
Radiological Measurement of Sella Turcica Dimensions in Different Skeletal Patterns in Romanian Patients

 ,
, 
 ,
,
Abstract
1. Introduction
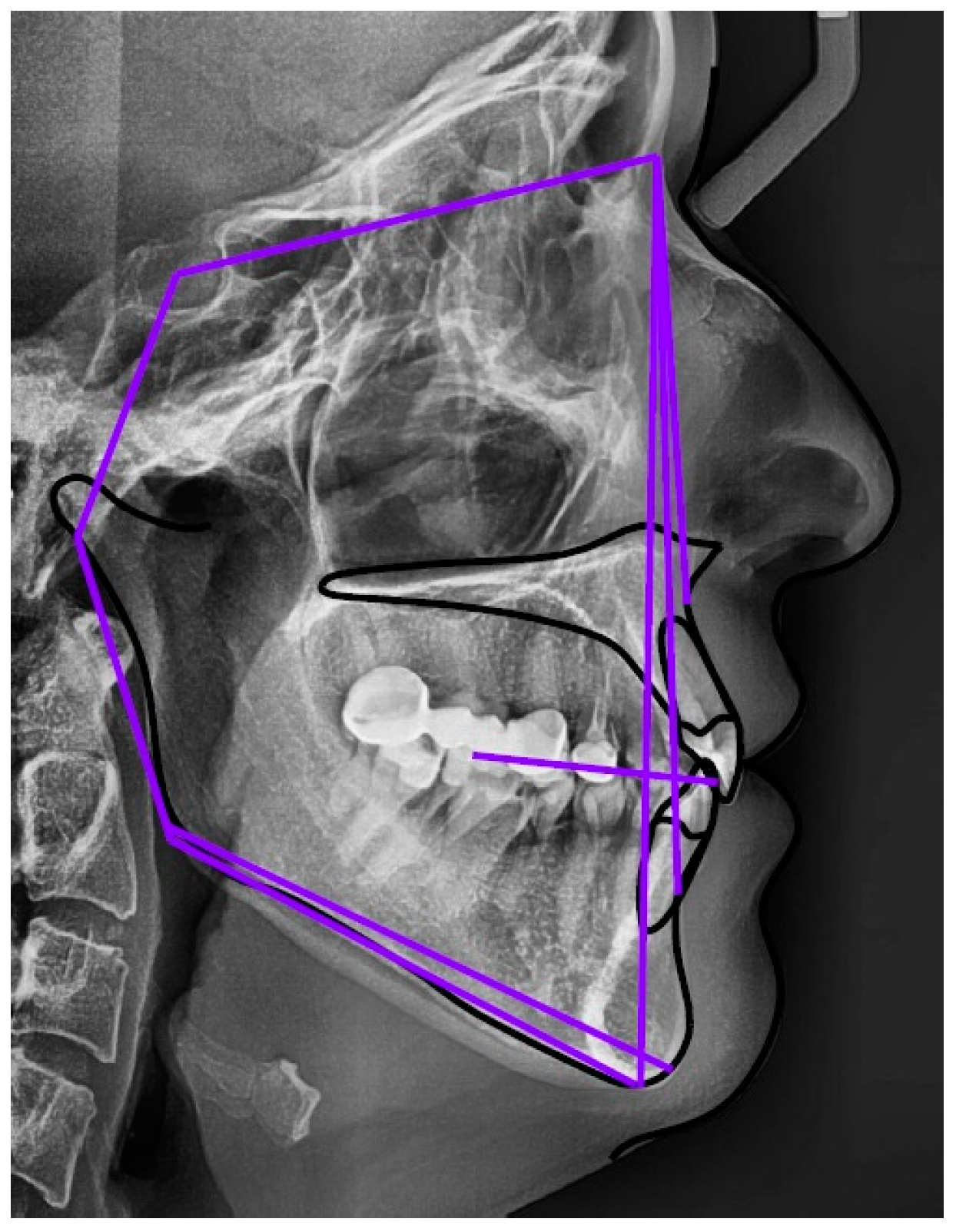
2. Materials and Methods
2.1. Distribution into Skeletal Classes
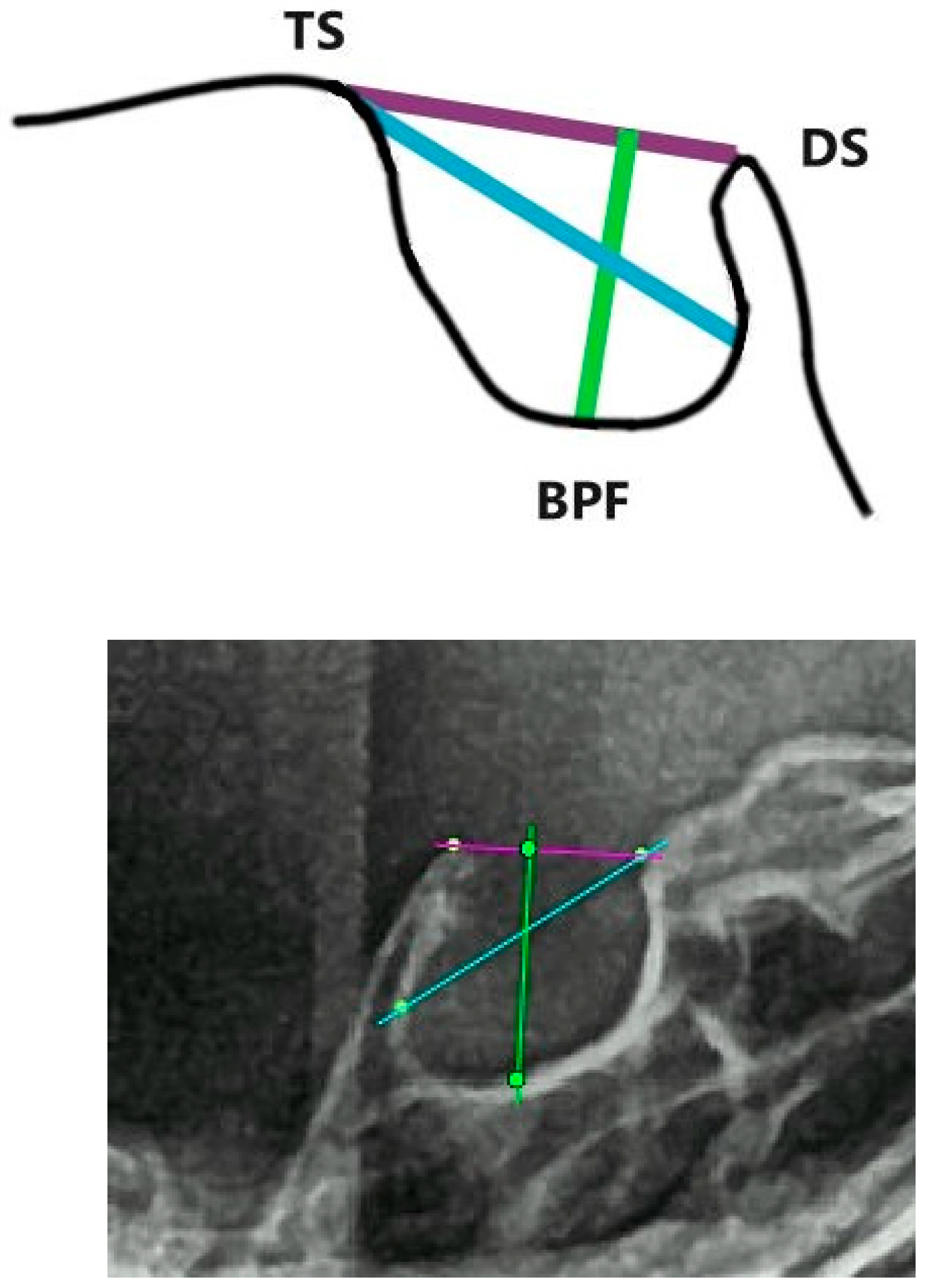
2.2. Dimensions of Sella Turcica
2.3. Morphology of Sella Turcica
2.4. Statistical Analysis
3. Results
3.1. Sella Turcica Dimensions
3.2. Morphology of Sella Turcica
3.3. Statistical Analysis of the Experimental Data
4. Discussion
5. Conclusions
- The average length was 8.98 mm ± 1.470, the average depth was 7.99 mm ± 1.081, and the average diameter was 10.29 mm ± 1.267.
