
Ergonomics Study of Musculoskeletal Disorders Among Tram Drivers


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
- Anthropometric parameters were obtained from existing datasets and adjusted using Muftić’s harmonic method.
- Postural risk levels were assessed using RULA and REBA tools within the ErgoFellow 3.0 software environment.
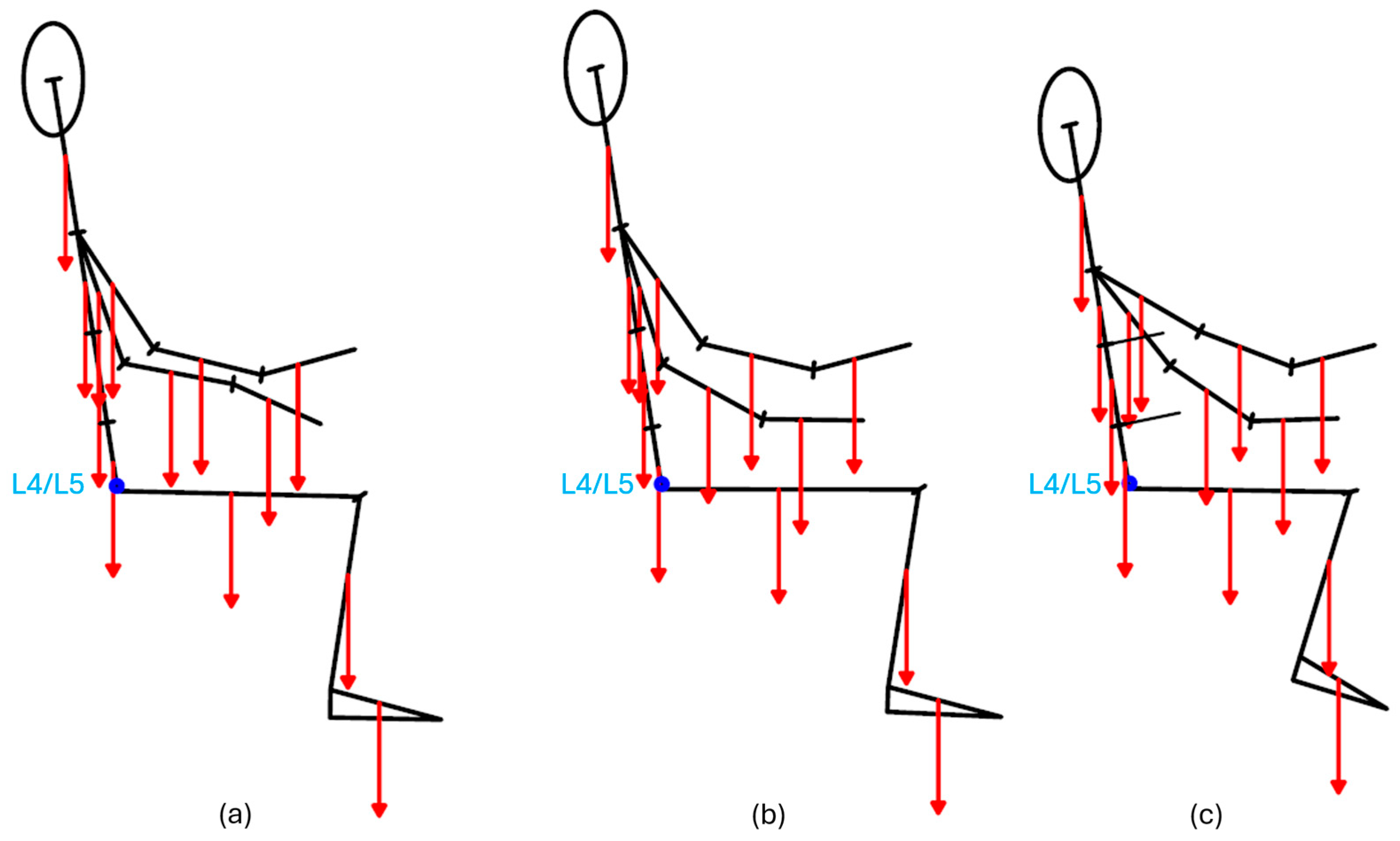
- Lumbar loading was estimated by calculating the moment at the L4/L5 spinal segment based on segmental mass and body posture.
