
Harnessing Generative Artificial Intelligence for Exercise and Training Prescription: Applications and Implications in Sports and Physical Activity—A Systematic Literature Review



Abstract
1. Introduction
2. Methods
2.1. Study Protocol and Study Finding Reporting
2.2. Search Strategy
2.3. Data Extraction and Data Synthesis
2.4. Critical Appraisal
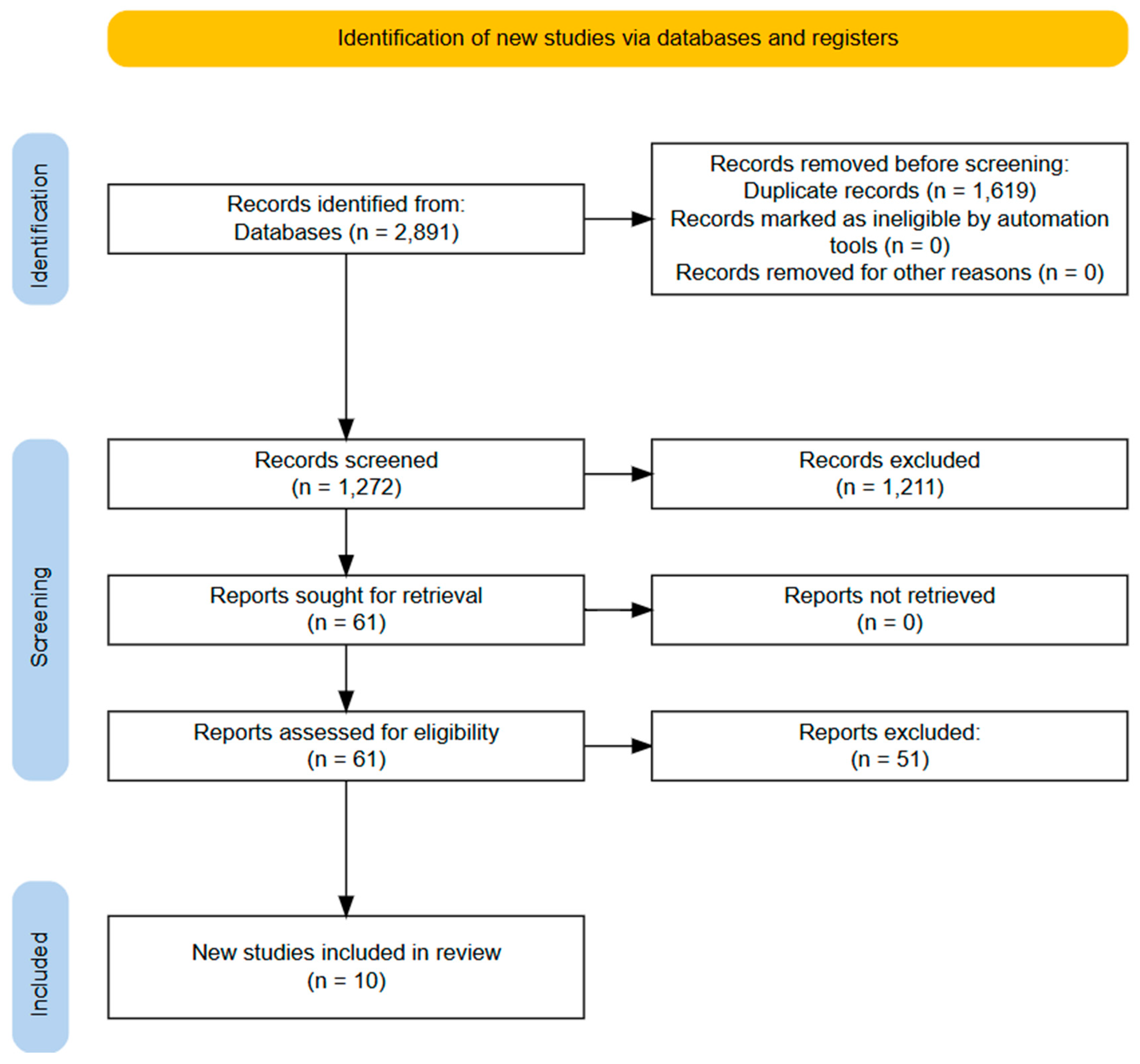
3. Results
Systematic Literature Review Findings
4. Discussion
4.1. The Role of Generative AI in Personalized Exercise Programs for Health and Disease
4.2. The Role of Generative AI in Personalized Exercise Programs for Athletes
4.3. Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health Benefits of Physical Activity: The Evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity--a systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ammar, A.; Trabelsi, K.; Hermassi, S.; Kolahi, A.-A.; Mansournia, M.; Jahrami, H.; Boukhris, O.; Boujelbane, M.; Glenn, J.; Clark, C.; et al. Global Disease Burden Attributed to Low Physical Activity in 204 Countries and Territories from 1990 to 2019: Insights from the Global Burden of Disease 2019 Study. Biol. Sport 2023, 40, 835–855. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.M.; Kennedy, M.A. The exercise prescription: A tool to improve physical activity. PM&R 2012, 4, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Wackerhage, H.; Schoenfeld, B.J. Personalized, Evidence-Informed Training Plans and Exercise Prescriptions for Performance, Fitness and Health. Sports Med. 2021, 51, 1805–1813. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W.; Roberts, M.D.; Church, T.S. Toward exercise as personalized medicine. Sports Med. 2013, 43, 157–165. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lehtonen, E.; Gagnon, D.; Eklund, D.; Kaseva, K.; Peltonen, J.E. Hierarchical framework to improve individualised exercise prescription in adults: A critical review. BMJ Open Sport Exerc. Med. 2022, 8, e001339. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lucini, D.; Pagani, M. Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 968. [Google Scholar] [CrossRef]
- Rooney, D.; Gilmartin, E.; Heron, N. Prescribing Exercise and Physical Activity to Treat and Manage Health Conditions. Ulst. Med. J. 2023, 92, 9–15. [Google Scholar]
