


Circulating Cell-Free Mitochondrial DNA and Inflammation in Older Adults with Pancreatic Cancer: Results from an Exploratory Study

 , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Blood Collection and Processing
2.3. Quantification of Circulating Cell-Free Mitochondrial DNA by Droplet Digital PCR
2.4. Quantification of Circulating Inflammatory Markers
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
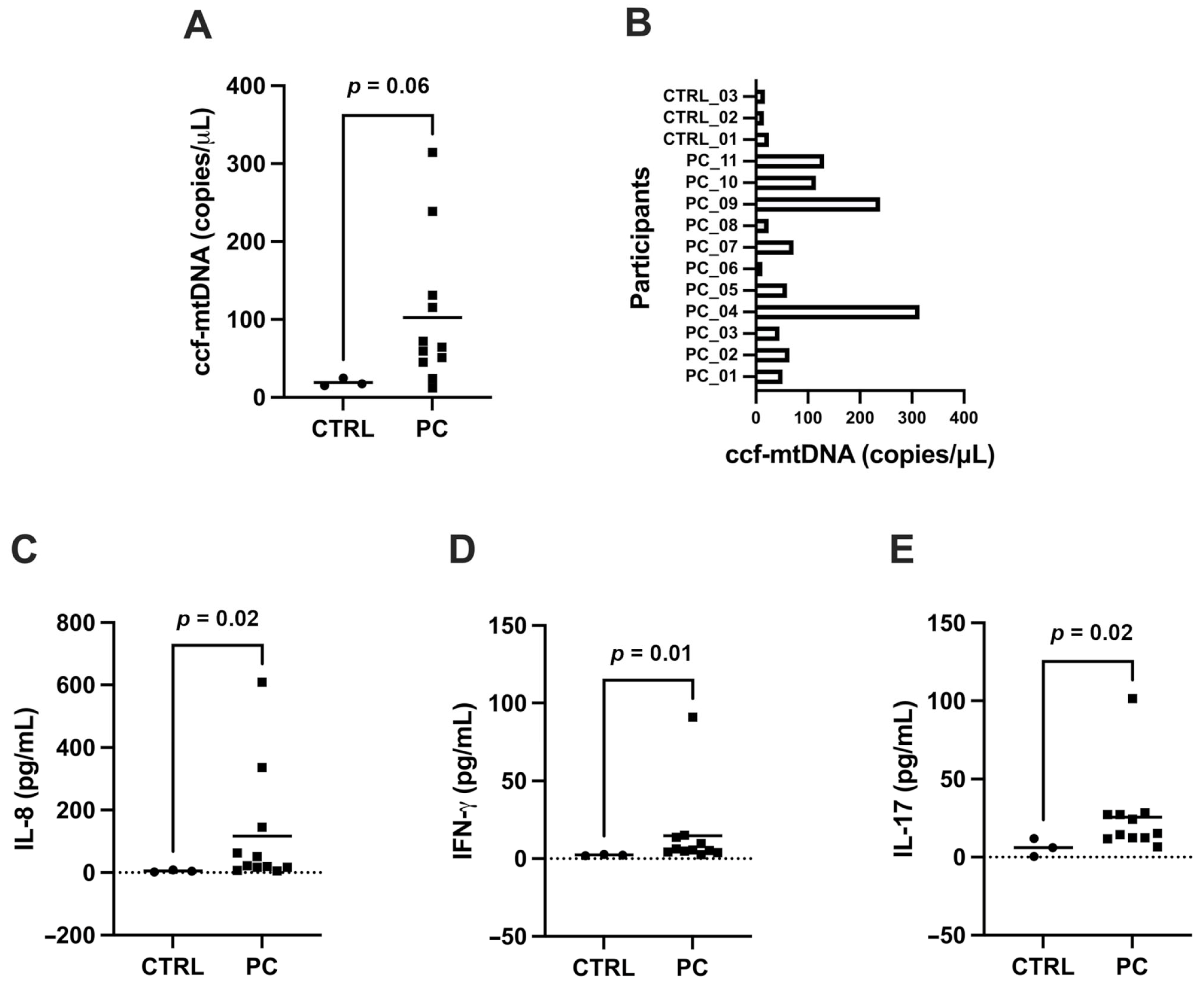
3.2. Circulating Cell-Free Mitochondrial DNA and Inflammatory Biomolecules in Pancreatic Cancer Patients and Controls
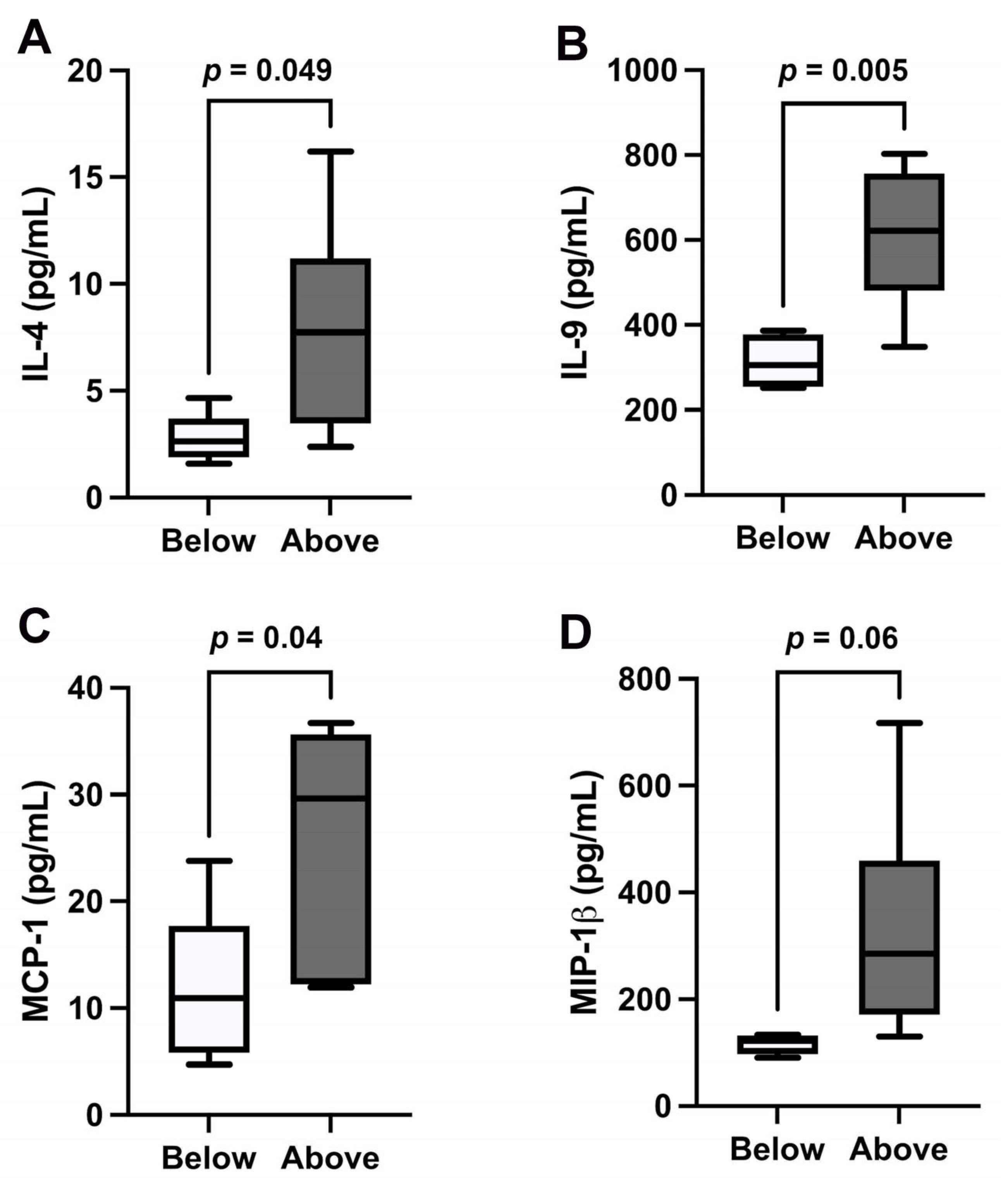
3.3. Cytokine Signatures According to Cell-Free Mitochondrial DNA Circulating Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BHQ1 | Black Hole Quencher-1 |
| ccf-mtDNA | Circulating cell-free mitochondrial DNA |
| CCL | C-C motif chemokine ligand |
| cf-mtDNA | Cell-free mitochondrial DNA |
| cGAS–STING | Cyclic GMP-AMP synthase–stimulator of interferon genes |
| CTR | Control participant |
| DAMP | Damage-associated molecular pattern |
| DCs | Dendritic cells |
| ddPCR | Droplet digital PCR |
| EVs | Extracellular vesicles |
| EXOPanc | role of EXOsomes in Pancreatic cancer progression |
| F | Forward |
| FAM | 6-carboxyfluorescein |
| FGF | Fibroblast growth factor |
| FOLFIRINOX | 5- fluorouracil with leucovorin, oxaliplatin, and irinotecan |
| G-CSF | Granulocyte colony-stimulating factor |
| GM-CSF | Granulocyte macrophage colony-stimulating factor |
| HMGB1 | High mobility group box 1 |
| IL | Interleukin |
| IL-1ra | Interleukin 1 receptor agonist |
| IP | Interferon-induced protein |
| MCP-1 | Monocyte chemoattractant protein 1 |
| MDSCs | Myeloid-derived suppressor cells |
| MIP | Macrophage inflammatory protein |
| mtDAMP | Mitochondrial damage-associated molecular pattern |
| NLRP3 | Nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3 |
| PaCa | Pancreatic cancer |
| PC | Participant with pancreatic cancer |
| PDGF-BB | Platelet derived growth factor BB |
| R | Reverse |
| SD | Standard deviation |
| TGF-β | Transforming growth factor beta |
| TLR9 | Toll-like receptor 9 |
| TME | Tumor microenvironment |
| TNF-α | Tumor necrosis factor-alpha |
| Treg | Regulatory T-lymphocytes |
| VEGF | Vascular endothelial growth factor |
