Abstract
Falls at height are among the major causes of fatal accidents at work, especially in the construction sector. Maintaining balance while performing a tool with both hands generates physical efforts and mental loading that needs to be managed for workers’ safety and health. The purpose of the study is to compare perceived (dis)comfort (overall and localized), the ergonomic risk, and the perceived effort through the acquired postures that subjects assumed during the execution of simple and common tasks both on a ladder and on the ground. 26 subjects were asked to perform four tasks in both conditions: top screwing, frontal screwing, object picking from the bottom forward, and object picking from the bottom sideways. Subjective and objective data were gathered for assessing subjective experience (discomfort and effort, perceived) and ergonomic risk. Results highlighted few ergonomic risk differences among “on ladder” and “on ground” tasks, while subjective data reveal significant differences in different scenarios. Furthermore, the knees and neck areas are the most critical ones.
1. Introduction
Work at height is considered to be all those work activities carried out at such a height that it exposes the worker to the risk of falling and personal injury. In cases of low risks and short-duration tasks, fall protection systems are not required, and a ladder can be used to reach the heights. Moreover, in cases where it is impossible to change the workplace layout to use platforms or other safety features, a portable ladder has to be used. To establish whether an activity is carried out safely or not, the level of risk must be considered. Ladders should only be used in situations where they can be used safely, e.g., where the ladder will be level and stable or where, if possible, the ladder can be fixed.
Much of the literature relating to ladders has emphasized the prevention of injuries associated with working on ladders [1,2,3,4,5,6,7,8,9,10]. The main causes of these falls are foot slipping [11,12,13] on a ladder rung; the usage of broken, collapsed, or folded ladders [1,9,14,15,16]; loss of balance and/or ladder movements during the usage, such as the sliding of the base. About the recovery of balance following slipping, different positions of the feet and hands were examined [11]. In [11,17,18,19] it is shown how grasping the rungs of the ladder rather than the rails provides a better grip, thus reducing the likelihood of slipping and preventing a fall.
Another investigated aspect is the angle of inclination of non-self-supporting ladders [3,6,20,21] and several methods to best set it. Climbing and using ladders is a common generic task in many occupations, professional and not. In the context of the use of non-professional ladders, the incidence of significant injuries is increasing. In the literature, different recommendations have been made to reduce the probability of falling from a ladder such as improving ladder design, using aerial lifts or scaffolds, training the user on how to use the ladder safely, training the user in the selection and inspection phases, and incentivize formal training programs and regulations governing the use of ladders [1,6,9,15,22,23].
Little scientific research has been carried out to ergonomically evaluate the ascent, the descent, and the handling of ladders in working activities [3,24]. The most investigated factors regard heavy loads and manipulation of objects while working at heights; incongruous posture, and repetitive arm use; loading/unloading ladders from vehicles; and placing ladders on the shoulder to move them. Some studies have been conducted, especially in the agricultural sector, and during apple harvesting operations [25,26,27,28,29]. In [25,26], two different apple harvesting methods were compared: a conventional ladder and a newly developed mobile platform. In [28,29], the analysis carried out using the RULA [30] method is aimed at identifying uncomfortable postures/activities that occurred during apple harvesting. In [24] the aim was to compare mechanical load, safety, energetic workload, perceived exertion, and perceived discomfort, among window cleaners that used some extension ladders with 30 and 35 cm rung separation. The biomechanical aspects relating to the daily use of the ladder have received very little attention, in particular, on the musculoskeletal load required and the postural discomfort perceived during its usage. Subjective and/or objective data can be useful to evaluate postural (dis)comfort regarding a generic task. To detect the subjective data (pain, discomfort, and level of fatigue), surveys, questionnaires, and self-reports are used. The most used are the BPD: Body Part (Dis)comfort and the LPD: Localized Postural (Dis)comfort [31,32,33]. To detect the objective data (ergonomically valid posture and postural comfort), sensors, methods, and tools are used [34,35]. The software CAMan [30,36,37,38,39,40] considers the angles assumed by the upper limbs during the execution of a task and gives an output of a postural comfort index. The tool, realized by the University of Salerno, gives the comfort index on a 10-point scale where 10 is the maximum.
The reason for this study was born in this context. The aim of this study was to examine joint loading along with ratings of perceived discomfort and perceived strain during a simple work task with and without the use of a ladder. The research questions are: How much does performing a simple task on a ladder instead of on the ground affect perceived discomfort? Is the difference in perceived discomfort related to biomechanical overload (evaluating it with the RULA method)?
2. Material and Methods
2.1. Purpose
In cases of work at height, working on scaffolding allows one to experience a perceived stability when performing the operation that is almost the same as working from the ground, while if the operation must be performed on a ladder, balance, and freedom of movement are compromised, which is results in strong perceived discomfort and reduced user safety; unfortunately, sometimes is not possible (or not convenient) to use fixed systems, such as scaffolding, thus it is necessary to use a ladder.
