
Information Merging for Improving Automatic Classification of Electrical Impedance Mammography Images

 , and
, and
Abstract
1. Introduction
2. Related Work
3. Materials and Methods
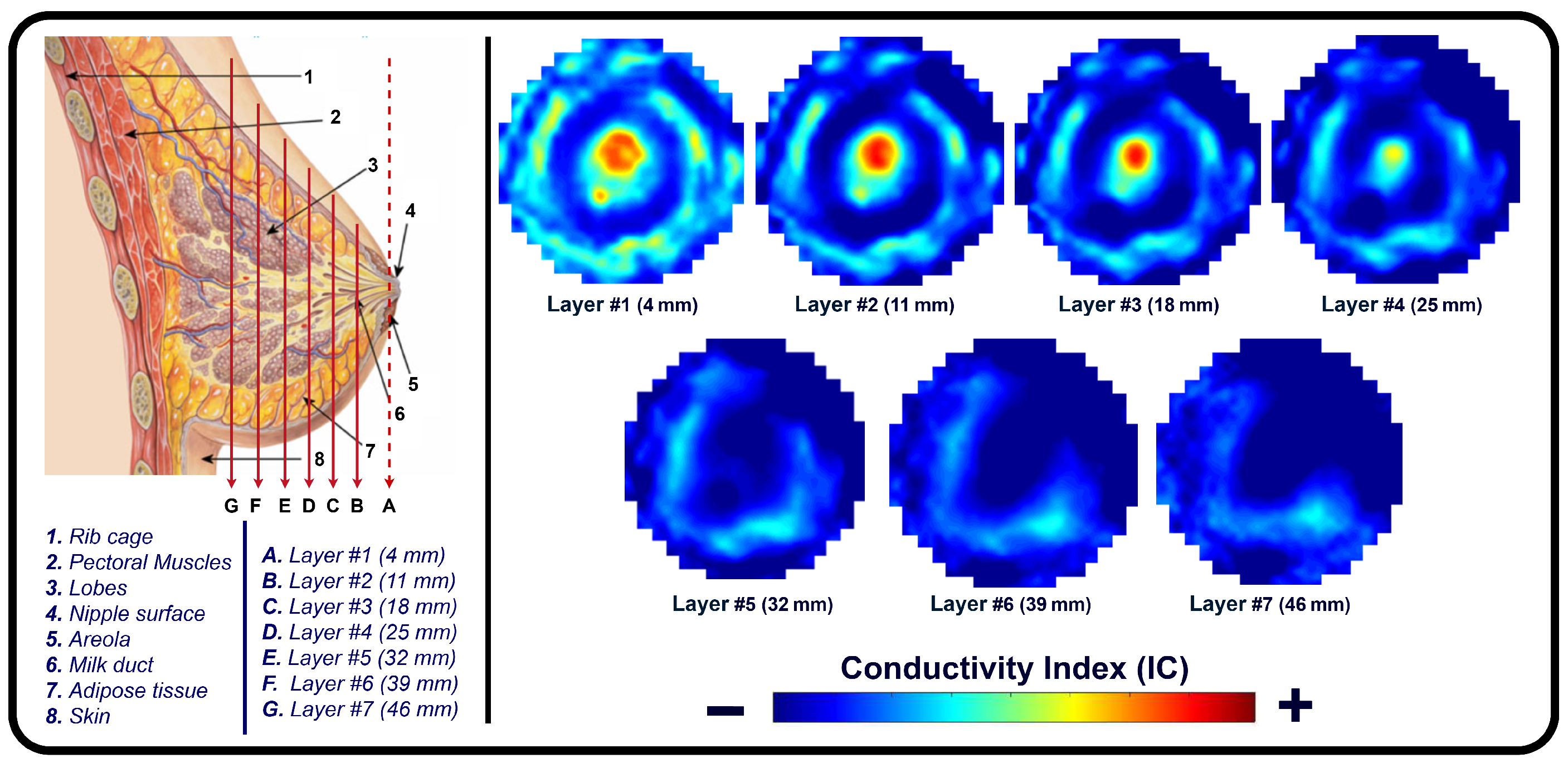
3.1. Electrical Impedance Mammography (EIM)
3.2. MEX-IEM Dataset
3.3. EIM Data Processing and Classification
3.3.1. Integration Methods
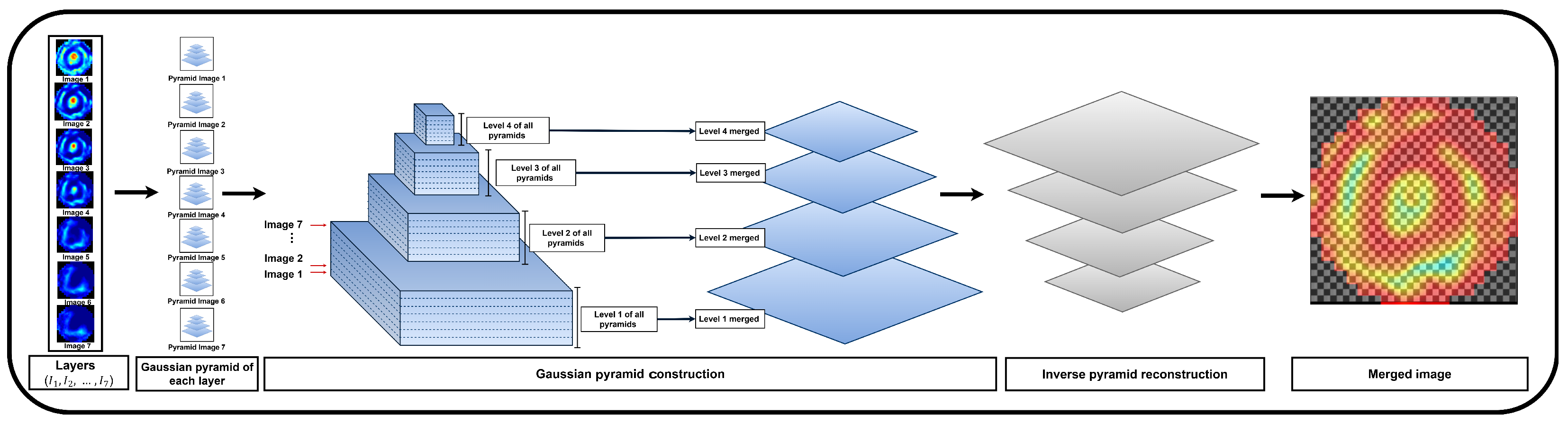
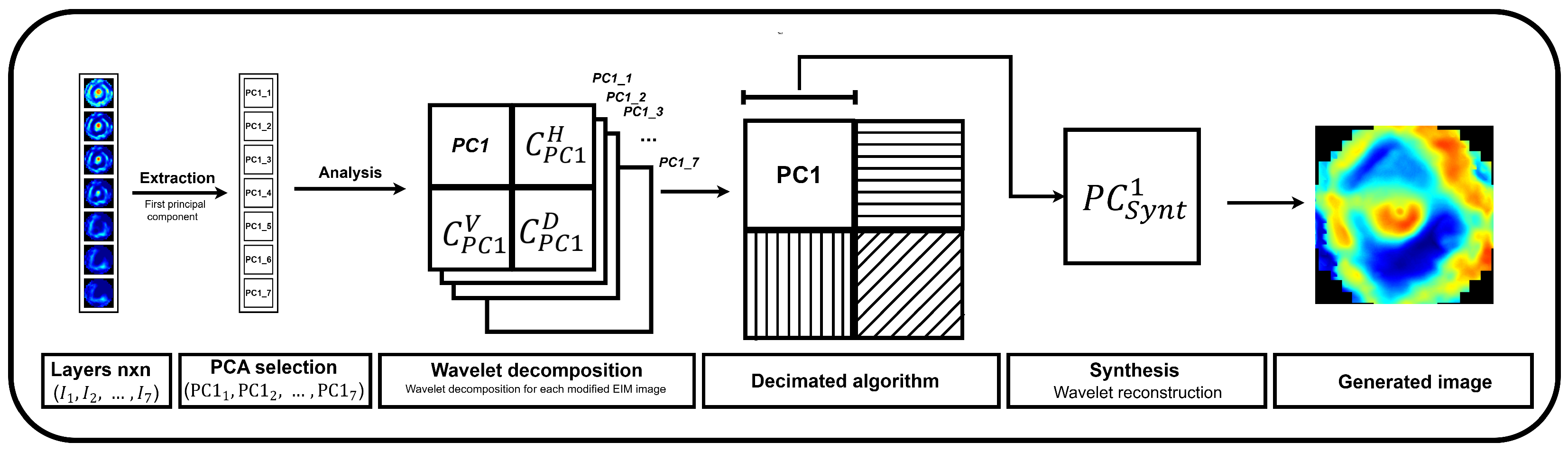
3.3.2. Fusion Methods
3.3.3. Feature Extraction and Classification
4. Results
Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Breast Cancer. In WHO Fact Sheets; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- INEGI. Estadisticas a Propósito del Día Internacional de la Lucha Contra el Cáncer de Mama (19 de Octubre); Comunicado de prensa número 595/23; INEGI: Aguascalientes, Mexico, 2023. [Google Scholar]
- Ghadge, D.; Hon, S.; Saraf, T.; Wagh, T.; Tambe, A.; Deshmukh, Y. Analysis on Machine Learning-Based Early Breast Cancer Detection. In Proceedings of the 2024 4th International Conference on Innovative Practices in Technology and Management (ICIPTM), Noida, India, 21–23 February 2024; pp. 1–5. [Google Scholar] [CrossRef]
- National Breast and Ovarian Cancer Centre. Breast Cancer Risk Factors: A Review of the Evidence; National Breast and Ovarian Cancer Centre: Surry Hills, NSW, Australia, 2009. [Google Scholar]
- Mendelson, E.B.; Baum, J.K.; Berg, W.A.; Merritt, C.R.; Rubin, E. ACR BI-RADS® Mammography. Breast Imaging Report. Data Syst. (BI-RADS) 2001, 4, 43–53. [Google Scholar]
- Samala, R.K.; Chan, H.P.; Hadjiiski, L.; Helvie, M.A.; Richter, C.D.; Cha, K.H. Breast Cancer Diagnosis in Digital Breast Tomosynthesis: Effects of Training Sample Size on Multi-Stage Transfer Learning Using Deep Neural Nets. IEEE Trans. Med Imaging 2019, 38, 686–696. [Google Scholar] [CrossRef]
- Poplack, S.P.; Tosteson, A.N.; Kogel, C.A.; Nagy, H.M. Digital breast tomosynthesis: Initial experience in 98 women with abnormal digital screening mammography. AJR Am. J. Roentgenol. 2007, 189, 616–623. [Google Scholar] [CrossRef]
- Henry, N.; Wagner, M.D., Jr.; Peter, S.; Conti, M.D.P. The impact of early detection on cancer survival. J. Clin. Oncol. 2019, 37, 123–132. [Google Scholar]
- Romero Coripuna, R.L.; Hernández Farías, D.I.; Murillo Ortiz, B.O.; Padierna, L.C.; Fraga, T.C. Machine Learning for the Analysis of Conductivity From Mono Frequency Electrical Impedance Mammography as a Breast Cancer Risk Factor. IEEE Access 2021, 9, 152397–152407. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, L.; Wu, Z.; Li, P. Electrical impedance tomography of breast cancer: Clinical trial results. IEEE Trans. Med Imaging 2016, 35, 722–730. [Google Scholar]
