CT Conversion Workflow for Intraoperative Usage of Bony Models: From DICOM Data to 3D Printed Models

 , ,
, ,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
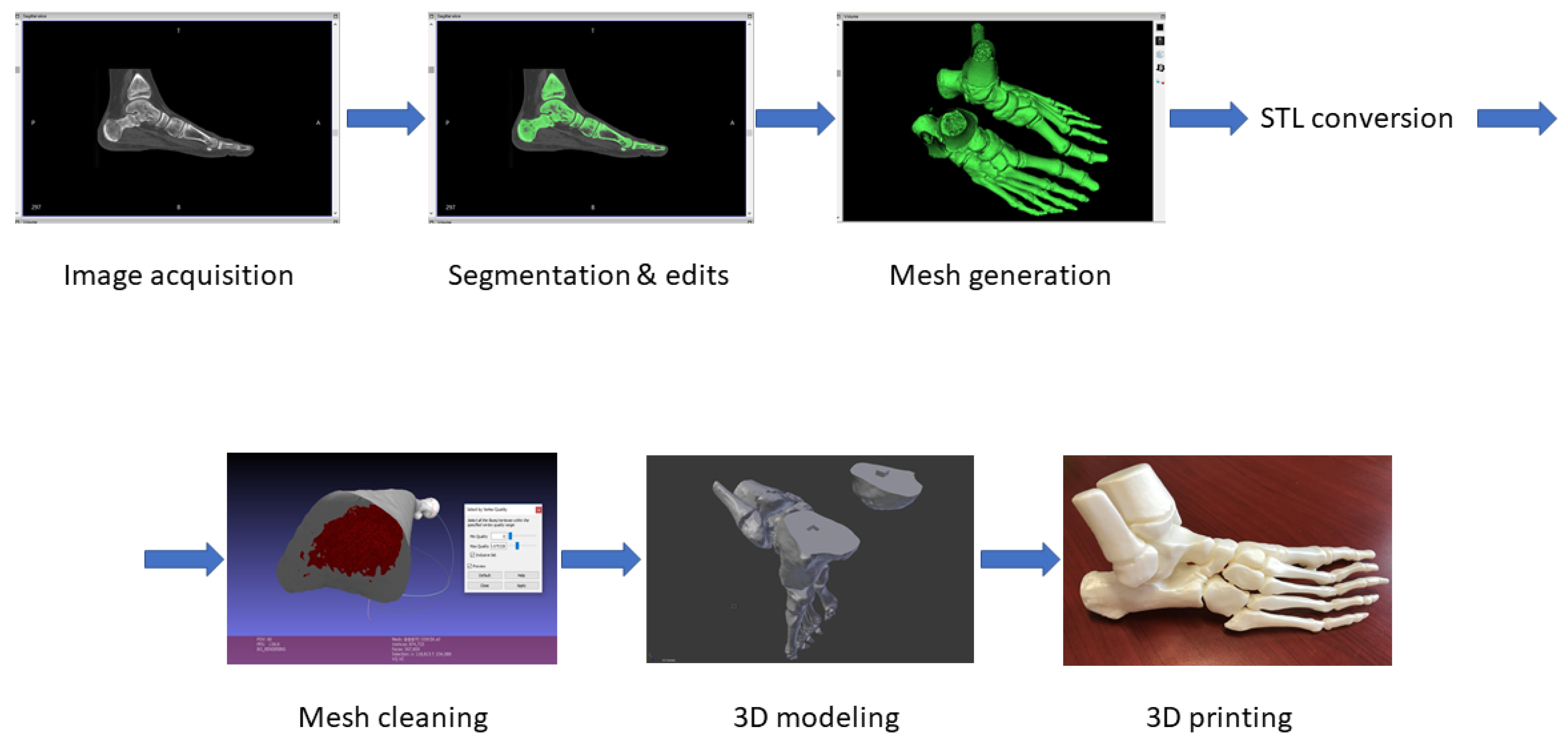
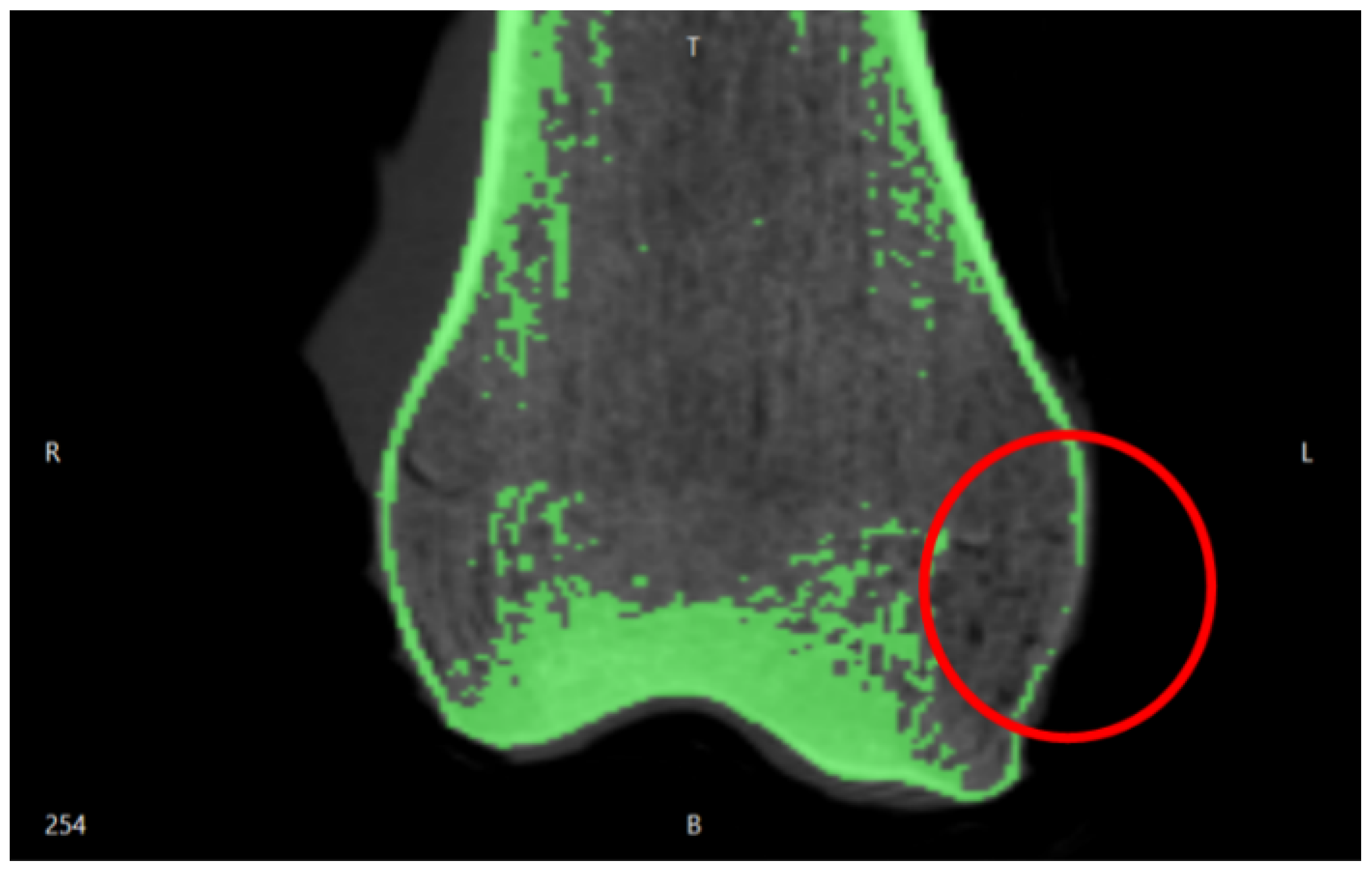
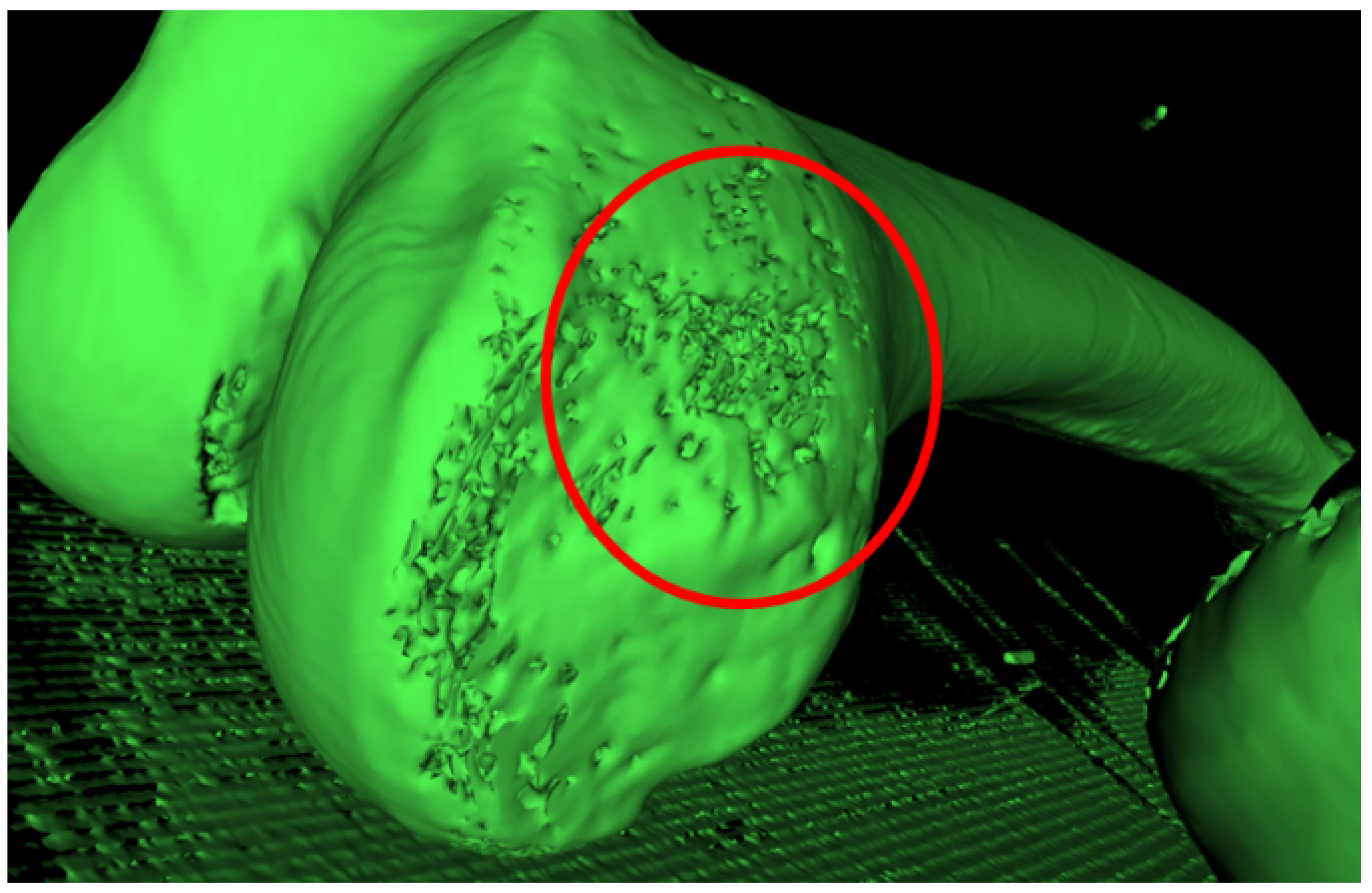
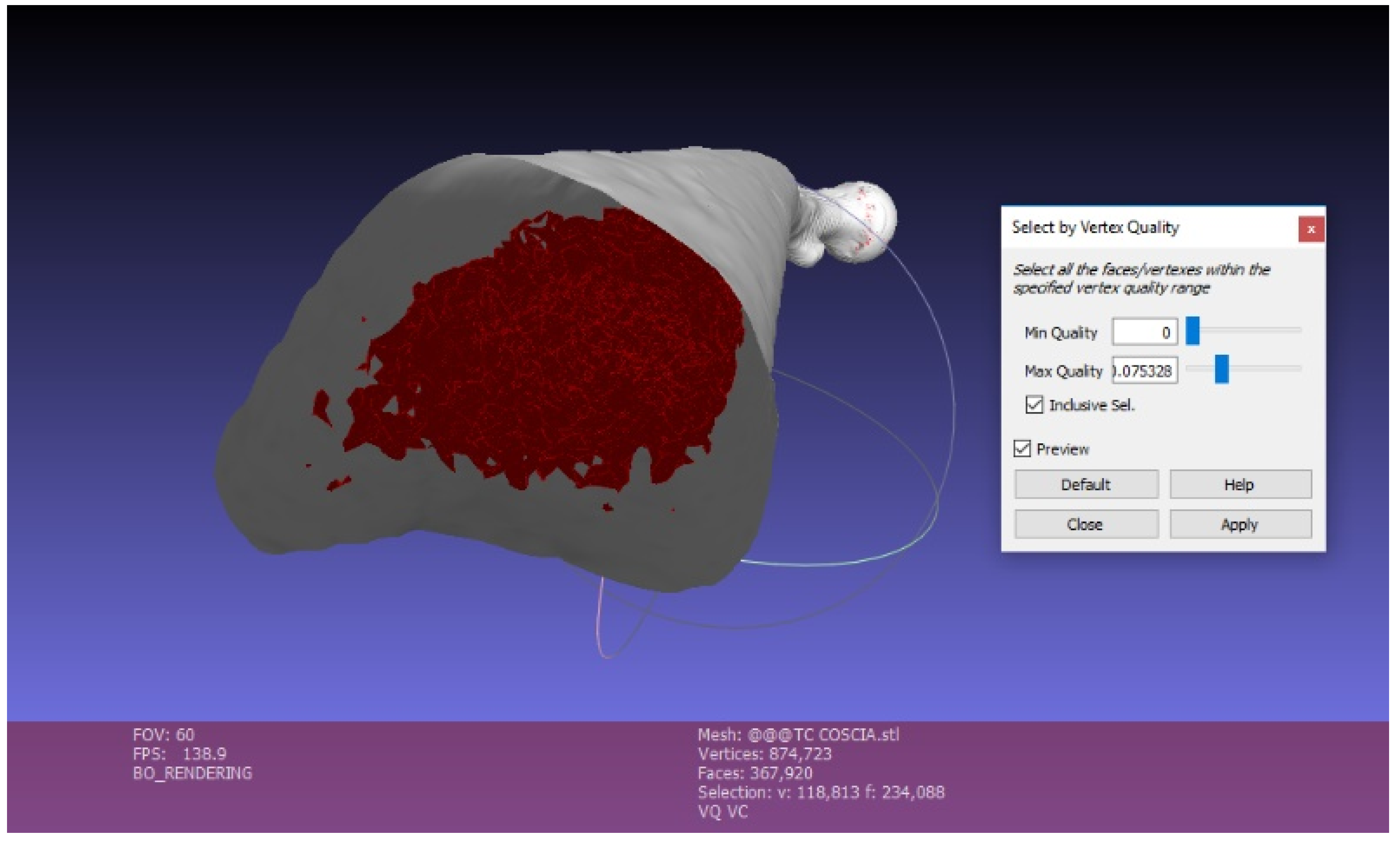
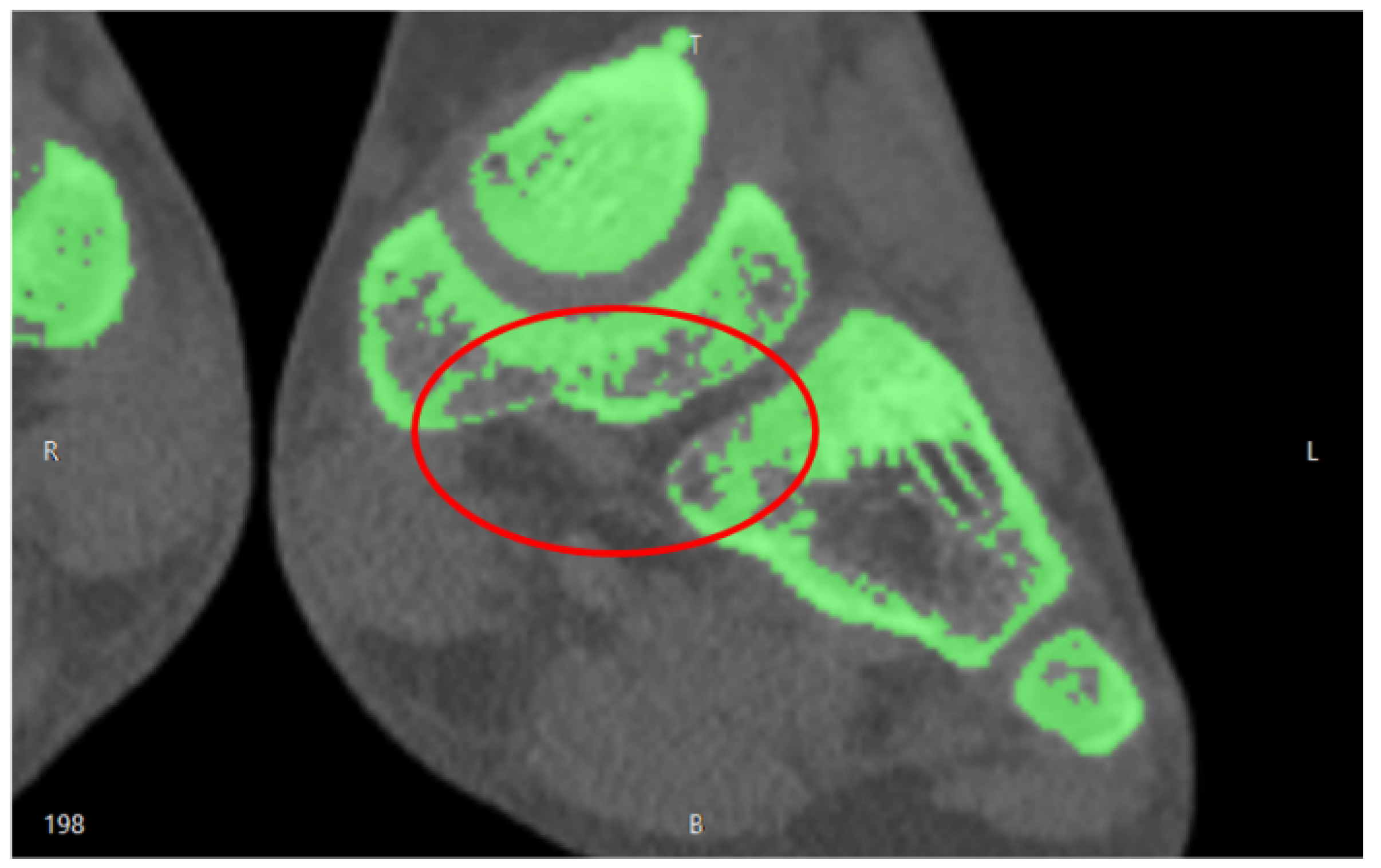
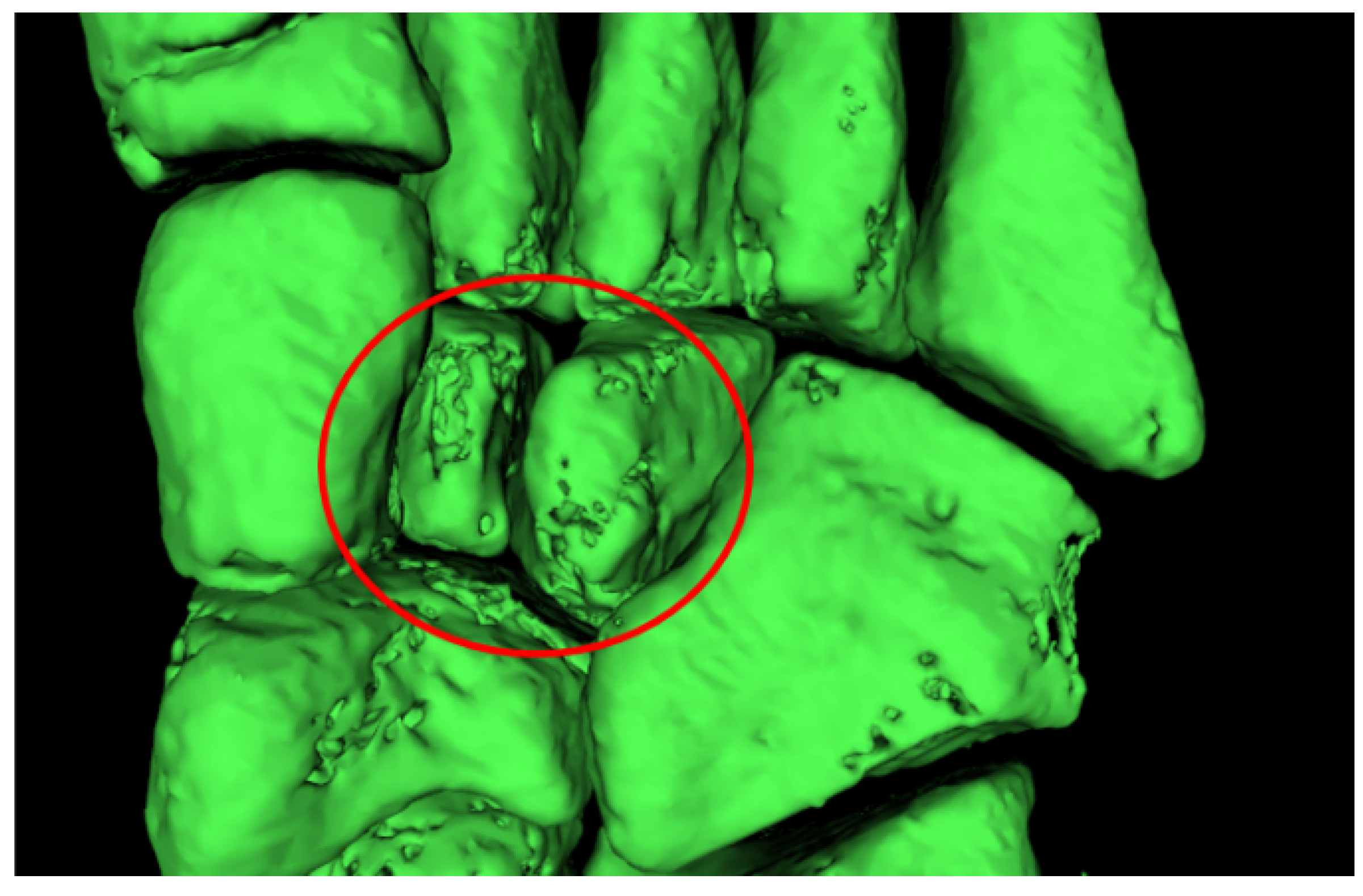
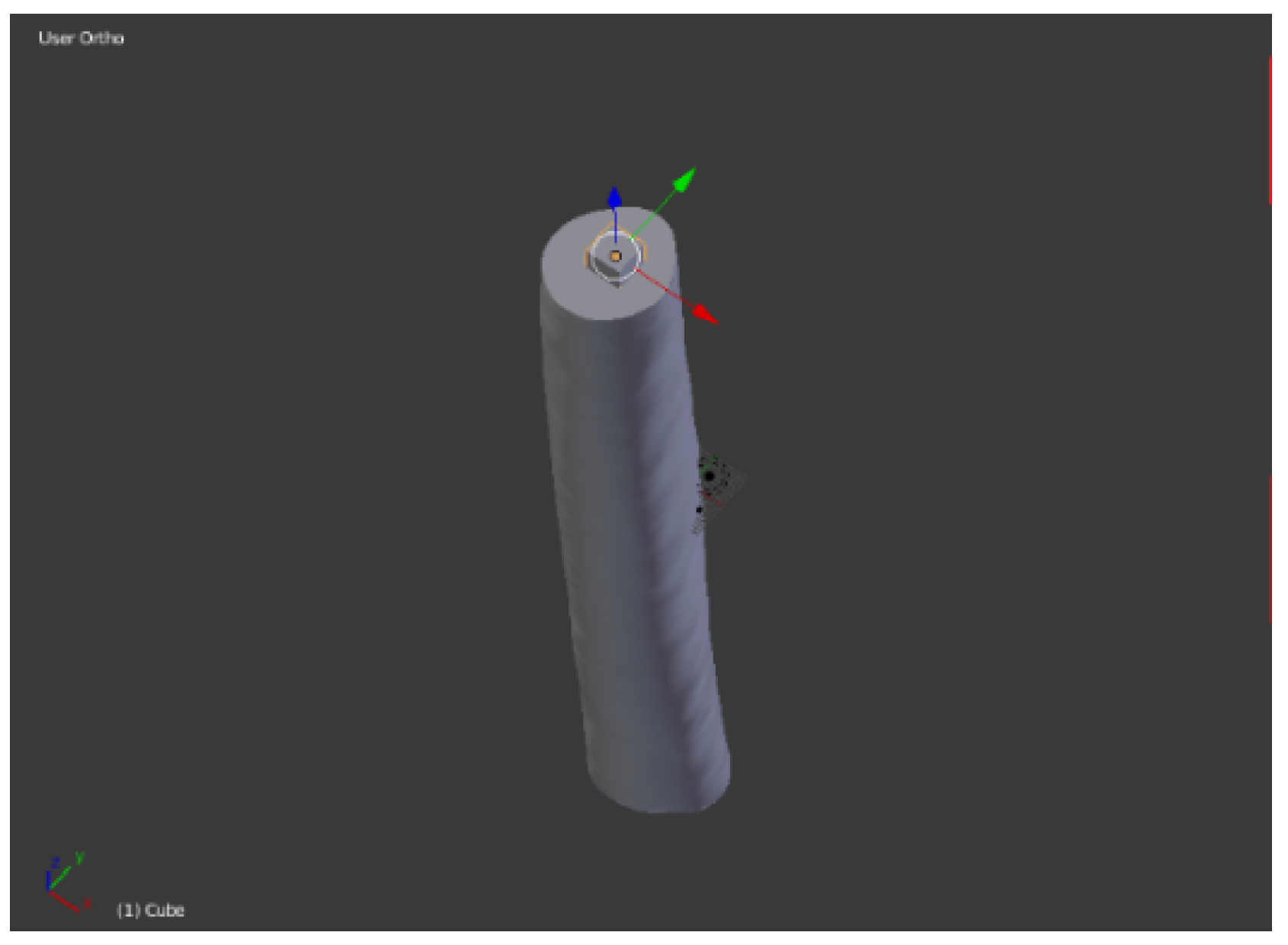
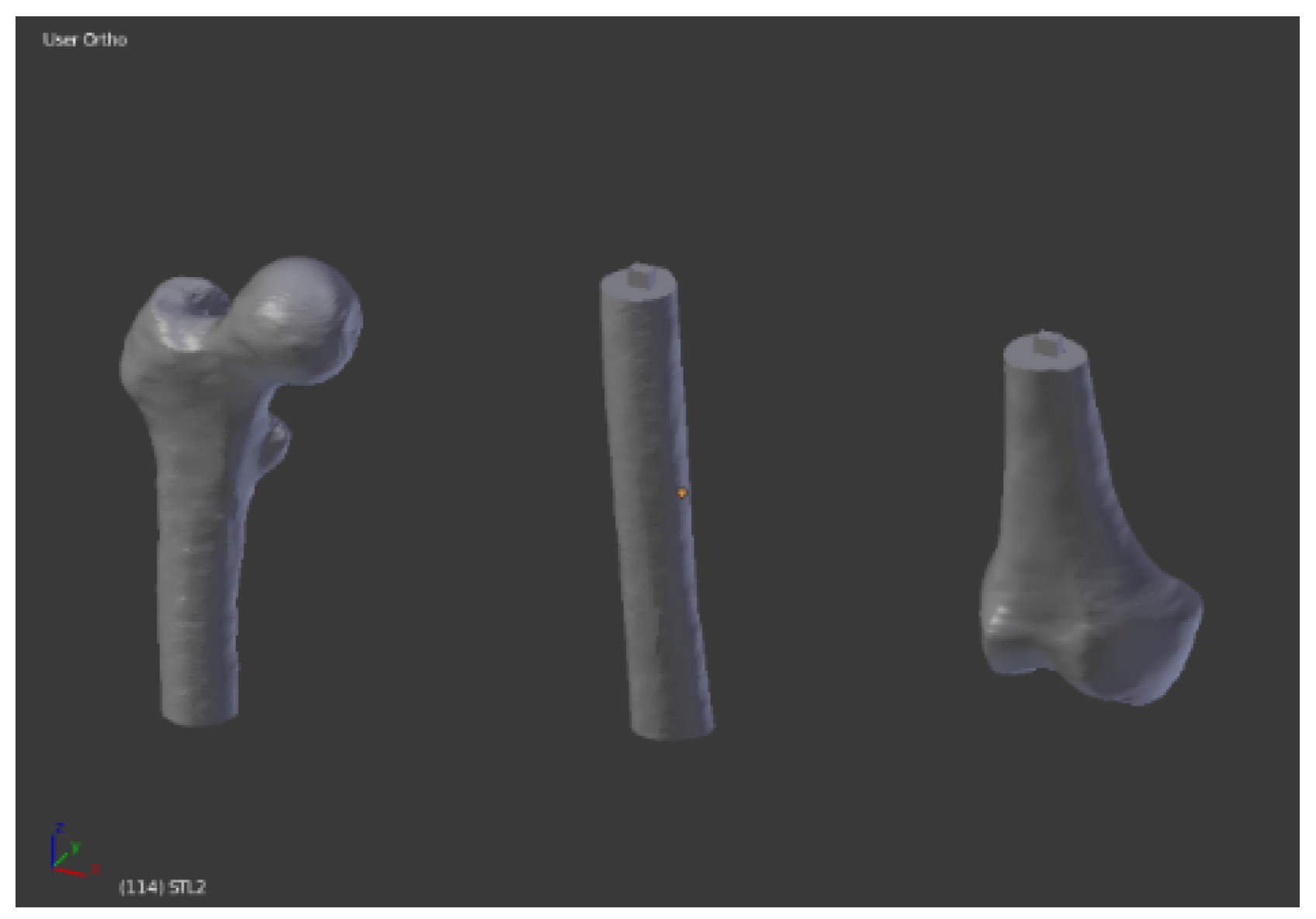
2.1. Imaging Acquisition and Mesh Processing
2.2. 3D Printing
3. Results
3.1. Imaging Acquisition and Mesh Processing
3.2. 3D Printing
3.3. Cost Analysis