The aim of this study was to compare simple tasks, performed on the ground and on a ladder, in terms of subjective experience and objective evaluation. For the subjective and objective comfort data, questionnaires and CAMan were used, respectively. For the ergonomics evaluation, RULA analysis was performed.
2.2. Pilot Tests to Identify the Critical Tasks
First, brainstorming among the authors (experts) and three people who usually carry out operations on a ladder (furniture, curtain, and air conditioning assembly workers) was conducted to identify the most frequent and critical actions in terms of ergonomics and discomfort. Given the heterogeneity of the group, experts, and non-experts, a first list of operations, both domestic and non-domestic, which require a ladder to be carried out has been drawn up. Some examples were window washing, painting, cleaning the internal roof of the house room, screwing the plasterboard, changing a light bulb, and picking up and moving objects. Then, starting from these activities, a list of the movements to be carried out for each of them was drawn up. For example, to clean windows it needs to make repetitive vertical movements with just one arm; to screw in a light bulb, make a rotating movement with one hand; to clean a top it needs to make repetitive horizontal movements with just one arm. After the identification of the movements, a pre-experimental phase was carried out on a sample of 15 users. Each participant was asked to perform each movement twice, once standing and once using a ladder. Informed consent was obtained. The sample consisted of 8 men and 7 women, aged between 24 and 32. The height varied from 165 cm (female participant) to 180 cm (male participant), no specific inclusion Criteria have been applied, but the subject does not have disabilities and has to be able to work on a ladder (no height-related dizziness has to be recorded in the subject history). The tests were carried out randomly and at the end of each test, the participant had to assign a score of perceived discomfort on a scale from 1 to 10. The tests were necessary to be able to select the movements that reported a significant difference if performed from the ground or on the ladder. The authors chose 4 operations: the operations that, in the re-experimental phase, presented a difference of at least two points between the two setups for 80% of the sample.
The identified tasks were:
- (1)
- Top screwing: representative of all those operations that require the arms to be raised, with possibly the handling of a tool needed to carry out the operation, and a force exertion in the vertical direction. This group includes operations such as: screwing at the top of a ceiling, drilling at the top, painting the ceiling, changing a light bulb, etc. (Figure 1a).
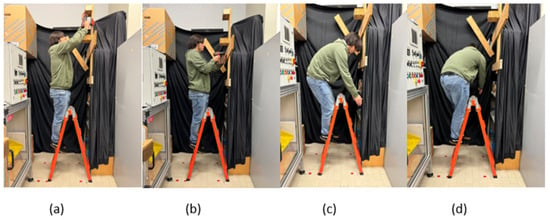 Figure 1. Critical tasks: (a) Top screwing; (b) Frontal screwing; (c) Object picking from the bottom forward; (d) Object picking from the bottom sideways.
Figure 1. Critical tasks: (a) Top screwing; (b) Frontal screwing; (c) Object picking from the bottom forward; (d) Object picking from the bottom sideways. - (2)
- Frontal screwing: representative of all those operations that require the arms to be maintained horizontally to carry out the operation, with possibly the handling of a tool needed to carry out the operation far from the body’s center of gravity and force-exertion in the horizontal direction. This group includes operations such as frontal screwing, frontal drilling, wall painting, fixing of a frame, etc. (Figure 1b).
- (3)
- Object picking from bottom forward: representative of all those operations that require a forward bend with a vertical applied load, for example, to pose or take an object positioned in front of the ladder, in a lowered position (Figure 1c).
- (4)
- Object picking from the bottom sideways: representative of all those operations that require a downward bending and a twist of the torso with a vertical applied load, for example, to pose or take an object positioned laterally on the ladder, in a lowered position (Figure 1d).
2.3. Participants
A statistical sample of twenty-six healthy young people (22 males and 4 females), all volunteers, participated in the experiment. None had a history of musculoskeletal diseases. The sample ranges from the 20th percentile female to the 95th percentile male, ensuring a good description of the population. The main characteristics of the subjects are summarized in Table 1. The subjects were informed of the nature of the tests and their written consent, in accordance with ethical standards of the University of Salerno, was obtained.

Table 1.
Demographic data of the participants.
2.4. Experimental Setup
For the experimental phase, a setup was prepared to reproduce the four selected tasks (both from the ground and on the ladder. Three video cameras (Nikon D3300, Tokyo, Japan) were positioned on the right side (Figure 2a), behind (Figure 2b), and above (Figure 2c), in order to acquire the postures assumed by each subject for each task.
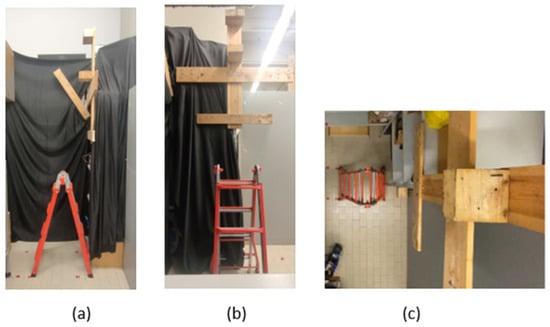
Figure 2.