- Milani, J.G.P.O.; Milani, M.; Verboven, K.; Cipriano, G.; Hansen, D. Exercise Intensity Prescription in Cardiovascular Rehabilitation: Bridging the Gap between Best Evidence and Clinical Practice. Front. Cardiovasc. Med. 2024, 11, 1380639. [Google Scholar] [CrossRef]
- Almarcha, M.; Sturmberg, J.; Balagué, N. Personalizing the Guidelines of Exercise Prescription for Health: Guiding Users from Dependency to Self-Efficacy. Apunt. Sports Med. 2024, 59, 100449. [Google Scholar] [CrossRef]
- Zenko, Z.; Ekkekakis, P. Knowledge of Exercise Prescription Guidelines Among Certified Exercise Professionals. J. Strength Cond. Res. 2015, 29, 1422–1432. [Google Scholar] [CrossRef] [PubMed]
- Vyas, S.; Gupta, S.; Shukla, V.K. Towards Edge AI and Varied Approaches of Digital Wellness in Healthcare Administration: A Study. In Proceedings of the 2023 International Conference on Computational Intelligence and Knowledge Economy (ICCIKE), Dubai, United Arab Emirates, 9–10 March 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 186–190. [Google Scholar]
- Al Kuwaiti, A.; Nazer, K.; Al-Reedy, A.; Al-Shehri, S.; Al-Muhanna, A.; Subbarayalu, A.V.; Al Muhanna, D.; Al-Muhanna, F.A. A Review of the Role of Artificial Intelligence in Healthcare. J. Pers. Med. 2023, 13, 951. [Google Scholar] [CrossRef]
- Iqbal, J.; Jaimes, D.C.C.; Makineni, P.; Subramani, S.; Hemaida, S.; Thugu, T.R.; Butt, A.N.; Sikto, J.T.; Kaur, P.; Lak, M.A.; et al. Reimagining healthcare: Unleashing the power of artificial intelligence in medicine. Cureus 2023, 15, e44658. [Google Scholar]
- Sezgin, E. Artificial intelligence in healthcare: Complementing, not replacing, doctors and healthcare providers. Digit. Health 2023, 9, 20552076231186520. [Google Scholar] [PubMed]
- Reis, F.J.J.; Alaiti, R.K.; Vallio, C.S.; Hespanhol, L. Artificial Intelligence and Machine Learning Approaches in Sports: Concepts, Applications, Challenges, and Future Perspectives. Braz. J. Phys. Ther. 2024, 28, 101083. [Google Scholar] [CrossRef]
- Mateus, N.; Abade, E.; Coutinho, D.; Gómez, M.-Á.; Peñas, C.L.; Sampaio, J. Empowering the Sports Scientist with Artificial Intelligence in Training, Performance, and Health Management. Sensors 2024, 25, 139. [Google Scholar] [CrossRef]
