

Potential Benefits of Polar Transformation of Time–Frequency Electrocardiogram (ECG) Signals for Evaluation of Cardiac Arrhythmia


Abstract
Featured Applications
Abstract
1. Introduction
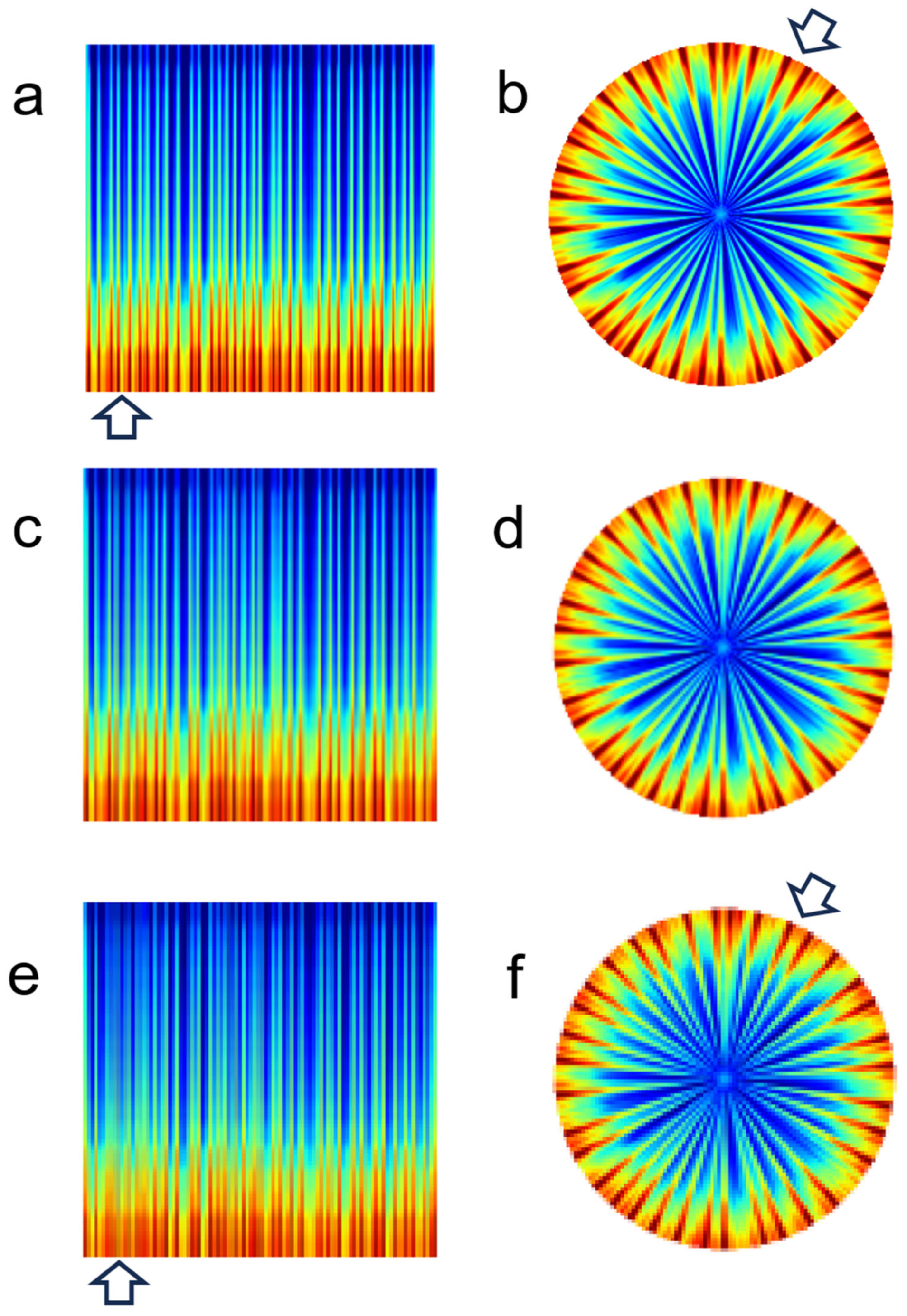
- We demonstrated the advantage of polar-transformed ECG spectrograms in approximately 30 s ECG signals compared to conventional rectangular spectrograms.
