
Acute Effect of Passive Hyperthermia on Lactate Concentrations
 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Familiarisation
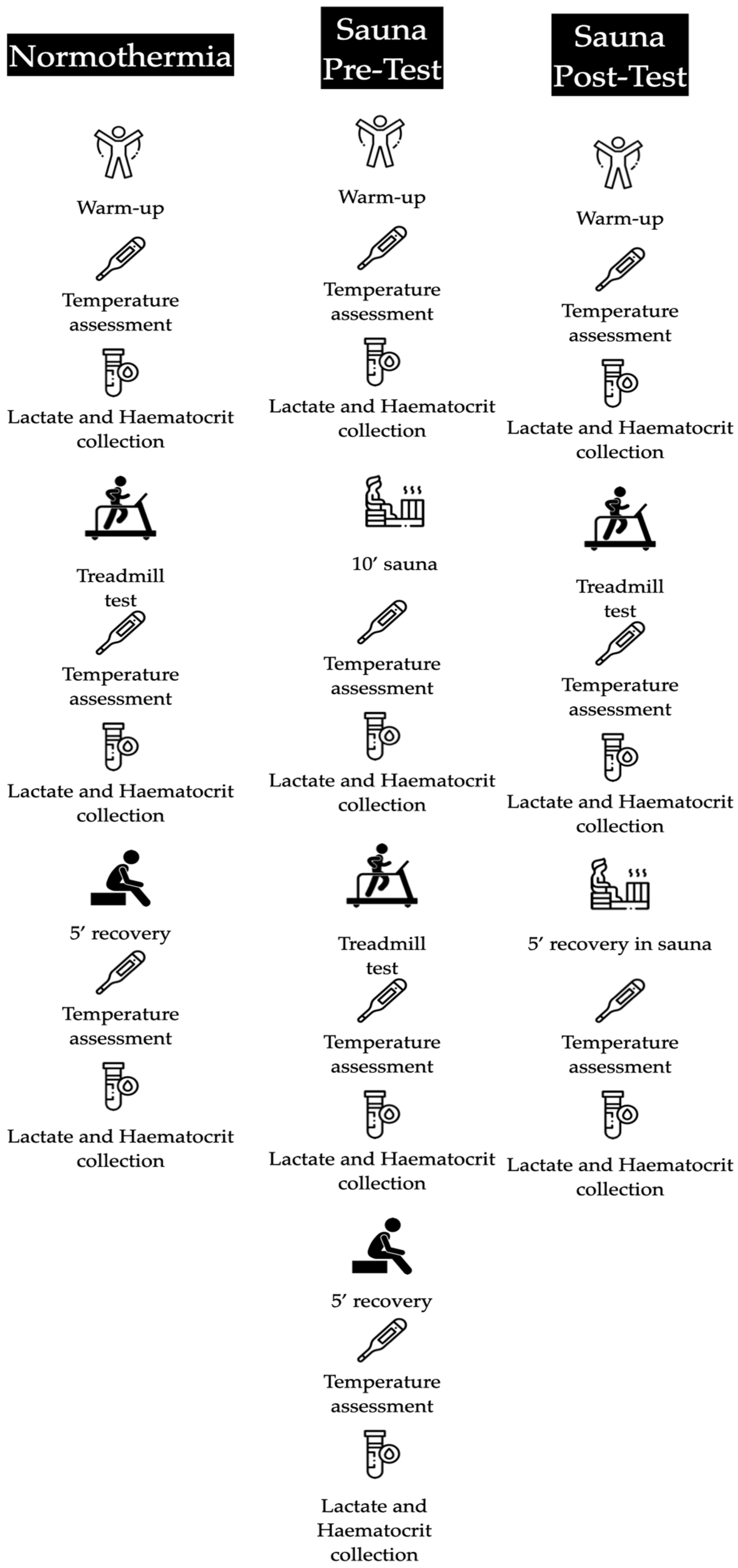
2.4. Experimental Protocol
2.5. Treadmill Test
2.6. Nutritional Assessment and Weekly Training
2.7. Anthropometric Study
2.8. Haematocrit and Lactate Assessment
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kenney, W.L.; Wilmore, J.; Costill, D. Physiology of Sport and Exercise, 6th ed.; Human Kinetics: Champaign, IL, USA, 2015; ISBN 1450477674. [Google Scholar]
- Febbraio, M.A.; Carey, M.F.; Snow, R.J.; Stathis, C.G.; Hargreaves, M. Influence of Elevated Muscle Temperature on Metabolism during Intense, Dynamic Exercise. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 1996, 271, R1251–R1255. [Google Scholar] [CrossRef] [PubMed]
- Toro-Román, V.; Prieto-González, I.; Siquier-Coll, J.; Bartolomé, I.; Grijota, F.J.; Maynar-Mariño, M. Effects of High Temperature Exposure on the Wingate Test Performance in Male University Students. Int. J. Environ. Res. Public Health 2023, 20, 4782. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K. The Anaerobic Threshold: Definition, Physiological Significance and Identification. Adv. Cardiol. 1986, 35, 1–23. [Google Scholar] [PubMed]
- Melkonian, E.A.; Schury, M.P. Biochemistry, Anaerobic Glycolysis; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Leverve, X.M.; Mustafa, I.; Péronnet, F. Pivotal Role of Lactate in Aerobic Energy Metabolism. In Yearbook of Intensive Care and Emergency Medicine 1998; Springer: Berlin/Heidelberg, Germany, 1998; pp. 588–596. [Google Scholar]
- Karlsson, J.; Bonde-Petersen, F.; Henriksson, J.; Knuttgen, H.G. Effects of Previous Exercise with Arms or Legs on Metabolism and Performance in Exhaustive Exercise. J. Appl. Physiol. 1975, 38, 763–767. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, J.D.; Reddan, W.G.; Layton, C.R.; Dempsey, J.A. Effects of Metabolic Hyperthermia on Performance during Heavy Prolonged Exercise. J. Appl. Physiol. 1974, 36, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Sekine, N.; Cirulli, V.; Regazzi, R.; Brown, L.J.; Gine, E.; Tamarit-Rodriguez, J.; Girotti, M.; Marie, S.; MacDonald, M.J.; Wollheim, C.B. Low Lactate Dehydrogenase and High Mitochondrial Glycerol Phosphate Dehydrogenase in Pancreatic Beta-Cells. Potential Role in Nutrient Sensing. J. Biol. Chem. 1994, 269, 4895–4902. [Google Scholar] [CrossRef]
- Folk, B.; Einbinder, M.; Weinstein, Y.; Epstein, S.; Kami, Y.; Yarom, Y.; Rotstein, A. Blood Lactate Concentration Following Exercise: Effects of Heat Exposure and of Active Recovery in Heat-Acclimatized Subjects. Int. J. Sports Med. 1995, 16, 7–12. [Google Scholar] [CrossRef]
- Maxwell, N.S.; Aitchison, T.C.; Nimmo, M.A. The Effect of Climatic Heat Stress on Intermittent Supramaximal Running Performance in Humans. Exp. Physiol. Transl. Integr. 1996, 81, 833–845. [Google Scholar] [CrossRef] [PubMed]