- Krstić, D.; Vučković, T.; Dakić, D.; Ristić, S.; Stefanović, D. The application and impact of artificial intelligence on sports performance improvement: A systematic literature review. In Proceedings of the 2023 4th International Conference on Communications, Information, Electronic and Energy Systems (CIEES), Plovdiv, Bulgaria, 23–25 November 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 1–8. [Google Scholar]
- Naughton, M.; Salmon, P.M.; Compton, H.R.; McLean, S. Challenges and Opportunities of Artificial Intelligence Implementation within Sports Science and Sports Medicine Teams. Front. Sports Act. Living 2024, 6, 1332427. [Google Scholar] [CrossRef]
- Chen, H.-K.; Chen, F.-H.; Lin, S.-F. An AI-Based Exercise Prescription Recommendation System. Appl. Sci. 2021, 11, 2661. [Google Scholar] [CrossRef]
- Balpande, M.; Sharma, J.; Nair, A.; Khandelwal, M.; Dhanray, S. AI Based Gym Trainer and Diet Recommendation System. In Proceedings of the 2023 IEEE 4th Annual Flagship India Council International Subsections Conference (INDISCON), Mysore, India, 5–7 August 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 1–7. [Google Scholar]
- Reddy, S. Generative AI in Healthcare: An Implementation Science Informed Translational Path on Application, Integration and Governance. Implement. Sci. 2024, 19, 27. [Google Scholar] [CrossRef]
- Fayed, A.M.; Mansur, N.S.B.; de Carvalho, K.A.; Behrens, A.; D’hooghe, P.; Netto, C.d.C. Artificial Intelligence and ChatGPT in Orthopaedics and Sports Medicine. J. Exp. Orthop. 2023, 10, 74. [Google Scholar] [CrossRef] [PubMed]
- Oliver, A.; Guiller, J. Generative AI in Sport and Exercise Psychology: Exploring Opportunities and Overcoming Challenges. Sport Exerc. Psychol. Rev. 2025, 19, 36–45. [Google Scholar] [CrossRef]
- Chang, Y.; Wang, X.; Wang, J.; Wu, Y.; Yang, L.; Zhu, K.; Chen, H.; Yi, X.; Wang, C.; Wang, Y.; et al. A Survey on Evaluation of Large Language Models. ACM Trans. Intell. Syst. Technol. 2024, 15, 1–45. [Google Scholar] [CrossRef]
- Naveed, H.; Khan, A.U.; Qiu, S.; Saqib, M.; Anwar, S.; Usman, M.; Akhtar, N.; Barnes, N.; Mian, A. A Comprehensive Overview of Large Language Models. arXiv 2024, arXiv:2307.06435. [Google Scholar]
- Solomon, T.; Laye, M. Examining the Sports Nutrition Knowledge of Large Language Model. (LLM) Artificial Intelligence (AI) Chatbots. 2024. Available online: https://osf.io/zckya/resources (accessed on 13 March 2025).
