Intra-Oral 3D Scanning for the Digital Evaluation of Dental Arch Parameters



Abstract
1. Introduction
2. Methods
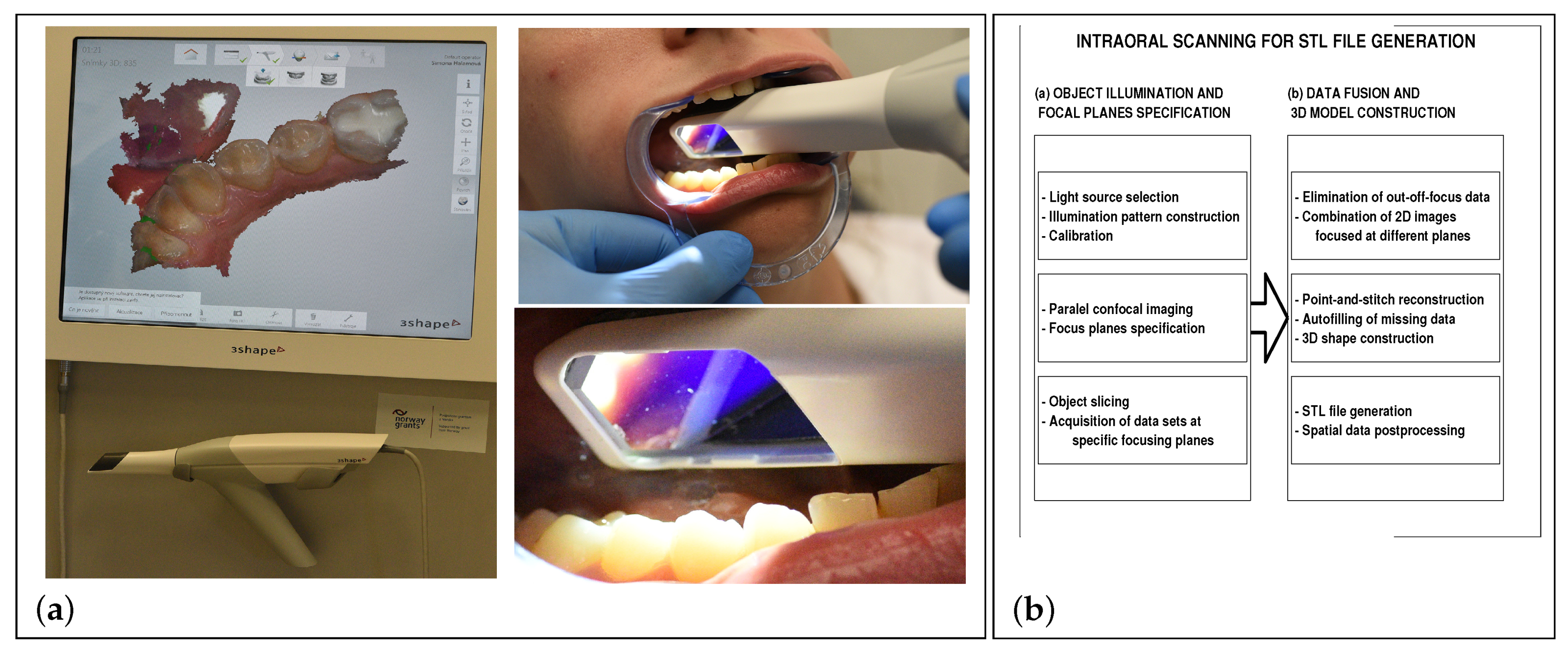
2.1. Data Acquisition
- (a)
- Visualisation of the STL data allowing the surface model rotation and its detailed study from different view-points,
- (b)
- The STL data transform and the spatial model construction in the selected coordinate system enabling application of specific mathematical methods for data processing,
- (c)
- The detailed 3D model and contour plot construction of all teeth allowing detection of specific surface areas for further processing and evaluation of dental arch parameters.