2.2. Anthropometry in Tram Driver Workspace
2.3. RULA
2.4. REBA
2.5. Ergofellow 3.0 Software
2.6. Driver’s Working Posture in the Tram Cabin
2.7. Lumbar Moment Calculation at L4/L5
3. Results
3.1. RULA and REBA
3.2. Lumbar Moment at L4/L5 and the Influence of Anthropometry
4. Discussion
4.1. Interpretation of Postural Risk Scores
4.2. Interpretation of Lumbar Moment Results
4.3. Study Limitations
4.4. Practical Implications and Design Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| WMSD | Work-related musculoskeletal disorders |
| RULA | Rapid Upper Limb Assessment |
| REBA | Rapid Entire Body Assessment |
References
- Wickens, C.D.; Gordon, S.E.; Liu, Y.; Lee, J. An introduction to Human Factors Engineering; Addison Wesley Longman: Upper Saddle River, NJ, USA, 1997. [Google Scholar]
- Gajšek, B.; Draghici, A.; Boatca, M.E.; Gaureanu, A.; Robescu, D. Linking the Use of Ergonomics Methods to Workplace Social Sustainability: The Ovako Working Posture Assessment System and Rapid Entire Body Assessment Method. Sustainability 2022, 14, 4301. [Google Scholar] [CrossRef]
- Zink, K.J. Social Sustainability and Quality of Working Life. In Sustainability and Human Resource Management: Developing Sustainable Business Organizations; Ehnert, I., Harry, W., Zink, K.J., Eds.; Springer: Berlin, Heidelberg, 2014; pp. 35–55. ISBN 978-3-642-37524-8. [Google Scholar]
- Ehnert, I.; Harry, W.; Zink, K.J. Sustainability and HRM. In Sustainability and Human Resource Management: Developing Sustainable Business Organizations; Ehnert, I., Harry, W., Zink, K.J., Eds.; Springer: Berlin, Heidelberg, 2014; pp. 3–32. ISBN 978-3-642-37524-8. [Google Scholar]
- Meyer, F.; Eweje, G.; Tappin, D. Ergonomics as a tool to improve the sustainability of the workforce. WORK 2017, 57, 339–350. [Google Scholar] [CrossRef]
- National Research Council and Institute of Medicine. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities; National Academy Press: Washington, DC, USA, 2001; ISBN 0-309-07284-0. [Google Scholar]
- Larsman, P.; Lindegård, A.; Ahlborg, G., Jr. Longitudinal relations between psychosocial work environment, stress and the development of musculoskeletal pain. Stress Health 2011, 27, e228–e237. [Google Scholar] [CrossRef]
- Kee, D. Comparison of LEBA and RULA Based on Postural Load Criteria and Epidemiological Data on Musculoskeletal Disorders. Int. J. Environ. Res. Public Health 2022, 19, 3967. [Google Scholar] [CrossRef]
- Winkel, J.; Westgaard, R. Occupational and individual risk factors for shoulder-neck complaints: Part II—The scientific basis (literature review) for the guide. Int. J. Ind. Ergon. 1992, 10, 85–104. [Google Scholar] [CrossRef]
- Wilson, D.J.; Hickey, K.M.; Gorham, J.L.; Childers, M.K. Lumbar spinal moments in chronic back pain patients during supported lifting: A dynamic analysis. Arch. Phys. Med. Rehabil. 1997, 78, 967–972. [Google Scholar] [CrossRef]
- Fredriksson, K.; Bildt, C.; Hägg, G.; Kilbom, Å. The impact on musculoskeletal disorders of changing physical and psychosocial work environment conditions in the automobile industry. Int. J. Ind. Ergon. 2001, 28, 31–45. [Google Scholar] [CrossRef]
- Adams, R.; Nino, V. Work-Related Psychosocial Factors and Their Effects on Mental Workload Perception and Body Postures. Int. J. Environ. Res. Public Health 2024, 21, 876. [Google Scholar] [CrossRef]
- Naweed, A.; Bowditch, L.; Trigg, J.; Unsworth, C. Injury by design: A thematic networks and system dynamics analysis of work-related musculoskeletal disorders in tram drivers. Appl. Ergon. 2022, 100, 103644. [Google Scholar] [CrossRef]
- Bovenzi, M. A prospective cohort study of neck and shoulder pain in professional drivers. Ergonomics 2015, 58, 1103–1116. [Google Scholar] [CrossRef]