- Puce, L.; Ceylan, H.İ.; Trompetto, C.; Cotellessa, F.; Schenone, C.; Marinelli, L.; Zmijewski, P.; Bragazzi, N.; Mori, L. Optimizing Athletic Performance through Advanced Nutritionstrategies: Can. AI and Digital Platforms Have a Role in Ultraendurance Sports? Biol. Sport 2024, 41, 305–313. [Google Scholar] [CrossRef]
- Sheikh, H.; Prins, C.; Schrijvers, E. Artificial Intelligence: Definition and Background. In Research for Policy; Springer: Berlin/Heidelberg, Germany, 2023; pp. 15–41. [Google Scholar] [CrossRef]
- Razno, M. Machine learning text classification model with NLP approach. Comput. Linguist. Intell. Syst. 2019, 2, 71–73. [Google Scholar]
- Gupta, N.; Khatri, K.; Malik, Y.; Lakhani, A.; Kanwal, A.; Aggarwal, S.; Dahuja, A. Exploring Prospects, Hurdles, and Road Ahead for Generative Artificial Intelligence in Orthopedic Education and Training. BMC Med. Educ. 2024, 24, 1544. [Google Scholar] [CrossRef]
- Millington, B.; Naraine, M.L.; Wanless, L.; Safai, P.; Manley, A. Sport and the Promise of Artificial Intelligence: Human and Machine Futures. Sociol. Sport J. 2025, 1, 1–10. [Google Scholar]
- Desai, V. The future of artificial intelligence in sports medicine and return to play. In Seminars in Musculoskeletal Radiology; Thieme Medical Publishers Inc.: New York, NY, USA, 2024; Volume 28, pp. 203–212. [Google Scholar]
- Lotfi, N.; Madani, M. Evaluating the Qualitative and Quantitative Performance of Generative AI on Knowledge in Sports Medicine: The Case of GPT. In General Aspects of Applying Generative AI in Higher Education: Opportunities and Challenges; Springer Nature: Cham, Switzerland, 2024; pp. 103–119. [Google Scholar]
- Chemnad, K.; Othman, A. Digital Accessibility in the Era of Artificial Intelligence—Bibliometric Analysis and Systematic Review. Front. Artif. Intell. 2024, 7, 1349668. [Google Scholar] [CrossRef]
- Shuford, J. Contribution of artificial intelligence in improving accessibility for individuals with disabilities. J. Knowl. Learn. Sci. Technol. 2023, 2, 421–433, ISSN 2959-6386. [Google Scholar]
- Kulkarni, M. Digital accessibility: Challenges and opportunities. IIMB Manag. Rev. 2019, 31, 91–98. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- UNO per Tutto. Available online: https://unopertutto.unige.net/discovery/search?vid=39GEN_INST:39GEN_VU1 (accessed on 13 March 2025).
- Sallam, M.; Barakat, M.; Sallam, M. A Preliminary Checklist (METRICS) to Standardize the Design and Reporting of Studies on Generative Artificial Intelligence–Based Models in Health Care Education and Practice: Development Study Involving a Literature Review. Interact. J. Med. Res. 2023, 13, e54704. [Google Scholar]
- Masagca, R.C. The AI Coach: A 5-Week AI-Generated Calisthenics Training Program on Health-Related Physical Fitness Components of Untrained Collegiate Students. J. Hum. Sport Exerc. 2024, 20, 39–56. [Google Scholar] [CrossRef]
- Dergaa, I.; Ben Saad, H.; El Omri, A.; Glenn, J.; Clark, C.; Washif, J.; Guelmami, N.; Hammouda, O.; Al-Horani, R.; Reynoso-Sánchez, L.; et al. Using Artificial Intelligence for Exercise Prescription in Personalised Health Promotion: A Critical Evaluation of OpenAI’s GPT-4 Model. Biol. Sport 2024, 41, 221–241. [Google Scholar] [CrossRef]
- Düking, P.; Sperlich, B.; Voigt, L.; Hooren, B.V.; Zanini, M.; Zinner, C. ChatGPT Generated Training Plans for Runners Are Not Rated Optimal by Coaching Experts, but Increase in Quality with Additional Input Information. J. Sports Sci. Med. 2024, 23, 56–72. [Google Scholar] [CrossRef]
- Erol, E.; Arıkan, H. Does ChatGPT Provide Comprehensive and Accurate Information Regarding the Effects, Types and Programming of Core Exercises? Turk. J. Kinesiol. 2024, 10, 178–182. [Google Scholar] [CrossRef]
- Havers, T.; Masur, L.; Isenmann, E.; Geisler, S.; Zinner, C.; Sperlich, B.; Düking, P. Reproducibility and Quality of Hypertrophy-Related Training Plans Generated by GPT-4 and Google Gemini as Evaluated by Coaching Experts. Biol. Sport 2025, 42, 289–329. [Google Scholar] [CrossRef]
