Using Artificial Neural Networks for Identifying Patients with Mild Cognitive Impairment Associated with Depression Using Neuropsychological Test Features

 ,
, 


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Evaluation
- Attention. Digit Span Forward and Backward. These tests evaluate the number of digits that a person can immediately hold in the same direction (attentional span) or in the opposite direction (working memory). These include the Trail Making Test Part A (TMT A) [31].
- Executive Function. The Frontal Assessment Battery (FAB) [32], a bedside cognitive and behavioral battery to assess frontal lobe function and identify a dysexecutive syndrome. The Verbal fluency p and Verbal fluency animals test involves the generation of items from two specific categories in a minute: words that begin with p and animals. The Spanish multicenter normative studies (NEURONORMA project) [33] were used.
- Memory. The Spanish adaptation of the California Verbal Learning Test was used, called the Test of Verbal Learning España-Complutense (TAVEC) [34], where the patient must learn 16 words in five trials. Then, the patient must learn a new list of interferences. After that, the patient must remember the first list in short-term free recall, memory with short-term cued recall, long-term free recall, memory with long-term cued recall, and recognition. The Rey–Osterrieth Complex Figure Test (Memory) [35] was used to evaluate visual memory; patients had to reproduce the complex figure they have previously drawn.
- Praxis. The abbreviated Barcelona Test (a-BT) [36], a subtest of gestural and bimanual praxis, where the patient must make and copy different gestures such as saying hello, asking for silence, etc., and the visuo-constructional praxis and the Rey–Osterrieth Complex Figure Test (Copy) [35], where the patient must draw a complex figure.
- Language. The Abbreviated Boston Naming Test (BNT Abbreviated) [37], where the patient must name 15 drawings, and the abbreviated Barcelona Test (a-BT) command, where the patient must perform a series of simple commands.
2.3. Statistical Analysis
2.4. Classification Using Artificial Neural Networks
- Data partition. Data partitioning can be used to determine the accuracy of a model’s estimates of new data. For this work, we chose a 10-fold repeated cross-validation method. This subtype of cross-validation method randomly breaks the dataset into 10 subsets, which are sequentially used as test sets, while the other nine are used for training. This cross-validation method was repeated 50 times to obtain the information necessary to perform a statistically significant evaluation.
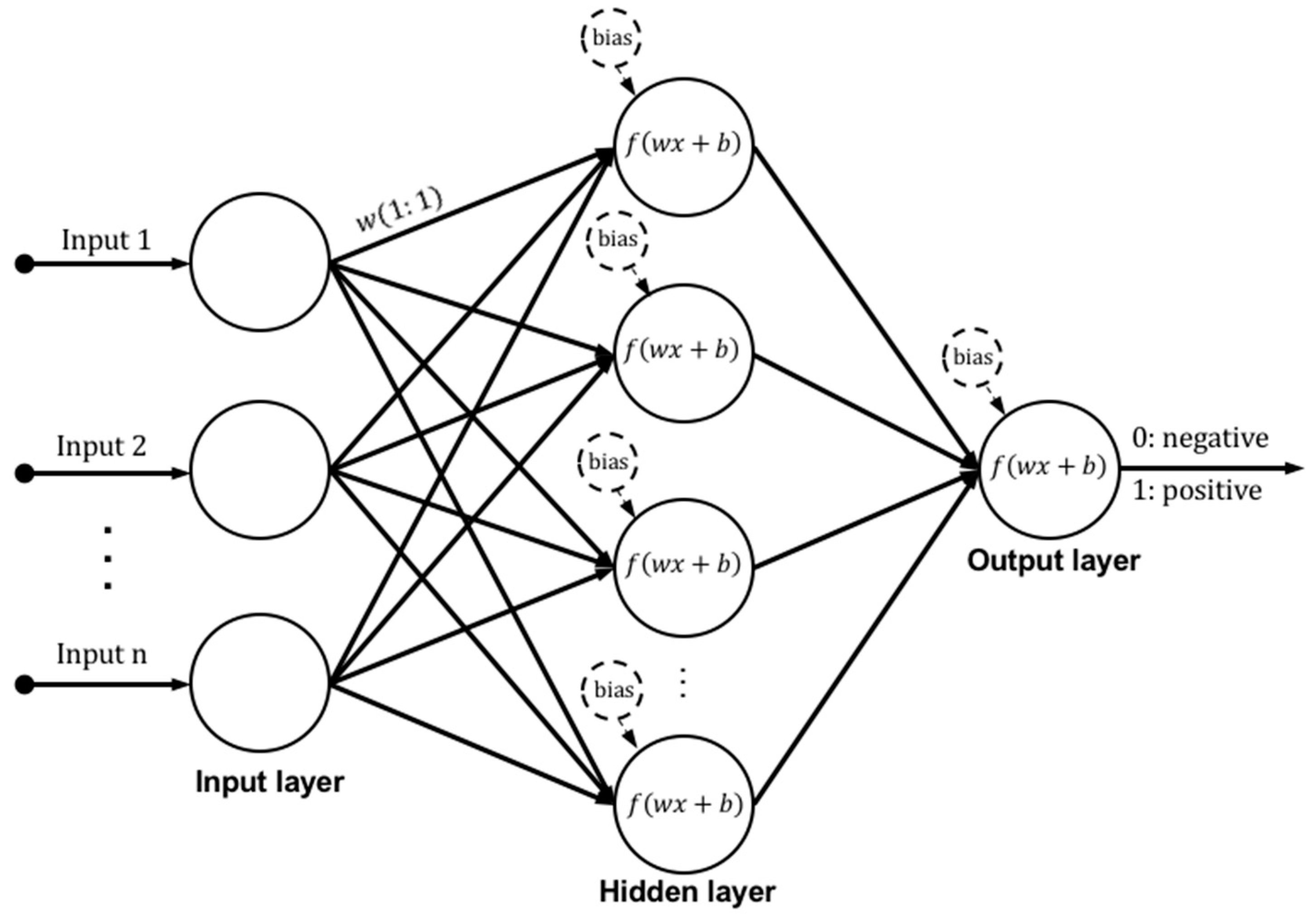