- Tan, C.F.; Chen, W.; Delbressine, F.; Rauterberg, M. Objectifying discomfort seat measurement for next generation truck driver’s seat. In Proceedings of the FISITA World Automotive Congress, Munich, Germany, 14–19 September 2008. [Google Scholar]
- Das, S. Soumyajit Das Comparative Ergonomic Review Study of common Road-transport Drivers. SSRN 2021, 3855769. [Google Scholar] [CrossRef]
- Gao, K.; Du, J.; Ding, R.; Zhang, Z. Lumbar spinal loads and lumbar muscle forces evaluation with various lumbar supports and backrest inclination angles in driving posture. Eur. Spine J. 2023, 32, 408–419. [Google Scholar] [CrossRef]
- Roossien, C.C.; Baten, C.T.; van der Waard, M.W.; Reneman, M.F.; Verkerke, G.J. Automatically Determining Lumbar Load during Physically Demanding Work: A Validation Study. Sensors 2021, 21, 2476. [Google Scholar] [CrossRef]
- Lis, A.M.; Black, K.M.; Korn, H.; Nordin, M. Association between sitting and occupational LBP. Eur. Spine J. 2007, 16, 283–298. [Google Scholar] [CrossRef]
- Bhattacharya, A. Costs of occupational musculoskeletal disorders (MSDs) in the United States. Int. J. Ind. Ergon. 2014, 44, 448–454. [Google Scholar] [CrossRef]
- Khan, I.A.; Deb, R.K. Postural Analysis Through RULA, REBA And QEC of Vendors Selling Edible Items At Railway Stations And In The Trains. Int. J. Eng. Adv. Technol. IJEAT 2019, 9, 7269–7277. [Google Scholar] [CrossRef]
- Rahman, C.M. Study and Analysis of Work Postures of Workers working in a Ceramic Industry through Rapid Upper Limb Assessment (RULA). Int. J. Eng. Appl. Sci. 2014, 5, 14–20. [Google Scholar]
- Pandarinath, M.; Rao, T.R.; Venkatesh, S. Ramamohan Rao; Sriram Venkatesh Evaluation of Drivers Seating Posture by REBA Analysis. J. Mobil. Technol. 2024, 4, 1138–1146. [Google Scholar] [CrossRef]
- Westgaard, R.H.; Winkel, J. Ergonomic intervention research for improved musculoskeletal health: A critical review. Int. J. Ind. Ergon. 1997, 20, 463–500. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet Lond. Engl. 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Arslan, S.A.; Hadian, M.R.; Olyaei, G.; Talebian, S.; Yekaninejad, M.S.; Hussain, M.A. Comparative effect of driving side on low back pain due to Repetitive Ipsilateral Rotation. Pak. J. Med. Sci. 2019, 35, 1018–1023. [Google Scholar] [CrossRef]
- Kee, D. Systematic Comparison of OWAS, RULA, and REBA Based on a Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 595. [Google Scholar] [CrossRef]
- Choobineh, A.; Tabatabaei, S.H.; Tozihian, M.; Ghadami, F. Musculoskeletal problems among workers of an Iranian communication company. Indian J. Occup. Environ. Med. 2007, 11, 32–36. [Google Scholar] [CrossRef]
- Labbafinejad, Y.; Imanizade, Z.; Danesh, H. Ergonomic Risk Factors and Their Association With Lower Back and Neck Pain Among Pharmaceutical Employees in Iran. Workplace Health Saf. 2016, 64, 586–595. [Google Scholar] [CrossRef]
- Bertrand, S.; Skalli, W.; Delacherie, L.; Bonneau, D.; Kalifa, G.; Mitton, D. External and internal geometry of European adults. Ergonomics 2006, 49, 1547–1564. [Google Scholar] [CrossRef]
- Casadei, K.; Kiel, J. Anthropometric Measurement. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- National Health and Nutrition Examination Survey (U.S.); National Center for Health Statistics (U.S.); Westat (Eds.) National Health and Nutrition Examination Survey III: Body Measurements (Anthropometry); Centers for Disease Control and Prevention: Rockville, MD, USA, 1988. [Google Scholar]
- ISSA Section Machine and System Safety: Anthropometrics. Available online: https://www.safe-machines-at-work.org/human-factors/work-place-design-issues/design-to-fit-body-dimensions/anthropometrics (accessed on 10 July 2025).
