Analysis of a Customized Clutch Joint Designed for the Safety Management of an Ultrasound Robot

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
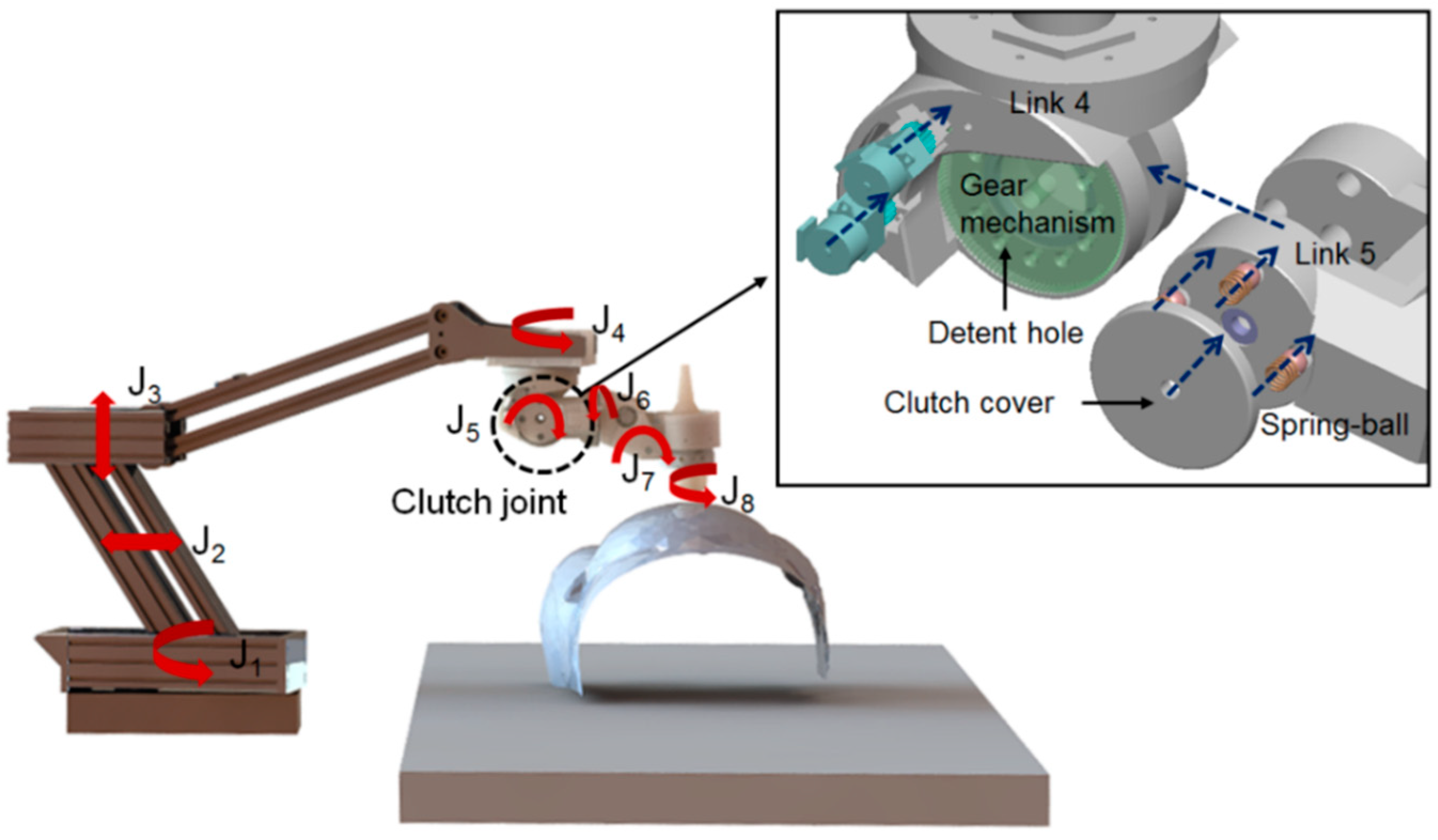
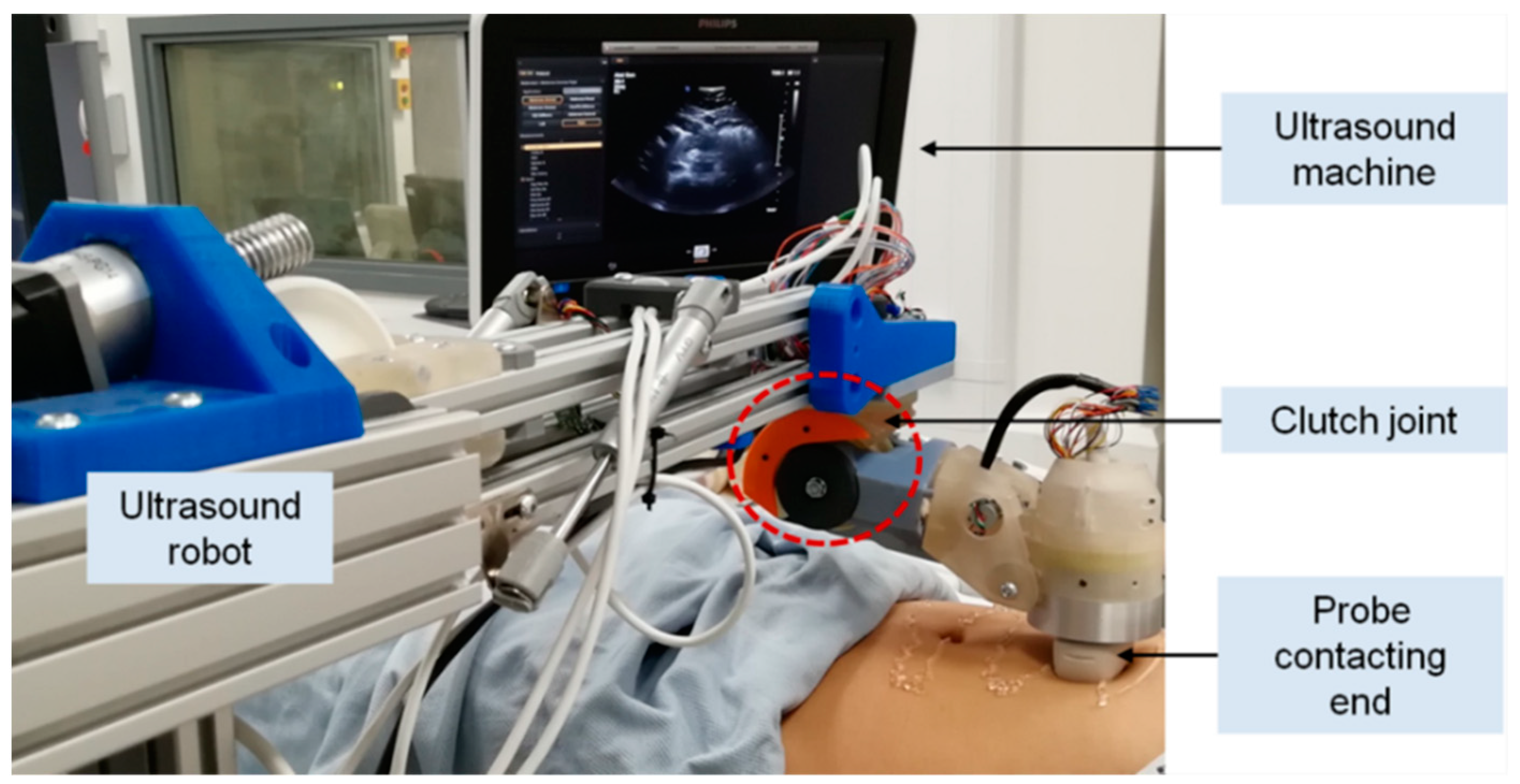
2.1. System Overview
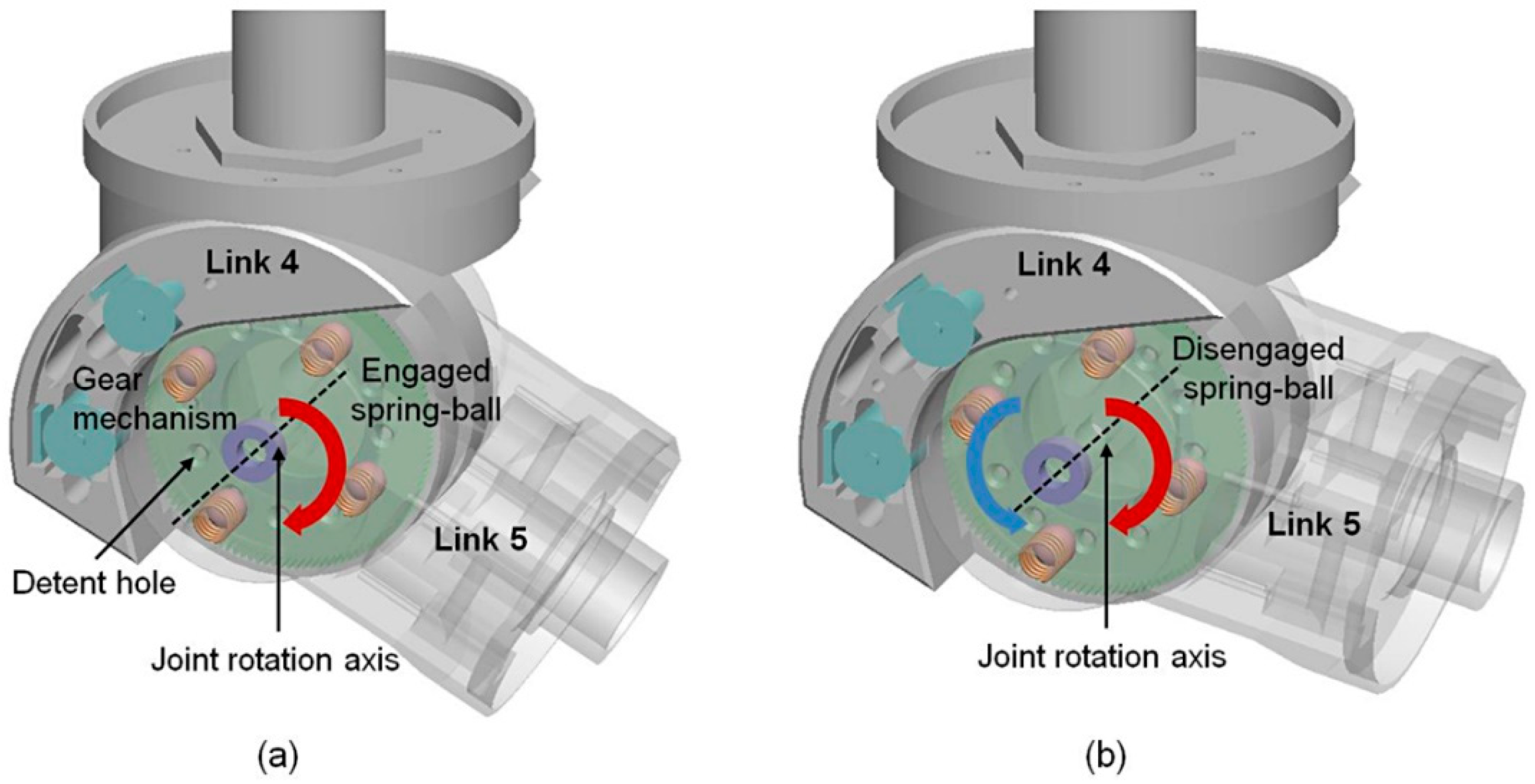
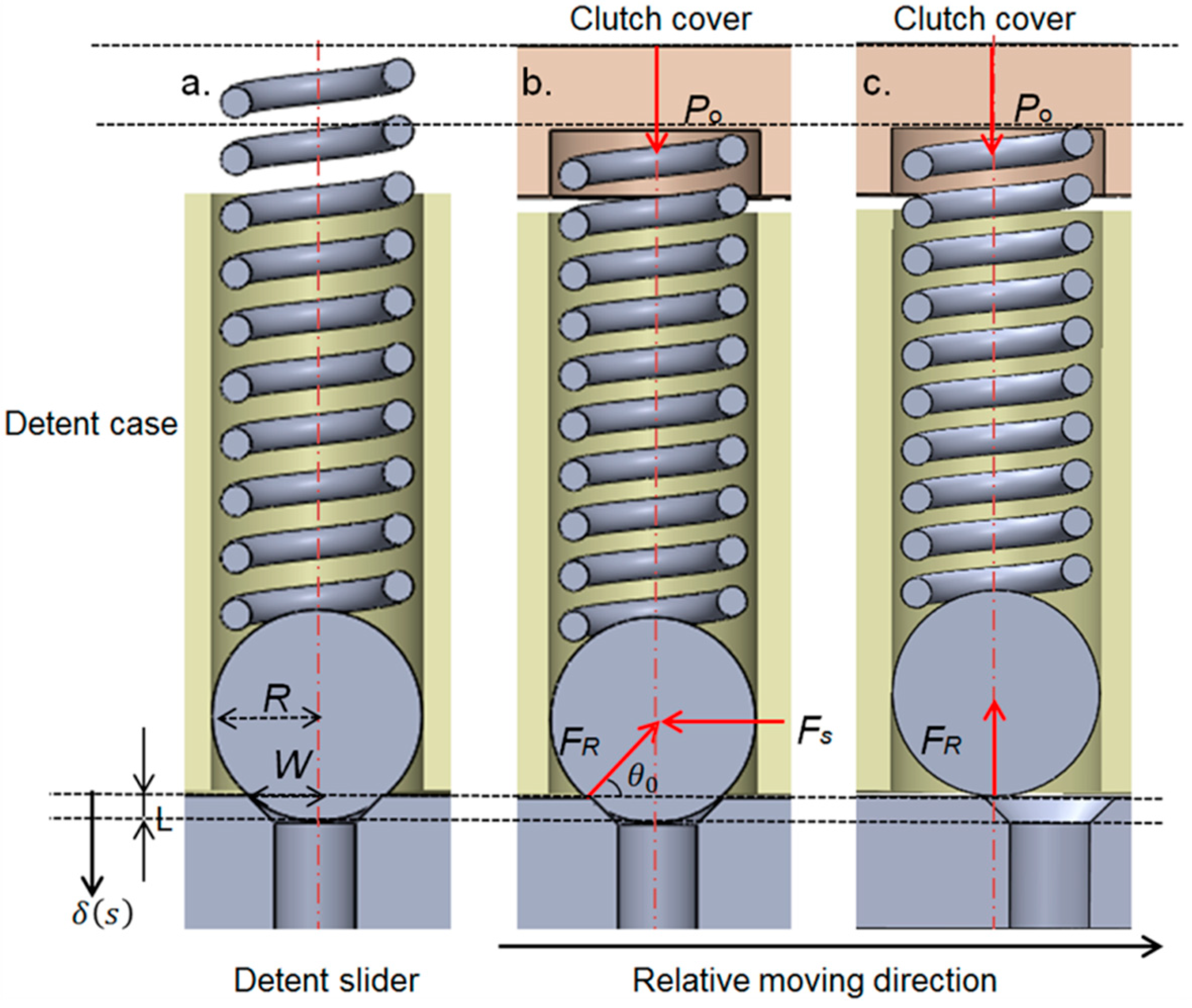
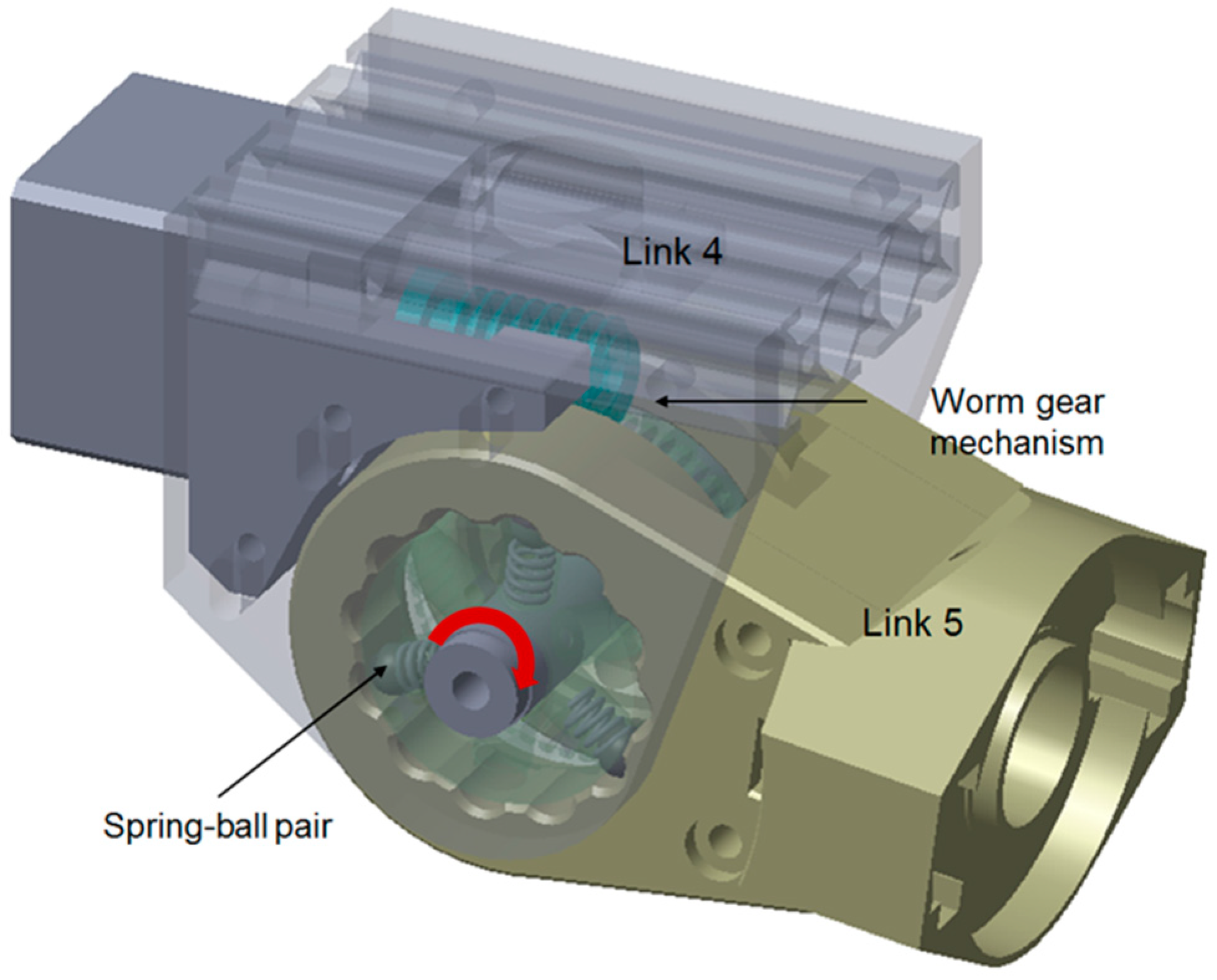
2.2. Customized Spring-Loaded Ball Clutch
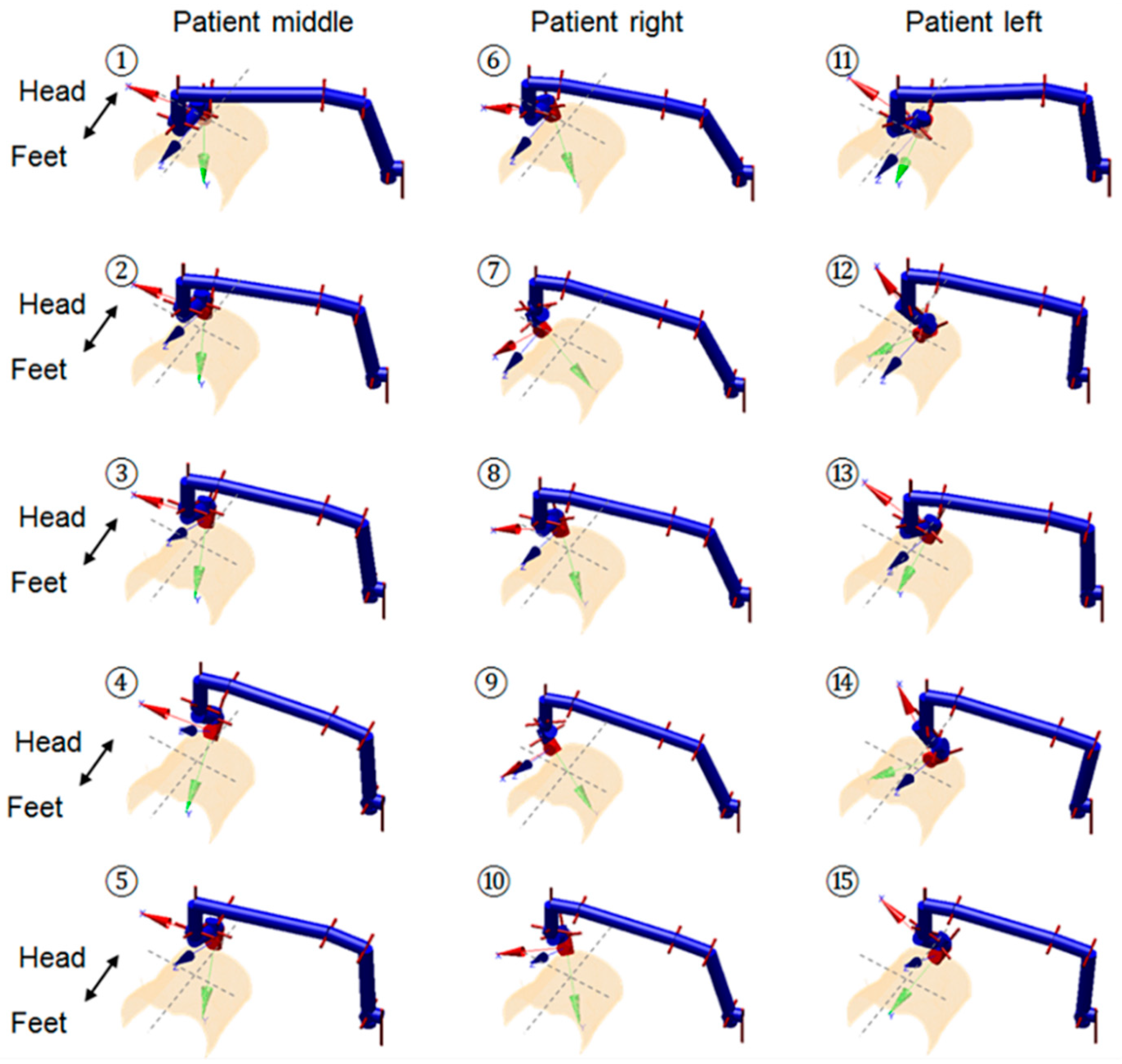
2.3. Kinematic-Based Performance Analysis
3. Results and Discussion
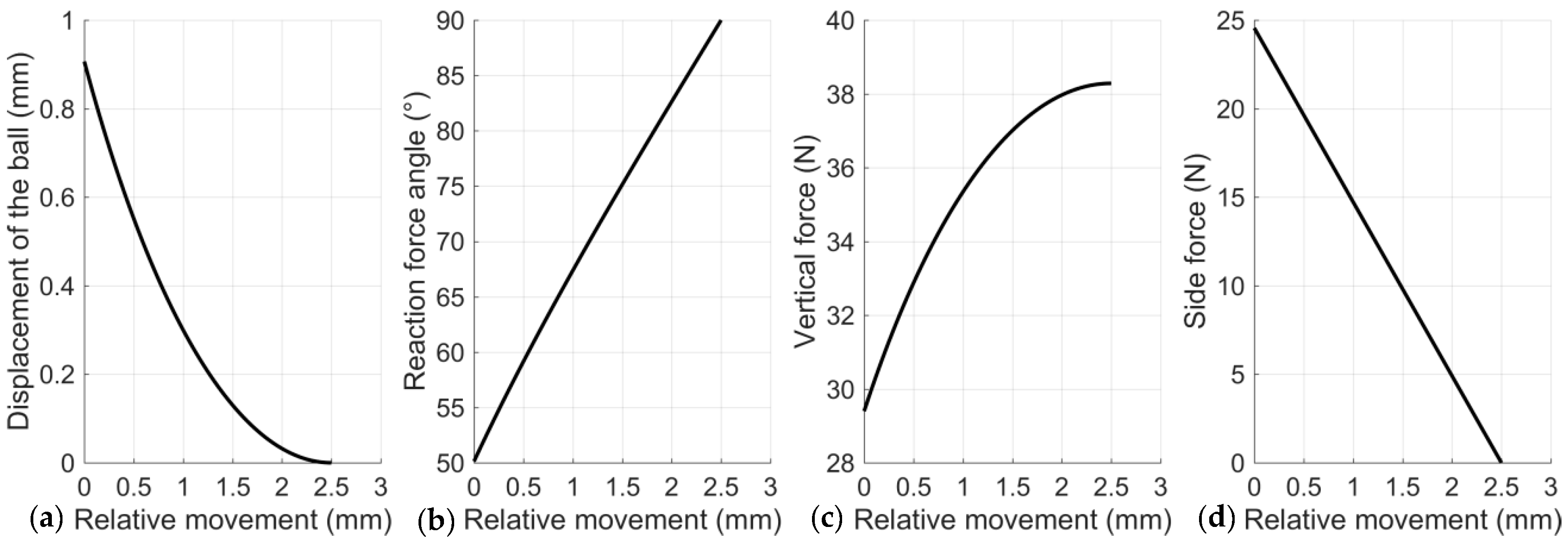
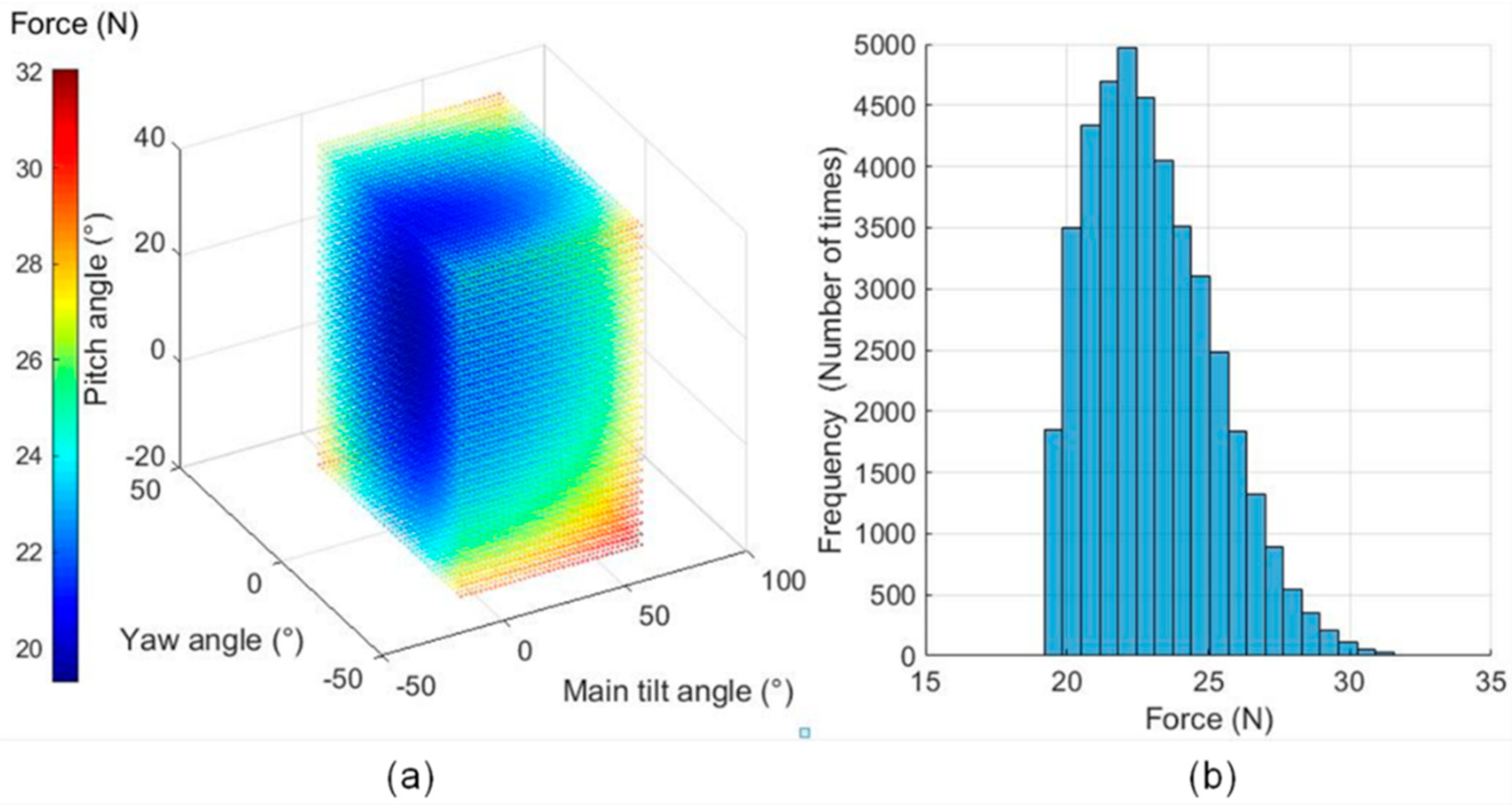
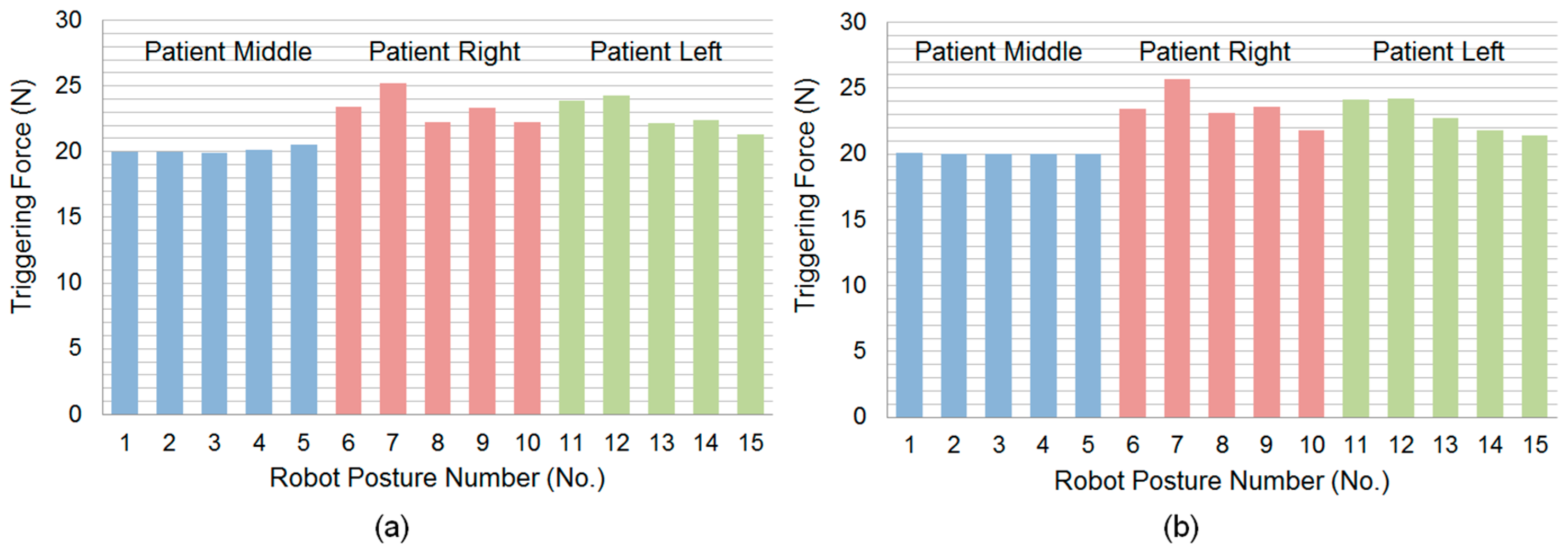
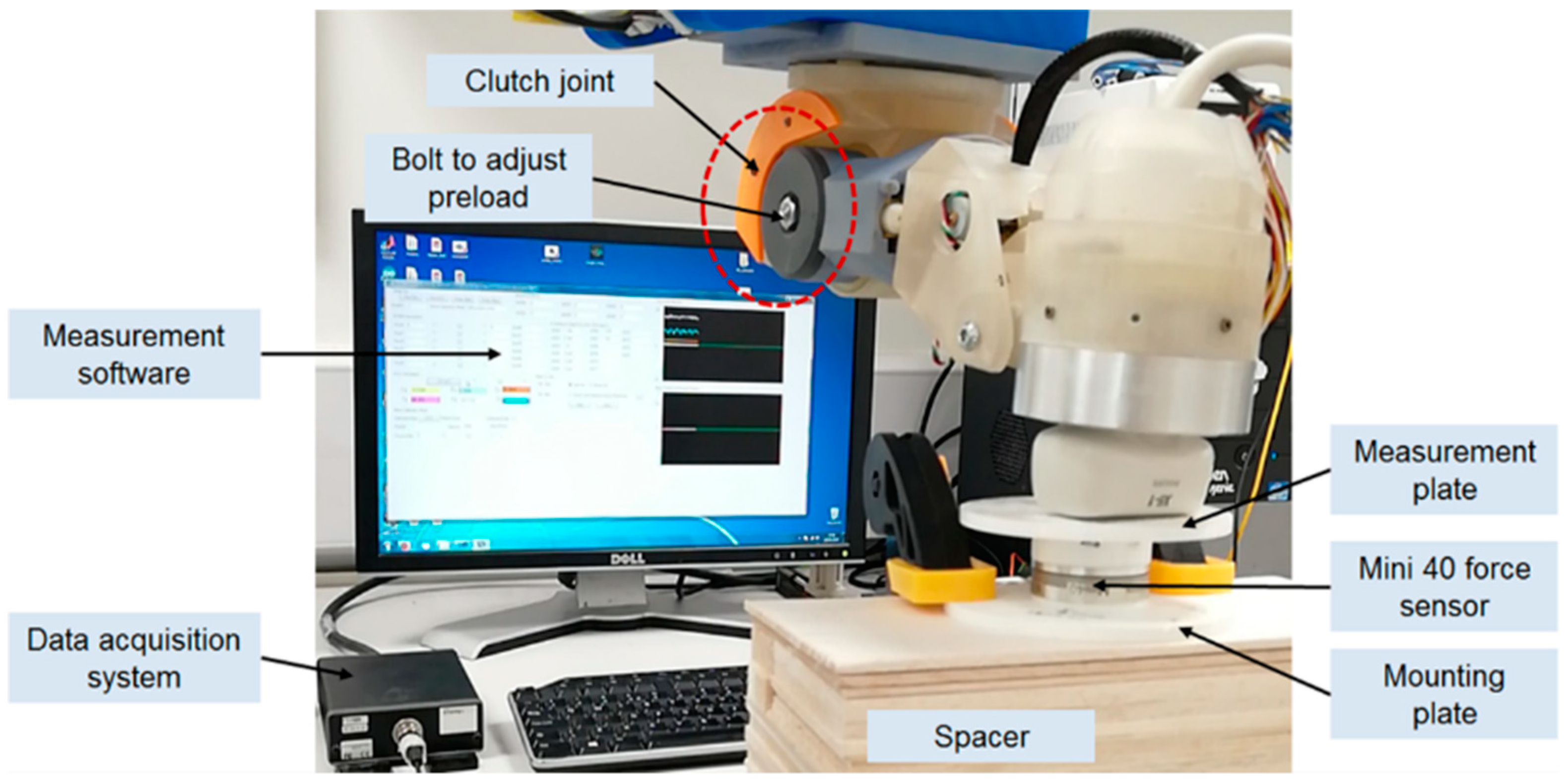
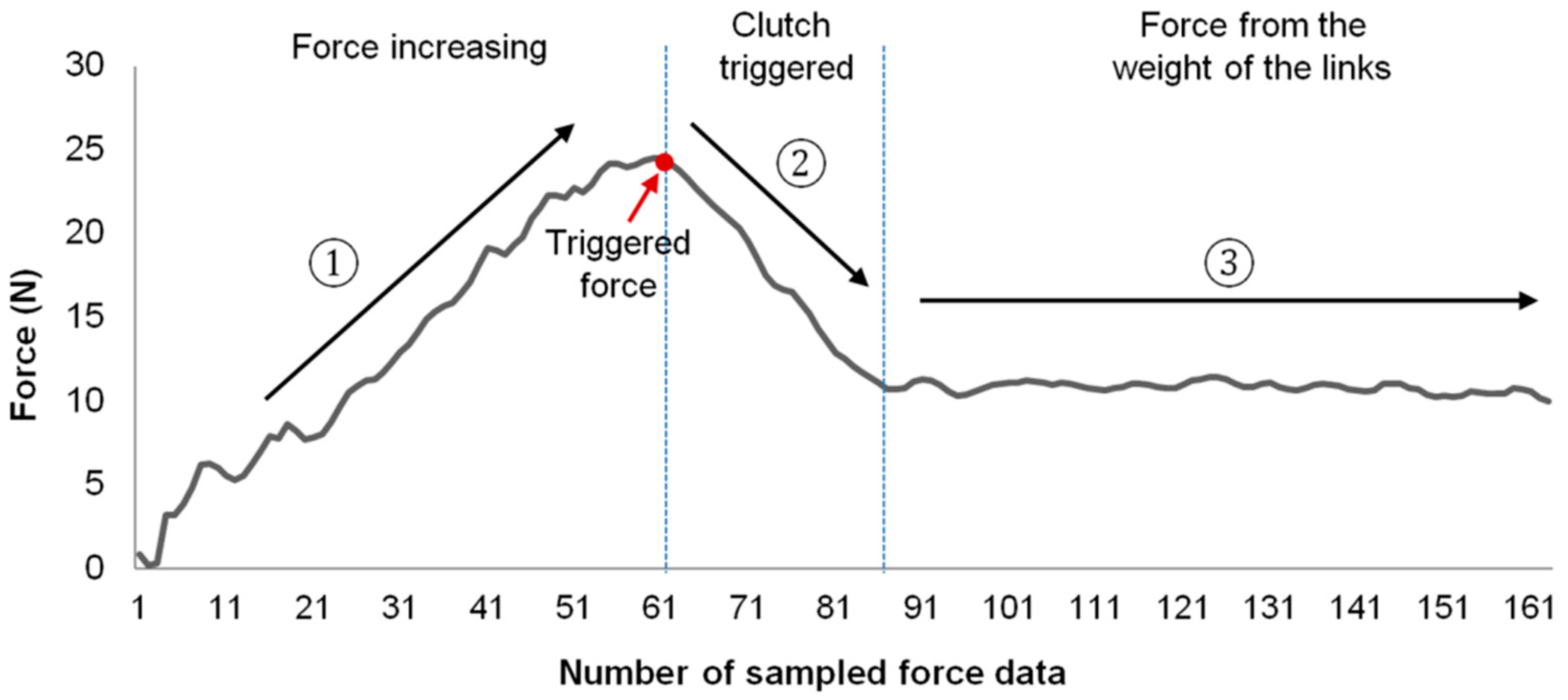
3.1. Clutch Performance
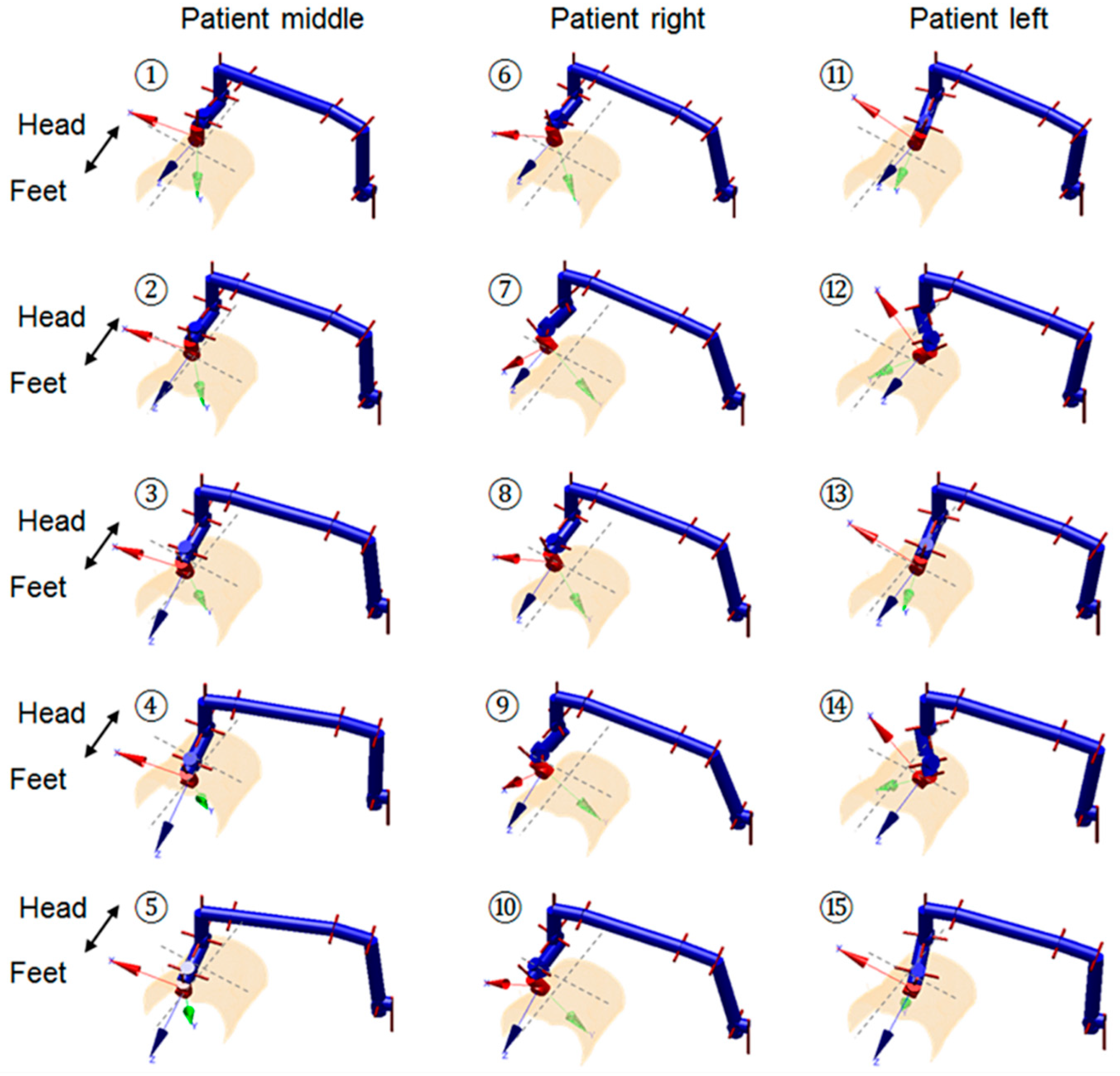
3.2. Implementation and Practical Experiments
3.3. Design Variation
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- LaGrone, L.N.; Sadasivam, V.; Kushner, A.L.; Groen, R.S. A review of training opportunities for ultrasonography in low and middle income countries. Trop. Med. Int. Health 2012, 17, 808–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Bellows, B.A.; Adedipe, A.A.; Totten, J.E.; Backlund, B.H.; Sajed, D. Perceived barriers in the use of ultrasound in developing countries. Crit. Ultrasound J. 2015, 7, 11. [Google Scholar] [CrossRef]
