Ten Years of Gabor-Domain Optical Coherence Microscopy



Abstract
Featured Application
Abstract
1. Introduction
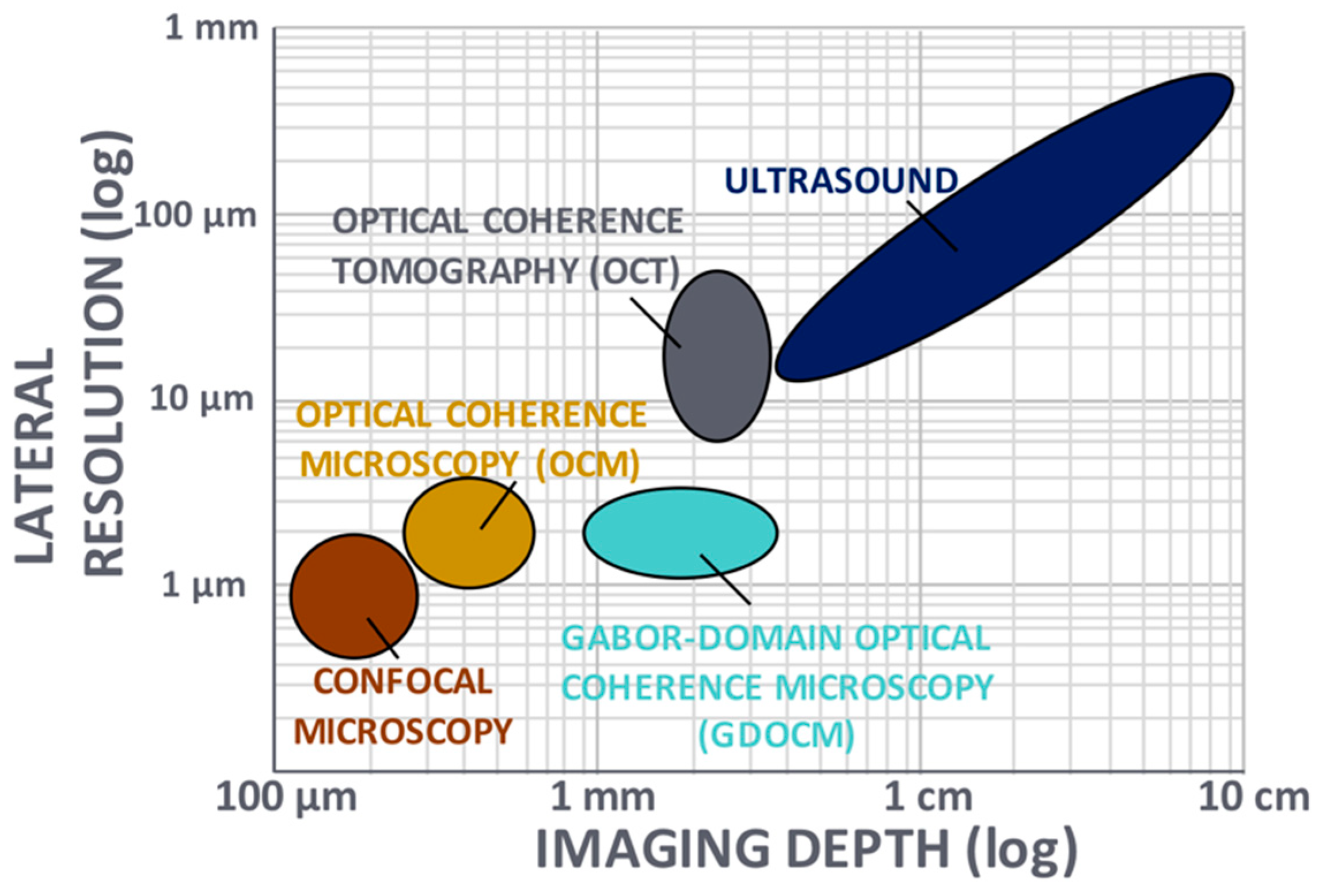
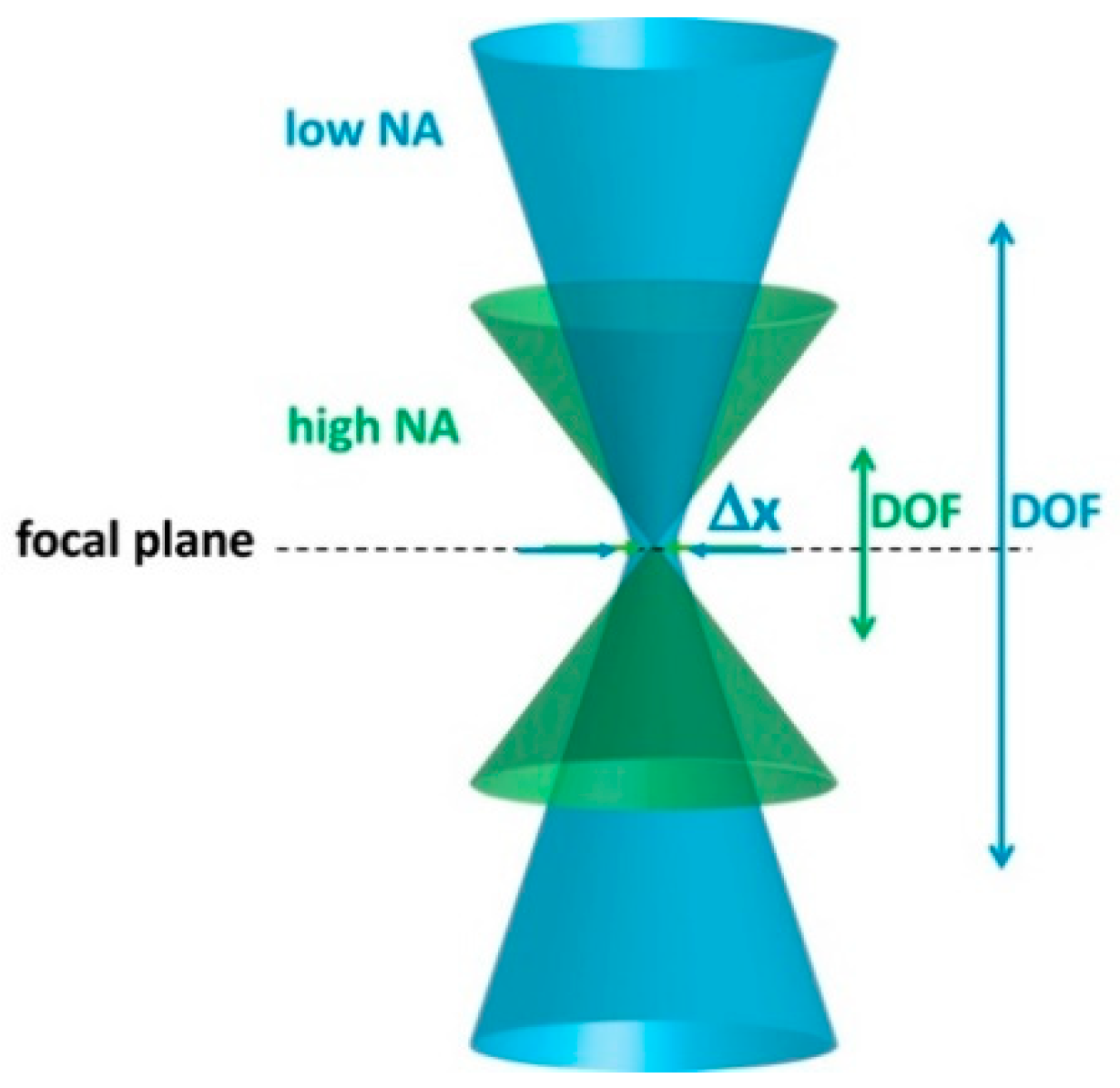
2. Strategies for Cellular-Resolution Imaging
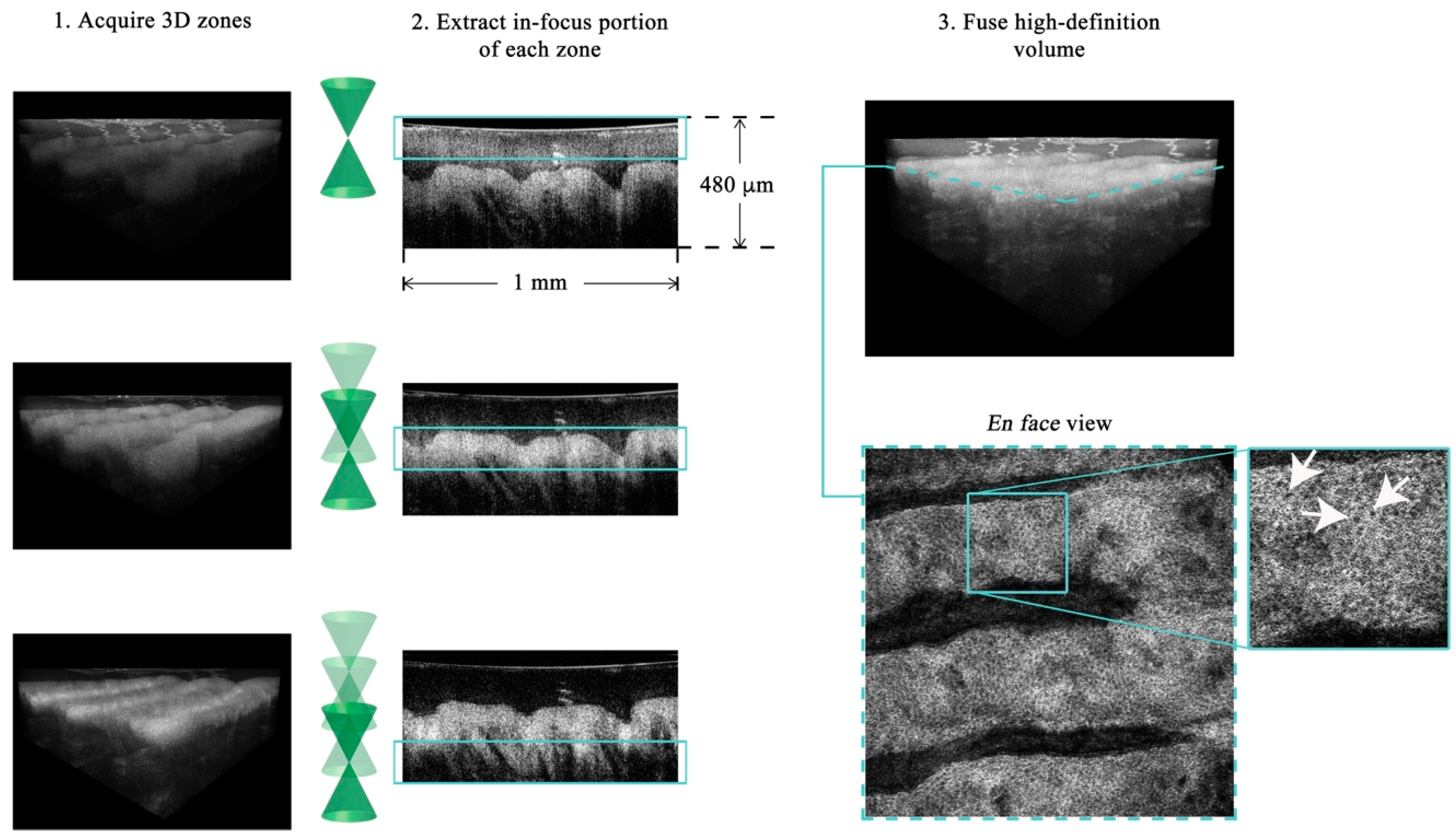
3. Gabor-Domain Optical Coherence Microscopy
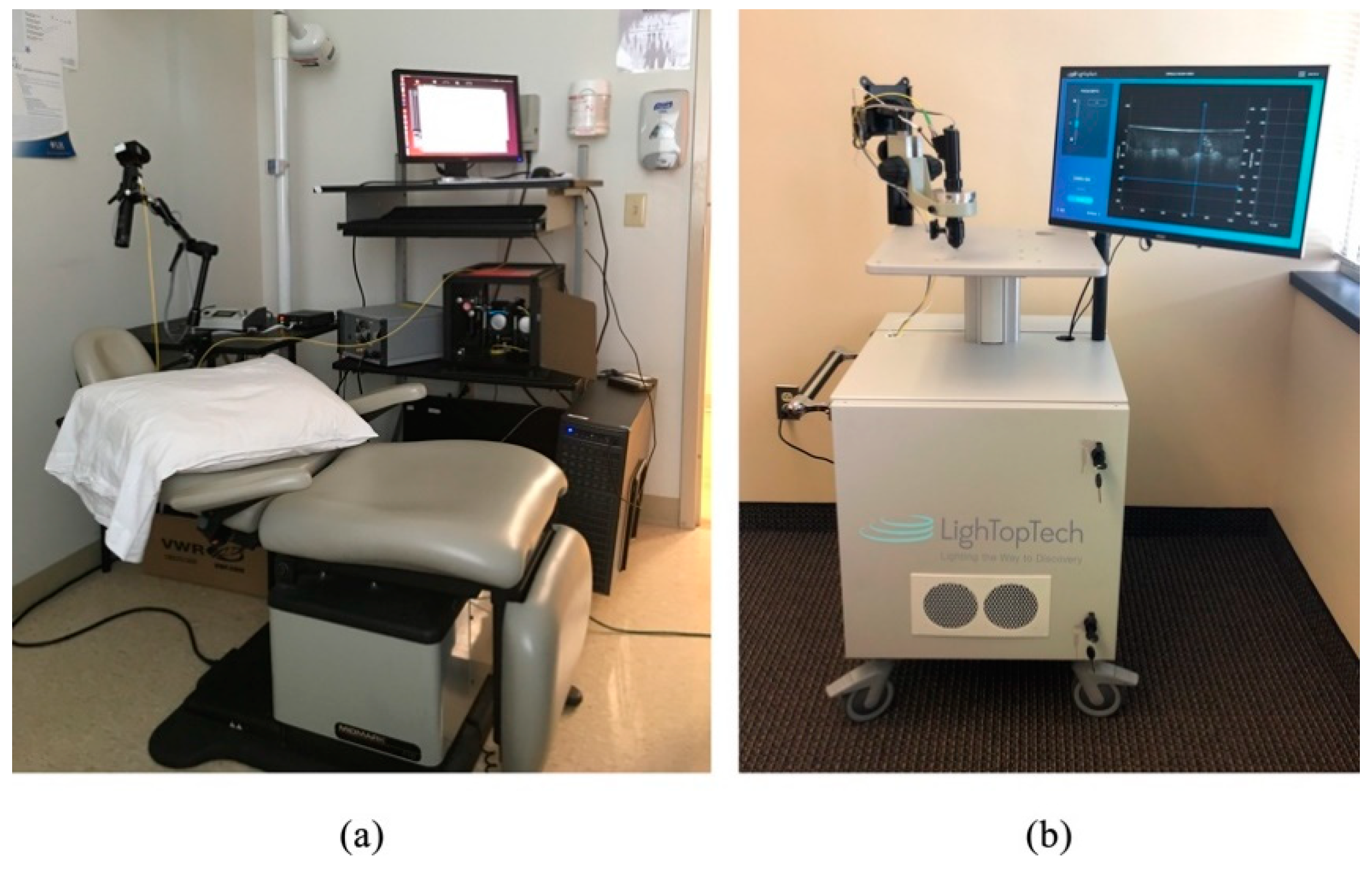
4. Applications
5. Conclusions
Funding
Conflicts of Interest
References
- Fujimoto, J.G. Optical Coherence Tomography: Introduction. In Handbook of Optical Coherence Tomography; Bouma, B.E., Tearney, G.J., Eds.; Taylor & Francis: Boca Raton, FL, USA, 2001; ISBN 9781420002508. [Google Scholar]
- Drexler, W.; Liu, M.; Kumar, A.; Kamali, T.; Unterhuber, A.; Leitgeb, R.A. Optical coherence tomography today: Speed, contrast, and multimodality. J. Biomed. Opt. 2014, 19, 71412. [Google Scholar] [CrossRef] [PubMed]
- Zysk, A.M.; Nguyen, F.T.; Oldenburg, A.L.; Marks, D.L.; Boppart, S.A. Optical coherence tomography: A review of clinical development from bench to bedside. J. Biomed. Opt. 2007, 12, 051403. [Google Scholar] [CrossRef] [PubMed]
- Minsky, M. Microscopy Apparatus. U.S. Patent 3,013,467, 19 December 1961. [Google Scholar]
- Aguirre, A.D.; Hsiung, P.; Ko, T.H.; Hartl, I.; Fujimoto, J.G. High-resolution optical coherence microscopy for high-speed, in vivo cellular imaging. Opt. Lett. 2003, 28, 2064–2066. [Google Scholar] [CrossRef] [PubMed]
- Dubois, A.; Grieve, K.; Moneron, G.; Lecaque, R.; Vabre, L.; Boccara, C. Ultrahigh-resolution full-field optical coherence tomography. Appl. Opt. 2004, 43, 2874–2883. [Google Scholar] [CrossRef] [PubMed]
- Leitgeb, R.A. En face optical coherence tomography: A technology review. Biomed. Opt. Express 2019, 10, 2177–2201. [Google Scholar] [CrossRef]
- Thouvenin, O.; Grieve, K.; Xiao, P.; Apelian, C.; Boccara, A.C. En face coherence microscopy. Biomed. Opt. Express 2017, 8, 622–639. [Google Scholar] [CrossRef]
- Ralston, T.S.; Marks, D.L.; Carney, P.S.; Boppart, S.A. Interferometric synthetic aperture microscopy. Nat. Phys. 2007, 3, 129–134. [Google Scholar] [CrossRef]
- Ahmad, A.; Shemonski, N.D.; Adie, S.G.; Kim, H.-S.; Hwu, W.-M.W.; Carney, P.S.; Boppart, S.A. Real-time in vivo computed optical interferometric tomography. Nat. Photonics 2013, 7, 444–448. [Google Scholar] [CrossRef]