Camera positions: (a) Lateral; (b) Behind; (c) Above.
A wooden structure on which the drilling operations were carried out at the top and front was built, and the holder surfaces at a fixed height for the object-picking operations were prepared.
Particularly, the experimental setup included:
- (1)
- Top screwing:
- -
- Ladder leaning against the wall
- -
- Drilling height is equal to 210 cm, measured from the plane on which the user placed his feet (the floor and the second step of the telescopic ladder in the case of screwing on a ladder)
- -
- Drilling is to be made about 7 cm from the wall
- (2)
- Frontal screwing:
- -
- Ladder leaning against the wall
- -
- Height at which the drill is equal to 153 cm, measured from the plane on which the user placed his feet (the floor and the second step of the telescopic ladder in the case of screwing on a ladder)
- (3)
- Object picking from bottom forward:
- -
- Object height to be picked/deposited equal to 61 cm, measured from the plane on which the user placed his feet (the floor and the second step of the telescopic ladder in the case of screwing on a ladder)
- -
- The front distance of the object to be picked up/deposited is equal to 65 cm
- (4)
- Object picking from the bottom sideways:
- -
- Object height to be picked up/deposited equal to 61 cm, measured from the plane on which the user placed his feet (the floor and the second step of the telescopic ladder in the case of screwing on a ladder)
- -
- The lateral distance of the object to be picked up/deposited is equal to 70 cm.
All distances reproduced in the experimental setup were initially tested in a simulation environment DELMIA® (V5R16, Dassault Systèmes, Vélizy-Villacoublay, France). The experimental setup was created in a virtual environment and subsequently tested with three mannikins belonging to the 5th, 50th, and 95th percentile. The chosen solution forced the three mannequins to assume different postures but ensured the absence of reachability problems.
2.5. Test Procedure
Before starting the tests, personal data were recorded for each participant. Each subject was then associated with an increasing number from one to 26 to be inserted in each questionnaire to be completed. The personal information requested were age, gender, height, weight, dominant arm (right-handed or left-handed), and frequency usage of a ladder to carry out general tasks. For each participant arm length and foot-to-shoulder distance were acquired.
Subsequently, each participant performed the 8 activities.
- -
- Frontal screwing on the ladder.
- -
- Frontal screwing from the ground.
- -
- Top screwing on the ladder.
- -
- Top screwing from the ground.
- -
- Sideways object picking on the ladder.
- -
- Sideways object picking from the ground.
- -
- Frontal object picking on the ladder.
- -
- Frontal object picking from the ground.
Each activity included an initial explanation from one of the supervisors and the compiling of the questionnaire, specific to the task, immediately at the end of each of them.
The testing order was planned for each participant adopting the Latin Square Method [41] to randomize the order while keeping the experiments’ repeatability. The task order was chosen randomly in order to avoid any task-order effect. After every 2 activities, the participants were asked to rest for 5 min to prevent tiredness from influencing the performance of the activities and, therefore, the answers to the questionnaire.
2.6. Questionnaire
All twenty-six participants in the experiment promptly completed an online survey using the Google Forms platform. The questionnaire aimed to evaluate the discomfort (overall and localized) perceived during the task execution, the effort perceived, and the hand-wrist posture. This last was considered only for the screwing tasks. The perceived discomfort was evaluated on a 10-point scale (1 minimum discomfort, 10 maximum discomfort). The Localized Postural Discomfort regarded 17 body parts [31]. A body diagram similar to [42] was used to define localized ratings (Figure 3). The effort perceived was evaluated through the Borg CR10 scale [39]. The hand-wrist position was evaluated on a 5-point Likert scale [32] (very good, good, neutral, harmful, very harmful).
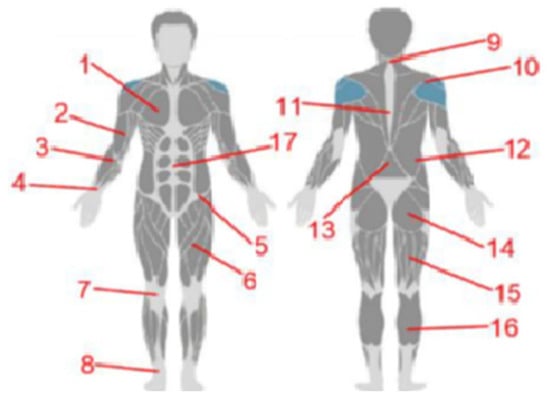
Figure 3.
Localized Postural Discomfort Assessment. (1) chest; (2) arm (left and right); (3) forearm (left and right); (4) wrist (left and right); (5) pelvis; (6) thigh (left and right); (7) knee (left and right); (8) ankle (left and right); (9) neck; (10) shoulder (left and right); (11) back (dorsal area); (12) hip (left and right); (13) back (lumbar area); (14) buttock; (15) quadricep (left and right); (16) calf (left and right); (17) abdomen.