- Philuek, P.; Kusump, S.; Sathianpoonsook, T.; Jansupom, C.; Sawanyawisuth, P.; Sawanyawisuth, K.; Chainarong, A. The Effects of Chat GPT Generated Exercise Program in Healthy Overweight Young Adults. J. Hum. Sport Exerc. 2024, 20, 169–179. [Google Scholar]
- Washif, J.; Pagaduan, J.; James, C.; Dergaa, I.; Beaven, C. Artificial Intelligence in Sport: Exploring the Potential of usingChatGPT in Resistance Training Prescription. Biol. Sport 2024, 41, 209–220. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, Q.; Pang, J.; Zeng, C.; Ma, X.; Li, P.; Ma, L.; Huang, J.; Xie, H. Assessment of Personalized Exercise Prescriptions Issued by ChatGPT 4.0 and Intelligent Health Promotion Systems for Patients with Hypertension Comorbidities Based on the Transtheoretical Model: A Comparative Analysis. J. Multidiscip. Healthc. 2024, 17, 5063–5078. [Google Scholar] [CrossRef] [PubMed]
- Zaleski, A.L.; Berkowsky, R.; Craig, K.J.T.; Pescatello, L.S. Comprehensiveness, Accuracy, and Readability of Exercise Recommendations Provided by an AI-Based Chatbot: Mixed Methods Study. JMIR Med. Educ. 2024, 10, e51308. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Geng, W.; Huang, L.; Qin, X.; Chen, Z.; Yan, H. Who Could and Should Give Exercise Prescription: Physicians, Exercise and Health Scientists, Fitness Trainers, or ChatGPT? J. Sport Health Sci. 2024, 13, 368–372. [Google Scholar] [CrossRef]
- Wang, L.; Chen, X.; Deng, X.; Wen, H.; You, M.; Liu, W.; Li, Q.; Li, J. Prompt Engineering in Consistency and Reliability with the Evidence-Based Guideline for LLMs. npj Digit. Med. 2024, 7, 41. [Google Scholar] [CrossRef]
- Chen, B.; Zhang, Z.; Langrené, N.; Zhu, S. Unleashing the Potential. of Prompt Engineering in Large Language Models: A Comprehensive Review. arXiv 2024, arXiv:2310.14735. [Google Scholar]
- Kush, J.C. Integrating Sensor Technologies with Conversational AI: Enhancing Context-Sensitive Interaction Through Real-Time Data Fusion. Sensors 2025, 25, 249. [Google Scholar] [CrossRef] [PubMed]
- Oğul, H. Language of Actions: A Generative Model for Activity Recognition and next Move Prediction from Motion Sensors. Expert Syst. Appl. 2025, 264, 125947. [Google Scholar] [CrossRef]
- Li, Z.; Deldari, S.; Chen, L.; Xue, H.; Salim, F.D. SensorLLM: Aligning Large Language Models with Motion Sensors for Human Activity Recognition. arXiv 2024, arXiv:2410.10624. [Google Scholar]
- Casado, A.; González-Mohíno, F.; González-Ravé, J.M.; Foster, C. Training Periodization, Methods, Intensity Distribution, and Volume in Highly Trained and Elite Distance Runners: A Systematic Review. Int. J. Sports Physiol. Perform. 2022, 17, 820–833. [Google Scholar] [CrossRef]
- Galán-Rioja, M.Á.; Gonzalez-Ravé, J.M.; González-Mohíno, F.; Seiler, S. Training Periodization, Intensity Distribution, and Volume in Trained Cyclists: A Systematic Review. Int. J. Sports Physiol. Perform. 2023, 18, 112–122. [Google Scholar] [CrossRef]
- Mujika, I.; Halson, S.; Burke, L.M.; Balagué, G.; Farrow, D. An Integrated, Multifactorial Approach to Periodization for Optimal Performance in Individual and Team Sports. Int. J. Sports Physiol. Perform. 2018, 13, 538–561. [Google Scholar] [CrossRef]
- Cavazzotto, T.G.; Dantas, D.B.; Queiroga, M.R. ChatGPT and Exercise Prescription: Human vs. Machine or Human plus Machine? J. Sport Health Sci. 2024, 13, 661–662. [Google Scholar] [CrossRef]
- Mishra, N.; Habal, B.G.M.; Garcia, P.S.; Garcia, M.B. Harnessing an AI-Driven Analytics Model to Optimize Training and Treatment in Physical Education for Sports Injury Prevention. In Proceedings of the 2024 8th International Conference on Education and Multimedia Technology, Tokyo, Japan, 22–24 June 2024; ACM: New York, NY, USA, 2024; pp. 309–315. [Google Scholar]
- Lanotte, F.; O’Brien, M.K.; Jayaraman, A. AI in Rehabilitation Medicine: Opportunities and Challenges. Ann. Rehabil. Med. 2023, 47, 444–458. [Google Scholar] [CrossRef] [PubMed]
- Biró, A.; Cuesta-Vargas, A.I.; Szilágyi, L. AI-Assisted Fatigue and Stamina Control for Performance Sports on IMU-Generated Multivariate Times Series Datasets. Sensors 2023, 24, 132. [Google Scholar] [CrossRef]
