 4 | 12 | N/A | |||||||||
| Fernández-Coello et al., 2017 [2] | 13 | 13 | 13 | 6 | 6 | 1 | 25–62 | 13 | 5 | 8 | 1 | N/A | ||||||||
| Gao et al., 2015 ** [7] | 11 | 11 | 11 | 11 | 24–46 | 11 | 8 | 3 | 1 | 10 | N/A | |||||||||
| Sierpowska et al., 2018 [26] | 9 | 9 | 9 | 9 | 1 | 30–54 | N/AA | 5 | 4 | 9 | N/A | |||||||||
| Bello et al., 2006 [4] | 7 | 7 | 7 | 7 | 32-58 | 7 | 4 | 3 | 7 | N/A | ||||||||||
| Rapport et al., 1983 [27] | 7 | 3 | 1 | 1 | 2 | 5 | 2 | 3 | 3 | 1 | 23-45 | 7 | 5 | 2 | 2 | 7 | 21–45, N/A | |||
| Borius et al., 2012 [28] | 7 | 7 | 5 | 2 | 5 | 2 | 26-45 | 5 | 2 | 3 | 4 | 7 | N/A | |||||||
| Cervenka et al., 2011 [29] | 4 | 4 | 4 | 4 | 28-50 | 3 | 1 | 3 | 1 | 4 | 8 to 31 | |||||||||
| Ojemann & Whitaker, 1978 [3] | 2 | 2 | 1 | 1 | 1 | 1 | 37, 20 | 1 | 1 | 1 | 1 | N/A | N/A | 4, 6 | ||||||
| Sierpowska et al., 2013 [30] | 2 | 2 | 2 | 1 | 1 | 60, 36 | 2 | 2 | 2 | 36 | ||||||||||
| Kho et al., 2007 [31] | 2 | 1 | 1 | 2 | 1 | 1 | 36, 50 | 2 | 2 | 2 | 7, 44 | |||||||||
| Bilotta et al., 2011 [32] | 1 | 1 | 1 | 1 | 54 | N/A | N/A | N/A | 1 | N/A | N/A | 54 | ||||||||
| Połczyńska et al., 2016 [33] | 1 | 1 | 1 | 1 | 60 | 1 | 1 | 1 | 60 | |||||||||||
| Kin et al., 2013 [34] | 1 | 1 | 1 | 1 | 40 | 1 | 1 | 1 | 40 | |||||||||||
| Pouratian et al., 2000 [19] | 1 | 1 | 1 | 1 | 43 | 1 | 1 | 1 | 37 | |||||||||||
| Serafini et al., 2008 [35] | 1 | 1 | 1 | 1 | 13 | 1 | 1 | 1 | 6 | |||||||||||
| O’Grady et al., 2016 [36] | 1 | 1 | 1 | 1 | 33 | 1 | 1 | 1 | 5 | |||||||||||
| Gomez-Tortosa et al., 1995 [37] | 1 | 1 | 1 | 1 | 22 | 1 | 1 | 1 | 19 | |||||||||||
| Berthier et al., 1990 [38] | 1 | 1 | 1 | 1 | 25 | 1 | 1 | 1 | N/A | |||||||||||
| Lubrano et al., 2012 [39] | 1 | 1 | 1 | 1 | 31 | 1 | 1 | 1 | 31 | |||||||||||
| Navarro et al., 2009 [40] | 1 | 1 | 1 | 1 | 34 | 1 | 1 | N/A | N/A | 1 | ||||||||||
| Wang et al., 2013 [41] | 1 | 1 | 1 | 1 | 25 | 1 | 1 | 1 | 25 | |||||||||||
| TOTAL VALUES | 207 | 1255 | 74 | 6 | 2 | 171 | 33 | 3 | 111 | 42 | 55 | 179 | 12 | 6 | 102 | 86 | 23 | 116 | ||
| Study | Method | Tasks | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ESM | fMRI | Wada | Other | TOTAL | OBJ | ARN | Read | Count | ActionN | VerbG | Rep | VRN | OBJ S | Other | TOTAL | |
| Połczyńska et al., 2017 [20] | 1 | 1 | 1 | 1 | 1 | 3 | ||||||||||
| Lucas et al., 2004 [9] | 1 | 1 | 1 | 1 | ||||||||||||
| Cheung et al., 2009 [21] | 1 | 1 | 1 | 1 | ||||||||||||
| Roux et al., 2004 [22] | 1 | 1 | 1 | 1 | 2 | |||||||||||
| Walker et al., 2004 [23] | 1 | 1 | 1 | 1 | ||||||||||||
| Centeno et al., 2014 [24] | 1 | 1 | 1 | 1 | 2 | |||||||||||
| Roux & Trémoulet, 2002 [25] | 1 | 1 | 1 | 1 | 2 | |||||||||||