- The smallest dimensions were found in skeletal class II: length 6.12 mm, diameter 6.77 mm and depth 5.69 mm.
- The maximum dimensions were identified in class III, with length 12.45 mm, diameter 13.94 mm and depth 10.56 mm.
- The Q–Q plots, together with the Anova tests with Bonferroni correction and the procedure for calculating the Pearson correlation coefficient, indicate that our results are statistically significant and can be used in the clinical practice of dentistry.
- The morphology of the sella turcica varies greatly. This study found that 51.1% of its participants had a normal sella turcica, representing the majority across all three skeletal classes.
- The findings of the study on the shape and size of the sella turcica can be used as a reference for future research on the morphology of the sella turcica pertaining to a Romanian population.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class I | Length | Diameter | Depth | Class II | Length | Diameter | Depth | Class III | Length | Diameter | Depth |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 9.06 | 10.67 | 7.56 | 1 | 6.92 | 8.79 | 8.16 | 1 | 10.39 | 11.13 | 7.03 |
| 2 | 8.97 | 10.14 | 7.9 | 2 | 11.39 | 10.83 | 7.45 | 2 | 11.79 | 12.02 | 6.61 |
| 3 | 7.2 | 10.31 | 7.61 | 3 | 8.28 | 9.84 | 8.4 | 3 | 10.22 | 11.81 | 8.83 |
| 4 | 9.43 | 11.12 | 8.1 | 4 | 8.01 | 9.86 | 5.69 | 4 | 9.1 | 10.98 | 8.43 |
| 5 | 9.31 | 11.54 | 8.07 | 5 | 10.15 | 9.28 | 6.73 | 5 | 9.25 | 11.6 | 8.62 |
| 6 | 8.36 | 9.94 | 8.71 | 6 | 9.33 | 9.96 | 7.83 | 6 | 10.94 | 13.27 | 10.56 |
| 7 | 9.13 | 10.44 | 6.48 | 7 | 7.15 | 8.06 | 8.26 | 7 | 9.54 | 11.19 | 9.3 |
| 8 | 8.31 | 9.23 | 6.52 | 8 | 7.54 | 9.61 | 8.04 | 8 | 9.13 | 12.5 | 9.73 |
| 9 | 7.56 | 6.86 | 6.4 | 9 | 7.55 | 8.1 | 7.18 | 9 | 10.34 | 10.47 | 10.38 |
| 10 | 8.34 | 9.29 | 8.23 | 10 | 7.85 | 8.12 | 7.27 | 10 | 11.2 | 12.2 | 9.99 |
| 11 | 7.92 | 10.1 | 6.64 | 11 | 6.12 | 8.68 | 8.18 | 11 | 10.63 | 10.12 | 7.45 |
| 12 | 7.38 | 8.76 | 7.33 | 12 | 6.27 | 9.33 | 8.01 | 12 | 8.1 | 10.64 | 10.37 |
| 13 | 9.31 | 9.66 | 6.45 | 13 | 9.49 | 10.37 | 7.11 | 13 | 9.16 | 8.96 | 8.56 |
| 14 | 8.53 | 8.67 | 7.29 | 14 | 7.35 | 9.92 | 7.78 | 14 | 10.2 | 11.53 | 9.51 |
| 15 | 8.48 | 11.1 | 7.51 | 15 | 9.17 | 10.67 | 7.58 | 15 | 12.45 | 11.75 | 9.43 |
| 16 | 9.87 | 8.84 | 6.06 | 16 | 6.94 | 8.5 | 7.32 | 16 | 9.04 | 10.31 | 8.63 |
| 17 | 7.71 | 10.42 | 9.36 | 17 | 7.85 | 10.28 | 7.2 | 17 | 12.23 | 12.26 | 9.17 |
| 18 | 7.81 | 9.81 | 6.56 | 18 | 7.69 | 9.33 | 7.3 | 18 | 8.84 | 10.1 | 8.23 |
| 19 | 9.42 | 10.14 | 9.04 | 19 | 7.56 | 10.21 | 8.06 | 19 | 9.77 | 10.77 | 8.39 |
| 20 | 6.84 | 8.66 | 6.73 | 20 | 7.45 | 10.43 | 6.68 | 20 | 11.62 | 12.36 | 6.96 |
| 21 | 9.9 | 11.68 | 8.59 | 21 | 6.83 | 6.77 | 6.15 | 21 | 9.4 | 10.51 | 8.17 |
| 22 | 10.21 | 10.75 | 8.05 | 22 | 7.06 | 9.83 | 8.41 | 22 | 10.75 | 11.63 | 7.73 |
| 23 | 6.87 | 10.03 | 8.72 | 23 | 8.21 | 9.89 | 7.7 | 23 | 10 | 9.7 | 6.43 |
| 24 | 8.67 | 9.5 | 7.88 | 24 | 9.94 | 10.54 | 8.65 | 24 | 11.84 | 13.94 | 10.36 |
| 25 | 7.09 | 9.66 | 7.9 | 25 | 8.77 | 10.75 | 7.77 | 25 | 8.72 | 10.38 | 9.06 |
| 26 | 10.5 | 11.04 | 7.41 | 26 | 9.71 | 11.32 | 7.75 | 26 | 10.74 | 11.89 | 7.16 |