References
- Bisht, S.; Feldmann, G. Novel targets in pancreatic cancer therapy—Current status and ongoing translational efforts. Oncol. Res. Treat. 2018, 41, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Deplanque, G.; Demartines, N. Pancreatic cancer: Are more chemotherapy and surgery needed? Lancet 2017, 389, 985–986. [Google Scholar] [CrossRef] [PubMed]
- Yako, Y.Y.; Kruger, D.; Smith, M.; Brand, M. Cytokines as biomarkers of pancreatic ductal adenocarcinoma: A systematic review. PLoS ONE 2016, 11, e0154016. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Brehm, C.U.; Gress, T.M.; Buchholz, M.; Alashkar Alhamwe, B.; von Strandmann, E.P.; Slater, E.P.; Bartsch, J.W.; Bauer, C.; Lauth, M. The immune microenvironment in pancreatic cancer. Int. J. Mol. Sci. 2020, 21, 7307. [Google Scholar] [CrossRef]
- Padoan, A.; Plebani, M.; Basso, D. Inflammation and pancreatic cancer: Focus on metabolism, cytokines, and immunity. Int. J. Mol. Sci. 2019, 20, 676. [Google Scholar] [CrossRef]
- Zhong, Z.; Liang, S.; Sanchez-Lopez, E.; He, F.; Shalapour, S.; Lin, X.J.; Wong, J.; Ding, S.; Seki, E.; Schnabl, B.; et al. New mitochondrial DNA synthesis enables NLRP3 inflammasome activation. Nature 2018, 560, 198–203. [Google Scholar] [CrossRef]
- West, A.P.; Khoury-Hanold, W.; Staron, M.; Tal, M.C.; Pineda, C.M.; Lang, S.M.; Bestwick, M.; Duguay, B.A.; Raimundo, N.; MacDuff, D.A.; et al. Mitochondrial DNA stress primes the antiviral innate immune response. Nature 2015, 520, 553–557. [Google Scholar] [CrossRef]
- Gao, Y.; Mi, N.; Wu, W.; Zhao, Y.; Fan, F.; Liao, W.; Ming, Y.; Guan, W.; Bai, C. Transfer of inflammatory mitochondria via extracellular vesicles from M1 macrophages induces ferroptosis of pancreatic beta cells in acute pancreatitis. J. Extracell. Vesicles 2024, 13, e12410. [Google Scholar] [CrossRef]
- West, A.P.; Shadel, G.S.; Ghosh, S. Mitochondria in innate immune responses. Nat. Rev. Immunol. 2011, 11, 389–402. [Google Scholar] [CrossRef]
- Simmons, J.D.; Lee, Y.L.; Mulekar, S.; Kuck, J.L.; Brevard, S.B.; Gonzalez, R.P.; Gillespie, M.N.; Richards, W.O. Elevated levels of plasma mitochondrial DNA DAMPs are linked to clinical outcome in severely injured human subjects. Ann. Surg. 2013, 258, 591–596; discussion 596–598. [Google Scholar] [CrossRef]