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- De Amicis, R.; Ceruti, A.; Francia, D.; Frizziero, L.; Simões, B. Augmented Reality for virtual user manual. Int. J. Interact. Des. Manuf. 2018, 12, 689–697. [Google Scholar] [CrossRef]
- Frizziero, L.; Francia, D.; Donnici, G.; Liverani, A.; Caligiana, G. Sustainable design of open molds with QFD and TRIZ combination. J. Ind. Prod. Eng. 2018, 35, 21–31. [Google Scholar] [CrossRef]
- Caligiana, G.; Francia, D.; Liverani, A. CAD-CAM integration for 3D hybrid manufacturing. Lect. Notes Mech. Eng. 2017, 329–337. [Google Scholar] [CrossRef]
- Mitsouras, D.; Liacouras, P.; Imanzadeh, A.; Giannopoulos, A.; Cai, T.; Kumamaru, K.K.; George, E.; Wake, N.; Caterson, E.J.; Pomahac, B.; et al. Medical 3D Printing for the Radiologist. Radiographics 2015, 35, 1965–1988. [Google Scholar] [CrossRef] [PubMed]
- Salmi, M.; Paloheimo, K.-S.; Tuomi, J.; Wolff, J.; Mäkitie, A. Accuracy of medical models made by additive manufacturing (rapid manufacturing). J. Cranio-Maxillofac. Surg. 2013, 41, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, J.S.; Morris, J.M.; Foley, T.A.; Williamson, E.E.; Leng, S.; McGee, K.P.; Kuhlmann, J.L.; Nesberg, L.E.; Vrtiska, T.J. Three-dimensional Physical Modeling: Applications and Experience at Mayo Clinic. RadioGraphics 2015, 35, 1989–2006. [Google Scholar] [CrossRef] [PubMed]
- Francia, D.; Caligiana, G.; Liverani, A.; Frizziero, L.; Donnici, G. PrinterCAD: A QFD and TRIZ integrated design solution for large size open moulding manufacturing. Int. J. Interact. Des. Manuf. 