- Brown, J.; Wilson, E.; Bradley, P. Electrical impedance spectroscopy for breast cancer diagnosis: A clinical study. J. Clin. Oncol. 2017, 35, 45–52. [Google Scholar]
- Sotskova, N.; Karpov, A.; Korotkova, M.; Sentcha, A. Particularities of electrical impedance images in different forms of growth of infiltrative breast cancer. In Proceedings of the 11th International Conference on Electrical Bioimpedance (ICEBI), Graz, Austria, 29 August–2 September 2007; Scharfetter, H., Merwa, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2007; pp. 560–563. [Google Scholar] [CrossRef]
- Raneta, O.; Ondruš D., B.V. Utilisation of Electrical Impedance Tomography in Breast Cancer Diagnosis. Klin Onkol. 2012, 25, 36–41. [Google Scholar]
- Korotkova, M.; Karpov, A.; Machin, M.; Tsofin, Y.; Tsyplyonkov, V.; Tchayev, A. Electric Impedance Imaging of the Mammary Gland in Circumstances of Skin Abnormality or Damage; Clinical Hospital №9: Yaroslavl, Russia, 2002. [Google Scholar]
- Karpov, A.; Korotkova, M. Diagnostic criteria for mass lesions differentiating in electrical impedance mammography. J. Physics Conf. Ser. 2013, 434, 012053. [Google Scholar] [CrossRef]
- Romero Coripuna, R.L.; Hernández Farías, D.I.; Murillo Ortiz, B.O.; Córdova Fraga, T. Electro-impedance mammograms for automatic breast cancer screening: First insights on Mexican patients. J. Intell. Fuzzy Syst. 2021, 42, 4659–4671. [Google Scholar] [CrossRef]
- Kurinjimalar, R.; Pradeep, J.; Harikrishnan, M. Underwater Image Enhancement Using Gaussian Pyramid, Laplacian Pyramid and Contrast Limited Adaptive Histogram Equalization. In Proceedings of the 2024 IEEE 3rd World Conference on Applied Intelligence and Computing (AIC), Gwalior, India, 27–28 July 2024; pp. 729–734. [Google Scholar] [CrossRef]
- Bhat, M.; S, T.P.M. Adaptive clip limit for contrast limited adaptive histogram equalization (CLAHE) of medical images using least mean square algorithm. In Proceedings of the 2014 IEEE International Conference on Advanced Communications, Control and Computing Technologies, Ramanathapuram, India, 8–10 May 2014; pp. 1259–1263. [Google Scholar] [CrossRef]