- Muftić, O.; Ibrahimagić, L.; Milčić, D. The Compact Formulation of Anthropodynamical Measures in Physiological Anthropology. Coll. Antropol. 2001, 25, 269–277. [Google Scholar]
- Muftić, O.; Jurčević Lulić, T.; Godan, B. Harmonic distribution of the segmental masses of the human body. Sigurnost 2011, 53, 1–10. [Google Scholar]
- Halek, R.B.A.; Dev, A.; Chew, K.H.; Hannan, M.A. Evaluation of Validity and Reliability of Rapid Upper Limb Assessment (RULA) Method in Research Experiment: A Systematic Review. Open J. Saf. Sci. Technol. 2025, 15, 1–13. [Google Scholar] [CrossRef]
- Landekić, M.; Bačić, M.; Bakarić, M.; Šporčić, M.; Pandur, Z. Working Posture and the Center of Mass Assessment While Starting a Chainsaw: A Case Study among Forestry Workers in Croatia. Forests 2023, 14, 395. [Google Scholar] [CrossRef]
- Marras, W.S.; Knapik, G.G.; Ferguson, S. Loading along the lumbar spine as influence by speed, control, load magnitude, and handle height during pushing. Clin. Biomech. Bristol Avon 2009, 24, 155–163. [Google Scholar] [CrossRef]
- Sahin, A.; Eldem, C. Ergonomic evaluation of USB used in buses. Selcuk Univ. J. Eng. Sci. 2021, 21, 131–137. [Google Scholar]
- Mihăilă, D.; Iordache, R.M.; Petreanu, V. Dorsopathy in urban public transport drivers in relation to occupational risks and workloads. MATEC Web Conf. 2021, 342, 01018. [Google Scholar] [CrossRef]
- Gao, Y.; Kaiser, R.; Wagner, P.-O.; Abendroth, B.; Paternoster, S. Driving Posture Assessment: A New Approach. In Proceedings of the 21st Congress of the International Ergonomics Association (IEA 2021), Online, 13–18 June 2021; Black, N.L., Neumann, W.P., Noy, I., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 639–646. [Google Scholar]
- Buchman-Pearle, J.M.; Fewster, K.M.; Pinto, B.L.; Callaghan, J.P. Moving Toward Individual-Specific Automotive Seat Design: How Individual Characteristics and Time Alter the Selected Lumbar Support Prominence. Hum. Factors 2023, 65, 1394–1406. [Google Scholar] [CrossRef]
- Yasobant, S.; Chandran, M.; Reddy, E.M. Are Bus Drivers at an Increased Risk for Developing Musculoskeletal Disorders? An Ergonomic Risk Assessment Study. J. Ergon. 2015, 3, 1–5. [Google Scholar]
- Das, S.; Patra, S.; Danda, S.; Mallick, B.; Pandey, A. Working Posture Evaluation of Bus Drivers—Using CMDQ and RULA Technique. In Proceedings of the International Conference of the Indian Society of Ergonomics, Aligarh, India, 8–10 December 2021; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Saftarina, F.; Mayasari, D.; Octaviani, D. Analysis of Work Posture Using Rapid Entire Body Assessment (REBA) as the Risk Factor of Work Related Musculoskeletal Disorders in Inter-provincial Bus Drivers. BMC Public Health 2017, 17, 897. [Google Scholar]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- ISO 7250-1:2017; Basic Human Body Measurements for Technological Design—Part 1: Body Measurement Definitions and Landmarks. ISO: Geneva, Switzerland, 2017. Available online: https://www.iso.org/standard/65246.html (accessed on 10 July 2025).