3. Postural Data Acquisition
The photos for each participant and each task were processed using Kenova® software version 0.9.5-x64 (Figure 4). Kinovea® is a free software application for the analysis, comparison, and evaluation of movement. The limb movements acquired were:
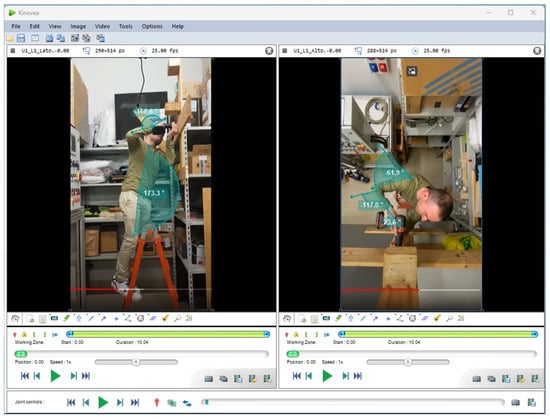
Figure 4.
Example of Kinovea® angle measurement.
- For the neck: frontal flexion, rotation, and lateral flexion.
- For the shoulder: frontal flexion, abduction/adduction.
- For the elbow: flexion/extension, pronation/supination.
- For the wrist: flexion/extension, radio/ulnar deviation.
The reference position for the detection and measurement of joint angles was the geometric-zero position. This position is defined as the one that allows the maximum state of comfort among the values in the “Comfort Range of Motion” (CROM) [38].
The aforementioned data were used to calculate RULA and CAMan indices.
RULA method was used to investigate the potential upper limb disorders, for right and left sides.
CAMan software was used to calculate the comfort index of the neck, shoulder, elbow, and wrist. Finally, the comfort index for the right, left side, and overall ones (Figure 5).
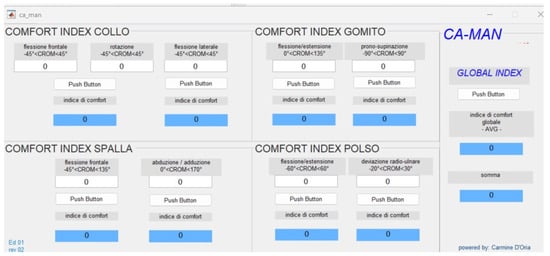
Figure 5.
CAMan Software Interface. Comfort index for each body part and the whole body. Based on postural angles.
4. Result and Discussion
Wilcoxon Signed Rank test has been performed to calculate whether there were significant differences between data, particularly between the data collected among the four tasks and for the same task but in the two configurations: on the ground and the ladder.
24 out of 26 subjects were right-handed and only 2 were left-handed. Given the limited number of left-handed subjects, it was decided not to conduct the analyses separately as the results obtained would not have been statistically significant. Correlations and the strength of the relationship between the variables, particularly between the subjective data (perceived (dis)comfort, from questionnaires and CAMan) and objective ones (RULA) were calculated with IBM® (Armonk, NY, USA) SPSS® Statistics version 24. Spearman index was computed since data was not normally distributed.
The data analysis had two specific purposes:
The first target was to understand, for each task, if there was a significant difference between the task carried out from the ground and the ladder. This analysis was carried out both in terms of RULA score, in terms of discomfort (questionnaire) rating, and in terms of comfort (CAMan) rating. Since the operations involved an asymmetrical use of the body, the right and left sides were considered separately.
The second target was to understand, for each task, which parts of the body were most in discomfort and whether there were correlations between the data acquired from the questionnaire and the results of the RULA and CAMan analysis.
- -
- Frontal screwing
The RULA and CAMan analysis shows no significant differences, neither between the right and left side of the body nor between the tasks performed from the ground and on a ladder (score = 3–4, further investigations are needed) (Table 2). CAMan results show the lowest values for the wrist (very low comfort).
Table 2.
Frontal screwing Ground-Ladder differences among absolute values.
Otherwise, the perceived discomfort is significantly higher when the task is carried out on the ladder. The reason lies in the discomfort perceived in the knee. RULA and CAMan do not consider the lower limbs and do not show significant differences between ground and ladder tasks. However, a significant difference emerges from the questionnaire in terms of global comfort. This confirms that the discriminating factor is the knees, assessed only in the questionnaire. Furthermore, the questionnaires show a higher average knee discomfort value for ladder work.
Correlation analysis confirms this result. For the ladder operation, knee discomfort has a positive correlation with the overall discomfort (and a negative correlation with to participant height (Table 3). The difference in perceived discomfort between the ground and on the ladder, therefore, is due to the forced contact between the knees and the steps in order to facilitate the balance of the body during the execution of the task. For height, from the analysis of the videos it was noted that the taller the subject, the lower the area/time of contact between knees and parts of the ladder (steps). Furthermore, the cross-analysis shows strong negative correlations between the CAMan results and the questionnaire. As perceived discomfort increases (questionnaire), postural comfort decreases (CAMan). This result shows that the participants answered consistently to the questionnaire.