- We investigated the effects of image resolution on visualization quality in both rectangular and polar spectrograms.
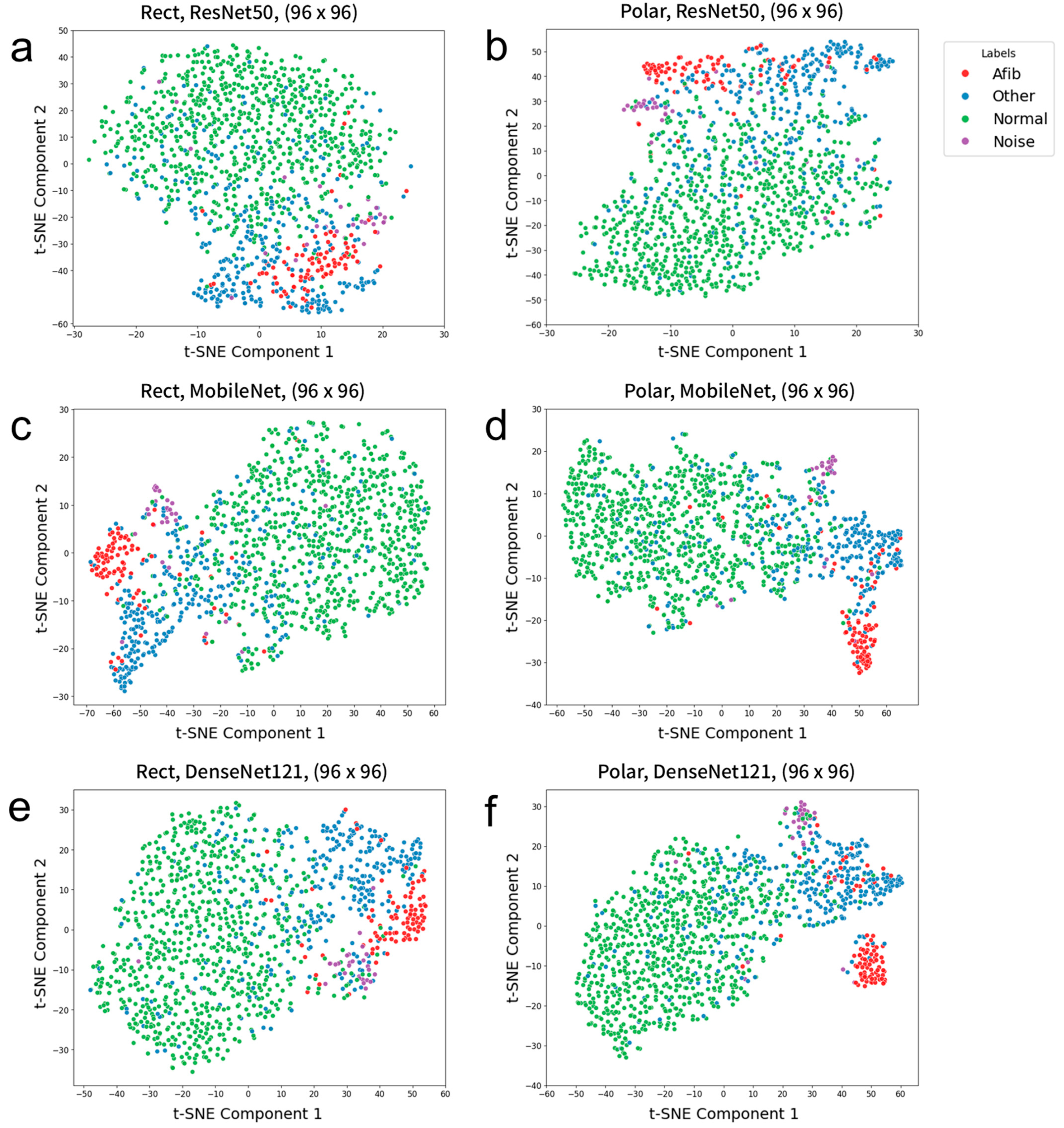
- We assessed the effects of image resolution on deep CNN prediction performance for both rectangular and polar spectrograms.