- Architecture selection. The number of neurons, layers, and their connections determine the architecture of an ANN. There is no general rule in choosing the best architecture, and optimization is based on testing several architectures until finding one that might offer satisfactory results [25]. Several architectures of the ANN with one and two hidden layers were tested to choose the best one. We evaluated architectures of 3, 8, 12, and 15 neurons for one-layer examples and architectures of {5 3}, {8 5}, {10 8}, and {12 10} neurons for two-layer examples. The optimization algorithm used to train these ANNs is a variation of the gradient descent known as scaled conjugate gradient backpropagation [38]. The results were compared using an analysis of variance (ANOVA) and Tukey’s honest significance test [39], and a p-value of <0.01 was used to determine whether there were statistically significant differences between the proposed architectures.
- Cut-off value selection. For a given cut-off value or decision threshold, each patient was classified in one of the diagnostic groups by comparing the measurement to this cut-off value. Choosing an appropriate decision threshold is of paramount importance in using a test effectively. There are various methods to determine the optimal test cut-off value, mostly based on a receiver operating characteristic (ROC) analysis. The ROC curve offers a graphical illustration of the true positive rate (sensitivity) against the false positive rate (1–specificity) for all possible cut-off values. Thus, each point on an ROC curve corresponds to a cut-off value and is associated with a test sensitivity and specificity. Sensitivity is the number of correctly detected positive patterns/total number of actual positive patterns. A positive pattern in this context indicates an MCI patient with depression. On the other hand, specificity is the number of correctly detected negative patterns/total number of actual negative patterns. A negative pattern in this context indicates an MCI patient without depression. Locating the best cut-off point requires a compromise between both measures. One of the most common criteria, and the one chosen in this work, is the point on an ROC curve with the best trade-off between specificity and sensitivity, trying to maximize both indices.
- Performance analysis. The following statistical parameters were computed to evaluate the MLPNN classification performance:
- ⚬
- Accuracy: Number of correctly classified patterns/total number of patterns.
- ⚬
- Sensitivity: The MLPNN’s ability to correctly detect MCI patients with depression.
- ⚬
- Specificity: The MLPNN’s ability to correctly detect MCI patients without depression.