| 27 | 8.76 | 11.19 | 8.29 | 27 | 9.19 | 9.23 | 8.02 | 27 | 11.9 | 12.34 | 9.44 |
| 28 | 7.39 | 9.99 | 9.22 | 28 | 6.43 | 9.6 | 8.02 | 28 | 10.47 | 10.85 | 8.9 |
| 29 | 8.39 | 9.08 | 6.79 | 29 | 8.16 | 9.99 | 6.93 | 29 | 10.41 | 11.07 | 10.11 |
| 30 | 9.33 | 10.29 | 9.07 | 30 | 9.56 | 8.98 | 7.09 | 30 | 10.84 | 11.97 | 8.88 |
References
- Nielsen, I.L. Cephalometric Analysis: History and Clinical Application. Taiwan J. Orthod. 2022, 34, 1. [Google Scholar] [CrossRef]
- Basavaraj, S.P. An Atlas on Cephalometric Landmarks; JP Medical Ltd.: Tokyo, Japan, 2013; pp. 3–69. [Google Scholar]
- Cohen, A.M.; Ip, H.H.; Linney, A.D. A preliminary study of computer recognition and identification of skeletal landmarks as a new method of cephalometric analysis. Br. J. Orthod. 1984, 11, 143–154. [Google Scholar] [CrossRef]
- Russell, S.J.; Norvig, P. Artificial Intelligence: A Modern Approach, 3rd ed.; Prentice Hall: Hoboken, NJ, USA, 2010; pp. 64–112, 234–436, 610–859, 928–934. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning with Applications in R; Springer: New York, NY, USA, 2013. [Google Scholar]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning, 1st ed.; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Nielsen, M.A. Neural Networks and Deep Learning; Determination Press: San Francisco, CA, USA, 2015; Available online: http://neuralnetworksanddeeplearning.com/ (accessed on 22 February 2024).
- Agrawal, P.; Nikhade, P. Artificial Intelligence in Dentistry: Past, Present, and Future. Cureus 2022, 14, e27405. [Google Scholar] [CrossRef] [PubMed]
- Durão, A.P.R.; Morosolli, A.; Pittayapat, P.; Bolstad, N.; Ferreira, A.P.; Jacobs, R. Cephalometric landmark variability among orthodontists and dentomaxillofacial radiologists: A comparative study. Imaging Sci. Dent. 2015, 45, 213–220. [Google Scholar] [CrossRef]
- Uysal, T.; Baysal, A.; Yagci, A. Evaluation of speed, repeatability, and reproducibility of digital radiography with manual versus computer-assisted cephalometric analyses. Eur. J. Orthod. 2009, 31, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Kiełczykowski, M.; Kamiński, K.; Perkowski, K.; Zadurska, M.; Czochrowska, E. Application of Artificial Intelligence (AI) in a Cephalometric Analysis: A Narrative Review. Diagnostics 2023, 13, 2640. [Google Scholar] [CrossRef] [PubMed]
- Cederberg, R.; Benson, B.; Nunn, M.; English, J. Calcification of the interclinoid and petroclinoid ligaments of sella turcica: A radiographic study of the prevalence. Orthod. Craniofac. Res. 2003, 6, 227–232. [Google Scholar] [CrossRef]
- Hasan, H.A.; Alam, M.K.; Yusof, A.; Mizushima, H.; Kida, A.; Osuga, N. Size and morphology of sella turcica in Malay populations: A 3D CT study. J. Hard Tissue Biol. 2016, 25, 313–320. [Google Scholar] [CrossRef]
- Gibelli, D.; Cellina, M.; Gibelli, S.; Panzeri, M.; Oliva, A.G.; Termine, G.; Sforza, C. Sella turcica bridging and ossified carotico-clinoid ligament: Correlation with sex and age. Neuroradiol. J. 2018, 31, 299–304. [Google Scholar] [CrossRef]
- Kucia, A.; Jankowski, T.; Siewniak, M.; Janiszewska-Olszowska, J.; Grocholewicz, K.; Szych, Z.; Wilk, G. Sella turcica anomalies on lateral cephalometric radiographs of Polish children. Dentomaxillofacial Radiol. 2014, 43, 20140165. [Google Scholar] [CrossRef]