- Zhang, Q.; Raoof, M.; Chen, Y.; Sumi, Y.; Sursal, T.; Junger, W.; Brohi, K.; Itagaki, K.; Hauser, C.J. Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature 2010, 464, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.; Radpour, R.; Barekati, Z.; Asadollahi, R.; Bitzer, J.; Wight, E.; Burki, N.; Diesch, C.; Holzgreve, W.; Zhong, X.Y. Levels of plasma circulating cell free nuclear and mitochondrial DNA as potential biomarkers for breast tumors. Mol. Cancer 2009, 8, 105. [Google Scholar] [CrossRef] [PubMed]
- Ellinger, J.; Albers, P.; Muller, S.C.; von Ruecker, A.; Bastian, P.J. Circulating mitochondrial DNA in the serum of patients with testicular germ cell cancer as a novel noninvasive diagnostic biomarker. BJU Int. 2009, 104, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Ellinger, J.; Muller, D.C.; Muller, S.C.; Hauser, S.; Heukamp, L.C.; von Ruecker, A.; Bastian, P.J.; Walgenbach-Brunagel, G. Circulating mitochondrial DNA in serum: A universal diagnostic biomarker for patients with urological malignancies. Urol. Oncol. 2012, 30, 509–515. [Google Scholar] [CrossRef]
- Zachariah, R.R.; Schmid, S.; Buerki, N.; Radpour, R.; Holzgreve, W.; Zhong, X. Levels of circulating cell-free nuclear and mitochondrial DNA in benign and malignant ovarian tumors. Obstet. Gynecol. 2008, 112, 843–850. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Podlesniy, P.; Trullas, R. Biomarkers in cerebrospinal fluid: Analysis of cell-free circulating mitochondrial DNA by digital PCR. Methods Mol. Biol. 2018, 1768, 111–126. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Kleeff, J.; Michl, P.; Costello, E.; Greenhalf, W.; Palmer, D.H. Therapeutic developments in pancreatic cancer: Current and future perspectives. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 333–348. [Google Scholar] [CrossRef]
- Fahrmann, J.F.; Bantis, L.E.; Capello, M.; Scelo, G.; Dennison, J.B.; Patel, N.; Murage, E.; Vykoukal, J.; Kundnani, D.L.; Foretova, L.; et al. A plasma-derived protein-metabolite multiplexed panel for early-stage pancreatic cancer. J. Natl. Cancer Inst. 2019, 111, 372–379. [Google Scholar] [CrossRef]