- Magnavita, N.; Bevilacqua, L.; Mirk, P.; Fileni, A.; Castellino, N. Work-related musculoskeletal complaints in sonologists. J. Occup. Environ. Med. 1999, 41, 981–988. [Google Scholar] [CrossRef]
- Brown, G. Work related musculoskeletal disorders in sonographers. BMUS Bull. 2003, 11, 6–13. [Google Scholar] [CrossRef]
- Antico, M.; Sasazawa, F.; Wu, L.; Jaiprakash, A.; Roberts, J.; Crawford, R.; Pandey, A.K.; Fontanarosa, D. Ultrasound guidance in minimally invasive robotic procedures. Med. Image Anal. 2019, 54, 149–167. [Google Scholar] [CrossRef] [PubMed]
- Priester, A.M.; Natarajan, S.; Culjat, M.O. Robotic ultrasound systems in medicine. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 507–523. [Google Scholar] [CrossRef]
- Swerdlow, D.R.; Cleary, K.; Wilson, E.; Azizi-Koutenaei, B.; Monfaredi, R. Robotic arm–assisted sonography: Review of technical developments and potential clinical applications. Am. J. Roentgenol. 2017, 208, 733–738. [Google Scholar] [CrossRef]
- Vilchis Gonzales, A.; Cinquin, P.; Troccaz, J.; Guerraz, A.; Hennion, B.; Pellissier, F.; Thorel, P.; Courreges, F.; Gourdon, A.; Poisson, G. Ter: A system for robotic tele-echography. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI, Utrecht, The Netherlands, 14–17 October 2001; Springer: Heidelberg, Germany, 2001; pp. 326–334. [Google Scholar]
