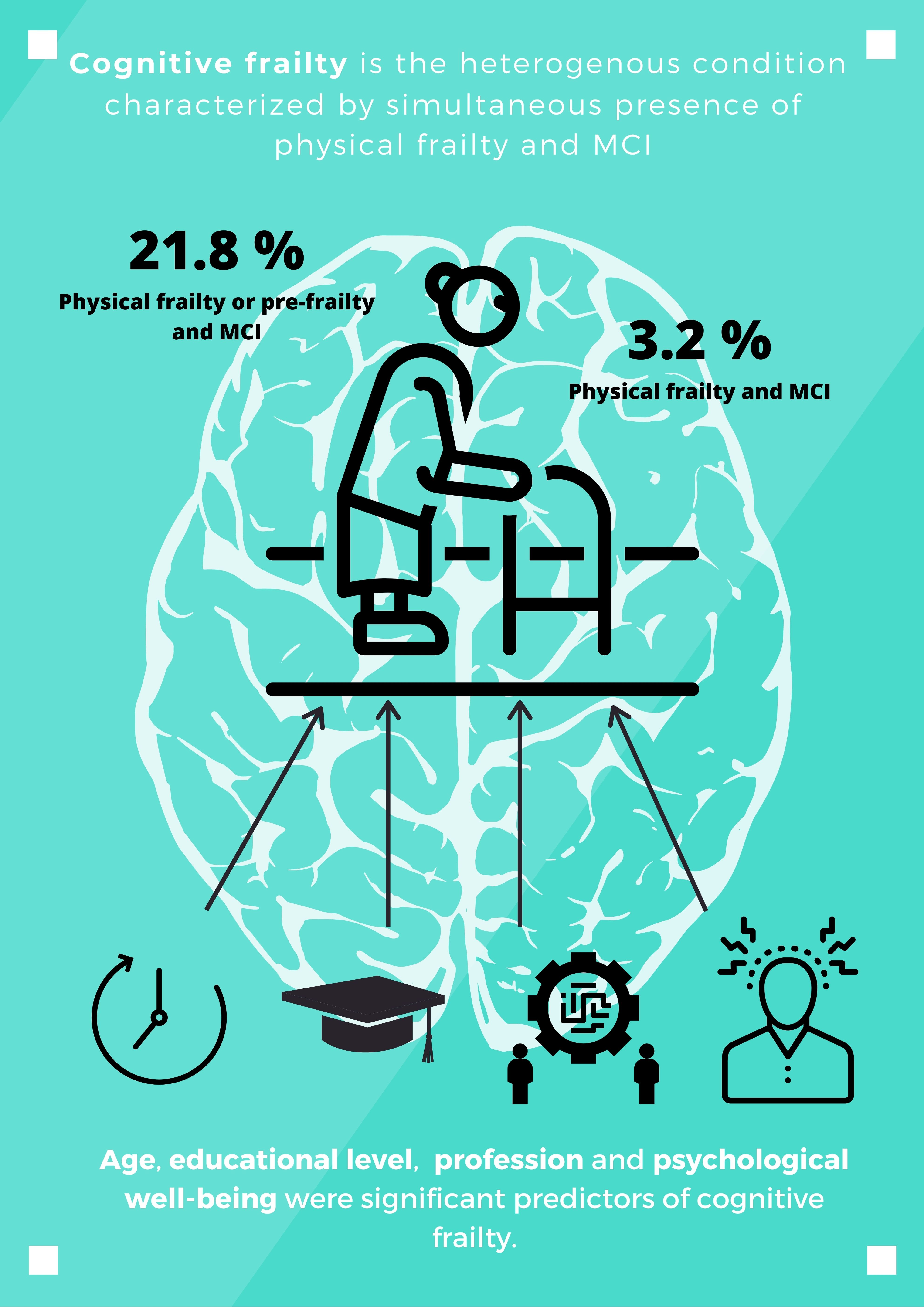
Prevalence of Cognitive Frailty, Do Psychosocial-Related Factors Matter?