- Girolimetti, G.; Pelisenco, I.A.; Eusebi, L.H.; Ricci, C.; Cavina, B.; Kurelac, I.; Verri, T.; Calcagnile, M.; Alifano, P.; Salvi, A.; et al. Dysregulation of a subset of circulating and vesicle-associated miRNA in pancreatic cancer. Noncoding RNA 2024, 10, 29. [Google Scholar] [CrossRef]
- Goonetilleke, K.S.; Siriwardena, A.K. Systematic review of carbohydrate antigen (CA 19-9) as a biochemical marker in the diagnosis of pancreatic cancer. Eur. J. Surg. Oncol. 2007, 33, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Ishige, F.; Hoshino, I.; Iwatate, Y.; Chiba, S.; Arimitsu, H.; Yanagibashi, H.; Nagase, H.; Takayama, W. MIR1246 in body fluids as a biomarker for pancreatic cancer. Sci. Rep. 2020, 10, 8723. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.; Chen, R.; Crispin, D.A.; May, D.; Stevens, T.; McIntosh, M.W.; Bronner, M.P.; Ziogas, A.; Anton-Culver, H.; Brentnall, T.A. Protein alterations associated with pancreatic cancer and chronic pancreatitis found in human plasma using global quantitative proteomics profiling. J. Proteome Res. 2011, 10, 2359–2376. [Google Scholar] [CrossRef]
- Farrow, B.; Albo, D.; Berger, D.H. The role of the tumor microenvironment in the progression of pancreatic cancer. J. Surg. Res. 2008, 149, 319–328. [Google Scholar] [CrossRef]
- Wang, M.; Zhao, J.; Zhang, L.; Wei, F.; Lian, Y.; Wu, Y.; Gong, Z.; Zhang, S.; Zhou, J.; Cao, K.; et al. Role of tumor microenvironment in tumorigenesis. J. Cancer 2017, 8, 761–773. [Google Scholar] [CrossRef]
- Whiteside, T.L. The tumor microenvironment and its role in promoting tumor growth. Oncogene 2008, 27, 5904–5912. [Google Scholar] [CrossRef]
- Ahmed, A.; Tait, S.W.G. Targeting immunogenic cell death in cancer. Mol. Oncol. 2020, 14, 2994–3006. [Google Scholar] [CrossRef]
- Krysko, D.V.; Garg, A.D.; Kaczmarek, A.; Krysko, O.; Agostinis, P.; Vandenabeele, P. Immunogenic cell death and DAMPs in cancer therapy. Nat. Rev. Cancer 2012, 12, 860–875. [Google Scholar] [CrossRef]
- Wallach, D.; Kovalenko, A.; Kang, T.B. ‘Necrosome’-induced inflammation: Must cells die for it? Trends Immunol. 2011, 32, 505–509. [Google Scholar] [CrossRef]
- Piccinini, A.M.; Midwood, K.S. DAMPening inflammation by modulating TLR signalling. Mediators Inflamm. 2010, 2010, 672395. [Google Scholar] [CrossRef]