- Shidlovski, V.R. Superluminescent diode light sources for OCT. In Optical Coherence Tomography: Technology and Applications, 2nd ed.; Drexler, W., Fujimoto, J.G., Eds.; Springer: Cham, Switzerland, 2015; ISBN 9783319064192. [Google Scholar]
- Fercher, A.F.; Hitzenberger, C.K.; Sticker, M.; Moreno-Barriuso, E.; Leitgeb, R.; Drexler, W.; Sattmann, H. Thermal light source technique for optical coherence tomography. Opt. Commun. 2000, 185, 57–64. [Google Scholar] [CrossRef]
- Sacchet, D.; Brzezinski, M.; Moreau, J.; Georges, P.; Dubois, A. Motion artifact suppression in full-field optical coherence tomography. Appl. Opt. 2010, 49, 1480–1488. [Google Scholar] [CrossRef]
- Ogien, J.; Dubois, A. High-resolution full-field optical coherence microscopy using a broadband light-emitting diode. Opt. Express 2016, 24, 9922–9931. [Google Scholar] [CrossRef] [PubMed]
- Froehly, L.; Meteau, J. Supercontinuum sources in optical coherence tomography: A state of the art and the application to scan-free time domain correlation techniques and depth dependant dispersion compensation. Opt. Fiber Technol. 2012, 18, 411–419. [Google Scholar] [CrossRef]
- Huang, J.; Yao, J.; Cirucci, N.; Ivanov, T.; Rolland, J.P. Performance analysis of optical coherence tomography in the context of a thickness estimation task Jinxin Huang tomography in the context of a thickness. J. Biomed. Opt. 2015, 20, 121306. [Google Scholar] [PubMed]
- Huang, J.; Hindman, H.B.; Rolland, J.P. In vivo thickness dynamics measurement of tear film lipid and aqueous layers with optical coherence tomography and maximum-likelihood estimation. Opt. Lett. 2016, 41, 1981–1984. [Google Scholar] [CrossRef] [PubMed]
- Klein, T.; Huber, R. High-speed OCT light sources and systems. Biomed. Opt. Express 2017, 8, 828–859. [Google Scholar] [CrossRef] [PubMed]
- Shu, X.; Beckmann, L.; Zhang, H.F. Visible-light optical coherence tomography: A review. J. Biomed. Opt. 2017, 22, 121707. [Google Scholar] [CrossRef] [PubMed]
- Rolland, J.P.; Meemon, P.; Murali, S.; Jain, A.; Papp, N.; Thompson, K.P.; Lee, K.-S. Gabor domain optical coherence microscopy. In Proceedings of the 1st Canterbury Workshop on Optical Coherence Tomography and Adaptive Optics, Proceedings of SPIE, Canterbury, UK, 30 December 2008; Podoleanu, A.G., Ed.; Volume 7139, p. 71390F. [Google Scholar]