- Vilchis, A.; Troccaz, J.; Cinquin, P.; Guerraz, A.; Pellisier, F.; Thorel, P.; Tondu, B.; Courrèges, F.; Poisson, G.; Althuser, M. Experiments with the ter tele-echography robot. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI, Tokyo, Japan, 25–28 September 2002; Springer: Heidelberg, Germany, 2002; pp. 138–146. [Google Scholar]
- Vilchis, A.; Troccaz, J.; Cinquin, P.; Masuda, K.; Pellissier, F. A new robot architecture for tele-echography. IEEE Trans. Robot. Autom. 2003, 19, 922–926. [Google Scholar] [CrossRef] [Green Version]
- Gourdon, A.; Poignet, P.; Poisson, G.; Vieyres, P.; Marche, P. A new robotic mechanism for medical application. In Proceedings of the International Conference on Advanced Intelligent Mechatronics 1999 IEEE/ASME, Atlanta, GA, USA, 19–23 September 1999; pp. 33–38. [Google Scholar]
- Arbeille, P.; Poisson, G.; Vieyres, P.; Ayoub, J.; Porcher, M.; Boulay, J.L. Echographic examination in isolated sites controlled from an expert center using a 2-d echograph guided by a teleoperated robotic arm. Ultrasound Med. Biol. 2003, 29, 993–1000. [Google Scholar] [CrossRef]