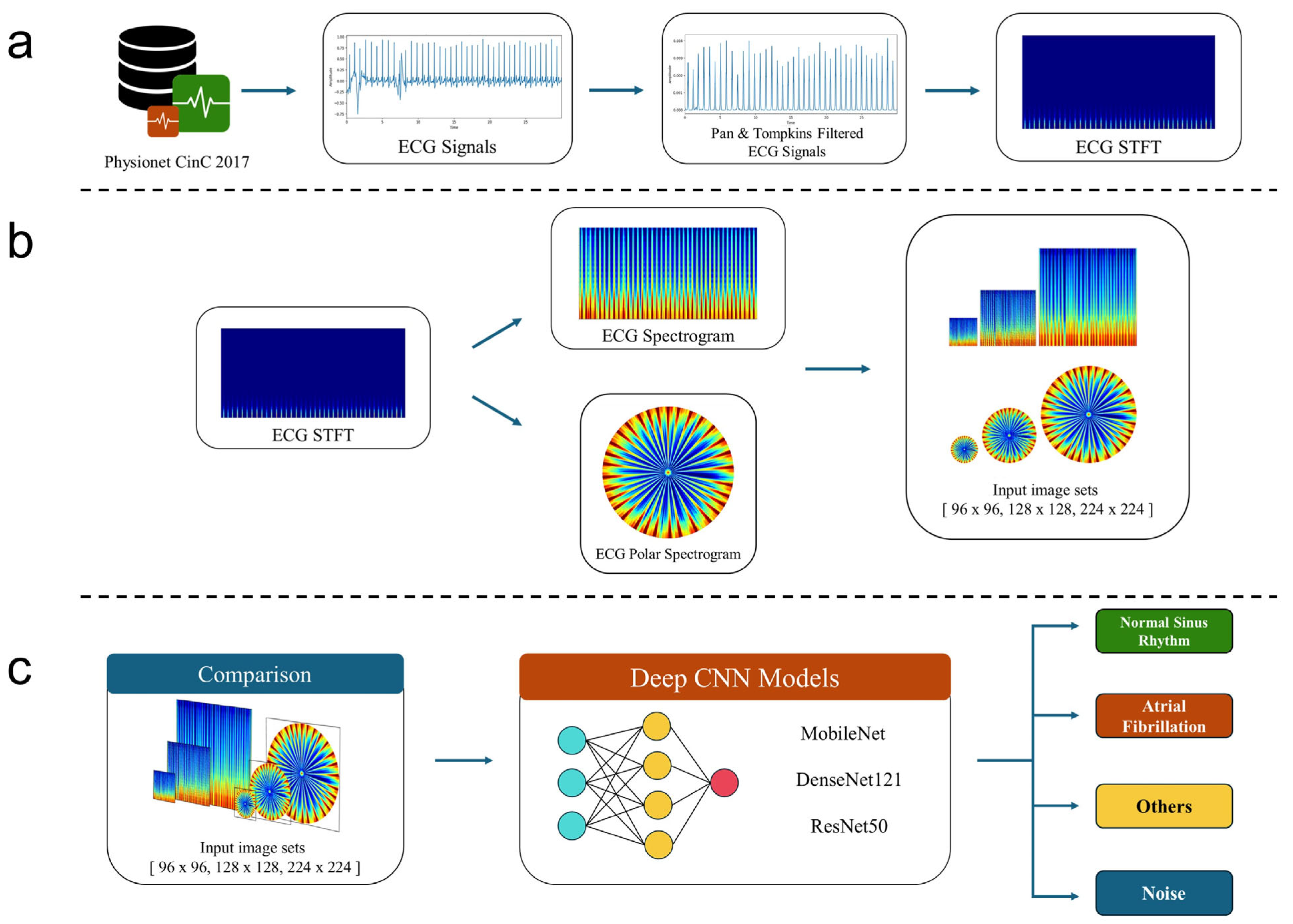
2. Materials and Methods
2.1. Data
2.2. Preprocessing of ECG Signals
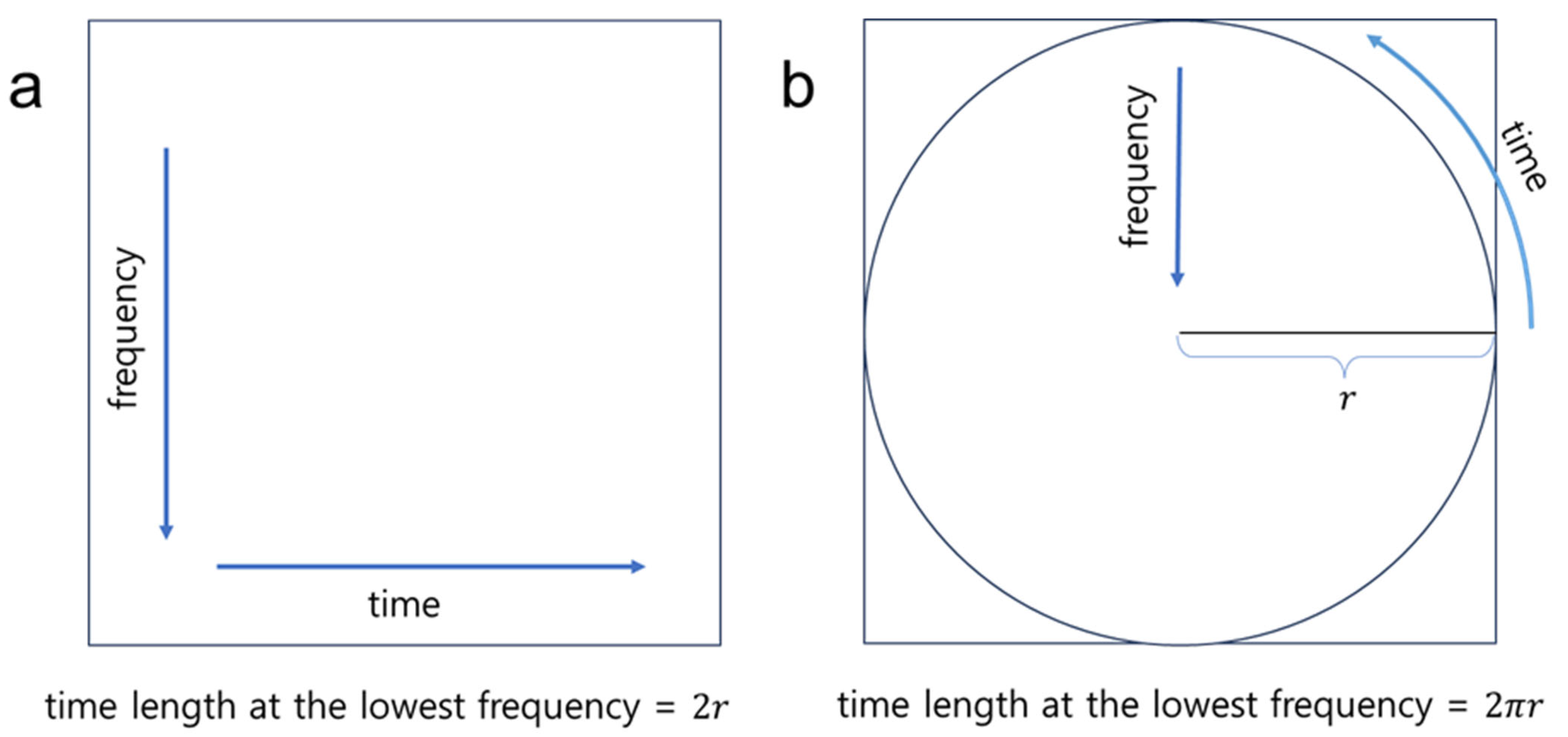
2.3. Polar Transformation
2.4. Deep Learning
2.5. Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ECG | Electrocardiogram |
| AI | Artificial intelligence |
| CinC | Computers in cardiology |
| 1-D | One-dimensional |
| 2-D | Two-dimensional |
| CNN | Convolutional neural network |
| LSTM | Long short-term memory |
| STFT | Short-time Fourier transform |
| PC | Personal computer |
| RAM | Random access memory |
| P-T | Pan–Tompkins |
| GAP | Global average pooling |
| SSIM | Structural similarity index measure |
| PSNR | Peak signal-to-noise ratio |
| t-SNE | t-distributed stochastic neighbor embedding |
| F1A | F1-score of the atrial fibrillation class |
| F1N | F1-score of the normal sinus rhythm class |
| F1O | F1-score of the other rhythm class |
References
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1–e156. [Google Scholar] [CrossRef] [PubMed]
- Sanna, T.; Diener, H.C.; Passman, R.S.; Crystal, A.F.S.C. Cryptogenic stroke and atrial fibrillation. N. Engl. J. Med. 2014, 371, 1261. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.Y.; Qaraqe, M.; Charafeddine, F.; Serpedin, E.; Righetti, R.; Qaraqe, K. Estimating age and gender from electrocardiogram signals: A comprehensive review of the past decade. Artif. Intell. Med. 2023, 146, 102690. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, Z.; Loni, M.; Daneshtalab, M.; Gharehbaghi, A. A review on deep learning methods for ECG arrhythmia classification. Expert Syst. Appl. X 2020, 7, 100033. [Google Scholar] [CrossRef]
- Kumar, A.; Kumar, S.A.; Dutt, V.; Dubey, A.K.; García-Díaz, V. IoT-based ECG monitoring for arrhythmia classification using Coyote Grey Wolf optimization-based deep learning CNN classifier. Biomed. Signal Process. Control 2022, 76, 103638. [Google Scholar] [CrossRef]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Tesfai, H.; Saleh, H.; Al-Qutayri, M.; Mohammad, M.B.; Tekeste, T.; Khandoker, A.; Mohammad, B. Lightweight Shufflenet Based CNN for Arrhythmia Classification. IEEE Access 2022, 10, 111842–111854. [Google Scholar] [CrossRef]