- Sousa, A.L.; Villar, S.A.; Korneta, W.; Acosta, G.; Rozenfeld, A. Resonancia estocástica para el mejoramiento del contraste y calidad en imágenes acústicas de sonar de barrido lateral. In Proceedings of the 2016 IEEE Biennial Congress of Argentina (ARGENCON), Buenos Aires, Argentina, 15–17 June 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Chang, C.I.; Liang, C.C.; Hu, P.F. Iterative Gaussian–Laplacian Pyramid Network for Hyperspectral Image Classification. IEEE Trans. Geosci. Remote Sens. 2024, 62, 5510122. [Google Scholar] [CrossRef]
- Reza, A. Realization of the Contrast Limited Adaptive Histogram Equalization (CLAHE) for Real-Time Image Enhancement. J. Vlsi Signal-Process.-Syst. Signal Image Video Technol. 2004, 38, 35–44. [Google Scholar] [CrossRef]
- Wu, J.; Liu, J.; Tian, J.; Yin, B. Wavelet-based Remote Sensing Image Fusion with PCA and Feature Product. In Proceedings of the 2006 International Conference on Mechatronics and Automation, Luoyang, China, 25–28 June 2006; pp. 2053–2057. [Google Scholar] [CrossRef]
- Krishn, A.; Bhateja, V.; Himanshi; Sahu, A. Medical image fusion using combination of PCA and wavelet analysis. In Proceedings of the 2014 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Delhi, India, 24–27 September 2014; pp. 986–991. [Google Scholar] [CrossRef]
- Taxak, N.; Singhal, S. High PSNR based Image Fusion by Weighted Average Brovery Transform Method. In Proceedings of the 2019 Devices for Integrated Circuit (DevIC), Kalyani, India, 23–24 March 2019; pp. 451–455. [Google Scholar] [CrossRef]
- Pessoa, D.; Petmezas, G.; Papageorgiou, V.E.; Rocha, B.M.; Stefanopoulos, L.; Kilintzis, V.; Maglaveras, N.; Frerichs, I.; de Carvalho, P.; Paiva, R.P. Pediatric Respiratory Sound Classification Using a Dual Input Deep Learning Architecture. In Proceedings of the IEEE BioCAS Grand Challenge, Toronto, ON, Canada, 19–21 October 2023. [Google Scholar]
- Wu, Y.; Rocha, B.M.; Kaimakamis, E.; Cheimariotis, G.A.; Petmezas, G.; Chatzis, E.; Kilintzis, V.; Stefanopoulos, L.; Pessoa, D.; Marques, A.; et al. A Deep Learning Method for Predicting the COVID-19 ICU Patient Outcome Fusing X-rays, Respiratory Sounds, and ICU Parameters. Expert Syst. Appl. 2024, 235, 121089. [Google Scholar] [CrossRef]
- Azam, K.S.F.; Ryabchykov, O.; Bocklitz, T. A Review on Data Fusion of Multidimensional Medical and Biomedical Data. Molecules 2022, 27, 7448. [Google Scholar] [CrossRef]
- Murillo-Ortiz, B.; Rodríguez-Penin, A.; Hernández-Ramírez, A.; Rivera-Villanueva, T.; Moran-Gonzalez, A.E.; Martínez-Garza, S.; Suárez-García, D.; Pérez-Murguía, M.; Romero-Coripuna, R. Diagnóstico de cáncer de mama mediante mamografía por electroimpedancia computarizada MEIK. Rev. Mex. Mastología 2019, 9, 20–28. [Google Scholar]