- Arbeille, P.; Ruiz, J.; Herve, P.; Chevillot, M.; Poisson, G.; Perrotin, F. Fetal tele-echography using a robotic arm and a satellite link. Ultrasound Obstet. Gynecol. 2005, 26, 221–226. [Google Scholar] [CrossRef] [Green Version]
- Arbeille, P.; Capri, A.; Ayoub, J.; Kieffer, V.; Georgescu, M.; Poisson, G. Use of a robotic arm to perform remote abdominal telesonography. Am. J. Roentgenol. 2007, 188, W317–CW322. [Google Scholar] [CrossRef]
- Salcudean, S.; Bell, G.; Bachmann, S.; Zhu, W.-H.; Abolmaesumi, P.; Lawrence, P.D. Robot-assisted diagnostic ultrasound–design and feasibility experiments. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI, Cambridge, UK, 19–22 September 1999; Springer: Heidelberg, Germany, 1999; pp. 1062–1071. [Google Scholar]
- Salcudean, S.E.; Bell, G.S.; Lawrence, P.D.; Marko, A.; Jameson, M. Robotically Assisted Medical Ultrasound. U.S. Patent No. 6,425,865, 30 July 2002. [Google Scholar]
- Abolmaesumi, P.; Sirouspour, M.R.; Salcudean, S. Real-time extraction of carotid artery contours from ultrasound images. In Proceedings of the 13th IEEE Symposium on Computer-Based Medical Systems, CBMS 2000, Houston, TX, USA, 24 June 2000; pp. 181–186. [Google Scholar]
- Abolmaesumi, P.; Salcudean, S.; Zhu, W. Visual servoing for robot-assisted diagnostic ultrasound, engineering in medicine and biology society, 2000. In Proceedings of the 22nd Annual International Conference of the IEEE, Chicago, IL, USA, 23–28 July 2000; pp. 2532–2535. [Google Scholar]