- Cao, P.; Li, X.Y.; Mao, K.D.; Lu, F.; Ning, G.M.; Fang, L.P.; Pan, Q. A novel data augmentation method to enhance deep neural networks for detection of atrial fibrillation. Biomed. Signal Process. Control 2020, 56, 101675. [Google Scholar] [CrossRef]
- Song, M.S.; Lee, S.B. Comparative study of time-frequency transformation methods for ECG signal classification. Front. Signal Process. 2024, 4, 1322334. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Proceedings of the Computer Vision–ECCV 2016: 14th European Conference, Amsterdam, The Netherlands, 11–14 October 2016; Proceedings, Part IV 14. pp. 630–645. [Google Scholar]
- Alzubaidi, L.; Zhang, J.L.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data-Ger. 2021, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Li, F.F. ImageNet: A Large-Scale Hierarchical Image Database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar] [CrossRef]
- Al Rahhal, M.M.; Bazi, Y.; Al Zuair, M.; Othman, E.; BenJdira, B. Convolutional Neural Networks for Electrocardiogram Classification. J. Med. Biol. Eng. 2018, 38, 1014–1025. [Google Scholar] [CrossRef]
- Eltrass, A.S.; Tayel, M.B.; Ammar, A. A new automated CNN deep learning approach for identification of ECG congestive heart failure and arrhythmia using constant-Q non-stationary Gabor transform. Biomed. Signal Process. 2021, 65, 102326. [Google Scholar] [CrossRef]
- Çinar, A.; Tuncer, S.A. Classification of normal sinus rhythm, abnormal arrhythmia and congestive heart failure ECG signals using LSTM and hybrid CNN-SVM deep neural networks. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.S.; Chen, B.Q.; Yao, B.; He, W.P. ECG Arrhythmia Classification Using STFT-Based Spectrogram and Convolutional Neural Network. IEEE Access 2019, 7, 92871–92880. [Google Scholar] [CrossRef]