- Miletich, I.; Sharpe, P.T. Neural crest contribution to mammalian tooth formation. Birth Defects Res. Part C Embryo Today Rev. 2004, 72, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Pisaneschi, M.; Kapoor, G. Imaging of the sella and parasellar region. Neuroimaging Clin. N. Am. 2005, 15, 203–219. [Google Scholar] [CrossRef] [PubMed]
- Alkofide, E.A. Pituitary adenoma: A cephalometric finding. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Kavitha, L.; Karthik, K. Comparison of cephalometric norms of caucasians and non-caucasians: A forensic aid in ethnic determination. J. Forensic Dent. Sci. 2012, 4, 53–55. [Google Scholar] [PubMed]
- Alkofide, E.A. The shape and size of the sella turcica in skeletal Class I, Class II, and Class III Saudi subjects. Eur. J. Orthod. 2007, 29, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Silverman, F.N. Roentgen standards fo-size of the pituitary fossa from infancy through adolescence. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1957, 78, 451–460. [Google Scholar]
- Ristau, B.; Coreil, M.; Chapple, A.; Armbruster, P.; Ballard, R. Comparison of AudaxCeph®’s fully automated cephalometric tracing technology to a semi-automated approach by human examiners. Int. Orthod. 2022, 20, 100691. [Google Scholar] [CrossRef]
- Plaza, S.P.; Reimpell, A.; Silva, J.; Montoya, D. Relationship between skeletal Class II and Class III malocclusions with vertical skeletal pattern. Dental Press J. Orthod. 2019, 24, 63–72. [Google Scholar] [CrossRef]
- Kisling, E. Cranial Morphology in Down’s Syndrome: A Comparative Roentgenencephalometric Study in Adult Males; Munksgaard: Copenhagen, Denmark, 1966. [Google Scholar]
- Axelsson, S.; Storhaug, K.; Kjaer, I. Post-natal size, and morphology of the Sella turcica. Longitudinal cephalometric standards for Norwegians between 6 and 21 years of age. Eur. J. Orthod. 2004, 26, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, G.K.; Pokharel, P.R.; Gyawali, R.; Bhattarai, B.; Giri, J. The morphology and bridging of the sella turcica in adult orthodontic patients. BMC Oral Health 2018, 18, 45. [Google Scholar] [CrossRef] [PubMed]
- Motwani, M.B.; Biranjan, R.; Dhole, A.; Choudhary, A.B.; Mohite, A. A Study to Evaluate the Shape and Size of Sella turcica and Its Correlation with the Type of Malocclusion on Lateral Cephalometric Radiographs. IOSR J. Dent. Med. Sci. 2017, 16, 126–132. [Google Scholar] [CrossRef]
- Sathyanarayana, H.P.; Kailasam, V.; Chitharanjan, A.B. The Size and Morphology of Sella Turcica in Different Skeletal Patterns among South Indian Population: A Lateral Cephalometric Study. J. Indian Orthod. Soc. 2013, 47 (Suppl. S4), 266–271. [Google Scholar] [CrossRef]
- Öktem, H.; Tuncer, N.I.; Şençelikel, T.; Bağcı, Z.; Cesaretli, S.; Arslan, A.; Gürsel, I.T.; Değirmenci, B. Sella turcica variations in lateral cephalometric radiographs and their association with malocclusions. Anatomy 2018, 12, 13–19. [Google Scholar] [CrossRef]
- Shah, A.M.; Bashir, U. The Shape and Size of the Sella Turcica in Skeletal Class I, II & III patients, presenting at Islamic International Dental Hospital, Islamabad. Pak. Oral Dent. J. 2011, 1, 104–110. [Google Scholar]