- Zarafshani, A.; Bach, T.; Chatwin, C.R.; Tang, S.; Xiang, L.; Zheng, B. Conditioning Electrical Impedance Mammography System. Measurement 2018, 116, 38–48. [Google Scholar] [CrossRef]
- Daglar, G.; Senol, K.; Yakut, Z.; Yuksek, Y.; Tutuncu, T.; Tez, M.; Yesiltepe, C. Effectiveness of breast electrical impedance imaging for clinically suspicious breast lesions. Bratisl. Med. J. 2016, 117, 505–510. [Google Scholar] [CrossRef]
- Aibar, L.; Santalla, A.; López-Criado, M.S.; González–Pérez, I.; Calderón, M.; Gallo, J.; Fernández-Parra, J. Clasificación radiológica y manejo de las lesiones mamarias. Clínica Investig. Ginecol. Obstet. 2011, 38, 141–149. [Google Scholar] [CrossRef]
- Alexander Karpov, A.K.; Korotkova, M. An Electrical Impedance Mammographic Scheme—Norms and Pathology. In Mammography Techniques and Review; IntechOpen: London, UK, 2015. [Google Scholar] [CrossRef]
- Gonzalez, R.C.; Woods, R.E. Digital Image Processing; Pearson: Upper Saddle River, NJ, USA, 2008. [Google Scholar]
- Alvarado-Godínez, J.; Peregrina-Barreto, H.; Farías, D.I.H.; Ortiz, B.O.M. Automatic Breast Lesions Classification in Electrical Impedance Mammography. In Proceedings of the 2024 IEEE International Autumn Meeting on Power, Electronics and Computing (ROPEC 2024), Ixtapa, Mexico, 11–13 November 2024. [Google Scholar]
- Peli, E. Contrast in complex images. J. Opt. Soc. Am. A 1990, 7, 2032–2040. [Google Scholar] [CrossRef]
- Chang, Y.; Jung, C.; Ke, P.; Song, H.; Hwang, J. Automatic Contrast-Limited Adaptive Histogram Equalization with Dual Gamma Correction. IEEE Access 2018, 6, 11782–11792. [Google Scholar] [CrossRef]
- Burt, P.J.; Adelson, E.H. The Laplacian Pyramid as a Compact Image Code. IEEE Trans. Commun. 1983, 31, 532–540. [Google Scholar] [CrossRef]
- Yin, H. Tensor Sparse Representation for 3-D Medical Image Fusion Using Weighted Average Rule. IEEE Trans. Biomed. Eng. 2018, 65, 2622–2633. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Zhao, X.; Wang, L.; Zhang, Y.; Han, X.; Deveci, M.; Parmar, M. A review of convolutional neural networks in computer vision. Artif. Intell. Rev. 2024, 57, 99. [Google Scholar] [CrossRef]
- Papageorgiou, V.E.; Petmezas, G.; Dogoulis, P.; Cordy, M.; Maglaveras, N. Uncertainty CNNs: A path to enhanced medical image classification performance. Math. Biosci. Eng. 2025, 22, 528–553. [Google Scholar] [CrossRef]