- Lee, K.-S.; Akcay, A.C.; Delemos, T.; Clarkson, E.; Rolland, J.P. Dispersion control with a Fourier-domain optical delay line in a fiber-optic imaging interferometer. Appl. Opt. 2005, 44, 4009–4022. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-S.; Thompson, K.P.; Rolland, J.P. Broadband astigmatism-corrected Czerny-Turner spectrometer. Opt. Express 2010, 18, 23378–23384. [Google Scholar] [CrossRef]
- Murali, S.; Meemon, P.; Lee, K.-S.; Kuhn, W.P.; Thompson, K.P.; Rolland, J.P. Assessment of a liquid lens enabled in vivo optical coherence microscope. Appl. Opt. 2010, 49, D145–D156. [Google Scholar] [CrossRef]
- Cogliati, A.; Canavesi, C.; Hayes, A.; Tankam, P.; Duma, V.-F.; Santhanam, A.; Thompson, K.P.; Rolland, J.P. MEMS-based handheld scanning probe with pre-shaped input signals for distortion-free images in Gabor-Domain Optical Coherence Microscopy. Opt. Express 2016, 24, 13365–13374. [Google Scholar] [CrossRef]
- Murali, S.; Thompson, K.P.; Rolland, J.P. Three-dimensional adaptive microscopy using embedded liquid lens. Opt. Lett. 2009, 34, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Rolland, J.P.; Meemon, P.; Murali, S.; Thompson, K.P.; Lee, K. Gabor-based fusion technique for Optical Coherence Microscopy. Opt. Express 2010, 18, 3632–3642. [Google Scholar] [CrossRef] [PubMed]
- Meemon, P.; Widjaja, J.; Rolland, J.P. Spectral fusing Gabor domain optical coherence microscopy. Opt. Lett. 2016, 41, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Tankam, P.; Santhanam, A.P.; Lee, K.-S.; Won, J.; Canavesi, C.; Rolland, J.P. Parallelized multi–graphics processing unit framework for high-speed Gabor-domain optical coherence microscopy. J. Biomed. Opt. 2014, 19, 71410. [Google Scholar] [CrossRef] [PubMed]
- Zhivov, A.; Stachs, O.; Stave, J.; Guthoff, R.F. In vivo three-dimensional confocal laser scanning microscopy of corneal surface and epithelium. Br. J. Ophthalmol. 2009, 93, 667. [Google Scholar] [CrossRef] [PubMed]
- Ang, M.; Baskaran, M.; Werkmeister, R.M.; Chua, J.; Schmidl, D.; Aranha dos Santos, V.; Garhöfer, G.; Mehta, J.S.; Schmetterer, L. Anterior segment optical coherence tomography. Prog. Retin. Eye Res. 2018, 66, 132–156. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.; Hosseinaee, Z.; Han, L.; Kralj, O.; Sorbara, L.; Bizheva, K. 250 kHz, 1.5 um resolution SD-OCT for in-vivo cellular imaging of the human cornea. Biomed. Opt. Express 2018, 9, 6569–6583. [Google Scholar] [CrossRef] [PubMed]