- Khorrami, H.; Moavenian, M. A comparative study of DWT, CWT and DCT transformations in ECG arrhythmias classification. Expert Syst. Appl. 2010, 37, 5751–5757. [Google Scholar] [CrossRef]
- Krak, I.; Stelia, O.; Pashko, A.; Efremov, M.; Khorozov, O. Electrocardiogram classification using wavelet transformations. In Proceedings of the 2020 IEEE 15th International Conference on Advanced Trends in Radioelectronics, Telecommunications and Computer Engineering (TCSET), Online, 25–29 February 2020; pp. 930–933. [Google Scholar]
- Li, C.; Zheng, C.; Tai, C. Detection of ECG characteristic points using wavelet transforms. IEEE Trans. Biomed. Eng. 1995, 42, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mewada, H.; Pires, I.M. Electrocardiogram signal classification using lightweight DNN for mobile devices. Procedia Comput. Sci. 2023, 224, 558–564. [Google Scholar] [CrossRef]
- Ozaltin, O.; Yeniay, O. A novel proposed CNN–SVM architecture for ECG scalograms classification. Soft Comput. 2023, 27, 4639–4658. [Google Scholar] [CrossRef] [PubMed]
- Rashidah Funke, O.; Ibrahim, S.N.; Ani Liza, A.; Hunain, A. Classification of ECG signals for detection of arrhythmia and congestive heart failure based on continuous wavelet transform and deep neural networks. Indones. J. Electr. Eng. Comput. Sci. 2021, 22, 1520–1528. [Google Scholar] [CrossRef]
- Kwon, D.; Kang, H.; Lee, D.; Kim, Y.C. Deep learning-based prediction of atrial fibrillation from polar transformed time-frequency electrocardiogram. PLoS ONE 2025, 20, e0317630. [Google Scholar] [CrossRef] [PubMed]
- Zhivomirov, H. A novel visual representation of the signals in the time-frequency domain. UPB Sci. Bull. Ser. C Electr. Eng. Comput. Sci. 2018, 80, 75–84. [Google Scholar]
- Alqudah, A.M.; Alqudah, A. Deep learning for single-lead ECG beat arrhythmia-type detection using novel iris spectrogram representation. Soft Comput. 2022, 26, 1123–1139. [Google Scholar] [CrossRef]
- Zyout, A.; Alquran, H.; Mustafa, W.A.; Alqudah, A.M. Advanced Time-Frequency Methods for ECG Waves Recognition. Diagnostics 2023, 13, 308. [Google Scholar] [CrossRef] [PubMed]