- ⚬
- AUC: Area under an ROC curve, one of the most important evaluation metrics for any classification model’s performance.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alexopoulos, G.S.; Kiosses, D.N.; Klimstra, S.; Kalayam, B.; Bruce, M.L. Clinical presentation of the “depression-executive dysfunction syndrome” of late life. Am. J. Geriatr. Psychiatry 2002, 10, 98–106. [Google Scholar] [PubMed]
- Butters, M.A.; Whyte, E.M.; Nebes, R.D.; Begley, A.E.; Dew, M.A.; Mulsant, B.H.; Zmuda, M.D.; Bhalla, R.; Meltzer, C.C.; Pollock, B.G.; et al. The nature and determinants of neuropsychological functioning in late-life depression. Arch. Gen. Psychiatry 2004, 61, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, S.S.; Kanellopoulos, D.; Manning, K.J.; Alexopoulos, G.S. Diagnosis and treatment of depression and cognitive impairment in late life. Ann. N. Y. Acad. Sci. 2015, 1345, 36–46. [Google Scholar] [CrossRef] [PubMed]
- De Assis Faria, C.; Alves, H.V.D.; Barbosa, E.N.B.E.; Charchat-Fichman, H. Cogbnitive deficits in older adults with mild cognitive impairment in a two-year follow-up study. Dement. Neuropsychol. 2018, 12, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Huang, C.; Zhao, K.; Ma, L.; Qiu, X.; Zhang, L.; Xiu, Y.; Chen, L.; Lu, W.; Huang, C.; et al. Depression as a risk factor for dementia and mild cognitive impairment: A meta-analysis of longitudinal studies. Int. J. Geriatr. Psychiatry 2013, 28, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Diniz, B.S.; Butters, M.A.; Albert, S.M.; Dew, M.A.; Reynolds, C.F., 3rd. Late-life depression and risk of vascular dementia and Alzheimer’s disease: Systematic review and meta-analysis of community-based cohort studies. Br. J. Psychiatry 2013, 202, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Makino, K.; Suzuki, T. Comorbid Mild Cognitive Impairment and Depressive Symptoms Predict Future Dementia in Community Older Adults: A 24-Month Follow-Up Longitudinal Study. J. Alzheimers Dis. 2016, 54, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Frisardi, V.; Capurso, C.; D’Introno, A.; Colacicco, A.M.; Imbimbo, B.P.; Santamato, A.; Vendemiale, G.; Seripa, D.; Pilotto, A.; et al. Late-life depression, mild cognitive impairment, and dementia: Possible continuum? Am. J. Geriatr. Psychiatry 2010, 18, 98–116. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, G.S.; Meyers, B.S.; Young, R.C.; Mattis, S.; Kakuma, T. The course of geriatric depression with “reversible dementia”: A controlled study. Am. J. Psychiatry 1993, 150, 1693–1699. [Google Scholar] [PubMed]
- Sarica, A.; Cerasa, A.; Quattrone, A.; Calhoun, V. Editorial on special issue: Machine learning on MCI. J. Neurosci. Methods 2018, 302, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.J.; Andreescu, C.; Price, J.C.; Edelman, K.L.; Reynolds, C.F., 3rd; Aizenstein, H.J. Machine learning approaches for integrating clinical and imaging features in late-life depression classification and response prediction. Int. J. Geriatr. Psychiatry 2015, 30, 1056–1067. [Google Scholar] [CrossRef] [PubMed]
- Zilcha-Mano, S.; Roose, S.P.; Brown, P.J.; Rutherford, B.R. A Machine Learning Approach to Identifying Placebo Responders in Late-Life Depression Trials. Am. J. Geriatr. Psychiatry 2018, 26, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.L.; Paradise, M.; Hickie, I.B.; Lewis, S.J.G.; Naismith, S.L.; Lagopoulos, J. Cognitive impairment with and without depression history: An analysis of white matter microstructure. J. Psychiatry Neurosci. 2014, 39, 135–143. [Google Scholar] [PubMed]