- Mazlin, V.; Xiao, P.; Dalimier, E.; Grieve, K.; Irsch, K.; Sahel, J.-A.; Fink, M.; Boccara, A.C. In vivo high resolution human corneal imaging using full-field optical coherence tomography. Biomed. Opt. Express 2018, 9, 557–568. [Google Scholar] [CrossRef]
- Fujimoto, J.; Swanson, E. The development, commercialization, and impact of optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT1–OCT13. [Google Scholar] [CrossRef]
- Vakoc, B.J.; Fukumura, D.; Jain, R.K.; Bouma, B.E. Cancer imaging by optical coherence tomography—Preclinical progress and clinical potential. Nat. Rev. Cancer 2012, 12, 363–368. [Google Scholar] [CrossRef]
- Drexler, W.; Fujimoto, J.G. State-of-the-art retinal optical coherence tomography. Prog. Retin. Eye Res. 2008, 27, 45–88. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Kashani, A.H.; Chen, C.L.; Gahm, J.K.; Zheng, F.; Richter, G.M.; Rosenfeld, P.J.; Shi, Y.; Wang, R.K. Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications. Prog. Retin. Eye Res. 2017, 60, 66–100. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Pljakic, A.; Schmitz, L. Recent advances in clinical application of optical coherence tomography of human skin. Clin. Cosmet. Investig. Dermatol. 2015, 8, 345–354. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Olsen, J.; Holmes, J.; Jemec, G.B.E. Advances in optical coherence tomography in dermatology—A review. J. Biomed. Opt. 2018, 23, 040901. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, P.; Krasieva, T.; Jung, W.-G.; Zhang, J.; Chen, Z.; Osann, K.; Tromberg, B. Noninvasive imaging of oral premalignancy and malignancy. J. Biomed. Opt. 2005, 10, 051601. [Google Scholar] [CrossRef] [PubMed]
- Escobar, P.F.; Rojas-Espaillat, L.; Tisci, S.; Enerson, C.; Brainard, J.; Smith, J.; Tresser, N.J.; Feldchtein, F.I.; Rojas, L.B.; Belinson, J.L. Optical coherence tomography as a diagnostic aid to visual inspection and colposcopy for preinvasive and invasive cancer of the uterine cervix. Int. J. Gynecol. Cancer 2006, 16, 1815–1822. [Google Scholar] [CrossRef] [PubMed]
- Gallwas, J.; Jalilova, A.; Ladurner, R.; Kolben, T.M.; Kolben, T.; Ditsch, N.; Homann, C.; Lankenau, E.; Dannecker, C. Detection of cervical intraepithelial neoplasia by using optical coherence tomography in combination with microscopy. J. Biomed. Opt. 2017, 22, 16013. [Google Scholar] [CrossRef]