- Abolmaesumi, P.; Salcudean, S.E.; Zhu, W.-H.; Sirouspour, M.R.; DiMaio, S.P. Image-guided control of a robot for medical ultrasound. IEEE Trans. Robot. Autom. 2002, 18, 11–23. [Google Scholar] [CrossRef]
- Ma, Y.; Penney, G.P.; Bos, D.; Frissen, P.; De Fockert, G.; Yao, C.; King, A.; Gao, G.; Rinaldi, C.A.; Razavi, R. Using a robotic arm for echocardiography to x-Ray image registration during cardiac catheterization procedures. In Proceedings of the Cardiovascular Interventional Imaging and Biophysical Modelling CI2BM09-MICCAI Workshop, London, UK, 20 September 2009; p. 8. [Google Scholar]
- Janvier, M.-A.; Soulez, G.; Allard, L.; Cloutier, G. Validation of 3d reconstructions of a mimicked femoral artery with an ultrasound imaging robotic system. Med. Phys. 2010, 37, 3868–3879. [Google Scholar] [CrossRef]
- Koizumi, N.; Warisawa, S.I.; Nagoshi, M.; Hashizume, H.; Mitsuishi, M. Construction methodology for a remote ultrasound diagnostic system. IEEE Trans. Robot. 2009, 25, 522–538. [Google Scholar] [CrossRef]
- Mathiassen, K.; Fjellin, J.E.; Glette, K.; Hol, P.K.; Elle, O.J. An ultrasound robotic system using the commercial robot ur5. Front. Robot. AI 2016, 3, 1. [Google Scholar] [CrossRef]