- Rubartelli, A.; Lotze, M.T. Inside, outside, upside down: Damage-associated molecular-pattern molecules (DAMPs) and redox. Trends Immunol. 2007, 28, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, C.; Huebener, P.; Schwabe, R.F. Damage-associated molecular patterns in cancer: A double-edged sword. Oncogene 2016, 35, 5931–5941. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wu, X.; Hu, Q.; Wu, J.; Wang, G.; Hong, Z.; Ren, J.; Lab for Trauma and Surgical Infections. Mitochondrial DNA in liver inflammation and oxidative stress. Life Sci. 2019, 236, 116464. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Crother, T.R.; Karlin, J.; Dagvadorj, J.; Chiba, N.; Chen, S.; Ramanujan, V.K.; Wolf, A.J.; Vergnes, L.; Ojcius, D.M.; et al. Oxidized mitochondrial DNA activates the NLRP3 inflammasome during apoptosis. Immunity 2012, 36, 401–414. [Google Scholar] [CrossRef]
- Mathios, D.; Johansen, J.S.; Cristiano, S.; Medina, J.E.; Phallen, J.; Larsen, K.R.; Bruhm, D.C.; Niknafs, N.; Ferreira, L.; Adleff, V.; et al. Detection and characterization of lung cancer using cell-free DNA fragmentomes. Nat. Commun. 2021, 12, 5060. [Google Scholar] [CrossRef]
- Ma, X.; Chen, Y.; Tang, W.; Bao, H.; Mo, S.; Liu, R.; Wu, S.; Bao, H.; Li, Y.; Zhang, L.; et al. Multi-dimensional fragmentomic assay for ultrasensitive early detection of colorectal advanced adenoma and adenocarcinoma. J. Hematol. Oncol. 2021, 14, 175. [Google Scholar] [CrossRef]
- Jin, C.; Liu, X.; Zheng, W.; Su, L.; Liu, Y.; Guo, X.; Gu, X.; Li, H.; Xu, B.; Wang, G.; et al. Characterization of fragment sizes, copy number aberrations and 4-mer end motifs in cell-free DNA of hepatocellular carcinoma for enhanced liquid biopsy-based cancer detection. Mol. Oncol. 2021, 15, 2377–2389. [Google Scholar] [CrossRef]
- Cristiano, S.; Leal, A.; Phallen, J.; Fiksel, J.; Adleff, V.; Bruhm, D.C.; Jensen, S.O.; Medina, J.E.; Hruban, C.; White, J.R.; et al. Genome-wide cell-free DNA fragmentation in patients with cancer. Nature 2019, 570, 385–389. [Google Scholar] [CrossRef]
- Liu, Y.; Peng, F.; Wang, S.; Jiao, H.; Dang, M.; Zhou, K.; Guo, W.; Guo, S.; Zhang, H.; Song, W.; et al. Aberrant fragmentomic features of circulating cell-free mitochondrial DNA as novel biomarkers for multi-cancer detection. EMBO Mol. Med. 2024, 16, 3169–3183. [Google Scholar] [CrossRef]