- Assayag, O.; Grieve, K.; Devaux, B.; Harms, F.; Pallud, J.; Chretien, F.; Boccara, C.; Varlet, P. Imaging of non-tumorous and tumorous human brain tissues with full-field optical coherence tomography. NeuroImage Clin. 2013, 2, 549–557. [Google Scholar] [CrossRef]
- Nguyen, F.T.; Zysk, A.M.; Chaney, E.J.; Kotynek, J.G.; Oliphant, U.J.; Bellafiore, F.J.; Rowland, K.M.; Johnson, P.A.; Boppart, S.A. Intraoperative evaluation of breast tumor margins with optical coherence tomography. Cancer Res. 2009, 69, 8790–8796. [Google Scholar] [CrossRef]
- Betz, C.S.; Volgger, V.; Silverman, S.M.; Rubinstein, M.; Kraft, M.; Arens, C.; Wong, B.J.F. Clinical optical coherence tomography in head & neck oncology: Overview and outlook. Head Neck Oncol. 2013, 5, 35. [Google Scholar]
- Wang, J.; Xu, Y.; Boppart, S.A. Review of optical coherence tomography in oncology. J. Biomed. Opt. 2017, 22, 121711. [Google Scholar] [CrossRef] [PubMed]
- Machoy, M.; Seeliger, J.; Szyszka-Sommerfeld, L.; Koprowski, R.; Gedrange, T.; Woźniak, K. The Use of Optical Coherence Tomography in Dental Diagnostics: A State-of-the-Art Review. J. Healthc. Eng. 2017, 2017. [Google Scholar] [CrossRef]
- Fujimoto, J.G.; Schmitt, J.M.; Swanson, E.A.; Jang, I.K. The development of OCT. In Cardiovascular OCT Imaging; Springer: Cham, Switzerland, 2015; ISBN 9783319108018. [Google Scholar]
- Bezerra, H.G.; Costa, M.A.; Guagliumi, G.; Rollins, A.M.; Simon, D.I. Intracoronary Optical Coherence Tomography: A Comprehensive Review. Clinical and Research Applications. JACC Cardiovasc. Interv. 2009, 2, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Tearney, G.J.; Brezinski, M.E.; Bouma, B.E.; Boppart, S.A.; Pitris, C.; Southern, J.F.; Fujimoto, J.G. In vivo endoscopic optical biopsy with optical coherence tomography. Science 1997, 276, 2037–2039. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.-H.; Leggett, C.L.; Trindade, A.J. Optical coherence tomography in gastroenterology: A review and future outlook. J. Biomed. Opt. 2017, 22, 121716. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, R.A.; Yang, X.; Quirk, B.C.; Lorenser, D.; Kirk, R.W.; Noble, P.B.; Sampson, D.D. Static and dynamic imaging of alveoli using optical coherence tomography needle probes. J. Appl. Physiol. 2012, 113, 967–974. [Google Scholar] [CrossRef]