- Rocha-Silva, R.; Rodrigues, M.A.M.; Viana, R.B.; Nakamoto, F.P.; Vancini, R.L.; Andrade, M.S.; Rosemann, T.; Weiss, K.; Knechtle, B.; De Lira, C.A.B. Critical Analysis of Information Provided by ChatGPT on Lactate, Exercise, Fatigue, and Muscle Pain: Current Insights and Future Prospects for Enhancement. Adv. Physiol. Educ. 2024, 48, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.; Guo, Q.; He, Y.; Lu, Y.; Xie, R.; Li, C.; Wu, H. Artificial Intelligence in Sports Medicine: Could GPT-4 Make Human Doctors Obsolete? Ann. Biomed. Eng. 2023, 51, 1658–1662. [Google Scholar] [CrossRef]
- Mekki, Y.M.; Ahmed, O.H.; Powell, D.; Price, A.; Dijkstra, H.P. Games Wide Open to athlete partnership in building artificial intelligence systems. npj Digit. Med. 2024, 7, 267, Erratum in: npj Digit. Med. 2024, 7, 291. https://doi.org/10.1038/s41746-024-01284-5. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mennella, C.; Maniscalco, U.; De Pietro, G.; Esposito, M. Ethical and Regulatory Challenges of AI Technologies in Healthcare: A Narrative Review. Heliyon 2024, 10, e26297. [Google Scholar] [CrossRef]

{kind=link}
| Search Strategy Items | Details |
|---|---|
| Search string | (“generative artificial intelligence” OR “large language model*” OR chatbot* OR “conversational agent” OR “digital assistant” OR “virtual assistant” OR “google bard” OR “google gemini” OR “microsoft copilot” OR chatgpt* OR “generative pre-trained transformer*”) AND (sport* OR exercis* OR “physical activity” OR athlet* OR training) AND (prescribing OR prescription* OR recommend*) |
| Databases | UnoPerTutto hosted by Genoa University, Genoa, Italy |
| Inclusion Criteria |
|
| Exclusion criteria |
|
| Language filter | None (any language) |
| Time filter | None (from inception) |
| Study | Study Country | Study Design | Sample Size | Evaluation Framework and Systems Compared | Exercise Prescription | Key Metrics | Main Findings |
|---|---|---|---|---|---|---|---|
| Dergaa et al., 2024 [43] | 20 countries | Quasi-qualitative assessment and expert panel review | Five hypothetical patient scenarios (hypertension, osteoarthritis, anxiety, type 2 diabetes, asthma; 2 males, 3 females, age 27–50 years) | GPT-4 vs. 38 specialists in sports medicine, exercise science, and rehabilitation | Standardized prompt asking GPT-4 to create a 30-day exercise program using the FITT principles | Adherence to FITT principles, integration of perceived exertion, safety considerations, and individualization | GPT-4 created safe, general exercise programs, which lacked specificity and progression for individual health conditions Other key limitations include overemphasis on safety and moderate intensity, lack of real-time feedback and monitoring, generic approach due to the single-interaction design |
| Düking et al., 2024 [44] | Germany, Netherlands, UK | Mixed-methods approach (expert panel review, quasi-qualitative assessments) | A fictional 20-year-old male runner | ChatGPT (version 3.0.1) vs. 10 experienced coaches with seven years of experience | 6-week running plans incorporating intervals, long runs, and recovery | 22 criteria (18 primary and 4 secondary) | Plans with more input received higher quality ratings However, AI-generated plans lack direct interactions and feedback with users and are not completely evidence-based, requiring expert validation |
| Erol and Arıkan, 2024 [45] | Turkey | Quantitative assessments | Not applicable | ChatGPT-3.5 vs. nine experienced physiotherapists with 6–11 years of experience | 23 knowledge items related to core exercises | Accuracy/adequacy | ChatGPT was generally satisfactory in providing answers related to core exercises Best performance was in general knowledge questions, while it struggled with individualized programming and specific recommendations |