2018, 11, 81–94. [Google Scholar] [CrossRef]
- Popov, I.; Onuh, S.O. Reverse engineering of pelvic bone for hip joint replacement. J. Med. Eng. Technol. 2009, 33, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Bortolotto, C.; Eshja, E.; Peroni, C.; Orlandi, M.A.; Bizzotto, N.; Poggi, P. 3D Printing of CT Dataset: Validation of an Open Source and Consumer-Available Workflow. J. Digit. Imaging 2016, 29, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Bizzotto, N.; Sandri, A.; Regis, D.; Romani, D.; Tami, I.; Magnan, B. Three-Dimensional Printing of Bone Fractures: A New Tangible Realistic Way for Preoperative Planning and Education. J. Abbr. 2008, 10, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Farbman, D.; McCoy, C. Materials Testing of 3D Printed ABS and PLA Samples to Guide Mechanical Design. In Proceedings of the ASME 2016 11th International Manufacturing Science and Engineering Conference, Blacksburg, VA, USA, 27 June–1 July 2016. [Google Scholar]
- Brouwers, L.; Pull ter Gunne, A.F.; de Jongh, M.A.C.; van der Heijden, F.H.W.M.; Leenen, L.P.H.; Spanjersberg, W.R.; van Helden, S.H.; Verbeek, D.O.; Bemelman, M.; Lansink, K.W.W. The Value of 3D Printed Models in Understanding Acetabular Fractures. 3D Print. Addit. Manuf. 2018, 5, 37–46. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Thickness [mm] | Printing Time [h:m] | Measured Error |