- Lorenser, D.; Quirk, B.C.; Auger, M.; Madore, W.-J.; Kirk, R.W.; Godbout, N.; Sampson, D.D.; Boudoux, C.; McLaughlin, R.A. Dual-modality needle probe for combined fluorescence imaging and three-dimensional optical coherence tomography. Opt. Lett. 2013, 38, 266–268. [Google Scholar] [CrossRef] [PubMed]
- Hariri, L.P.; Mino-Kenudson, M.; Lanuti, M.; Miller, A.J.; Mark, E.J.; Suter, M.J. Diagnosing lung carcinomas with optical coherence tomography. Ann. Am. Thorac. Soc. 2015, 12, 193–201. [Google Scholar] [CrossRef]
- Kim, J.; Brown, W.; Maher, J.R.; Levinson, H.; Wax, A. Functional optical coherence tomography: Principles and progress. Phys. Med. Biol. 2015, 60, R211–R237. [Google Scholar] [CrossRef]
- de Boer, J.F.; Hitzenberger, C.K.; Yasuno, Y. Polarization sensitive optical coherence tomography—A review. Biomed. Opt. Express 2017, 8, 1838. [Google Scholar] [CrossRef]
- Canavesi, C.; Morichetti, F.; Canciamilla, A.; Persia, F.; Melloni, A. Polarization- and phase-sensitive low-coherence interferometry setup for the characterization of integrated optical components. J. Light. Technol. 2009, 27, 3062–3074. [Google Scholar] [CrossRef]
- Zvietcovich, F.; Rolland, J.P.; Yao, J.; Meemon, P.; Parker, K.J. Comparative study of shear wave-based elastography techniques in optical coherence tomography. J. Biomed. Opt. 2017, 22, 35010. [Google Scholar] [CrossRef] [PubMed]
- Meemon, P.; Yao, J.; Chu, Y.-J.; Zvietcovich, F.; Parker, K.J.; Rolland, J.P. Crawling wave optical coherence elastography. Opt. Lett. 2016, 41, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Standish, B.; Yang, V.X.D. Optical coherence elastography: Current status and future applications. J. Biomed. Opt. 2011, 16, 043001. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Larin, K.V. Optical coherence elastography for tissue characterization: A review. J. Biophotonics 2015, 8, 279–302. [Google Scholar] [CrossRef]
- Kennedy, B.F.; Kennedy, K.M.; Sampson, D.D. A review of optical coherence elastography: Fundamentals, techniques and prospects. IEEE J. Sel. Top. Quantum Electron. 2014, 20, 1–17. [Google Scholar] [CrossRef]
- Rolland, J.P.; Zvietcovich, F.; Ge, G.; Parker, K.J. Perspectives and advances in optical elastography. In Proceedings of the Optical Elastography and Tissue Biomechanics VI, San Francisco, CA, USA, 2–7 February 2019; Volume 10880, p. 108800G. [Google Scholar]