- Lo, Y.M.; Chan, K.C.; Sun, H.; Chen, E.Z.; Jiang, P.; Lun, F.M.; Zheng, Y.W.; Leung, T.Y.; Lau, T.K.; Cantor, C.R.; et al. Maternal plasma DNA sequencing reveals the genome-wide genetic and mutational profile of the fetus. Sci. Transl. Med0 2010, 2, 61ra91. [Google Scholar] [CrossRef]
- Avital, G.; Buchshtav, M.; Zhidkov, I.; Tuval Feder, J.; Dadon, S.; Rubin, E.; Glass, D.; Spector, T.D.; Mishmar, D. Mitochondrial DNA heteroplasmy in diabetes and normal adults: Role of acquired and inherited mutational patterns in twins. Hum. Mol. Genet. 2012, 21, 4214–4224. [Google Scholar] [CrossRef] [PubMed]
- Trumpff, C.; Marsland, A.L.; Sloan, R.P.; Kaufman, B.A.; Picard, M. Predictors of ccf-mtDNA reactivity to acute psychological stress identified using machine learning classifiers: A proof-of-concept. Psychoneuroendocrinology 2019, 107, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Picard, M.; McEwen, B.S.; Epel, E.S.; Sandi, C. An energetic view of stress: Focus on mitochondria. Front. Neuroendocrinol. 2018, 49, 72–85. [Google Scholar] [CrossRef] [PubMed]
- Picard, M.; McEwen, B.S. Psychological Stress and Mitochondria: A Systematic Review. Psychosom. Med. 2018, 80, 141–153. [Google Scholar] [CrossRef]
- Ferrara, N.; Houck, K.; Jakeman, L.; Leung, D.W. Molecular and biological properties of the vascular endothelial growth factor family of proteins. Endocr. Rev. 1992, 13, 18–32. [Google Scholar] [CrossRef]
- Koch, A.E.; Polverini, P.J.; Kunkel, S.L.; Harlow, L.A.; DiPietro, L.A.; Elner, V.M.; Elner, S.G.; Strieter, R.M. Interleukin-8 as a macrophage-derived mediator of angiogenesis. Science 1992, 258, 1798–1801. [Google Scholar] [CrossRef]
- Pirnia, F.; Breuleux, M.; Schneider, E.; Hochmeister, M.; Bates, S.E.; Marti, A.; Hotz, M.A.; Betticher, D.C.; Borner, M.M. Uncertain identity of doxorubicin-resistant MCF-7 cell lines expressing mutated p53. J. Natl. Cancer Inst. 2000, 92, 1535–1536. [Google Scholar] [CrossRef]
- Hou, Y.C.; Wang, C.J.; Chao, Y.J.; Chen, H.Y.; Wang, H.C.; Tung, H.L.; Lin, J.T.; Shan, Y.S. Elevated serum interleukin-8 level correlates with cancer-related cachexia and sarcopenia: An indicator for pancreatic cancer outcomes. J. Clin. Med. 2018, 7, 502. [Google Scholar] [CrossRef]