|---|---|---|
| 0.05 | 28 h and 28 min | 0.23% ± 0.32% |
| 0.1 | 15 h 7 min | 0.45% ± 0.15% |
| 0.2 | 7 h and 37 min | 0.68% ± 0.45% |
| 0.3 | 4 h and 58 min | 0.83% ± 0.52% |
| Extruder Percentage [%] | Printing Time [h:m] | Type of Error |
|---|---|---|
| 90 | 7 h 37 min | Weak Infill; Under-Extrusion; Gaps in Top Layers; Gaps Between Infill and Outline |
| 100 | 7 h 37 min | None |
| 105 | 7 h and 37 min | Blobs and Zits; Over-Extrusion |
| 110 | 7 h 37 min | Blobs and Zits; Over-Extrusion; Curling or Rough Corners |
| Infill Percentage [%] | Printing Time [h:m] | Type of Error |
|---|---|---|
| 10 | 5 h 7 min | Gaps in Top Layers |
| 15 | 7 h 37 min | None |
| 20 | 10 h and 17 min | None |
| 25 | 12 h 42 min | None |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osti, F.; Santi, G.M.; Neri, M.; Liverani, A.; Frizziero, L.; Stilli, S.; Maredi, E.; Zarantonello, P.; Gallone, G.; Stallone, S.; et al. CT Conversion Workflow for Intraoperative Usage of Bony Models: From DICOM Data to 3D Printed Models. Appl. Sci. 2019, 9, 708. https://doi.org/10.3390/app9040708
Osti F, Santi GM, Neri M, Liverani A, Frizziero L, Stilli S, Maredi E, Zarantonello P, Gallone G, Stallone S, et al. CT Conversion Workflow for Intraoperative Usage of Bony Models: From DICOM Data to 3D Printed Models. Applied Sciences. 2019; 9(4):708. https://doi.org/10.3390/app9040708
Chicago/Turabian StyleOsti, Francesco, Gian Maria Santi, Marco Neri, Alfredo Liverani, Leonardo Frizziero, Stefano Stilli, Elena Maredi, Paola Zarantonello, Giovanni Gallone, Stefano Stallone, and et al. 2019. "CT Conversion Workflow for Intraoperative Usage of Bony Models: From DICOM Data to 3D Printed Models" Applied Sciences 9, no. 4: 708. https://doi.org/10.3390/app9040708
APA StyleOsti, F., Santi, G. M., Neri, M., Liverani, A., Frizziero, L., Stilli, S., Maredi, E., Zarantonello, P., Gallone, G., Stallone, S., & Trisolino, G. (2019). CT Conversion Workflow for Intraoperative Usage of Bony Models: From DICOM Data to 3D Printed Models. Applied Sciences, 9(4), 708. https://doi.org/10.3390/app9040708