- Richard, E.; Reitz, C.; Honig, L.H.; Schupf, N.; Tang, M.X.; Manly, J.J.; Mayeux, R.; Devanand, D.; Luchsinger, J.A. Late-life depression, mild cognitive impairment, and dementia. JAMA Neurol. 2013, 70, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.; Zhang, X.; Shu, H.; Wang, Z.; Liu, D.; Zhang, Z. The characteristic of cognitive dysfunction in remitted late life depression and amnestic mild cognitive impairment. Psychiatry Res. 2017, 251, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Lebedeva, A.K.; Westman, E.; Borza, T.; Beyer, M.K.; Engedal, K.; Aarsland, D.; Selbaek, G.; Haberg, A.K. MRI-Based Classification Models in Prediction of Mild Cognitive Impairment and Dementia in Late-Life Depression. Front. Aging Neurosci. 2017, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.M. Neural Networks for Pattern Recognition; Clarendon Press: Gloucestershire, UK, 1995; ISBN 9780198538646. [Google Scholar]
- Quintana, M.; Guàrdia, J.; Sánchez-Benavides, G.; Aguilar, M.; Molinuevo, J.L.; Robles, A.; Barquero, M.S.; Antúnez, C.; Martínez-Parra, C.; Frank-García, A.; et al. Using artificial neural networks in clinical neuropsychology: High performance in mild cognitive impairment and Alzheimer’s disease. J. Clin. Exp. Neuropsychol. 2012, 34, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, P.J.; Taktak, A.F.G. The use of artificial neural networks in decision support in cancer: A systematic review. Neural Netw. 2006, 19, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Erkaymaz, O.; Ozer, M.; Perc, M. Performance of small-world feedforward neural networks for the diagnosis of diabetes. Appl. Math. Comput. 2017, 311, 22–28. [Google Scholar] [CrossRef]
- Çelik, G.; Baykan, Ö.K.; Kara, Y.; Tireli, H. Predicting 10-day mortality in patients with strokes using neural networks and multivariate statistical methods. J. Stroke Cerebrovasc. Dis. 2014, 23, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Ion-Mărgineanu, A.; Kocevar, G.; Stamile, C.; Sima, D.M.; Durand-Dubief, F.; Van Huffel, S.; Sappey-Marinier, D. A Comparison of Machine Learning Approaches for Classifying Multiple Sclerosis Courses Using MRSI and Brain Segmentations. In Artificial Neural Networks and Machine Learning—ICANN 2017; Springer: Cham, Switzerland, 2017; pp. 643–651. [Google Scholar]
- Valverde, S.; Cabezas, M.; Roura, E.; González-Villà, S.; Pareto, D.; Vilanova, J.C.; Ramió-Torrentà, L.; Rovira, À.; Oliver, A.; Lladó, X. Improving automated multiple sclerosis lesion segmentation with a cascaded 3D convolutional neural network approach. Neuroimage 2017, 155, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Peker, M.; Sen, B.; Delen, D. Computer-Aided Diagnosis of Parkinson’s Disease Using Complex-Valued Neural Networks and mRMR Feature Selection Algorithm. J. Healthc. Eng. 2015, 6, 281–302. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Rivero, D.; Pazos, A. Epileptic seizure detection using multiwavelet transform based approximate entropy and artificial neural networks. J. Neurosci. Methods 2010, 193, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Kocadagli, O.; Langari, R. Classification of EEG signals for epileptic seizures using hybrid artificial neural networks based wavelet transforms and fuzzy relations. Expert Syst. Appl. 2017, 88, 419–434. [Google Scholar] [CrossRef]