Table 3.
Frontal screwing Spearman coefficients.
- -
- Top screwing
Unlike frontal screwing, screwing from above is more critical (higher values for both RULA®, perceived discomfort). This is due to a posture that involves greater extension of the arms, the inability to lean against the wall to improve balance, and greater flexion of the neck. CAMan shows the lowest values for the neck and arms for both tasks, performed on a ladder and from the ground. The arms and neck are the most critical parts body. However, there are no significant differences between the right side and the left side. Furthermore, the exertion of the force is in the vertical direction, adding the gravitational effects to the exerted force. The RULA analysis shows a significant difference between ground and ladder only for the right arm, despite assuming high scores in both cases (score = 5–6. Investigation and changes required soon). The knee is, once again, the most uncomfortable part with significantly higher values in the task carried out on a scale. The perceived effort is greater for the operation carried out on a ladder (Table 4). From the correlation analysis, effort is positively correlated with all right limbs. In this operation, therefore, the asymmetry of posture and activity is accentuated. Even for the top screwing tasks, such as the frontal screwing, there is a positive correlation between knee discomfort and global discomfort and a negative correlation between knee discomfort and the height of the subjects. Also, the arm length had a negative correlation with the local discomfort on the right forearm (Table 5). The reason can be found in being higher and having a longer arm makes it easier to reach the screwing height without stretching. Results show strong correlations between CAMan and the questionnaire, particularly, as the global discomfort assessed through the questionnaire increases, and the arms comfort assessed in the CAMan decreases.
Table 4.
Top screwing Ground Ladder difference.
Table 5.
Top screwing Spearman coefficients.
- -
- Sideways object picking
The RULA analysis shows no differences, neither between the right and left side of the body nor between the tasks performed from the ground and on a ladder (score = 5–6. Investigation and changes required soon). The perceived discomfort, instead, is higher for the task carried out on the ladder (Table 6). Discomfort is strongly correlated to the upper limbs (arm, forearm), knees, and back discomfort. The correlation analysis, for this task, highlights that leg discomfort is a crucial element. As the perceived discomfort in the leg increases, the general discomfort increases and, at the same time, the perceived effort, during the execution of the task. CAMan, instead, shows significant differences between the right and left sides, in particular, the right side has a lower comfort score, due to a greater effort to reach the object. The cross-analysis shows strong correlations between CAMan and the questionnaire. As perceived discomfort increases (questionnaire), postural comfort decreases (CAMan) (Table 7).
Table 6.
Sideways object picking Ground-Ladder difference.
Table 7.
Sideways object picking Spearman coefficients.
- -
- Frontal object picking
The RULA and CAMan analysis show no differences, neither between the right and left side of the body nor between the tasks performed from the ground and on a ladder (score = 5–6. Investigation and changes required soon). The perceived discomfort, instead, is higher for the task carried out on the ladder (Table 8). Since the difference between the ground and ladder can only be seen from the questionnaires that consider the lower limbs, then it can be concluded that the (dis)comfort depends exclusively on the knee (Table 8). The frontal object-picking task presents the lowest level of discomfort compared to the other ones.
Table 8.
Frontal object picking Ground-Ladder difference.
Spearman indices show two important correlations (Table 9). Neck discomfort is strongly correlated with overall discomfort and perceived effort. This demonstrates how the neck is the most critical body part for this operation.
Table 9.
Frontal object picking Spearman coefficients.
5. Limitations
This work shows comparative results, in terms of discomfort perceived, effort needed, and ergonomics risk, regarding the execution of simple and common tasks both on a ladder and on the ground. Some limitations need to be acknowledged:
26 participants in the test cannot be considered sufficient to carry out an in-depth study of the issues, even if the sample is statistically representative. Furthermore, the sample was composed of only young people, and a group of only 4 women, out of a sample of 26, is considered a limiting factor.
No EMG acquisition was performed to provide objective information measures of a person’s behavior and effort. The test setup, the choice of activities to simulate, and the procedure were found to be adequate to be able to acquire both subjective and subjective data. However, the setup was the same for the entire sample without taking into account the different anthropometry among the participants and the difference in terms of force and exertion that each subject had to need to accomplish a task.
In the ladder-knee contact, which has been discovered as the most impacting factor on perceived discomfort, no physical parameters, such as contact pressure, contact area, and contact time, have been investigated. This can be an improvement to do in future experiments.
6. Conclusions
When it is necessary to carry out work at height and it is not possible (or not convenient) to use fixed systems such as scaffolding, the use of a ladder is necessary, carrying out a task, even a simple one, on a ladder compromises balance and freedom of movement, resulting in strong perceived discomfort and reduced safety for the user.