| Havers et al., 2025 [46] | Germany | Mixed-methods approach (expert panel review, quasi-qualitative assessment) | A fictitious person | Google Gemini 1.0 Pro and GPT-4 vs. 12 coaching experts with at least 3 years of experience | 8-week muscle hypertrophy-related resistance training plans | Key training aspects covering exercise selection, training intensity, weekly frequency, repetition range, and recovery principle | More detailed input improved LLM-generated plans, but coaching experts still rated them below optimal levels GPT-4 outperformed Google Gemini in training plan quality, regardless of input detail Reproducibility varied |
| Masagca, 2025 [42] | Philippines | Quasi-experimental; one-group pre-test-post-test for within-group comparison and two-group pre-test-post-test for between-group comparison | 87 untrained collegiate students (44 females, 43 males); 43 in the AI-generated calisthenics training program (AIGCTP) group, 44 in the human-made calisthenics training program (HMCTP) group | ChatGPT-3.5 | Prompt based on FITT principles—a 5-week calisthenics training program, including flexibility, cardiovascular endurance, and muscular endurance components | Flexibility (sit and reach test), cardiovascular endurance (3-min step test), muscular endurance (wall sit, plank, and push-up tests) | AIGCTP significantly improved lower extremity flexibility and upper extremity muscular endurance in males but had limited impact on females HMCTP showed improvements in cardiovascular endurance, lower limb flexibility, and muscular endurance of upper and lower extremities in males The traditional program outperformed AI-generated training in cardiovascular endurance and some male-specific metrics |
| Philuek et al., 2025 [47] | Thailand | Randomized controlled trial (intervention study) | 9 participants aged 19 years (ChatGPT-generated exercise program: 6; Control: 3) | ChatGPT-4.0 | Exercise for weight reduction—8-week program, 3 sessions per week (a 5–10-min warm-up, 45–60 min of physical fitness exercises—aerobic, resistance training, flexibility –, and a 5–10-min cool-down) | BMI, percent of fat, level of visceral fat, basal metabolic rate, percent of skeletal muscle, percent of subcutaneous fat, heart rate after standing and knee lifting for 3 min, hand grip strength, sit and stand in 30 s, flexibility, and lung capacity | The ChatGPT group showed significant improvements in BMI, heart rate after standing and knee lifting, and sit-and-stand repetitions in 30 s |
| Washif et al., 2024 [48] | Malaysia, Czech Republic, Hong Kong, Qatar, Tunisia, New Zealand | Qualitative assessments | A hypothetic male and female individual, aged 20 years, with intermediate and advanced resistance training experience | ChatGPT-3.5 and -4.0 vs. established guidelines (e.g., National Strength and Conditioning Association textbook) | Standardized instructions requesting 12-week resistance training programs for specific experience levels | Periodization, exercise selection, training volume, load intensity, tempo, rest intervals, and progression | GPT 4.0 generated more comprehensive and tailored programs than GPT 3.5, considering advanced training principles like block periodization and active recovery However, programs required expert modification to align with best practices Key limitations included lack of real-time adaptability, emerging methodologies (e.g., blood flow restriction), and sex-specific guidance |
| Xu et al., 2024 [49] | China | Mixed-methods approach with patient data collected via questionnaires and hardware tools | 5 hypertensive patients (3 females, 2 males) with comorbidities, aged 69–79 years, with conditions such as diabetes, COPD, chronic nephritis, Parkinson’s disease, and gouty arthritis | ChatGPT-4.0 and Intelligent Health Promotion Systems (IHPS) vs. 24 multidisciplinary experts from over ten different professional fields, with more than 10 years of experience | Exercise prescription for hypertensive patients based on expected health benefits, FITT principles, and safety | Accuracy, comprehensiveness, applicability, and evaluation based on the Transtheoretical Model | ChatGPT outperformed IHPS in accuracy and comprehensiveness, but IHPS had better applicability consistency ChatGPT did not take into account cultural preferences and delivered standardized, repetitive prescriptions Gaps in medication management, adaptability, and personalization |