- Payan, A.; Montana, G. Predicting Alzheimer’s disease: A neuroimaging study with 3D convolutional neural networks. arXiv 2015, arXiv:1502.02506. [Google Scholar]
- Munteanu, C.R.; Fernandez-Lozano, C.; Mato Abad, V.; Pita Fernández, S.; Álvarez-Linera, J.; Hernández-Tamames, J.A.; Pazos, A. Classification of mild cognitive impairment and Alzheimer’s Disease with machine-learning techniques using 1H Magnetic Resonance Spectroscopy data. Expert Syst. Appl. 2015, 42, 6205–6214. [Google Scholar] [CrossRef]
- Basaia, S.; Agosta, F.; Wagner, L.; Magnani, G.; Filippi, M. Automatic classification of patients with Alzheimer’s disease (AD) and mild cognitive impairment (MCI) who will convert to AD using deep neural networks (P3.179). Neurology 2018, 90, P3.179. [Google Scholar]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Peña-Casanova, J.; Quiñones-Ubeda, S.; Quintana-Aparicio, M.; Aguilar, M.; Badenes, D.; Molinuevo, J.L.; Torner, L.; Robles, A.; Barquero, M.S.; Villanueva, C.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Norms for verbal span, visuospatial span, letter and number sequencing, trail making test, and symbol digit modalities test. Arch. Clin. Neuropsychol. 2009, 24, 321–341. [Google Scholar] [CrossRef] [PubMed]
- Appollonio, I.; Leone, M.; Isella, V.; Piamarta, F.; Consoli, T.; Villa, M.L.; Forapani, E.; Russo, A.; Nichelli, P. The Frontal Assessment Battery (FAB): Normative values in an Italian population sample. Neurol. Sci. 2005, 26, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Peña-Casanova, J.; Quiñones-Ubeda, S.; Gramunt-Fombuena, N.; Quintana-Aparicio, M.; Aguilar, M.; Badenes, D.; Cerulla, N.; Molinuevo, J.L.; Ruiz, E.; Robles, A.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Norms for verbal fluency tests. Arch. Clin. Neuropsychol. 2009, 24, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Benedet, M.J. TAVEC: Test de Aprendizaje Verbal España-Complutense; TEA: Madrid, Spain, 1998; ISBN 9788471745293. [Google Scholar]
- Peña-Casanova, J.; Gramunt-Fombuena, N.; Quiñones-Úbeda, S.; Sánchez-Benavides, G.; Aguilar, M.; Badenes, D.; Molinuevo, J.L.; Robles, A.; Barquero, M.S.; Payno, M.; et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Norms for the Rey-Osterrieth Complex Figure (Copy and Memory), and Free and Cued Selective Reminding Test. Arch. Clin. Neuropsychol. 2009, 24, 371–393. [Google Scholar] [CrossRef] [PubMed]
- Peña-Casanova, J.; Guardia, J.; Bertran-Serra, I.; Manero, R.M.; Jarne, A. Versión abreviada del test Barcelona (I): Subtests y perfiles normales. Neurología 1997, 12, 99–111. [Google Scholar] [PubMed]
- Calero, M.D.; Arnedo, M.L.; Navarro, E.; Ruiz-Pedrosa, M.; Carnero, C. Usefulness of a 15-item version of the Boston Naming Test in neuropsychological assessment of low-educational elders with dementia. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P187–P191. [Google Scholar] [CrossRef] [PubMed]
- Møller, M.F. A scaled conjugate gradient algorithm for fast supervised learning. Neural Netw. 1993, 6, 525–533. [Google Scholar] [CrossRef]
- Abdi, H.; Willians, L.J. Tukey’s Honestly Significant Difference (HSD) Test. In Encyclopedia of Research Design; Sage: Thousand Oaks, CA, USA, 2010; pp. 1–5. [Google Scholar]