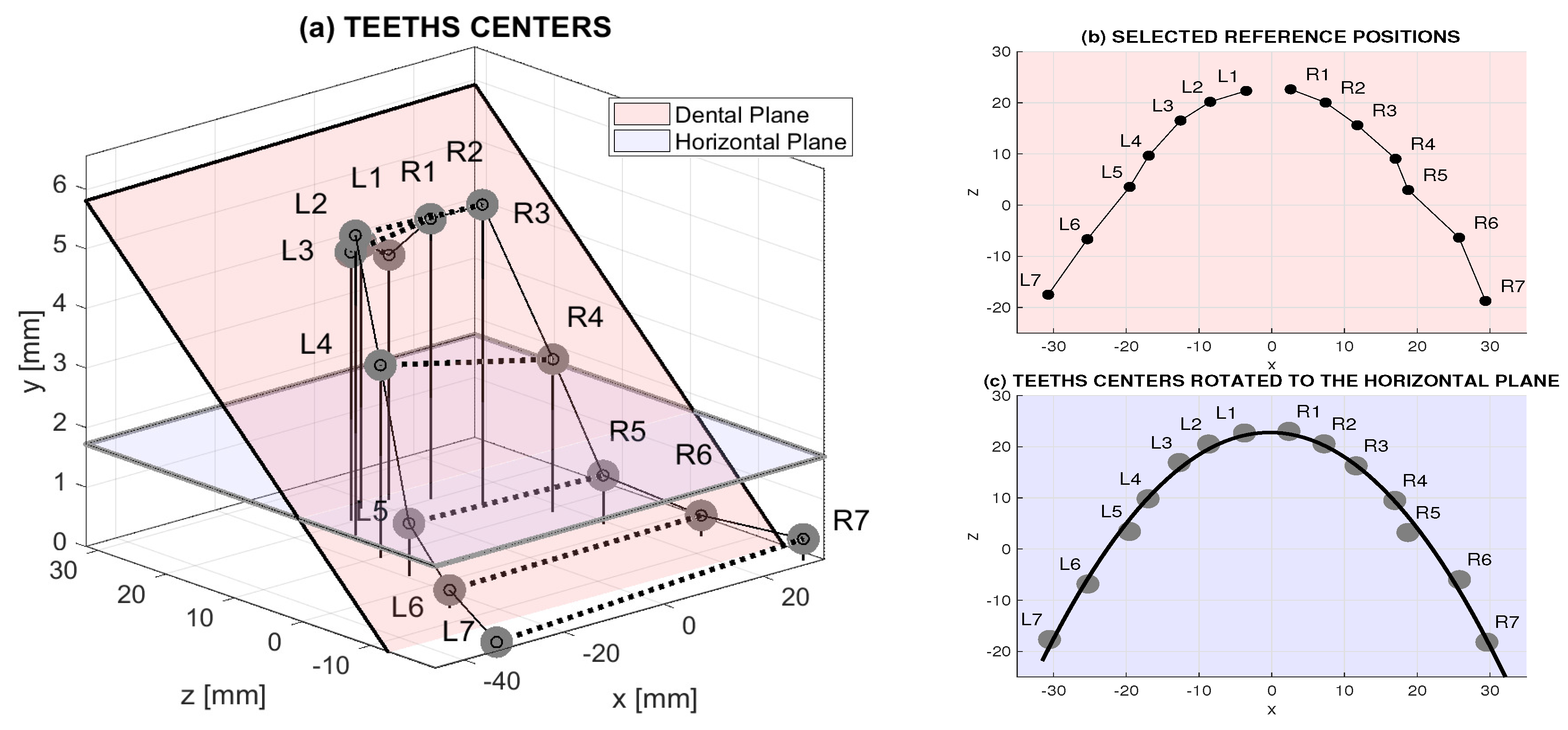
2.2. Data Processing
- Data acquisition, their visualisation and transform into the 3D space in the selected coordinate system,
- Data preprocessing using linear and nonlinear filters to reject noise components,
- Estimation of the dental plane defined by tops of individual teeth using the least square method,
- 3D data rotation into the horizontal plane and image registration,
- The use of the digital model for evaluation of selected dental arch parameters.