- Piro, G.; Simionato, F.; Carbone, C.; Frizziero, M.; Malleo, G.; Zanini, S.; Casolino, R.; Santoro, R.; Mina, M.M.; Zecchetto, C.; et al. A circulating T(H)2 cytokines profile predicts survival in patients with resectable pancreatic adenocarcinoma. Oncoimmunology 2017, 6, e1322242. [Google Scholar] [CrossRef]
- Liu, C.Y.; Xu, J.Y.; Shi, X.Y.; Huang, W.; Ruan, T.Y.; Xie, P.; Ding, J.L. M2-polarized tumor-associated macrophages promoted epithelial-mesenchymal transition in pancreatic cancer cells, partially through TLR4/IL-10 signaling pathway. Lab. Investig. 2013, 93, 844–854. [Google Scholar] [CrossRef]
- Lu, D.; Qin, Q.; Lei, R.; Hu, B.; Qin, S. Targeted blockade of interleukin 9 inhibits tumor growth in murine model of pancreatic cancer. Adv. Clin. Exp. Med. 2019, 28, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- van der Sijde, F.; Dik, W.A.; Mustafa, D.A.M.; Vietsch, E.E.; Besselink, M.G.; Debets, R.; Koerkamp, B.G.; Haberkorn, B.C.M.; Homs, M.Y.V.; Janssen, Q.P.; et al. Serum cytokine levels are associated with tumor progression during FOLFIRINOX chemotherapy and overall survival in pancreatic cancer patients. Front. Immunol. 2022, 13, 898498. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Primer | Name | Sequence |
|---|---|---|
| Forward | mtDNA-85F | 5′-CTCACTCCTTGGCGCCTGCC-3′ |
| Reverse | mtDNA-85R | 5′-GGCGGTTGAGGCGTCTGGTG-3′ |
| Probe | FAM-mtDNA-85P | FAM-5′-CCTCCAAATCACCACAGGACTATTCCTAGCCATGCA-3′-BHQ-1 |
| Type | Mediator |
|---|---|
| Cytokines | IFN-γ, IL-1β, IL-1ra, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12, IL-13, IL-15, IL-17A, TNF-α |
| Chemokines | CCL11, IP-10, MCP-1, MIP-1α, MIP-1β, RANTES |
| Growth factors | FGF-basic, G–CSF, GM–CSF, PDGF-BB, VEGF |
| PaCa (n = 11) | Controls (n = 3) | |
|---|---|---|
| Age (years), mean ± standard deviation | 69.1 ± 10.0 | 52.0 ± 16.0 |
| Women, n (%) | 3 (27) | 2 (67) |
| Size of primary lesion, mm (mean diameter range) | 35.7 (15–59) | |
| Tumor stage, n (%) | ||
| II | 1 (9) | |
| III | 3 (27) | |
| IV | 7 (63) | |
| Primary lesion location, n (%) | ||
| Pancreas head | 7 (64) | |
| Pancreas body | 3 (27) | |
| Pancreas tail | 1 (9) | |
| Distant metastases, n (%) | ||
| No | 4 (36.4) | |
| Yes | 7 (63.6) | |
| Presence of comorbidity *, n (%) | 7 (63.6) |