- Ouaknine, G.E.; Hardy, J. Microsurgical anatomy of the pituitary gland and the sellar region: The pituitary Gland. Am. Surg. 1987, 53, 285–290. [Google Scholar] [PubMed]
- Nagaraj, T.; Shruthi, R.; James, L.; Keerthi, I.; Balraj, L.; Goswami, R.D. The size and morphology of sella turcica: A lateral cephalometric study. J. Med. Radiol. Pathol. Surg. 2015, 1, 3–7. [Google Scholar] [CrossRef]
- Filipovie, G.; Burie, M.; Janoševie, M.; Stošie, M. Radiological measuring of sella turcica’s size in different malocclusions. Acta Stomatol. Naissi 2011, 27, 1035–1042. [Google Scholar] [CrossRef]
- Marsan, G.; Oztas, E. Incidence of bridging and dimensions of Sella turcica inclass I and class III Turkish adult female patients. World J. Orthod. 2009, 10, 99–103. [Google Scholar]
- Abdullah, I.M.; Mohammed, L.K. Normal and Abnormal Variations of Sella Turcica in Three Facial Types of Adolescent Iraqi Samples. Med. J. Babylon 2015, 12, 653–660. [Google Scholar]
- Becktor, J.P.; Einersen, S.; Kjaer, I. A sella turcica bridge in subjects with severe craniofacial deviations. Eur. J. Orthod. 2000, 22, 69–74. [Google Scholar] [CrossRef]
- Leonardi, R.; Barbato, E.; Vichi, M.; Caltabiano, M. A sella turcica bridge in subjects with dental anomalies. Eur. J. Orthod. 2006, 28, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Kader, H.M. Sella turcica bridges in orthodontic and orthognathic surgery patients. A retrospective cephalometric study. Aust. Orthod. J. 2007, 23, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Canigur Bavbek, N.; Dincer, M. Dimensions and morphologic variations of sella turcica in type 1 diabetic patients. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Tekiner, H.; Acer, N.; Kelestimur, F. Sella turcica: An anatomical, endocrinological, and historical perspective. Pituitary 2015, 18, 575–578. [Google Scholar] [CrossRef]
- Mansour, A.A.; Alhamza, A.H.A.; Almomin, A.M.S.A.; Zaboon, I.A.; Alibrahim, N.T.Y.; Hussein, R.N.; Kadhim, M.B.; Alidrisi, H.A.Y.; Nwayyir, H.A.; Mohammed, A.G.; et al. Spectrum of Pituitary disorders: A retrospective study from Basrah, Iraq. F1000Research 2018, 7, 430. [Google Scholar] [CrossRef]





| Inclusion | Exclusion |
|---|---|
| Age over 12 years | Craniofacial cleft (syndrome or non-syndrome related) |
| Romanian nationality | History of orthognathic surgery |
| A clear rendering of sella turcica | History of maxillofacial trauma |
| Patients willing to participate in the study | History of neurologic disturbances |
| Endocrine disorders | |
| Hormonal treatment | |
| Corticosteroid treatment |
| Skeletal Class | Number | Mean | Standard Deviation | Standard Error of the Mean | 95% Confidence Interval for Mean | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower Bond | Upper Bond | ||||||||
| Length | Class I | 30 | 8.53 | 0.990 | 0.180 | 8.18 | 8.88 | 6.84 | 10.5 |
| Class II | 30 | 8.13 | 1.264 | 0.230 | 7.67 | 8.58 | 6.12 | 11.39 | |
| Class III | 30 | 10.30 | 1.115 | 0.203 | 9.90 | 10.69 | 8.1 | 12.45 | |
| Total | 90 | 8.98 | 1.470 | 7.13 | 10.84 | 6.12 | 12.45 | ||
| Diameter | Class I | 30 | 9.96 | 1.008 | 0.184 | 9.60 | 10.32 | 6.86 | 11.68 |