3. Results
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kašparová, M.; Gráfová, L.; Dvořák, P.; Dostálová, T.; Procházka, A.; Eliášová, H.; Pruša, J.; Kakawand, S. Possibility of reconstruction of dental plaster cast from 3D digital study models. BioMed. Eng. OnLine 2013, 12, 49. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Reddy, K.; Reddy, M.; Shah, S. Evaluation of virtual models (3Shape OrthoSystem) in assessing accuracy and duration of model analyses based on the severity of crowding. Saudi J. Dent. Res. 2017, 8, 11–18. [Google Scholar] [CrossRef]
- van der Meer, W.; Andriessen, F.; Wismeijer, D.; Ren, Y. Application of intra-oral dental scanners in the digital workflow of Implantology. PLoS ONE 2012, 7, e43312. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, Y.; Zhang, Y. Use of intraoral scanning and 3-dimensional printing in the fabrication of a removable partial denture for a patient with limited mouth opening. J. Am. Dent. Assoc. 2017, 148, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Barone, S.; Paoli, A.; Razionale, A. Creation of 3D multi-body orthodontic models by using independent imaging sensors. Sensors 2013, 13, 2033–2050. [Google Scholar] [CrossRef] [PubMed]
- Vogtlin, C.; Schulz, G.; Jager, K.; Muller, B. Comparing the accuracy of master models based on digital intra-oral scanners with conventional plaster casts. Phys. Med. 2016, 1, 20–26. [Google Scholar] [CrossRef]
- Logozzo, S.; Zanetti, E.; Franceschini, G.; Kilpela, A.; Makinen, A. Recent advances in dental optics—Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Jacob, H.; Wyatt, G.; Buschang, P. Reliability and validity of intraoral and extraoral scanners. Prog. Orthod. 2015, 16, 38. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.; Marti, B.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Kašparová, M.; Procházka, A.; Gráfová, L.; Yadollahi, M.; Vyšata, O.; Dostálová, T. Evaluation of dental morphometrics during the orthodontic treatment. BioMed. Eng. OnLine 2014, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed]
- Yadollahi, M.; Procházka, A.; Kašparová, M.; Vyšata, O.; Mařík, V. Separation of overlapping dental arch objects using digital records of illuminated plaster casts. BioMed. Eng. OnLine 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, E.M.; Bignardi, C. Chapter VI: Structural Analysis of Skeletal Body Elements: Numerical and Experimental Methods. In Biomechanical Systems Technology, Volume 3 Muscular Skeletal Systems; Leondes, C.T., Ed.; World Scientific Publishing Company: London, UK, 2009; pp. 185–225. [Google Scholar]
- Procházka, A.; Kašparová, M.; Yadollahi, M.; Vyšata, O.; Grajciarová, L. Multi-camera systems use for dental arch shape measurement. Visual Comput. 2015, 31, 1501–1509. [Google Scholar] [CrossRef]
- Yadollahi, M.; Procházka, A.; Kašparová, M.; Vyšata, O. The use of combined illumination in segmentation of orthodontic Bodies. Signal Image Video Process. 2015, 9, 243–250. [Google Scholar] [CrossRef]
- Mangano, F.; Veronesi, G.; Hauschild, U.; Mijiritsky, E.; Mangano, C. Trueness and precision of four intraoral scanners in oral implantology: A comparative in vitro study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Comparison of two intraoral scanners based on three-dimensional surface analysis. Prog. Orthod. 2018, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.; Fages, M.; Ducret, M. Intraoral scanner technologies: A review to make a successful impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, N.; Groth, C.; Jones, P.; Graham, J.; Redmond, W. Intraoral digital scanners. J. Clin. Orthod. 2014, 48, 337–347. [Google Scholar] [PubMed]