| Fernández-Coello et al., 2017 [2] | 1 | 1 | 1 | 1 | ||||||||||||
| Gao et al., 2015 [7] | 1 | 1 | 1 | 1 | 1 | 3 | ||||||||||
| Sierpowska et al., 2018 [26] | 1 | 1 | 2 | 1 | 1 | 1 | 1 | |||||||||
| Bello et al., 2006 [4] | 1 | 1 | 1 | 1 | 1 | 1 | 4 | |||||||||
| Rapport et al., 1983 [27] | 1 | 1 | 2 | 1 | 1 | 2 | ||||||||||
| Borius et al., 2012 [28] | 1 | 1 | 1 | 1 | 1 | 3 | ||||||||||
| Cervenka et al., 2011 [29] | 1 | 1 | 1 | 1 | ||||||||||||
| Ojemann & Whitaker, 1978 [3] | 1 | 1 | 1 | 1 | ||||||||||||
| Sierpowska et al., 2013 [30] | 1 | 1 | 2 | 1 | 1 | 1 | 3 | |||||||||
| Kho et al., 2007 [31] | 1 | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 4 | |||||||
| Bilotta et al., 2011 [32] | 1 | 1 | 1 | 1 | 1 | 1 | 4 | |||||||||
| Połczyńska et al., 2016 [33] | 1 | 1 | 2 | 1 | 1 | 1 | 3 | |||||||||
| Kin et al., 2013 [34] | 1 | 1 | 1 | 1 | 2 | |||||||||||
| Pouratian et al., 2000 [19] | 1 | 1 | 1 | 3 | 1 | 1 | ||||||||||
| Serafini et al., 2008 [35] | 1 | 1 | 1 | 1 | 1 | 3 | ||||||||||
| O’Grady et al., 2016 [36] | 1 | 1 | 1 | 1 | 4 | 6 | ||||||||||
| Gomez-Tortosa et al., 1995 [37] | 1 | 1 | 2 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | ||
| Berthier et al., 1990 [38] | 1 | 1 | 1 | 1 | 1 | 1 | 4 | |||||||||
| Lubrano et al., 2012 [39] | 1 | 1 | 1 | 1 | ||||||||||||
| Navarro et al., 2009 [40] | 1 | 1 | 1 | 1 | ||||||||||||
| Wang et al., 2013 [41] | 1 | 1 | 1 | 1 | 1 | 3 | ||||||||||
| TOTAL VALUES | 22 | 10 | 4 | 1 | 24 | 3 | 8 | 5 | 2 | 2 | 1 | 2 | 3 | 15 | ||
| Study | L2+ Languages | Proficiency Level | Age of acq. | Manner of acq. | Amount of Exposure | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L2 | L3 | L4 | L5 | High | Int. | Low | N/A | Early | Late | N/A | Form. | Inf. | N/A | Daily | Occ. | Rare | Never | N/A | |
| Połczyńska et al., 2017 [20] | 25 | 25 | 25 | 25 | 25 | ||||||||||||||
| Lucas et al., 2004 [9] | 22 | 17 | 5 | 22 | 22 | 22 | |||||||||||||
| Cheung et al., 2009 [21] * | 21 | 21 | 21 | 21 | 21 | ||||||||||||||
| Roux et al., 2004 [22] ** | 19 | 2 | 1 | 12 | 9 | 1 | 7 | 15 | 22 | 12 | 9 | 1 | |||||||
| Walker et al., 2004 [23] | 17 | 1 | 18 | 9 | 9 | 3 | 15 | 18 | |||||||||||
| Centeno et al., 2014 [24] | 16 | 5 | 6 | 5 | 5 | 11 | 16 | 16 | |||||||||||
| Roux & Trémoulet, 2002 [25] | 12 | 1 | 1 | 7 | 7 | 4 | 10 | 14 | 7 | 7 | |||||||||
| Fernández-Coello et al., 2017 [2] | 13 | 13 | 4 | 1 | 31 | 12 | 19 | 31 | 31 | ||||||||||
| Gao et al., 2015 [7] | 11 | 11 | 11 | 11 | 9 | 11 | |||||||||||||
| Sierpowska et al., 2018 [26] | 9 | 9 | 7 | 2 | 9 | 9 | |||||||||||||
| Bello et al., 2006 [4] | 7 | 7 | 5 | 2 | 21 | 21 | 21 | 21 | |||||||||||