 ,
,  ,
,  and
and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Study Design and Procedure
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Solfrizzi, V.; Frisardi, V.; Magg, S.; Sancarlo, D.; Adante, F.; D’Onofrio, G.; Seripa, D.; Pilotto, A. Different models of frailty in predementia and dementia syndromes. J. Nutr. Health Aging 2011, 15, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yu, Z.; Chen, M.; Chen, M.; Bao, Z.; Li, J.; He, W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res. Rev. 2015, 20, 1–10. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; Van Kan, G.A.; Ousset, P.-J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Fougère, B.; Daumas, M.; Lilamand, M.; Sourdet, S.; Delrieu, J.; Vellas, B.; Abellan van Kan, G. Association between frailty and cognitive impairment: Cross-sectional data from Toulouse frailty day hospital. J. Am. Med. Dir. Assoc. 2017, 18, 1–5. [Google Scholar] [CrossRef]
- Gale, C.; Ritchie, S.; Starr, J.; Deary, I.J. Physical frailty and decline in general and specific cognitive abilities: The Lothian Birth Cohort 1936. J. Epidemiol. Community Health 2020, 74, 108–113. [Google Scholar] [CrossRef]
- Ma, L.; Li Zhang, L.; Zhang, Y.; Li, Y.; Tang, Z.; Chan, P. Cognitive frailty in China: Results from China Comprehensive Geriatric Assessment Study. Front. Med. 2017, 4, 174. [Google Scholar] [CrossRef]
- Rivan, N.; Shahar, S.; Rajab, N.; Singh, D.; Che Din, N.; Mahadzir, H.; Sakian, N.I.M.; Ishak, W.S.; Rahman, M.H.A.; Mohammed, Z.; et al. Incidence and predictors of cognitive frailty among older adults: A community-based longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 1547. [Google Scholar] [CrossRef]
- Facal, D.; Maseda, A.; Pereiro, A.; Gandoy-Crego, M.; Lorenzo-López, L.; Yanguas, J.; Millán-Calente, J.C. Cognitive frailty: A conceptual systematic review and an operational proposal for future research. Maturitas 2019, 121, 48–56. [Google Scholar] [CrossRef]
- Jha, S.R.; Hannu, M.K.; Gore, K.; Chang, S.; Newton, P.; Wilhelm, K.; Hayward, C.S.; Jabbour, A.; Kotlyar, E.; Keogh, A.; et al. Cognitive impairment improves the predictive validity of physical frailty for mortality in patients with advanced heart failure referred for heart transplantation. J. Heart Lung Transplant 2016, 35, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.; Hwang, S.; Lee, D.; Lee, C.; Song, W. Physical frailty and cognitive functioning in Korea rural community-dwelling older adults. J. Clin. Med. 2018, 711, 405. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Lozupone, M.; Solfrizzi, V.; Sardone, R.; Dibello, V.; Di Lena, L.; D’Urso, F.; Stallone, R.; Petruzzi, M.; Giannelli, G.; et al. Different cognitive frailty models and health- and cognitive-related outcomes in older age: From epidemiology to prevention. J. Alzheimers Dis. 2018, 62, 993–1012. [Google Scholar] [CrossRef] [PubMed]
- Roppolo, M.; Mulasso, A.; Rabaglietti, E. Cognitive frailty in Italian community-dwelling older adults: Prevalence rate and its association with disability. J. Nutr. Health Aging 2017, 21, 631–636. [Google Scholar] [CrossRef]