- Martin, C.; Chalmers, E.; McIntyre, G.; Cochrane, H.; Mossey, P. Orthodontic scanners: What’s available? J. Orthod. 2015, 42, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Nedelcua, R.; Olssonb, P.; Nyströmb, I.; Rydénc, J.; Thora, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Logozzo, S.; Kilpel, A.; Makynen, A.; Zanetti, E.M.; Franceschini, G. Recent advances in dental optics—Part II: Experimental tests for a new intraoral scanner. Opt. Lasers Eng. 2014, 54, 187–196. [Google Scholar] [CrossRef]
- Zarauz, C.; Valverde, A.; Martinez-Rus, F.; Hassan, B.; Pradies, G. Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions. Clin. Oral Investig. 2016, 20, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Ortega, U.; Dirckx, J.; Meneses-Fabian, C. Fully automated low-cost setup for fringe projection profilometry. Appl. Opt. 2015, 54, 1350–1353. [Google Scholar] [CrossRef] [PubMed]
- Koopaie, M.; Kolahdouz, S. Three-dimensional simulation of human teeth and its application in dental education and research. Med. J. Islam Repub. Iran 2016, 30, 461. [Google Scholar] [PubMed]
- Hošťálková, E.; Vyšata, O.; Procházka, A. Multi-dimensional biomedical image de-noising using Haar transform. In Proceedings of the 15th International Conference on Digital Signal Processing, Cardiff, UK, 1–4 July 2007; pp. 175–179. [Google Scholar]
- Jerhotová, E.; Švihlík, J.; Procházka, A. Biomedical Image Volumes Denoising via the Wavelet Transform. In Applied Biomedical Engineering; INTECH: London, UK, 2011; pp. 435–458. [Google Scholar]
- Chun, J.; Tahk, J.; Chun, Y.; Park, J.; Kim, M. Analysis on the accuracy of intraoral scanners: The effects of mandibular anterior interdental space. Appl. Sci. 2017, 7, 719. [Google Scholar] [CrossRef]
- Hong-Seoka, P.; Chintal, S. Development of high speed and high accuracy 3D dental intra oral scanner. Procedia Eng. 2015, 100, 1174–1181. [Google Scholar] [CrossRef]
- Ahn, J.; Park, A.; Kim, J.; Lee, B.; Eom, J. Development of three-dimensional dental scanning apparatus using structured illumination. Sensors 2017, 17, 1634. [Google Scholar] [CrossRef] [PubMed]
- Logozzo, S.; Franceschini, A.; Kilpela, A.; Caponi, M.; Governi, L.; Blois, L. A comparative analysis of intraoral 3D digital scanners for restorative dentistry. Internet J. Med. Technol. 2011, 5, 1–18. [Google Scholar]
- Cali, M.; Oliveri, S.M.; Ambu, R.; Fichera, G. An Integrated Approach to Characterize the Dynamic Behaviour of a Mechanical Chain Tensioner by Functional Tolerancing. J. Mech. Eng. 2018, 64, 245–257. [Google Scholar]
- Nedelcu, R.; Olsson, P.; Nystrom, I.; Thor, A. Finish line distinctness and accuracy in 7 intraoral scanners versus conventional impression: an in vitro descriptive comparison. BMC Oral Res. 2018, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Goshtasby, A. Image Registration: Principles, Tools and Methods; Springer: Berlin, Germany, 2012. [Google Scholar]
- Hajnal, J.; Hawkes, D.; Hill, D.; Hajnal, J. Medical Image Registration; CRC Press: Boca Raton, FL, USA, 2001. [Google Scholar]
- Modersitzki, J. Numerical Methods for Image Registration; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Zanetti, E.M.; Aldieri, A.; Terzini, M.; Calì, M.; Franceschini1, J.; Bignardi, C. Additively manufactured custom load-bearing implantable devices: grounds for caution. Aust. Med. J. ASM 2017, 10, 694–700. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lower Dental Arch Distances [mm] | Upper Dental Arch Distances [mm] | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Exp. | L3-R3 | L4-R4 | L5-R5 | L3-R3 | L4-R4 | L5-R5 | |||||||
| O | R | O | R | O | R | O | R | O | R | O | R | ||