- Smolander, J.; Kolari, P.; Korhonen, O.; Ilmarinen, R. Aerobic and Anaerobic Responses to Incremental Exercise in a Thermoneutral and a Hot Dry Environment. Acta Physiol. Scand. 1986, 128, 15–21. [Google Scholar] [CrossRef]
- Oyono-Enguelle, S.; Heitz, A.; Marbach, J.; Ott, C.; Pape, A.; Freund, H. Heat Stress Does Not Modify Lactate Exchange and Removal Abilities during Recovery from Short Exercise. J. Appl. Physiol. 1993, 74, 1248–1255. [Google Scholar] [CrossRef]
- Falk, B.; Radom-Isaac, S.; Hoffmann, J.R.; Wang, Y.; Yarom, Y.; Magazanik, A.; Weinstein, Y. The Effect of Heat Exposure on Performance of and Recovery from High-Intensity, Intermittent Exercise. Int. J. Sports Med. 1998, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bartolomé, I.; Toro-Román, V.; Siquier-Coll, J.; Muñoz, D.; Robles-Gil, M.C.; Maynar-Mariño, M. Acute Effect of Exposure to Extreme Heat (100 ± 3 °C) on Lower Limb Maximal Resistance Strength. Int. J. Environ. Res. Public Health 2022, 19, 10934. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D. The Effect of Training on Aerobic and Anaerobic Metabolism during a Short Exhaustive Run. Med. Sci. Sports Exerc. 1969, 1, 65–69. [Google Scholar] [CrossRef]
- O’Loughlin, E.K.; Marashi, M.; Sabiston, C.M.; Lucibello, K.M.; Sylvestre, M.-P.; O’Loughlin, J.L. Predictors of Food and Physical Activity Tracking Among Young Adults. Health Educ. Behav. 2023, 50, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Esparza, F.; Alvero, J.R.; Aragonés, M.T.; Cabañas, M.D.; Canda, A.; Casajús, J.A.; Chamorro, M.; Galiano, D. Manual de Cineantropometría; GREC-FEMEDE: Pamplona, Spain, 1993. [Google Scholar]
- Yanchatuña Agualongo, M.N. Determinación de Electrolitos, Glucosa, Hematocrito Pre y Post Entrenamiento En La División Formativa Sub 12 y Sub 14 Del Club Deportivo Mushuc Runa S.C. y Su Relación Con El Tiempo de Actividad Física. Bachelor’s Thesis, Universidad Técnica de Ambato, Ambato, Ecuador, 2017. [Google Scholar]
- Garcia-Vega, O.; Ramos, M.; Mancera, E. Perfiles Hematológicos e Hidroelectrolíticos En Sujetos Sedentarios Durante Ejercicio de Resistencia: Efecto de La Hidratación. Rev. Med. Fac. Med. 2007, 15, 26–39. [Google Scholar]
- Van Beaumont, W. Evaluation of Hemoconcentration from Hematocrit Measurements. J. Appl. Physiol. 1972, 32, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, J. Warming up and Its Physiological Effects. Pharmacol. Physiol. 1978, 6, 31–39. [Google Scholar]
- Racinais, S.; Cocking, S.; Périard, J.D. Sports and Environmental Temperature: From Warming-up to Heating-Up. Temperature 2017, 4, 227–257. [Google Scholar] [CrossRef] [PubMed]
- Cotter, J.D.; Patterson, M.J.; Taylor, N.A.S. Sweat Distribution before and after Repeated Heat Exposure. Eur. J. Appl. Physiol. Occup. Physiol. 1997, 76, 181–186. [Google Scholar] [CrossRef]