- Obeidat, Y.; Alqudah, A.M. A hybrid lightweight 1D CNN-LSTM architecture for automated ECG beat-wise classification. Trait. Du Signal 2021, 38, 1281–1291. [Google Scholar] [CrossRef]
- Banerjee, R.; Ghose, A. A Light-Weight Deep Residual Network for Classification of Abnormal Heart Rhythms on Tiny Devices. In Proceedings of the Joint European Conference on Machine Learning and Knowledge Discovery in Databases, Turin, Italy, 18–22 September 2023; Volume 1753, pp. 317–331. [Google Scholar] [CrossRef]
- Clifford, G.D.; Liu, C.; Moody, B.; Li-wei, H.L.; Silva, I.; Li, Q.; Johnson, A.; Mark, R.G. AF classification from a short single lead ECG recording: The PhysioNet/computing in cardiology challenge 2017. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods. 2020, 17, 352. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.I.; Meyer, C.H.; Nishimura, D.G.; Macovski, A. Selection of a convolution function for Fourier inversion using gridding (computerised tomography application). IEEE Trans. Med. Imaging 1991, 10, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F.O. Deep Learning with Python, 2nd ed.; Manning Publications: Shelter Island, NY, USA, 2021; pp. 68–94. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Hore, A.; Ziou, D. Image quality metrics: PSNR vs. SSIM. In Proceedings of the 2010 20th International Conference on Pattern Recognition, Istanbul, Turkey, 23–26 August 2010; pp. 2366–2369. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Merenda, M.; Porcaro, C.; Iero, D. Edge Machine Learning for AI-Enabled IoT Devices: A Review. Sensors 2020, 20, 2533. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Pal, S.; Yearwood, J.; Karmakar, C. Analysing performances of DL-based ECG noise classification models deployed in memory-constraint IoT-enabled devices. IEEE Trans. Consum. Electron. 2024, 70, 704–714. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Model Development | Test |
|---|---|---|
| Atrial fibrillation (Afib) | 409 | 90 |
| Normal sinus rhythm | 2924 | 754 |