The aim of this study was to compare simple tasks, performed on the ground and a ladder, in subjective and objective terms. For the subjective data, questionnaires were used; for the objective data, the RULA and CAMan analysis were carried out.
The research questions are: how much does perceived discomfort affect performing a simple task on a ladder instead of on the ground? Is the difference in perceived discomfort linked to biomechanical overload?
Summarizing, the RULA analysis does not highlight significant differences, neither between the right and left side of the body nor between the activities carried out from the ground and on a ladder (with the exception of the frontal screwing in which there is a significant difference, for the right arm, between the ground and the ladder). The RULA values for all activities, ground, and ladder, are always high, therefore the activities selected are significant for the analysis. The activities are compromising in terms of discomfort and biomechanical overload. CAMan confirms the results of the questionnaire. The cross-analysis shows strong negative correlations between the CAMan results and the questionnaire. The areas of the body that obtain the highest results in terms of perceived discomfort (questionnaires) are the same ones that are most compromised from a postural comfort point of view (CAMan). From the questionnaires, however, it emerges that, for all operations, there is a significant difference between the activity carried out on the ladder and the same activity carried out from the ground. Furthermore, the perceived discomfort is always less when the operation is carried out from the ground.
As for localized discomfort, the knee is the most critical body part. The difference in knee discomfort between ladder and ground is always significant; statistical analyses show correlations between knee discomfort and perceived discomfort and effort: as perceived knee discomfort increased, the perception of global discomfort and perceived effort increased. Carrying out the operation on the ladder creates weight imbalance and therefore balance problems. From the videos, it appears that the subjects, to maintain balance, rest their knee on one of the steps of the ladder and this causes localized pain. The results also show a correlation between knee discomfort and participants’ height: to increase the participants’ height the discomfort knee perceived decreases. Direct observation showed that as the height of the participants increased, contact between knees and ladder steps was reduced until it was lost completely. Thus, the absence of pressure in the knee on the step caused less discomfort to the subjects.
In the frontal object picking, Spearman indices show two important correlations. Neck discomfort is strongly related to general discomfort and perceived exertion. This shows how the neck is the most critical part of the body for this operation. For all tasks, the perceived effort is greater for the operation carried out on a ladder. This result can be found using the CAMan indices. The neck takes on low postural comfort values.
The findings would have a significant impact on ladder design. The ladder has not undergone major evolutions over time and remains a simple tool for reaching points that are difficult to reach but do not require specific platforms and scaffolding. However, the risks deriving from its use should not be underestimated, especially when performing tasks involving both arms. Not being able to use arms, because engaged in an activity, the knees contact on the ladder plays a fundamental role in maintaining balance and stability. The study has in fact demonstrated that the knees are affected, more than other parts of the body, by the discomfort perceived during the execution of the task. It would therefore be necessary to provide for changes from an ergonomic perspective intervening on the distance of the rungs. The distance between the rungs is a topic addressed in the literature to reduce the risk of falling, the speed of climbing, and the reduction of fatigue [19]. The results of this study show how it is necessary to intervene in the distance of the rungs, to reduce, at the same time, discomfort, and improve balance and performance in all those commonly carried out activities that involve the use of both arms. The distance of the rungs should be modified depending on the height of the subjects to guarantee solid contact between the knees and the rungs.
Author Contributions