- Buono, M.J.; Lee, N.V.L.; Miller, P.W. The Relationship between Exercise Intensity and the Sweat Lactate Excretion Rate. J. Physiol. Sci. 2010, 60, 103–107. [Google Scholar] [CrossRef]
- Weller, R.S.; Buono, M.J. The Effect of Heat Acclimation on the Sweat Lactate Concentration vs. Sweat Rate Relationship. J. Therm. Biol. 2022, 109, 103325. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, S.; Kosmidis, I.; Sougioultzis, M.; Kabasakalis, A.; Mougios, V. Diurnal Variation and Reliability of the Urine Lactate Concentration after Maximal Exercise. Chronobiol. Int. 2018, 35, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, S.; Karpouzi, C.; Tsalis, G.; Kabasakalis, A.; Papaioannou, K.G.; Mougios, V. Reliability of Urine Lactate as a Novel Biomarker of Lactate Production Capacity in Maximal Swimming. Biomarkers 2016, 21, 328–334. [Google Scholar] [CrossRef]
- Crandall, C.G.; Gonzalez-Alonso, J. Cardiovascular Function in the Heat-stressed Human. Acta Physiol. 2010, 199, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Marchant, E.D.; Nelson, W.B.; Hyldahl, R.D.; Gifford, J.R.; Hancock, C.R. Passive Heat Stress Induces Mitochondrial Adaptations in Skeletal Muscle. Int. J. Hyperth. 2023, 40, 2205066. [Google Scholar] [CrossRef]
- McCutcheon, L.J.; Geor, R.J.; Hinchcliff, K.W. Effects of Prior Exercise on Muscle Metabolism during Sprint Exercise in Horses. J. Appl. Physiol. 1999, 87, 1914–1922. [Google Scholar] [CrossRef]
- Rowell, L.B.; Brengelmann, G.L.; Blackmon, J.R.; Twiss, R.D.; Kusumi, F. Splanchnic Blood Flow and Metabolism in Heat-Stressed Man. J. Appl. Physiol. 1968, 24, 475–484. [Google Scholar] [CrossRef]
- Martin, D.E. The Effect of Heat Stress on Excess Post Exercise Oxygen Consumption; Microform Publications, University of Oregon: Eugene, OR, USA, 1994. [Google Scholar]
- Nybo, L.; Nielsen, B. Hyperthermia and Central Fatigue during Prolonged Exercise in Humans. J. Appl. Physiol. 2001, 91, 1055–1060. [Google Scholar] [CrossRef]
- Périard, J.D.; Cramer, M.N.; Chapman, P.G.; Caillaud, C.; Thompson, M.W. Neuromuscular Function Following Prolonged Intense Self-Paced Exercise in Hot Climatic Conditions. Eur. J. Appl. Physiol. 2011, 111, 1561–1569. [Google Scholar] [CrossRef]
- Racinais, S.; Girard, O. Neuromuscular Failure Is Unlikely to Explain the Early Exercise Cessation in Hot Ambient Conditions. Psychophysiology 2012, 49, 853–865. [Google Scholar] [CrossRef]
- Chalmers, S.; Esterman, A.; Eston, R.; Bowering, K.J.; Norton, K. Short-Term Heat Acclimation Training Improves Physical Performance: A Systematic Review, and Exploration of Physiological Adaptations and Application for Team Sports. Sports Med. 2014, 44, 971–988. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Carter, R.; Haymes, E.M.; Sawka, M.N. No Effect of Moderate Hypohydration or Hyperthermia on Anaerobic Exercise Performance. Med. Sci. Sports Exerc. 2006, 38, 1093–1097. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normothermia | Hyperthermia Pre | Hyperthermia Post | |