- Chaffin, D.B.; Andersson, G.B.; Martin, B.J. Occupational Biomechanics; John Wiley & Sons: Hoboken, NJ, USA, 2006; ISBN 0-471-72343-6. [Google Scholar]
- Elbert, K.K. Fitting the Human—Introduction to Ergonomics/Human Factors Engineering; CRC Press Taylor & Francis Group: Boca Raton, FL, USA, 2017; ISBN 978-1-498-4689-2. [Google Scholar]
- DIN 33402-2:2005-12; Ergonomics—Human Body Dimensions—Part 2: Values. DIN Media: Berlin, Germany, 2005. Available online: https://www.dinmedia.de/en/standard/din-33402-2/84092742 (accessed on 10 July 2025).
- Neufert, E.; Neufert, P. Neufert Architects’ Data; Wiley-Blackwell: Hoboken, NJ, USA, 2012. [Google Scholar]
- ISO 3411:2007; Earth-moving machinery — Physical dimensions of operators and minimum operator space envelope. ISO: Geneva, Switzerland, 2017. Available online: https://www.iso.org/standard/38911.html (accessed on 10 July 2025).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TallM | MidM | SmallW | ||||
|---|---|---|---|---|---|---|
| Height, cm | 184.8 | 179.6 | 159.1 | |||
| Mass, kg | 100.2 | 76.1 | 50.4 | |||
| Weight force, N | Length, cm | Weight force, N | Length, cm | Weight force, N | Length, cm | |
| Foot | 12.7 | 23.1 | 10.5 | 22.5 | 5.7 | 19.9 |
| Lower leg | 37.4 | 40.4 | 29.3 | 39.3 | 27.4 | 34.8 |
| Thigh | 140.0 | 52.0 | 105.4 | 50.5 | 75.8 | 44.7 |
| Hand | 5.6 | 20.2 | 4.6 | 19.6 | 2.8 | 17.4 |
| Forearm | 15.3 | 23.1 | 11.9 | 22,5 | 7.8 | 19.9 |
| Upper arm | 27.2 | 28.9 | 20.2 | 28.1 | 14.9 | 24.9 |
| Head and neck | 55.2 | 32.2 | 50.4 | 31.3 | 46.3 | 29.6 |
| Upper trunk | 158.5 | 21.0 | 117.4 | 20.5 | 61.7 | 15.4 |
| Mid-trunk | 169.8 | 19.7 | 120.4 | 18,4 | 75.8 | 16.5 |
| Lower trunk | 111.2 | 13.7 | 85.6 | 14.0 | 55.6 | 13.0 |
| TallM | MidM | SmallW | |
|---|---|---|---|
| RULA | 6 | 6 | 6 |
| REBA | 6 | 6 | 6 |
| L4/L5, Nm | 101.67 | 71.12 | 51.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leder Horina, J.; Blašković Zavada, J.; Slavulj, M.; Budimir, D. Ergonomics Study of Musculoskeletal Disorders Among Tram Drivers. Appl. Sci. 2025, 15, 8348. https://doi.org/10.3390/app15158348
Leder Horina J, Blašković Zavada J, Slavulj M, Budimir D. Ergonomics Study of Musculoskeletal Disorders Among Tram Drivers. Applied Sciences. 2025; 15(15):8348. https://doi.org/10.3390/app15158348
Chicago/Turabian StyleLeder Horina, Jasna, Jasna Blašković Zavada, Marko Slavulj, and Damir Budimir. 2025. "Ergonomics Study of Musculoskeletal Disorders Among Tram Drivers" Applied Sciences 15, no. 15: 8348. https://doi.org/10.3390/app15158348
APA StyleLeder Horina, J., Blašković Zavada, J., Slavulj, M., & Budimir, D. (2025). Ergonomics Study of Musculoskeletal Disorders Among Tram Drivers. Applied Sciences, 15(15), 8348. https://doi.org/10.3390/app15158348