| Class II | 30 | 9.56 | 0.980 | 0.179 | 9.21 | 9.91 | 6.77 | 11.32 | |
| Class III | 30 | 11.34 | 1.054 | 0.192 | 10.96 | 11.71 | 8.96 | 13.94 | |
| Total | 90 | 10.29 | 1.267 | 8.165 | 12.41 | 6.77 | 13.94 | ||
| Depth | Class I | 30 | 7.68 | 0.934 | 0.170 | 7.347 | 8.01 | 6.06 | 9.36 |
| Class II | 30 | 7.55 | 0.669 | 0.122 | 7.317 | 7.79 | 5.69 | 8.65 | |
| Class III | 30 | 8.74 | 1.153 | 0.210 | 8.334 | 9.16 | 6.43 | 10.56 | |
| Total | 90 | 7.99 | 1.081 | 6.343 | 9.64 | 5.69 | 10.56 | ||
| Frequency | Percentage | |
|---|---|---|
| Normal | 46 | 51.1% |
| Oblique anterior wall | 9 | 10% |
| Double contour | 7 | 7.77% |
| Irregular posterior wall | 10 | 11.11% |
| Sella turcica bridge | 9 | 10% |
| Pyramidal shape | 9 | 10% |
| Skeletal Class | Number | Mean ± Standard Deviation | Comparison between Skeletal Classes | Students t-Test p Value | ANOVA with Bonferroni Correction | |
|---|---|---|---|---|---|---|
| Length | Class I | 30 | 8.53 ± 0.990 | Class I and Class II | 0.138 | 1.049 × 10−10 (<0.001) |
| Class II | 30 | 8.13 ± 1.264 | Class I and Class III | <0.001 | ||
| Class III | 30 | 10.30 ± 1.115 | Class II and Class III | <0.001 | ||
| Diameter | Class I | 30 | 9.96 ± 1.008 | Class I and Class II | 0.133 | 3.89 × 10−9 (<0.001) |
| Class II | 30 | 9.56 ± 0.980 | Class I and Class III | <0.001 | ||
| Class III | 30 | 11.34 ± 1.054 | Class II and Class III | <0.001 | ||
| Depth | Class I | 30 | 7.68 ± 0.934 | Class I and Class II | 0.567 | 5.24 × 10−6 (<0.001) |
| Class II | 30 | 7.55 ± 0.669 | Class I and Class III | <0.001 | ||
| Class III | 30 | 8.74 ± 1.153 | Class II and Class III | <0.001 |
| Dimensions | Classes | The Pearson Coefficient |
|---|---|---|
| Length | Class I and Class II | 0.213803 |
| Diameter | 0.041007 | |
| Depth | −0.0275 | |
| Length | Class I and Class III | −0.03701 |
| Diameter | 0.102483 | |
| Depth | −0.04229 | |
| Length | Class II and Class III | 0.359194 |
| Diameter | 0.252937 | |
| Depth | 0.110141 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szuhanek, C.-A.; Uzun, A.-P.; Galuscan, A.; Alexa, V.T.; Romanec, L.-C.; Feştilă, D.-G. Radiological Measurement of Sella Turcica Dimensions in Different Skeletal Patterns in Romanian Patients. Appl. Sci. 2024, 14, 2164. https://doi.org/10.3390/app14052164
Szuhanek C-A, Uzun A-P, Galuscan A, Alexa VT, Romanec L-C, Feştilă D-G. Radiological Measurement of Sella Turcica Dimensions in Different Skeletal Patterns in Romanian Patients. Applied Sciences. 2024; 14(5):2164. https://doi.org/10.3390/app14052164
Chicago/Turabian StyleSzuhanek, Camelia-Alexandrina, Anca-Patricia Uzun, Atena Galuscan, Vlad Tiberiu Alexa, Liviu-Cristian Romanec, and Dana-Gabriela Feştilă. 2024. "Radiological Measurement of Sella Turcica Dimensions in Different Skeletal Patterns in Romanian Patients" Applied Sciences 14, no. 5: 2164. https://doi.org/10.3390/app14052164
APA StyleSzuhanek, C.-A., Uzun, A.-P., Galuscan, A., Alexa, V. T., Romanec, L.-C., & Feştilă, D.-G. (2024). Radiological Measurement of Sella Turcica Dimensions in Different Skeletal Patterns in Romanian Patients. Applied Sciences, 14(5), 2164. https://doi.org/10.3390/app14052164