- Fang, T.-Y.; Zhang, H.K.; Finocchi, R.; Taylor, R.H.; Boctor, E.M. Force-assisted ultrasound imaging system through dual force sensing and admittance robot control. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.K.; Cheng, A.; Bottenus, N.; Guo, X.; Trahey, G.E.; Boctor, E.M. Synthetic tracked aperture ultrasound imaging: Design, simulation, and experimental evaluation. J. Med. Imaging 2016, 3, 027001. [Google Scholar] [CrossRef]
- Şen, H.T.; Cheng, A.; Ding, K.; Boctor, E.; Wong, J.; Iordachita, I.; Kazanzides, P. Cooperative control with ultrasound guidance for radiation therapy. Front. Robot. AI 2016, 3, 49. [Google Scholar] [CrossRef]
- Hennersperger, C.; Fuerst, B.; Virga, S.; Zettinig, O.; Frisch, B.; Neff, T.; Navab, N. Towards mri-based autonomous robotic us acquisitions: A first feasibility study. IEEE Trans. Med. Imaging 2017, 36, 538–548. [Google Scholar] [CrossRef]
- Essomba, T.; Nouaille, L.; Laribi, M.A.; Poisson, G.; Zeghloul, S. Design process of a robotized tele-echography system. In Applied Mechanics and Materials; Trans Tech Publications: Zurich, Switzerland, 2012; pp. 384–393. [Google Scholar]