| mtDNA vs. IL-1b | mtDNA vs. IL-1ra | mtDNA vs. IL-4 | mtDNA vs. IL-5 | mtDNA vs. IL-8 | mtDNA vs. IL-9 | mtDNA vs. IL-10 | mtDNA vs. IL-13 | mtDNA vs. IL-17A | mtDNA vs. Eotaxin | mtDNA vs. FGF b | mtDNA vs. G–CSF | mtDNA vs. IFN-γ | mtDNA vs. IP-10 | mtDNA vs. MCP-1 | mtDNA vs. MIP-1a | mtDNA vs. MIP-1b | mtDNA vs. RANTES | mtDNA vs. TNF-α | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Spearman r | 0.26 | −0.01 | 0.46 | 0.51 | 0.70 | 0.37 | 0.20 | −0.35 | −0.07 | 0.25 | 0.69 | −0.30 | 0.37 | 0.30 | 0.66 | 0.53 | 0.40 | 0.24 | −0.08 |
| 95% CI | −0.42 to 0.75 | −0.62 to 0.61 | −0.22 to 0.84 | −0.15 to 0.86 | 0.15 to 0.92 | −0.35 to 0.79 | −0.47 to 0.72 | −0.80 to 0.33 | −0.65 to 0.57 | −0.42 to 0.75 | 0.14 to 0.92 | −0.70 to 0.50 | −0.35 to 0.79 | −0.38 to 0.77 | 0.09 to 0.90 | −0.13 to 0.86 | −0.27 to 0.82 | −0.44 to 0.74 | −0.66 to 0.56 |
| p value * | 0.435 | 0.999 | 0.164 | 0.111 | 0.02 | 0.313 | 0.557 | 0.288 | 0.844 | 0.451 | 0.022 | 0.650 | 0.313 | 0.371 | 0.031 | 0.100 | 0.214 | 0.485 | 0.818 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girolimetti, G.; Guerra, F.; Eusebi, L.H.U.; Ricci, C.; Marzetti, E.; Picca, A.; Bucci, C. Circulating Cell-Free Mitochondrial DNA and Inflammation in Older Adults with Pancreatic Cancer: Results from an Exploratory Study. Appl. Sci. 2025, 15, 4410. https://doi.org/10.3390/app15084410
Girolimetti G, Guerra F, Eusebi LHU, Ricci C, Marzetti E, Picca A, Bucci C. Circulating Cell-Free Mitochondrial DNA and Inflammation in Older Adults with Pancreatic Cancer: Results from an Exploratory Study. Applied Sciences. 2025; 15(8):4410. https://doi.org/10.3390/app15084410
Chicago/Turabian StyleGirolimetti, Giulia, Flora Guerra, Leonardo Henry Umberto Eusebi, Claudio Ricci, Emanuele Marzetti, Anna Picca, and Cecilia Bucci. 2025. "Circulating Cell-Free Mitochondrial DNA and Inflammation in Older Adults with Pancreatic Cancer: Results from an Exploratory Study" Applied Sciences 15, no. 8: 4410. https://doi.org/10.3390/app15084410
APA StyleGirolimetti, G., Guerra, F., Eusebi, L. H. U., Ricci, C., Marzetti, E., Picca, A., & Bucci, C. (2025). Circulating Cell-Free Mitochondrial DNA and Inflammation in Older Adults with Pancreatic Cancer: Results from an Exploratory Study. Applied Sciences, 15(8), 4410. https://doi.org/10.3390/app15084410