Conceptualization, R.C. and A.N.; Methodology, R.C. and A.N.; Validation, A.N.; Formal analysis, A.A., M.C., L.D., V.F. and A.L.; Data curation, R.C., A.A., M.C., L.D., V.F. and A.L.; Writing—original draft, A.A., M.C., L.D., V.F. and A.L.; Writing—review & editing, R.C.; Supervision, R.C. and A.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study because the study involved, in very simple activities, 26 volunteer subjects that were asked to perform some simple tasks. For this kind of involvement, the Ethical Board of University of Salerno (art. 8 and art. 16 of Ethical Code—https://web.unisa.it/uploads/rescue/41/76/2017-10-25---DR-codice-etico.pdf, accessed on 6 March 2024) requires the respect of GDPR—Rule 2016-679 of UE in Personal data treatment and of DLGS 81/08, Italian Law, about safety on workplace. Both were respected: Personal Data were managed after the acquisition of a signed informed consent that were stored in the Department (Lab) repository, in respect of GDPR, while “Safety on workplace” regulation was controlled by the supervision of Lab’s Safety Manager, Prof. Nicola Cappetti.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shepherd, G.W.; Kahler, R.J.; Cross, J. Ergonomic design interventions—A case study involving portable ladders. Ergonomics 2006, 49, 221–234. [Google Scholar] [CrossRef]
- Jüptner, H. Safety on ladders: An ergonomic design approach. Appl. Ergon. 1976, 7, 221–223. [Google Scholar] [CrossRef]
- Bloswick, D.S.; Chaffin, D.B. An ergonomic analysis of the ladder climbing activity. Int. J. Ind. Ergon. 1990, 6, 17–27. [Google Scholar] [CrossRef]
- Dewar, M.E. Body Movements in Climbing a Ladder. Ergonomics 1977, 20, 67–86. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, B.F. Occupational hazards in window cleaning. BMJ 1975, 3, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Young, S.L.; Wogalter, M.S. On improving set-up angle accuracy for extension ladders. In Proceedings of the XIVth Triennial Congress of the International Ergonomics Association and the 44th Annual Meeting of the Human Factors and Ergonomics Society: Ergonomics for the New Millennium, San Diego, CA, USA, 29 July–4 August 2000; pp. 111–114. [Google Scholar]
- National Safety Council Injury. National Safety Council Injury Facts 2. Injury Fact; National Safety Council: Chicago, IL, USA, 2013. [Google Scholar]
- Rockett, I.R.H.; Regier, M.D.; Kapusta, N.D.; Coben, J.H.; Miller, T.R.; Hanzlick, R.L.; Todd, K.H.; Sattin, R.W.; Kennedy, L.W.; Kleinig, J.; et al. Leading Causes of Unintentional and Intentional Injury Mortality: United States, 2000–2009. Am. J. Public Health 2012, 102, e84–e92. [Google Scholar] [CrossRef]
- Lombardi, D.A.; Smith, G.S.; Courtney, T.K.; Brennan, M.J.; Kim, J.Y.; Perry, M.J. Work-related falls from ladders—A follow-back study of US emergency department cases. Scand. J. Work Environ. Health 2011, 37, 525–532. [Google Scholar] [CrossRef]
- Marsh, S.M.; Jackson, L.L. A comparison of fatal occupational injury event characteristics from the Census of Fatal Occupational Injuries and the Vital Statistics Mortality System. J. Saf. Res. 2013, 46, 119–125. [Google Scholar] [CrossRef]
- Pliner, E.M.; Campbell-Kyureghyan, N.H.; Beschorner, K.E. Effects of foot placement, hand positioning, age and climbing biodynamics on ladder slip outcomes. Ergonomics 2014, 57, 1739–1749. [Google Scholar] [CrossRef]
- Pliner, E.; Beschorner, K. Effects of Ladder Climbing Patterns on Fall Severity. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2017, 61, 940–944. [Google Scholar] [CrossRef]
- Pliner, E.M.; Seo, N.J.; Beschorner, K.E. Factors affecting fall severity from a ladder: Impact of climbing direction, gloves, gender and adaptation. Appl Ergon. 2017, 60, 163–170. [Google Scholar] [CrossRef]
- ANSI ASC A14.5-2017: Ladders—Portable Reinforced Plastic—Safety Requirements. Available online: www.americanladderinstitute.org (accessed on 20 December 2023).
- Hsiao, H.; Simeonov, P.; Pizatella, T.; Stout, N.; McDougall, V.; Weeks, J. Extension-ladder safety: Solutions and knowledge gaps. Int. J. Ind. Ergon. 2008, 38, 959–965. [Google Scholar] [CrossRef]
- Ronk, C.J.; Dennerlein, J.T.; Hoffman, E.; Perry, M.J. Is renovation riskier than new construction? An observational comparison of risk factors for stepladder-related falls. Am. J. Ind. Med. 2011, 54, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Young, J.G.; Woolley, C.; Armstrong, T.J.; Ashton-Miller, J.A. Hand-handhold coupling: Effect of handle shape, orientation, and friction on breakaway strength. Hum. Factors: J. Hum. Factors Ergon. Soc. 2009, 51, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Barnett, R.; Poczynok, P. Ladder rung vs. siderail hand grip strategies. Saf. Br. 2000, 16, 1–15. Available online: https://www.scopus.com/inward/record.uri?eid=2-s2.00346549447&partnerID=40&md5=267fd759b67506c915dcab22a98e925c (accessed on 15 December 2023).