- Kim, H.; Awata, S.; Watanabe, Y.; Kojima, N.; Osuka, Y.; Motokawa, K.; Sakuma, N.; Inagaki, H.; Edahiro, A.; Hosoi, E.; et al. Cognitive frailty in community-dwelling older Japanese people: Prevalence and its association with falls. Geriatr. Gerontol. Int. 2019, 19, 647–653. [Google Scholar] [CrossRef]
- Ruan, Q.; Xiao, F.; Gong, K.; Zhang, W.; Zhang, M.; Ruan, J.; Zhang, X.; Chen, Q.; Yu, Z. Prevalence of cognitive frailty phenotypes and associated factors in a community-dwelling elderly population. J. Nutr. Health Aging 2020, 24, 172–180. [Google Scholar] [CrossRef]
- Gutierrez-Robledo, L.; Avila-Funes, J. How to include the social factor for determining frailty? J. Frailty Aging 2012, 1, 13–17. [Google Scholar]
- Lang, P.; Michel, J.; Zekry, D. Frailty syndrome: A transitional state in a dynamic process. Gerontology 2009, 55, 539–549. [Google Scholar] [CrossRef]
- Casale-Martínez, R.; Navarrete-Reyes, A.; Avila-Funes, J. Social determinants of frailty in elderly Mexican community-dwelling adults. J. Am. Geriatr. Soc. 2012, 60, 800–802. [Google Scholar] [CrossRef]
- Andrew, M.; Rockwood, K. Psychiatric illness in relation to frailty in community-dwelling elderly people without dementia: A report from Canadian Study of Health and Aging. Can. J. Aging 2007, 26, 33–38. [Google Scholar] [CrossRef]
- Blaum, C.; Xue, Q.; Michelon, E.; Semba, R.; Fried, L. The association between obesity and the frailty syndrome in older women: The Women’s Health and Aging Studies. J. Am. Geriatr. Soc. 2005, 53, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Rocha, K.; Pérez, K.; Rodríguez-Sanz, M.; Borrell, C.; Obiols, J. Propiedades psicométricas y valores normativos del General Health Questionnaire (GHQ-12) en población general española. Int. J. Clin. Health Psychol. 2011, 11, 125–139. [Google Scholar]
- Goldberg, D. General Health Questionnaire (GHQ-12); NFER-Nelson: Windsor, UK, 1992. [Google Scholar]
- Revilla, L.; Luna, J.; Bailón, E.; Medina, I. Validación del cuestionario MOS de apoyo social en Atencion Primaria. Med. Fam. 2005, 1, 10–18. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Ruiz, A.; Pera, G.; Baena, J.M.; Mundet, X.; Alzamora, T.; Elosua, R.; Torán, P.; Heras, A.; Forés, R.; Fuesté, M.; et al. Validation of a Spanish Short Version of the Minnesota Leisure Time Physical Activity Questionnaire (VREM). Rev. Esp. Salud Pública 2012, 86, 495–508. [Google Scholar]
- Pereiro-Rozas, A.; Ramos-Lema, S.; Lojo-Seoane, C.; Guàrdia-Olmos, J.; Facal-Mayo, D.; Juncos-Rabadán, O. Correction to: Normative data for the Montreal Cognitive Assessment (MOCA) in a Spanish sample of community-dweller adults. Eur. Geriatr. Med. 2018, 9, 903–904. [Google Scholar] [CrossRef]
- Alley, D.E.; Shardell, M.D.; Peters, K.W.; McLean, R.R.; Dam, T.T.; Fragala, M.S.; Cawton, P.M. Grip strength cutpoints for the identification of clinically relevant weakness. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 559–566. [Google Scholar] [CrossRef]