| Other rhythm | 1352 | 323 |
| Noise | 96 | 29 |
| Total | 4781 | 1196 |
| Image Dimensions | Metric | Rect | Polar | p-Value |
|---|---|---|---|---|
| 128 × 128 | SSIM | 0.748 ± 0.053 | 0.880 ± 0.012 | <0.001 |
| PSNR | 17.20 ± 1.37 (dB) | 21.05 ± 1.01 (dB) | <0.001 | |
| 96 × 96 | SSIM | 0.576 ± 0.081 | 0.790 ± 0.019 | <0.001 |
| PSNR | 14.94 ± 1.43 (dB) | 18.59 ± 1.01 (dB) | <0.001 |
| Baseline Network | Input Image Dimensions | The Number of Weight/Bias Parameters in the Baseline network | The Number of Weight/Bias Parameters in the Dense Layers | Feature Map Dimensions (After the First Layer of the Baseline Network) | Feature Map Dimensions (After the Last Layer of the Baseline Network) |
|---|---|---|---|---|---|
| ResNet50 | 96 × 96 | 23,587,712 | 23,719,364 | (64, 48, 48) | (2048, 3, 3) |
| 128 × 128 | 23,587,712 | 23,719,364 | (64, 64, 64) | (2048, 4, 4) | |
| 224 × 224 | 23,587,712 | 23,719,364 | (64, 112, 112) | (2048, 7, 7) | |
| MobileNet | 96 × 96 | 3,228,864 | 3,294,980 | (32, 48, 48) | (1024, 3, 3) |
| 128 × 128 | 3,228,864 | 3,294,980 | (32, 64, 64) | (1024, 4, 4) | |
| 224 × 224 | 3,228,864 | 3,294,980 | (32, 112, 112) | (1024, 7, 7) | |
| DenseNet121 | 96 × 96 | 7,037,504 | 7,103,620 | (64, 48, 48) | (1024, 3, 3) |
| 128 × 128 | 7,037,504 | 7,103,620 | (64, 64, 64) | (1024, 4, 4) | |
| 224 × 224 | 7,037,504 | 7,103,620 | (64, 112, 112) | (1024, 7, 7) |
| Baseline Network | Input Image Dimensions | Type | F1A | F1N | F1O | Macro F1-Score | Macro Precision | Macro Recall | Accuracy |
|---|---|---|---|---|---|---|---|---|---|
| ResNet50 | 96 × 96 | Rect | 0.6338 | 0.8879 | 0.6401 | 0.7206 | 0.6727 | 0.8092 | 0.8743 |
| Polar | 0.7681 | 0.7284 | 0.6503 | 0.7681 | 0.7284 | 0.8283 | 0.8820 | ||
| 128 × 128 | Rect | 0.7058 | 0.9072 | 0.6938 | 0.7690 | 0.7283 | 0.8307 | 0.8937 | |
| Polar | 0.7483 | 0.8901 | 0.6531 | 0.7638 | 0.7638 | 0.8206 | 0.8806 | ||
| 224 × 224 | Rect | 0.7619 | 0.9100 | 0.7338 | 0.8019 | 0.7791 | 0.8301 | 0.9025 | |
| Polar | 0.7607 | 0.9052 | 0.7069 | 0.7909 | 0.8299 | 0.7617 | 0.8931 | ||