- Simeonov, P.; Hsiao, H.; Armstrong, T.; Fu, Q.; Woolley, C.; Kau, T.-Y. Effects of aerial ladder rung spacing on firefighter climbing biomechanics. Appl. Ergon. 2019, 82, 102911. [Google Scholar] [CrossRef] [PubMed]
- Knox, E.H.; Van Bree, M.P. Field Studies and Labeling Research on the Angle of Inclination of Non-Self Supporting Ladders. In Proceedings of the 2010 International Conference on Fall Prevention and Protection, Morgantown, WV, USA, 18–20 May 2010; p. 157. [Google Scholar]
- Simeonov, P.; Hsiao, H.; Kim, I.-J.; Powers, J.R.; Kau, T.-Y. Factors Affecting Extension Ladder Angular Positioning. Hum. Factors J. Hum. Factors Ergon. Soc. 2012, 54, 334–345. [Google Scholar] [CrossRef]
- Campbell, A.O.; Pagano, C.C. The effect of instructions on potential slide-out failures during portable extension ladder angular positioning. Accid. Anal. Prev. 2014, 67, 30–39. [Google Scholar] [CrossRef]
- Simeonov, P.; Hsiao, H.; Powers, J.; Kim, I.-J.; Kau, T.-Y.; Weaver, D. Research to improve extension ladder angular positioning. Appl. Ergon. 2012, 44, 496–502. [Google Scholar] [CrossRef]
- Hoozemans, M.J.; de Looze, M.P.; Kingma, I.; Reijneveld, K.C.; de Korte, E.M.; van der Grinten, M.P.; van Dieën, J.H. Workload of window cleaners using ladders differing in rung separation. Appl. Ergon. 2005, 36, 275–282. [Google Scholar] [CrossRef]
- Thamsuwan, O.; Aulck, L.; Galvin, K.; Johnson, P.W. Comparison of Exposure to Repetitive Upper Arm Motions and Non-neutral Upper Arm Postures between Apple Harvesting with Ladders and Mobile Platforms. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2014, 58, 1585–1589. [Google Scholar] [CrossRef]
- Thamsuwan, O.; Johnson, P.W. Comparing Upper Arm and Back Postural Exposures between Apple Harvesting with Ladders and Mobile Platform. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2015, 59, 1252–1256. [Google Scholar] [CrossRef]
- Thamsuwan, O.; Galvin, K.; Tchong-French, M.; Kim, J.H.; Johnson, P.W. A feasibility study comparing objective and subjective field-based physical exposure measurements during apple harvesting with ladders and mobile platforms. J. Agromedicine 2019, 24, 268–278. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, Y.; Zhang, Z.; Li, D.; Wu, Z.; Bai, R.; Meng, G. Ergonomic and efficiency analysis of conventional apple harvest process. Int. J. Agric. Biol. Eng. 2019, 12, 210–217. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, Z.; Wang, W.; Liu, H.; Sun, Z. The Role of a New Harvest Platform in Alleviation of Apple Workers’ Occupational Injuries During Harvest. J. Agric. Saf. Health 2019, 25, 11–24. [Google Scholar] [CrossRef] [PubMed]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Grinten, M.P. Development of a pratical method for measuring body part discomfort. In Advances in Industrial Egonomics and Safety IV; Taylor and Francis: London, UK, 1992; pp. 311–318. [Google Scholar]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert Scale: Explored and Explained. Br. J. Appl. Sci. Technol. 2015, 7, 396–403. [Google Scholar] [CrossRef]
- Corlett, E.N.; Bishop, R.P. A Technique for Assessing Postural Discomfort. Ergonomics 1976, 19, 175–182. [Google Scholar] [CrossRef]
- Smulders, M.; Berghman, K.; Koenraads, M.; Kane, J.; Krishna, K.; Carter, T.; Schultheis, U. Comfort and pressure distribution in a human contour shaped aircraft seat (developed with 3D scans of the human body). Work 2016, 54, 925–940. [Google Scholar] [CrossRef]
- Califano, R.; Naddeo, A.; Vink, P. The effect of human-mattress interface’s temperature on perceived thermal comfort. Appl. Ergon. 2017, 58, 334–341. [Google Scholar] [CrossRef]
- Naddeo, A.; Cappetti, N.; D’Oria, C. Proposal of a new quantitative method for postural comfort evaluation. Int. J. Ind. Ergon. 2015, 48, 25–35. [Google Scholar] [CrossRef]
- Naddeo, A.; Cappetti, N.; Vallone, M.; Califano, R. New trend line of research about comfort evaluation: Proposal of a framework for weighing and evaluating contributes coming from cognitive, postural and physiologic comfort perceptions. In Proceedings of the 5th International Conference on Applied Human Factors and Ergonomics AHFE 2014, Kraków, Poland, 19–23 July 2014; pp. 503–515. [Google Scholar] [CrossRef]
- Apostolico, A.; Cappetti, N.; D’oria, C.; Naddeo, A.; Sestri, M. Postural comfort evaluation: Experimental identification of Range of Rest Posture for human articular joints. Int. J. Interact. Des. Manuf. (IJIDeM) 2013, 8, 109–120. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Alessandro, N.; Sandro, M. Postural Comfort Inside a Car: Development of an Innovative Model to Evaluate the Discomfort Level. SAE Int. J. Passeng. Cars Mech. Syst. 2009, 2, 1065–1070. [Google Scholar] [CrossRef]
- Fisher, R.A. Statistical Methods for Research Workers. In Breakthroughs in Statistics: Methodology and Distribution; Kotz, S., Johnson, N.L., Eds.; Springer: New York, NY, USA, 1992; pp. 66–70. [Google Scholar] [CrossRef]
- Eminoğlu, M.; Ozguven, M.; Beyaz, A.; Acar, A. Determining Postural Discomfort at Working with Power Tiller. In Proceedings of the 9th International Conference on Energy Efficiency & Agricultural Engineering, Ruse, Bulgaria, 27–29 June 2009. [Google Scholar]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).