- Papageorgiou, V.E.; Zegkos, T.; Efthimiadis, G.; Tsaklidis, G. Analysis of digitalized ECG signals based on artificial intelligence and spectral analysis methods specialized in ARVC. Int. J. Numer. Methods Biomed. Eng. 2022, 38, e3644. [Google Scholar] [CrossRef]
- Berkson, J. Application of the Logistic Function to Bio-Assay. J. Am. Stat. Assoc. 1944, 39, 357–365. [Google Scholar] [CrossRef]
- Segal, M.R. Machine Learning Benchmarks and Random Forest Regression; UCSF: Center for Bioinformatics and Molecular Biostatistics: San Francisco, CA, USA, 2004. [Google Scholar]
- Breiman, L. Bagging predictors. Mach. Learn. 1996, 24, 123–140. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the KDD ’16: 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, New York, NY, USA, 13–17 August 2016; pp. 785–794. [Google Scholar] [CrossRef]
- Georgakis, A.; Papageorgiou, V.E.; Gatziolis, D.; Stamatellos, G. Temporal-Like Bivariate Fay-Herriot Model: Leveraging Past Responses and Advanced Preprocessing for Enhanced Small Area Estimation of Growing Stock Volume. SN Oper. Res. Forum 2024, 5, 9. [Google Scholar] [CrossRef]
- Georgakis, A.; Papageorgiou, V.E.; Stamatellos, G. A new approach to small area estimation: Improving forest management unit estimates with advanced preprocessing in a multivariate Fay–Herriot model. Forestry 2024, 1–18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BI-RADS | EIM Interpretation | EIM Scale |
|---|---|---|
| 0 | Insufficient sample | No score |
| 1 | Undefined lesion | 0–1 |
| 2 | Benign tumors—routine mammography | 2–3 |
| 3 | Probably benign | 4 |
| 4 | Suspicious anomaly—biopsy recommended | 5–7 |
| 5 | High suspicion of malignancy—biopsy and treatment | 8–10 |
| Feature | Description |
|---|---|
| Number of patients | 340 (BR1 = 85, BR2 = 85, BR3 = 128, BR4 = 38, BR5 = 4) |
| EIM package | 7 images per breast |
| Number of images | 4760 ( pixels) |
| Age range | 25 to 70 years old |
| Study design | Clinical, epidemiological, observational, prospective, cross-sectional, and serial screening study |
| Device used | MEIK v.5.6 (SIM-technika, Russia, Yaroslavl) |
| Exploration depths | From the surface to the inner layers of the breast tissue |
| Physiological conditions considered | Pregnancy, breastfeeding, recent hormonal or surgical treatments, breast prostheses due to mastectomy or cosmetic surgery, etc. |