| Rapport et al., 1983 [27] | 7 | 6 | 1 | 1 | 9 | 6 | 15 | 10 | 5 | 8 | 7 | ||||||||
| Borius et al., 2012 [28] | 7 | 7 | 2 | 5 | 7 | 7 | |||||||||||||
| Cervenka et al., 2011 [29] | 4 | 4 | 4 | 1 | 3 | 4 | |||||||||||||
| Ojemann & Whitaker, 1978 [3] | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||||||||||
| Sierpowska et al., 2013 [30] | 2 | 2 | 2 | 1 | 1 | 2 | |||||||||||||
| Kho et al., 2007 [31] | 2 | 1 | 1 | 2 | 1 | 1 | 2 | ||||||||||||
| Bilotta et al., 2011 [32] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Połczyńska et al., 2016 [33] | 1 | 1 | 1 | 3 | 3 | 3 | 1 | 1 | 1 | ||||||||||
| Kin et al., 2013 [34] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Pouratian et al., 2000 [19] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Serafini et al., 2008 [35] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| O’Grady et al., 2016 [36] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Gomez-Tortosa et al., 1995 [37] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Berthier et al., 1990 [38] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Lubrano et al., 2012 [39] | 1 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | |||||||||||
| Navarro et al., 2009 [40] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| Wang et al., 2013 [41] | 1 | 1 | 1 | 1 | 1 | ||||||||||||||
| TOTAL values (no. lang.) | 207 | 32 | 13 | 4 | 191 | 25 | 11 | 29 | 107 | 127 | 22 | 42 | 44 | 179 | 138 | 3 | 18 | 2 | 96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Połczyńska, M.M.; Bookheimer, S.Y. Factors Modifying the Amount of Neuroanatomical Overlap between Languages in Bilinguals—A Systematic Review of Neurosurgical Language Mapping Studies. Brain Sci. 2020, 10, 983. https://doi.org/10.3390/brainsci10120983
Połczyńska MM, Bookheimer SY. Factors Modifying the Amount of Neuroanatomical Overlap between Languages in Bilinguals—A Systematic Review of Neurosurgical Language Mapping Studies. Brain Sciences. 2020; 10(12):983. https://doi.org/10.3390/brainsci10120983
Chicago/Turabian StylePołczyńska, Monika M., and Susan Y. Bookheimer. 2020. "Factors Modifying the Amount of Neuroanatomical Overlap between Languages in Bilinguals—A Systematic Review of Neurosurgical Language Mapping Studies" Brain Sciences 10, no. 12: 983. https://doi.org/10.3390/brainsci10120983
APA StylePołczyńska, M. M., & Bookheimer, S. Y. (2020). Factors Modifying the Amount of Neuroanatomical Overlap between Languages in Bilinguals—A Systematic Review of Neurosurgical Language Mapping Studies. Brain Sciences, 10(12), 983. https://doi.org/10.3390/brainsci10120983