| MobileNet | 96 × 96 | Rect | 0.7354 | 0.8895 | 0.6432 | 0.7560 | 0.7151 | 0.8202 | 0.8797 |
| Polar | 0.7034 | 0.8920 | 0.6505 | 0.7486 | 0.6989 | 0.8355 | 0.8806 | ||
| 128 × 128 | Rect | 0.7600 | 0.9052 | 0.7164 | 0.7930 | 0.7456 | 0.8646 | 0.8974 | |
| Polar | 0.7625 | 0.8903 | 0.6857 | 0.7795 | 0.7521 | 0.8155 | 0.8843 | ||
| 224 × 224 | Rect | 0.8275 | 0.9148 | 0.7390 | 0.8271 | 0.8049 | 0.8601 | 0.9103 | |
| Polar | 0.8068 | 0.9001 | 0.6967 | 0.7968 | 0.7786 | 0.8375 | 0.8943 | ||
| DenseNet121 | 96 × 96 | Rect | 0.7058 | 0.8928 | 0.7012 | 0.7666 | 0.7375 | 0.8110 | 0.8846 |
| Polar | 0.7382 | 0.8970 | 0.7091 | 0.7814 | 0.7431 | 0.8422 | 0.8903 | ||
| 128 × 128 | Rect | 0.7600 | 0.9052 | 0.6987 | 0.7880 | 0.7365 | 0.8741 | 0.8977 | |
| Polar | 0.7790 | 0.9079 | 0.6929 | 0.7933 | 0.7678 | 0.8339 | 0.8983 | ||
| 224 × 224 | Rect | 0.8284 | 0.9150 | 0.7529 | 0.8321 | 0.8069 | 0.8641 | 0.9117 | |
| Polar | 0.8132 | 0.9179 | 0.7079 | 0.8238 | 0.8488 | 0.7841 | 0.8993 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, H.; Kwon, D.; Kim, Y.-C. Potential Benefits of Polar Transformation of Time–Frequency Electrocardiogram (ECG) Signals for Evaluation of Cardiac Arrhythmia. Appl. Sci. 2025, 15, 7980. https://doi.org/10.3390/app15147980
Kang H, Kwon D, Kim Y-C. Potential Benefits of Polar Transformation of Time–Frequency Electrocardiogram (ECG) Signals for Evaluation of Cardiac Arrhythmia. Applied Sciences. 2025; 15(14):7980. https://doi.org/10.3390/app15147980
Chicago/Turabian StyleKang, Hanbit, Daehyun Kwon, and Yoon-Chul Kim. 2025. "Potential Benefits of Polar Transformation of Time–Frequency Electrocardiogram (ECG) Signals for Evaluation of Cardiac Arrhythmia" Applied Sciences 15, no. 14: 7980. https://doi.org/10.3390/app15147980
APA StyleKang, H., Kwon, D., & Kim, Y.-C. (2025). Potential Benefits of Polar Transformation of Time–Frequency Electrocardiogram (ECG) Signals for Evaluation of Cardiac Arrhythmia. Applied Sciences, 15(14), 7980. https://doi.org/10.3390/app15147980