|---|---|---|---|
| Height (m) | 1.76 ± 0.08 | 1.76 ± 0.08 | 1.76 ± 0.08 |
| Weight (kg) | 72.13 ± 9.03 | 72.63 ± 9.30 | 73.00 ± 9.98 |
| BMI | 23.14 ± 2.17 | 23.38 ± 2.19 | 23.47 ± 2.18 |
| Weekly training (h) | 5.38 ± 4.57 | 4.88 ± 4.70 | 4.88 ± 4.29 |
| Fat (%) | 10.06 ± 2.19 | 10.48 ± 1.81 | 10.34 ± 1.93 |
| Fat (kg) | 7.39 ± 2.48 | 7.74 ± 2.25 | 7.69 ± 2.29 |
| Muscle (%) | 50.43 ± 1.92 | 50.03 ± 2.02 | 50.23 ± 1.80 |
| Muscle (kg) | 36.19 ± 3.61 | 36.31 ± 4.07 | 36.59 ± 3.91 |
| Σ 6 Fold (mm) | 66.38 ± 22.24 | 70.48 ± 18.71 | 69.04 ± 19.86 |
| Normothermia | Hyperthermia Pre | Hyperthermia Post | |
|---|---|---|---|
| Carbohydrates (g) | 272.38 ± 180.52 | 215.40 ± 167.54 | 206.00 ± 33.38 |
| Protein (g) | 99.84 ± 19.76 | 97.70 ± 45.03 | 112.25 ± 39.01 |
| Fat (g) | 76.88 ± 36.28 | 66.56 ± 14.35 | 65.98 ± 14.94 |
| Total daily intake (kcal) | 2585.51 ± 292.45 | 2201.29 ± 154.00 | 2395.97 ± 159.78 |
| Normothermia | Sauna Pre | Sauna Post | ||
|---|---|---|---|---|
| Basal (°C) | Internal | 35.88 ± 2.10 | 36.13 ± 0.52 | 36.46 ± 1.03 |
| External | 36.01 ± 1.89 | 36.56 ± 0.46 | 36.08 ± 0.94 | |
| Pre-test/post-sauna (°C) | Internal | - | - | 37.34 ± 0.77 |
| External | - | - | 37.56 ± 0.35 | |
| Post-test (°C) | Internal | 37.8 ± 0.3 | 37.9 ± 0.4 | 37.5 ± 0.25 |
| External | 37.8 ± 0.4 | 37.6 ± 0.56 | 37.9 ± 0.69 | |
| 5′ Recovery (°C) | Internal | 36.88 ± 0.47 | 37.3 ± 0.39 | 37.49 ± 0.73 |
| External | 37.6 ± 0.52 | 36.84 ± 0.65 | 37.88 ± 0.59 | |
| Test performance (s) | 61.38 ± 10.85 | 64.50 ± 13.83 | 66.88 ± 16.34 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siquier-Coll, J.; Flores, J.M.; Grijota, F.J.; Bartolomé, I.; Maynar-Mariño, M.; Toro-Román, V. Acute Effect of Passive Hyperthermia on Lactate Concentrations. Appl. Sci. 2024, 14, 2895. https://doi.org/10.3390/app14072895
Siquier-Coll J, Flores JM, Grijota FJ, Bartolomé I, Maynar-Mariño M, Toro-Román V. Acute Effect of Passive Hyperthermia on Lactate Concentrations. Applied Sciences. 2024; 14(7):2895. https://doi.org/10.3390/app14072895
Chicago/Turabian StyleSiquier-Coll, Jesús, Juan Manuel Flores, Francisco Javier Grijota, Ignacio Bartolomé, Marcos Maynar-Mariño, and Víctor Toro-Román. 2024. "Acute Effect of Passive Hyperthermia on Lactate Concentrations" Applied Sciences 14, no. 7: 2895. https://doi.org/10.3390/app14072895
APA StyleSiquier-Coll, J., Flores, J. M., Grijota, F. J., Bartolomé, I., Maynar-Mariño, M., & Toro-Román, V. (2024). Acute Effect of Passive Hyperthermia on Lactate Concentrations. Applied Sciences, 14(7), 2895. https://doi.org/10.3390/app14072895