| 1 | 24.43 | 24.45 | 34.14 | 34.40 | 38.17 | 38.29 | 35.19 | 35.23 | 42.59 | 42.61 | 50.08 | 50.09 | |
| 2 | 24.38 | 24.47 | 33.82 | 34.20 | 38.19 | 38.90 | 35.06 | 35.67 | 42.63 | 43.06 | 49.65 | 50.14 | |
| 3 | 24.24 | 24.74 | 33.86 | 34.05 | 37.69 | 38.51 | 35.16 | 35.21 | 42.16 | 42.27 | 50.12 | 50.37 | |
| 4 | 24.45 | 24.50 | 33.60 | 34.27 | 37.73 | 38.24 | 34.89 | 35.30 | 42.31 | 42.43 | 49.17 | 49.28 | |
| 5 | 24.37 | 24.43 | 33.84 | 34.09 | 37.47 | 38.37 | 35.17 | 35.68 | 42.19 | 42.86 | 49.60 | 49.34 | |
| 6 | 24.14 | 24.38 | 34.08 | 34.31 | 37.88 | 38.39 | 35.08 | 35.28 | 42.38 | 42.45 | 50.13 | 50.41 | |
| 7 | 24.17 | 24.42 | 33.78 | 34.09 | 37.64 | 38.36 | 34.85 | 35.62 | 42.36 | 42.58 | 49.05 | 50.94 | |
| 8 | 24.16 | 24.36 | 34.17 | 34.24 | 38.07 | 38.66 | 34.98 | 35.43 | 42.43 | 42.67 | 49.62 | 50.02 | |
| 9 | 24.26 | 24.56 | 34.17 | 34.15 | 38.16 | 38.62 | 34.61 | 35.03 | 42.48 | 42.54 | 49.11 | 49.45 | |
| 10 | 24.43 | 24.47 | 34.16 | 34.21 | 38.31 | 38.56 | 35.15 | 35.36 | 42.55 | 42.71 | 49.86 | 49.94 | |
| 11 | 24.14 | 24.47 | 34.11 | 34.16 | 38.07 | 38.24 | 34.76 | 35.06 | 42.13 | 42.23 | 49.47 | 50.29 | |
| 12 | 24.11 | 24.73 | 33.67 | 34.17 | 37.67 | 38.61 | 34.16 | 34.18 | 41.82 | 43.05 | 49.03 | 49.68 | |
| 13 | 24.46 | 24.58 | 34.09 | 34.18 | 38.10 | 38.44 | 35.12 | 35.17 | 42.59 | 42.82 | 50.16 | 50.26 | |
| 14 | 24.19 | 24.64 | 33.92 | 34.02 | 38.01 | 38.70 | 35.32 | 35.57 | 41.75 | 42.53 | 49.91 | 49.99 | |
| 15 | 24.26 | 24.63 | 34.12 | 34.29 | 37.96 | 38.77 | 34.52 | 35.94 | 42.54 | 42.61 | 49.86 | 50.18 | |
| 16 | 24.35 | 24.45 | 34.13 | 34.15 | 38.04 | 38.24 | 35.02 | 35.13 | 42.40 | 42.86 | 49.73 | 49.84 | |
| 17 | 24.29 | 24.36 | 34.01 | 34.13 | 38.11 | 38.62 | 34.93 | 35.27 | 42.81 | 42.91 | 50.08 | 50.13 | |
| 18 | 24.19 | 24.67 | 33.96 | 34.28 | 37.91 | 38.44 | 35.26 | 35.58 | 41.76 | 41.97 | 49.23 | 49.55 | |
| 19 | 24.38 | 24.41 | 34.08 | 34.37 | 37.87 | 38.49 | 34.64 | 34.83 | 42.55 | 42.78 | 49.42 | 50.14 | |
| 20 | 24.27 | 24.42 | 34.01 | 34.36 | 38.08 | 38.68 | 34.21 | 34.67 | 42.23 | 42.39 | 49.88 | 49.92 | |
| MEAN: | 24.29 | 24.51 | 33.99 | 34.21 | 37.98 | 38.51 | 34.90 | 35.26 | 42.33 | 42.62 | 49.66 | 50.00 | |
| STD: | 0.12 | 0.11 | 0.17 | 0.11 | 0.19 | 0.19 | 0.33 | 0.28 | 0.30 | 0.28 | 0.39 | 0.40 | |
| CV [%]: | 0.49 | 0.45 | 0.50 | 0.32 | 0.49 | 0.49 | 0.95 | 0.79 | 0.71 | 0.66 | 0.79 | 0.80 | |
| Lower Dental Arch Measures | Upper Dental Arch Measures | ||||||
|---|---|---|---|---|---|---|---|
| L3-R3 | L4-R4 | L5-R5 | L3-R3 | L4-R4 | L5-R5 | ||
| MEAN [mm]: | 24.51 | 34.21 | 38.51 | 35.26 | 42.62 | 50.00 | |
| MEAN change [%]: | +0.91 | +0.65 | +1.40 | +1.03 | +0.69 | +0.68 | |
| STD [mm]: | 0.11 | 0.11 | 0.19 | 0.28 | 0.28 | 0.40 | |
| STD change [%]: | −8.33 | −35.29 | 0 | −15.15 | −6.67 | +2.5 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kašparová, M.; Halamová, S.; Dostálová, T.; Procházka, A. Intra-Oral 3D Scanning for the Digital Evaluation of Dental Arch Parameters. Appl. Sci. 2018, 8, 1838. https://doi.org/10.3390/app8101838
Kašparová M, Halamová S, Dostálová T, Procházka A. Intra-Oral 3D Scanning for the Digital Evaluation of Dental Arch Parameters. Applied Sciences. 2018; 8(10):1838. https://doi.org/10.3390/app8101838
Chicago/Turabian StyleKašparová, Magdaléna, Simona Halamová, Taťjana Dostálová, and Aleš Procházka. 2018. "Intra-Oral 3D Scanning for the Digital Evaluation of Dental Arch Parameters" Applied Sciences 8, no. 10: 1838. https://doi.org/10.3390/app8101838
APA StyleKašparová, M., Halamová, S., Dostálová, T., & Procházka, A. (2018). Intra-Oral 3D Scanning for the Digital Evaluation of Dental Arch Parameters. Applied Sciences, 8(10), 1838. https://doi.org/10.3390/app8101838