- Pereiro, A.X.; Campos-Magdaleno, M.; Navarro-Pardo, E.; Juncos-Rabadán, O.; Facal, D. Datos normativos para el test Timed-Up & Go en una muestra de adultos a partir de 50 años. Aten Primaria 2020, in press. [Google Scholar]
- Pérez Díaz, J.; Abellán García, A.; Aceituno Nieto, P.; Ramiro Fariñas, D. Un perfil de las personas mayores en España, 2020. Indicadores estadísticos básicos. Inf. Envejec. Red 2020, 25, 39. [Google Scholar]
- Caffò, A.O.; Lopez, A.; Spano, G.; Saracino, G.; Stasolla, F.; Ciriello, G.; Bosco, A. The role of pre-morbid intelligence and cognitive reserve in predicting cognitive efficiency in a sample of Italian elderly. Aging Clin. Exp. Res. 2016, 28, 1203–1210. [Google Scholar] [CrossRef]
- Darwish, H.; Farran, N.; Assaad, S.; Chaaya, M. Cognitive reserve factors in a developing country: Education and occupational attainment lower the risk of dementia in a sample of lebanese older adults. Front. Aging Neurosci. 2018, 10, 277. [Google Scholar] [CrossRef] [PubMed]
- Facal, D.; Valladares-Rodriguez, S.; Lojo-Seoane, C.; Pereiro, A.X.; Anido-Rifon, L.; Juncos-Rabadán, O. Machine learning approaches to studying the role of cognitive reserve in conversion from mild cognitive impairment to dementia. Int. J. Geriatr. Psychiatry 2019, 34, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Kazama, M.; Kondo, N.; Suzuki, K.; Minai, J.; Imai, H.; Yamagata, Z. Early impact of depression symptoms on the decline in activities of daily living among older Japanese: Y-HALE cohort study. Environ. Health Prev. Med. 2011, 16, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Rondon, L.; Aguirre, B.; Garcia, F.; Gallego, C. Support and social contact as a decisive meta-variable in morbidity and social welfare of the older person. Curr. Aging Sci. 2017, 10, 282–290. [Google Scholar]
- Fernández Alonso, M. Social support networks in Spain: The factors that determine models of choice. Int. Sociol. 2012, 27, 384–402. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Characteristics | Frequencies (%) |
|---|---|
| Age groups | |
| 60–64 years | 56 (19.6%) |
| 65–69 years | 58 (20.4%) |
| 70–74 years | 57 (20.0%) |
| 75–79 years | 53 (18.6%) |
| 80 + years | 61 (21.4%) |
| Gender | |
| Men | 132 (46.3%) |
| Women | 153 (53.7%) |
| Formal education | |
| Low educ. level | 137 (51.7%) |
| High educ. level | 128 (48.3%) |
| Profession | |
| Low qualification | 161 (56.5%) |
| High qualification | 124 (43.5%) |
| Comorbidity | |
| No chronic conditions | 180 (63.2%) |
| One chronic condition | 74 (26.0%) |
| Two or more chronic conditions | 31 (10.9%) |
| Cognitive and frailty status | |
| Non-frail-cognitively unimpaired | 80 (28.1%) |
| Pre-frail-cognitively unimpaired | 109 (38.2%) |
| Frail-cognitively unimpaired | 14 (4.9%) |
| Non-frail-cognitive impairment | 20 (7.0%) |
| Pre-frail-cognitive impairment | 53 (18.6%) |
| Frail-possible cognitive impairment | 9 (3.2%) |
| Social support and psychological well-being | |
| Social support status | |
| With social support | 266 (93.3%) |
| Without social support | 19 (6.7%) |
| Psychological well-being | |