- Mulligan, J.A.; Untracht, G.R.; Chandrasekaran, S.N.; Brown, C.N.; Adie, S.G. Emerging Approaches for High-Resolution Imaging of Tissue Biomechanics with Optical Coherence Elastography. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 6800520. [Google Scholar] [CrossRef]
- Auksorius, E.; Bromberg, Y.; Motiejūnaitė, R.; Pieretti, A.; Liu, L.; Coron, E.; Aranda, J.; Goldstein, A.M.; Bouma, B.E.; Kazlauskas, A.; et al. Dual-modality fluorescence and full-field optical coherence microscopy for biomedical imaging applications. Biomed. Opt. Express 2012, 3, 661–666. [Google Scholar] [CrossRef]
- Makhlouf, H.; Perronet, K.; Dupuis, G.; Lévêque-Fort, S.; Dubois, A. Simultaneous optically sectioned fluorescence and optical coherence microscopy with full-field illumination. Opt. Lett. 2012, 37, 1613–1615. [Google Scholar] [CrossRef]
- Thouvenin, O.; Fink, M.; Boccara, C. Dynamic multimodal full-field optical coherence tomography and fluorescence structured illumination microscopy. J. Biomed. Opt. 2017, 22, 26004. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.S.; Yoo, H. Spectroscopic optical coherence tomography: A review of concepts and biomedical applications. Appl. Spectrosc. Rev. 2018, 53, 91–111. [Google Scholar] [CrossRef]
- Lee, K.-S.; Zhao, H.; Ibrahim, S.F.; Meemon, N.; Khoudeir, L.; Rolland, J.P. Three-dimensional imaging of normal skin and nonmelanoma skin cancer with cellular resolution using Gabor domain optical coherence microscopy. J. Biomed. Opt. 2012, 17, 126006. [Google Scholar] [CrossRef] [PubMed]
- Rolland, J.P.; Lee, K.S.; Meemon, P.; Ibrahim, S.F. Gabor Domain Optical Coherence Microscopy of Human Skin. In Advances in Dermatological Sciences; The Royal Society of Chemistry: London, UK, 2014; pp. 37–52. ISBN 978-1-84973-398-4. [Google Scholar]
- Tankam, P.; Soh, J.; Canavesi, C.; Lanis, M.; Hayes, A.; Cogliati, A.; Rolland, J.P.; Ibrahim, S.F. Gabor-Domain Optical Coherence Tomography to Aid in Mohs Resection of Basal Cell Carcinoma. J. Am. Acad. Dermatol. 2019, 80, 1766–1769. [Google Scholar] [CrossRef] [PubMed]
- Tankam, P.; He, Z.; Thuret, G.; Hindman, H.B.; Canavesi, C.; Coyoc Escudero, J.; Lepine, T.; Gain, P.; Rolland, J.P. Capabilities of Gabor-domain Optical Coherence Microscopy for the Assessment of Corneal Disease. J. Biomed. Opt. 2019, 24, 046002. [Google Scholar]