- Smith-Guerin, N.; Al Bassit, L.; Poisson, G.; Delgorge, C.; Arbeille, P.; Vieyres, P. Clinical validation of a mobile patient-expert tele-echography system using isdn lines. In Proceedings of the 4th International IEEE EMBS Special Topic Conference on Information Technology Applications in Biomedicine, Birmingham, UK, 18 August 2003; pp. 23–26. [Google Scholar]
- Virga, S.; Zettinig, O.; Esposito, M.; Pfister, K.; Frisch, B.; Neff, T.; Navab, N.; Hennersperger, C. Automatic force-compliant robotic ultrasound screening of abdominal aortic aneurysms. In Proceedings of the International Conference on Intelligent Robots and Systems (IROS), Daejeon, Japan, 9–14 October 2016; pp. 508–513. [Google Scholar]
- Dhyani, M.; Roll, S.C.; Gilbertson, M.W.; Orlowski, M.; Anvari, A.; Li, Q.; Anthony, B.; Samir, A.E. A pilot study to precisely quantify forces applied by sonographers while scanning: A step toward reducing ergonomic injury. Work 2017, 58, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Housden, J.; Noh, Y.; Singh, A.; Back, J.; Lindenroth, L.; Liu, H.; Hajnal, J.; Althoefer, K.; Singh, D.; et al. Design and implementation of a bespoke robotic manipulator for extra-corporeal ultrasound. JoVE 2019, e58811. [Google Scholar] [CrossRef]