- Ramírez-Morales, I.; Fernández-Blanco, E.; Rivero, D.; Pazos, A. Automated early detection of drops in commercial egg production using neural networks. Br. Poult. Sci. 2017, 58, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Elderkin-Thompson, V.; Mintz, J.; Haroon, E.; Lavretsky, H.; Kumar, A. Executive dysfunction and memory in older patients with major and minor depression. Arch. Clin. Neuropsychol. 2007, 22, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Lamar, M.; Charlton, R.; Zhang, A.; Kumar, A. Differential associations between types of verbal memory and prefrontal brain structure in healthy aging and late life depression. Neuropsychologia 2012, 50, 1823–1829. [Google Scholar] [CrossRef] [PubMed]
- Salvadori, E.; Dieci, F.; Caffarra, P.; Pantoni, L. Qualitative Evaluation of the Immediate Copy of the Rey-Osterrieth Complex Figure: Comparison between Vascular and Degenerative MCI Patients. Arch. Clin. Neuropsychol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.D.; Aizenstein, H.J.; Alexopoulos, G.S. The vascular depression hypothesis: Mechanisms linking vascular disease with depression. Mol. Psychiatry 2013, 18, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Samara, Z.; Evers, E.A.T.; Peeters, F.; Uylings, H.B.M.; Rajkowska, G.; Ramaekers, J.G.; Stiers, P. Orbital and Medial Prefrontal Cortex Functional Connectivity of Major Depression Vulnerability and Disease. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, G.S.; Hoptman, M.J.; Kanellopoulos, D.; Murphy, C.F.; Lim, K.O.; Gunning, F.M. Functional connectivity in the cognitive control network and the default mode network in late-life depression. J. Affect. Disord. 2012, 139, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.Q.; Himali, J.J.; Wolf, P.A.; DeCarli, D.C.; Beiser, A.; Au, R. Effects of white matter integrity and brain volumes on late life depression in the Framingham Heart Study. Int. J. Geriatr. Psychiatry 2017, 32, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA Publishing: Washington, DC, USA, 2013. [Google Scholar]


{kind=link}
| Clinical Features | LLD | MCI |
|---|---|---|
| Diagnostic criteria | Clinically significant alteration of mood Beginning in the elderly (>50 years) | Clinically significant CI determined by the presence of alteration of −1.5 SD below the average in one or more cognitive areas. |
| Other symptoms | Can present subjective memory impairment or MCI | Can or cannot present mood disturbance, apathy, anxiety, or mild behavioral impairment |
| Daily life activities | Can give up doing complex instrumental activities for motivational reasons or apathy. | Can present difficulties or have delegated complex instrumental activities to others but does not meet criteria for dementia. |
| Etiology | Psychological factors: motivation, social isolation, stressors, etc./Biological factors: alteration of white matter, brain volume, etc. | Biological factors: vascular small vessel disease (alteration of white matter), early signs of Alzheimer’s disease, etc. |
| Variables | MCI with Depression | MCI without Depression | F | p Value |
|---|---|---|---|---|
| Digit Span Forward | 0.20 ± 0.89 | 0.16 ± 0.74 | 0.04 | 0.845 |
| Digit Span Backward | −0.10 ± 0.96 | 0.53 ± 0.63 | 9.26 | 0.004 |
| TMT A | −0.48 ± 1.05 | −0.31 ± 0.82 | 0.49 | 0.484 |
| FAB | −1.95 ± 1.99 | −2.35 ± 1.71 | 0.67 | 0.416 |
| Verbal fluency P | −0.51 ± 0.66 | −0.49 ± 0.73 | 0.01 | 0.945 |
| Verbal fluency animals | −0.81 ± 0.85 | −1.06 ± 0.72 | 1.41 | 0.240 |
| TAVEC immediate memory | −0.84 ± 1.05 | −1.67 ± 0.62 | 14.31 | <0.001 |
| TAVEC short-term free recall | −0.77 ± 1.07 | −1.81 ± 1.07 | 13.25 | <0.001 |
| TAVEC memory (short-term cued recall) | −0.48 ± 0.93 | −1.71 ± 0.96 | 23.22 | <0.001 |