- Canavesi, C.; O’Connell, R.; Pazcos, T.; Cogliati, A.; Hayes, A.; Bonham, A.; Rolland, J.P. Gabor-domain optical coherence microscopy for optical biopsy, image-guided surgery, and intraoperative imaging. Int. J. CARS (Computer Assisted Radiology and Surgery) 2019, 14 (Suppl. 1), S18–S19. [Google Scholar]
- Canavesi, C.; Cogliati, A.; Hayes, A.; Santhanam, A.P.; Tankam, P.; Rolland, J.P. Gabor-domain optical coherence microscopy with integrated dual-axis MEMS scanner for fast 3D imaging and metrology. In Proceedings of the SPIE—The International Society for Optical Engineering, New York, NY, USA, 11 October 2015; Volume 9633, p. 96330O. [Google Scholar]
- Tankam, P.; Won, J.; Canavesi, C.; Cox, I.; Rolland, J.P. Optical Assessment of Soft Contact Lens Edge-Thickness. Optom. Vis. Sci. 2016, 93, 987–996. [Google Scholar] [CrossRef]
- Canavesi, C.; Cogliati, A.; Yoon, C.; Mietus, A.; Qi, Y.; Stone, J.J.; Hindman, H.B.; Rolland, J.P. 3D cellular imaging of the cornea with Gabor-domain optical coherence microscopy. In Proceedings of the SPIE 10867, Optical Coherence Tomography and Coherence Domain Optical Methods in Biomedicine XXIII, San Francisco, CA, USA, 2–7 February 2019; p. 108670F. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | Axial Resolution (μm) | Transverse Resolution (μm) | Imaging Depth (mm) | Field of View (mm) | Image Orientation | Contact |
|---|---|---|---|---|---|---|
| CM [29] | 7.6 | 1–2 | <0.1 | 0.4 × 0.4 | En face | Yes |
| SD-OCT [30] | 1–10 | 10–20 | 6 | 6–16 | Cross-sectional | No |
| OCM [31] | 1.5 | 1.5 | <0.2 | 0.8 × 0.8 | Cross-sectional | Not required |
| FF-OCT [14,32] | 0.7–7.7 | 1.7–2 | <1 | 0.9–1.3 × 0.9–1.3 | En face | Not required |
| GDOCM | 2 | 2.6 | 2.5 | 1.5 × 1.5 | Cross-sectional | Not required |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canavesi, C.; Rolland, J.P. Ten Years of Gabor-Domain Optical Coherence Microscopy. Appl. Sci. 2019, 9, 2565. https://doi.org/10.3390/app9122565
Canavesi C, Rolland JP. Ten Years of Gabor-Domain Optical Coherence Microscopy. Applied Sciences. 2019; 9(12):2565. https://doi.org/10.3390/app9122565
Chicago/Turabian StyleCanavesi, Cristina, and Jannick P. Rolland. 2019. "Ten Years of Gabor-Domain Optical Coherence Microscopy" Applied Sciences 9, no. 12: 2565. https://doi.org/10.3390/app9122565
APA StyleCanavesi, C., & Rolland, J. P. (2019). Ten Years of Gabor-Domain Optical Coherence Microscopy. Applied Sciences, 9(12), 2565. https://doi.org/10.3390/app9122565