- Wang, S.; Housden, J.; Noh, Y.; Singh, D.; Singh, A.; Skelton, E.; Matthew, J.; Tan, C.; Back, J.; Lindenroth, L. Robotic-assisted ultrasound for fetal imaging: Evolution from single-arm to dual-arm system. arXiv 2019, arXiv:1902.05458. [Google Scholar]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.; Housden, R.J.; Noh, Y.; Singh, A.; Lindenroth, L.; Liu, H.; Althoefer, K.; Hajnal, J.; Singh, D.; Rhode, K. Analysis of a Customized Clutch Joint Designed for the Safety Management of an Ultrasound Robot. Appl. Sci. 2019, 9, 1900. https://doi.org/10.3390/app9091900
Wang S, Housden RJ, Noh Y, Singh A, Lindenroth L, Liu H, Althoefer K, Hajnal J, Singh D, Rhode K. Analysis of a Customized Clutch Joint Designed for the Safety Management of an Ultrasound Robot. Applied Sciences. 2019; 9(9):1900. https://doi.org/10.3390/app9091900
Chicago/Turabian StyleWang, Shuangyi, Richard James Housden, Yohan Noh, Anisha Singh, Lukas Lindenroth, Hongbin Liu, Kaspar Althoefer, Joseph Hajnal, Davinder Singh, and Kawal Rhode. 2019. "Analysis of a Customized Clutch Joint Designed for the Safety Management of an Ultrasound Robot" Applied Sciences 9, no. 9: 1900. https://doi.org/10.3390/app9091900
APA StyleWang, S., Housden, R. J., Noh, Y., Singh, A., Lindenroth, L., Liu, H., Althoefer, K., Hajnal, J., Singh, D., & Rhode, K. (2019). Analysis of a Customized Clutch Joint Designed for the Safety Management of an Ultrasound Robot. Applied Sciences, 9(9), 1900. https://doi.org/10.3390/app9091900