| High well-being | 237 (83.2%) |
| Low well-being | 48 (16.8%) |
| Covariates | Cases | % | Wald’s | p-Values | OR | 95% CI |
|---|---|---|---|---|---|---|
| Age group | ||||||
| 60–64 | 7/53 | 13.2 | 1 | |||
| 65–69 | 7/54 | 13 | 0.01 | 0.97 | 0.98 | 0.32–3.01 |
| 70–74 | 14/52 | 26.9 | 2.98 | 0.084 | 2.42 | 0.89–6.61 |
| 75–79 | 9/49 | 18.4 | 0.51 | 0.476 | 1.48 | 0.51–4.33 |
| 80+ | 25/57 | 43.9 | 11.35 | 0.001 | 5.13 | 1.98–13.30 |
| Gender | ||||||
| Men | 22/123 | 17.9 | 1 | |||
| Women | 40/142 | 28.2 | 3.83 | 0.050 | 0.55 | 0.31–1.00 |
| Formal education | ||||||
| Low educ. level | 49/137 | 35.8 | 21.66 | 0.001 | 4.93 | 2.52–9.64 |
| High educ. level | 13/128 | 10.2 | 1 | |||
| Profession | ||||||
| Low qualification | 47/146 | 32.2 | 13.18 | <0.001 | 3.29 | 1.70–6.26 |
| High qualification | 15/119 | 12.6 | 1 | |||
| Comorbidity | ||||||
| No conditions | 38/161 | 23.6 | 1 | |||
| One condition | 17/74 | 23.0 | 0.001 | 0.975 | 1.02 | 0.40–2.55 |
| Two or more cond. | 7/30 | 23.3 | 0.002 | 0.968 | 0.98 | 0.36–2.68 |
| Social support | ||||||
| With support | 58/247 | 23.5 | 1 | |||
| Without support | 4/18 | 22.2 | 0.015 | 0.903 | 1.07 | 0.34–3.39 |
| Psychological well-being | ||||||
| Low well-being | 19/48 | 39.6 | 8.19 | 0.01 | 2.65 | 1.36–5.17 |
| High well-being | 43/217 | 19.8 | 1 |
| Covariates | B | S.E. | Wald’s | p-Values | OR | 95% CI |
|---|---|---|---|---|---|---|
| Age group | ||||||
| 60–64 | 1 | |||||
| 65–69 | −0.20 | 0.61 | 0.11 | 0.74 | 0.99 | 0.31–3.15 |
| 70–74 | 0.56 | 0.55 | 1.04 | 0.31 | 2.10 | 0.74–5.96 |
| 75–79 | −0.16 | 0.59 | 0.08 | 0.78 | 1.21 | 0.40–3.67 |
| 80+ | 1.00 | 0.53 | 6.28 | 0.05 | 4.24 | 1.57–11.44 |
| Formal education | ||||||
| Low | 1.23 | 0.38 | 10.59 | 0.01 | 3.43 | 1.63–7.21 |
| High | 1 | |||||
| Profession | ||||||
| Low qualification | 0.94 | 0.38 | 6.28 | 0.001 | 2.56 | 0.97–7.70 |
| High qualification | 1 | |||||
| Psychol. well-being | ||||||
| No problems | 1 | |||||
| Mental health problems | 1.08 | 0.40 | 7.43 | 0.001 | 2.94 | 1.35–6.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Pardo, E.; Facal, D.; Campos-Magdaleno, M.; Pereiro, A.X.; Juncos-Rabadán, O. Prevalence of Cognitive Frailty, Do Psychosocial-Related Factors Matter? Brain Sci. 2020, 10, 968. https://doi.org/10.3390/brainsci10120968
Navarro-Pardo E, Facal D, Campos-Magdaleno M, Pereiro AX, Juncos-Rabadán O. Prevalence of Cognitive Frailty, Do Psychosocial-Related Factors Matter? Brain Sciences. 2020; 10(12):968. https://doi.org/10.3390/brainsci10120968
Chicago/Turabian StyleNavarro-Pardo, Esperanza, David Facal, María Campos-Magdaleno, Arturo X. Pereiro, and Onésimo Juncos-Rabadán. 2020. "Prevalence of Cognitive Frailty, Do Psychosocial-Related Factors Matter?" Brain Sciences 10, no. 12: 968. https://doi.org/10.3390/brainsci10120968
APA StyleNavarro-Pardo, E., Facal, D., Campos-Magdaleno, M., Pereiro, A. X., & Juncos-Rabadán, O. (2020). Prevalence of Cognitive Frailty, Do Psychosocial-Related Factors Matter? Brain Sciences, 10(12), 968. https://doi.org/10.3390/brainsci10120968