| TAVEC long-term free recall | −0.86 ± 1.02 | −2.10 ± 1.00 | 21.10 | <0.001 |
| TAVEC memory (long-term cued recall) | −0.65 ± 1.02 | −2.14 ± 0.96 | 31.70 | <0.001 |
| TAVEC recognition | −0.57 ± 0.96 | −1.33 ± 1.12 | 7.07 | 0.010 |
| Rey–OCF (memory) | −0.58 ± 0.93 | −0.63 ± 0.88 | 0.04 | 0.838 |
| Rey–OCF (copy) | −0.52 ± 0.76 | −0.08 ± 0.51 | 7.11 | 0.010 |
| a-BT praxis | −0.69 ± 2.22 | −0.60 ± 1.96 | 0.029 | 0.865 |
| a-BT praxis bimanual | −0.57 ± 2.11 | −0.67 ± 3.04 | 0.02 | 0.900 |
| a-BT command | −0.32 ± 1.25 | −0.05 ± 0.84 | 0.97 | 0.329 |
| Net. Archit. | Accuracy | Sensitivity | Specificity | AUC | ||||
|---|---|---|---|---|---|---|---|---|
| Substudy 1 | Substudy 2 | Substudy 1 | Substudy 2 | Substudy 1 | Substudy 2 | Substudy 1 | Substudy 2 | |
| {3} | 0.75 ac ± 0.17 | 0.69 ac ± 0.11 | 0.72 ac ± 0.31 | 0.77 a ± 0.24 | 0.88 a ± 0.20 | 0.74 abc ± 0.19 | 0.93 a ± 0.07 | 0.89 a ± 0.10 |
| {8} | 0.78 ac ± 0.18 | 0.79 bc ± 0.15 | 0.69 ac ± 0.31 | 0.80 a ± 0.26 | 0.85 a ± 0.27 | 0.79 abd ± 0.24 | 0.94 a ± 0.04 | 0.92 a ± 0.08 |
| {12} | 0.78 ac ± 0.20 | 0.73 ac ± 0.17 | 0.76 ac ± 0.21 | 0.75 a ± 0.33 | 0.80 a ± 0.32 | 0.78 abd ± 0.21 | 0.94 a ± 0.06 | 0.91 a ± 0.07 |
| {15} | 0.86 b ± 0.19 | 0.74 ac ± 0.08 | 0.82 b ± 0.32 | 0.79 a ± 0.32 | 0.89 a± 0.17 | 0.68 ac ± 0.26 | 0.95 a ± 0.05 | 0.90 a ± 0.06 |
| {5 3} | 0.76 ac ± 0.16 | 0.80 b ± 0.12 | 0.88 bc ± 0.21 | 0.73 ab ± 0.25 | 0.69 b ± 0.27 | 0.84 bd ± 0.21 | 0.93 a ± 0.04 | 0.93 a ± 0.07 |
| {8 5} | 0.71 c ± 0.22 | 0.71 ac ± 0.16 | 0.76 ac ±0.31 | 0.75 a ± 0.29 | 0.67 b ± 0.33 | 0.68 ac ± 0.25 | 0.92 a ± 0.07 | 0.90 a ± 0.04 |
| {10 8} | 0.76 ac ± 0.19 | 0.70 ac ± 0.20 | 0.68 ac ± 0.39 | 0.68 ab ± 0.32 | 0.78 a ± 0.22 | 0.66 ac ± 0.34 | 0.92 a ± 0.04 | 0.90 a ± 0.10 |
| {12 10} | 0.79 b ± 0.15 | 0.71 ac ± 0.22 | 0.83 bc ± 0.18 | 0.62 b ± 0.38 | 0.83 a ± 0.19 | 0.86 bd ± 0.16 | 0.92 a ± 0.09 | 0.90 a ± 0.08 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mato-Abad, V.; Jiménez, I.; García-Vázquez, R.; Aldrey, J.M.; Rivero, D.; Cacabelos, P.; Andrade-Garda, J.; Pías-Peleteiro, J.M.; Rodríguez-Yáñez, S. Using Artificial Neural Networks for Identifying Patients with Mild Cognitive Impairment Associated with Depression Using Neuropsychological Test Features. Appl. Sci. 2018, 8, 1629. https://doi.org/10.3390/app8091629
Mato-Abad V, Jiménez I, García-Vázquez R, Aldrey JM, Rivero D, Cacabelos P, Andrade-Garda J, Pías-Peleteiro JM, Rodríguez-Yáñez S. Using Artificial Neural Networks for Identifying Patients with Mild Cognitive Impairment Associated with Depression Using Neuropsychological Test Features. Applied Sciences. 2018; 8(9):1629. https://doi.org/10.3390/app8091629
Chicago/Turabian StyleMato-Abad, Virginia, Isabel Jiménez, Rafael García-Vázquez, José M. Aldrey, Daniel Rivero, Purificación Cacabelos, Javier Andrade-Garda, Juan M. Pías-Peleteiro, and Santiago Rodríguez-Yáñez. 2018. "Using Artificial Neural Networks for Identifying Patients with Mild Cognitive Impairment Associated with Depression Using Neuropsychological Test Features" Applied Sciences 8, no. 9: 1629. https://doi.org/10.3390/app8091629
APA StyleMato-Abad, V., Jiménez, I., García-Vázquez, R., Aldrey, J. M., Rivero, D., Cacabelos, P., Andrade-Garda, J., Pías-Peleteiro, J. M., & Rodríguez-Yáñez, S. (2018). Using Artificial Neural Networks for Identifying Patients with Mild Cognitive Impairment Associated with Depression Using Neuropsychological Test Features. Applied Sciences, 8(9), 1629. https://doi.org/10.3390/app8091629