| Risk factors | Age of patient, body mass index, parity, age at menarche, age at menopause, hormonal therapy, family history of breast cancer, alcohol consumption, and smoking |
| Integration Methods | Fusion Methods | ||||||
|---|---|---|---|---|---|---|---|
| CV | CVCLAHE | CRMS | CLAHEF | Gaussian Pyramid | Weighted Avg. | Wavelet–PCA | |
| B1 |  |  |  |  |  |  |  |
| B2 |  |  |  |  |  |  |  |
| B3 |  |  |  |  |  |  |  |
| B4 |  |  |  |  |  |  |  |
| B5 |  |  |  |  |  |  |  |
 | |||||||
| Classifier | Method | Positive Predictions | Classifier Performance | ||
|---|---|---|---|---|---|
| Recall | Precision | Accuracy | F1–Score | ||
| Logistic Regression | CVCLAHE | ||||
| CV | |||||
| Random Forest | CVCLAHE | ||||
| CV | |||||
| Bagging | CVCLAHE | ||||
| CV | |||||
| XGBoost | CVCLAHE | ||||
| CV | |||||
| Classifier | Method | Positive Predictions | Classifier Performance | ||
|---|---|---|---|---|---|
| Recall | Precision | Accuracy | F1-Score | ||
| Logistic Regression | CLAHEF | ||||
| Gaussian pyramid | |||||
| Weighted Average | |||||
| Wavelet-PCA | |||||
| Random Forest | CLAHEF | ||||
| Gaussian pyramid | |||||
| Weighted Average | |||||
| Wavelet-PCA | |||||
| Bagging | CLAHEF | ||||
| Gaussian pyramid | |||||
| Weighted Average | |||||
| Wavelet-PCA | |||||
| XGBoost | CLAHEF | ||||
| Gaussian pyramid | |||||
| Weighted Average | |||||
| Wavelet-PCA | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarado-Godinez, J.; Peregrina-Barreto, H.; Hernández-Farías, D.I.; Murillo-Ortiz, B. Information Merging for Improving Automatic Classification of Electrical Impedance Mammography Images. Appl. Sci. 2025, 15, 7735. https://doi.org/10.3390/app15147735
Alvarado-Godinez J, Peregrina-Barreto H, Hernández-Farías DI, Murillo-Ortiz B. Information Merging for Improving Automatic Classification of Electrical Impedance Mammography Images. Applied Sciences. 2025; 15(14):7735. https://doi.org/10.3390/app15147735
Chicago/Turabian StyleAlvarado-Godinez, Jazmin, Hayde Peregrina-Barreto, Delia Irazú Hernández-Farías, and Blanca Murillo-Ortiz. 2025. "Information Merging for Improving Automatic Classification of Electrical Impedance Mammography Images" Applied Sciences 15, no. 14: 7735. https://doi.org/10.3390/app15147735
APA StyleAlvarado-Godinez, J., Peregrina-Barreto, H., Hernández-Farías, D. I., & Murillo-Ortiz, B. (2025). Information Merging for Improving Automatic Classification of Electrical Impedance Mammography Images. Applied Sciences, 15(14), 7735. https://doi.org/10.3390/app15147735