| Zaleski et al., 2024 [50] | USA | Mixed-methods approach (conceptual content analysis and thematic mapping) | 26 populations across the lifespan including healthy adults, older adults, children and adolescents, pregnant individuals, and those with chronic diseases such as CVD, diabetes, cancer, and HIV | ChatGPT-3.5 vs. ACSM guidelines | Exercise recommendations for diverse populations | Accuracy, comprehensiveness/depth (adherence to the FITT principles, and alignment with ACSM guidelines), and readability | Moderate comprehensiveness and high accuracy, with low readability and gaps in exercise frequency, intensity, time, and volume guidance, misinformation (e.g., medical clearance overemphasis for preparticipation screening), inconsistencies in the terminology used for exercise professionals, liability concerns leading to bias toward safety, and discrimination against age-based and disabled populations |
| Zhu et al., 2024 [51] | China and USA | Qualitative assessments, with case studies—two cases (a case from the ACSM Guidelines and a fictional case) | Patients undergoing post-stent cardiac rehabilitation (a 60-year-old woman) and with Parkinson’s disease | ChatGPT-4.0 vs. ACSM guidelines | Medical clearance for a professionally led walking program and an aerobic and strength training program | Adherence to the FITT-VP principles, alignment with ACSM guidelines | ChatGPT aligned with ACSM guidelines and provided additional context (e.g., balance, safety, and motivation) |
| Study | Model Specification | Evaluation Approach | Timing of Testing | Transparency of Data Source | Range of Tested Topics | Topic Selection (Randomized/Systematic) | Interrater Reliability/Reliability | Number of Queries | Prompt Specificity | Overall Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Dergaa et al., 2024 [43] | ✅ | ✅ | ✅ | ✅ | ✅ | ❌ | ❌ | ✅ | ✅ | Medium |
| Düking et al., 2024 [44] | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | High |
| Erol and Arıkan, 2024 [45] | ✅ | ✅ | ❌ | ❌ | ❌ | ✅ | ❌ | ✅ | ❌ | Low |
| Havers et al., 2025 [46] | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | High |
| Masagca, 2025 [42] | ✅ | ✅ | ❌ | ✅ | ❌ | ❌ | ✅ | ❌ | ✅ | Medium |
| Philuek et al., 2025 [47] | ✅ | ✅ | ❌ | ✅ | ❌ | ❌ | ✅ | ❌ | ❌ | Low |
| Washif et al., 2024 [48] | ✅ | ✅ | ✅ | ✅ | ✅ | ❌ | ❌ | ✅ | ✅ | Medium |
| Xu et al., 2024 [49] | ✅ | ✅ | ❌ | ❌ | ❌ | ❌ | ✅ | ❌ | ✅ | Low |
| Zaleski et al., 2024 [50] | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ✅ | ❌ | High |
| Zhu et al., 2024 [51] | ✅ | ✅ | ❌ | ✅ | ❌ | ❌ | ❌ | ❌ | ❌ | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puce, L.; Bragazzi, N.L.; Currà, A.; Trompetto, C. Harnessing Generative Artificial Intelligence for Exercise and Training Prescription: Applications and Implications in Sports and Physical Activity—A Systematic Literature Review. Appl. Sci. 2025, 15, 3497. https://doi.org/10.3390/app15073497
Puce L, Bragazzi NL, Currà A, Trompetto C. Harnessing Generative Artificial Intelligence for Exercise and Training Prescription: Applications and Implications in Sports and Physical Activity—A Systematic Literature Review. Applied Sciences. 2025; 15(7):3497. https://doi.org/10.3390/app15073497
Chicago/Turabian StylePuce, Luca, Nicola Luigi Bragazzi, Antonio Currà, and Carlo Trompetto. 2025. "Harnessing Generative Artificial Intelligence for Exercise and Training Prescription: Applications and Implications in Sports and Physical Activity—A Systematic Literature Review" Applied Sciences 15, no. 7: 3497. https://doi.org/10.3390/app15073497
APA StylePuce, L., Bragazzi, N. L., Currà, A., & Trompetto, C. (2025). Harnessing Generative Artificial Intelligence for Exercise and Training Prescription: Applications and Implications in Sports and Physical Activity—A Systematic Literature Review. Applied Sciences, 15(7), 3497. https://doi.org/10.3390/app15073497