

Brain Extraction Methods in Neonatal Brain MRI and Their Effects on Intracranial Volumes

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. MRI Protocol
2.3. Manual Segmentation for Brain Extraction
2.4. Selection of Automated Brain Extraction Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Brain Extraction Method | Software | Method Category [9] |
|---|---|---|
| Brain Extraction Tool (BET version 2.0, BET2) [8,14] | FSL (FMRIB Software Library) [44] | Deformable surface-based model |
| Simple Watershed Scalping (SWS)—unvalidated module in Morphologically Adaptive Neonate Tissue Segmentation (MANTiS, version 1.1) toolbox [42] | SPM (Statistical Parametric Mapping) [45] running in MATLAB® [46] or as an open-source standalone | Intensity-based (watershed transform) |
| HD Brain Extraction Tool (HD-BET, version 1.0) [19] | Extension of 3D Slicer [38] or as open-source standalone | Deep learning (based on U-Net architecture and its 3D derivatives) |
| SynthStrip (version 1.3) [26] | FreeSurfer [47] or as open-source standalone | Deep learning (based on 3D U-Net) |
2.5. Measurement of Intracranial Volumes
2.6. Hardware and Software
2.7. Evaluation Metrics and Statistical Analysis
2.7.1. Evaluation Metrics
- Voxel-overlap-based metrics: dice coefficient (DC); Jaccard coefficient (JC); precision (Pr); sensitivity (Se); specificity (Sp); false positive rate (FPR); and false negative rate (FNR).
- Volume-based metrics: volume similarity (VS); root mean square error (RMSE); and coefficient of variation of the root mean square error (CVRMSE).
- Surface distance-based metrics: Hausdorff distance (HD); Hausdorff distance 95% percentile (HD95); mean surface distance (MSD); median surface distance (MDSD); and standard deviation surface distance (STDSD).
2.7.2. Statistical Analysis
3. Results
3.1. Reliability Assessment of Manual Segmentation
3.2. Volume Differences between Gender and Gestational Age
3.3. Comparison of Manual vs. Automated Brain Extraction Methods
3.3.1. Segmentation Metrics
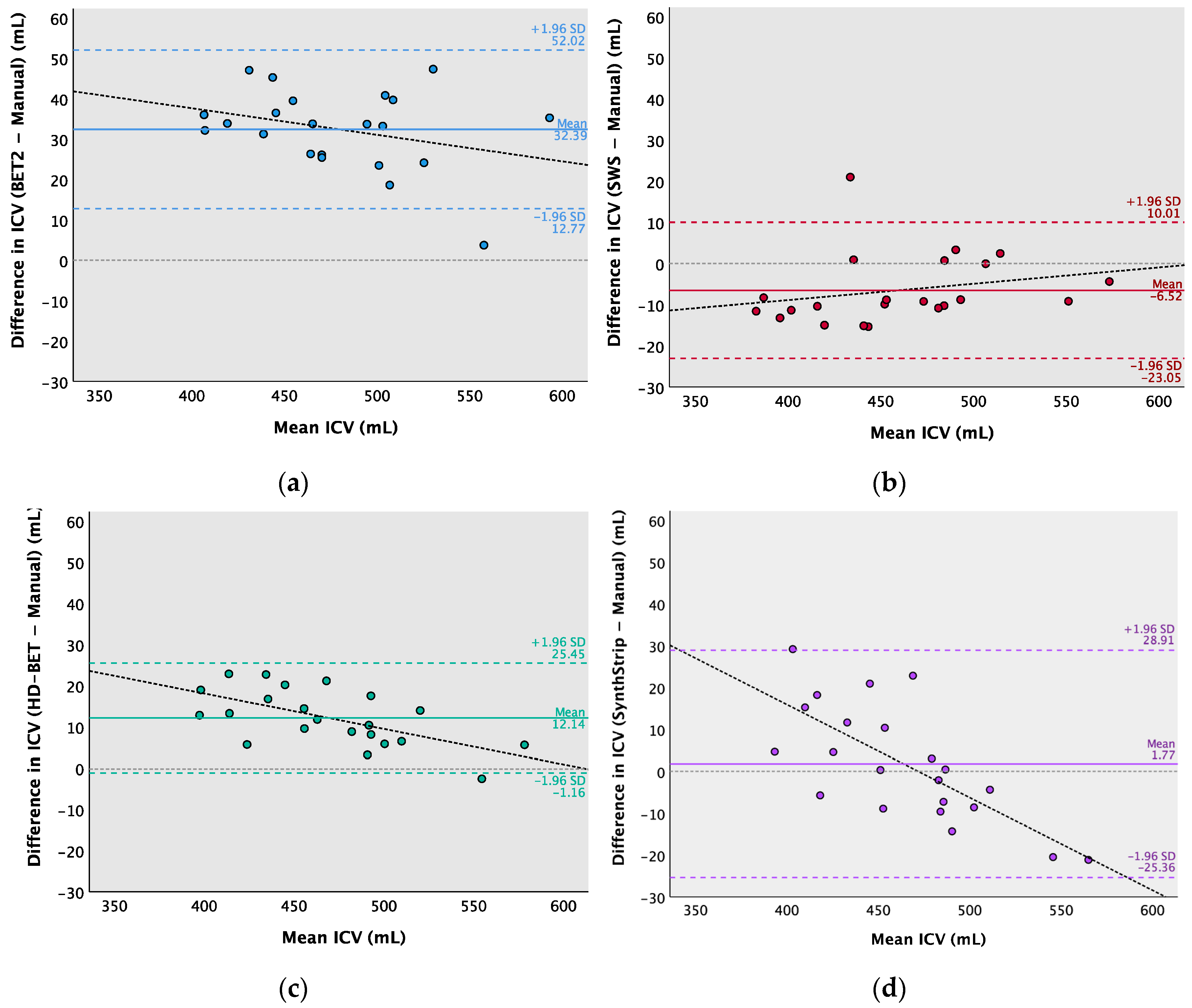
3.3.2. Intracranial Volume Estimation
3.4. Computation Time
4. Discussion
- The influence of our sample size on our Bland–Altman analysis [79] is difficult to determine due to the unknown clinically acceptable agreement limits for ICV measurements of preterm neonates at term. This analysis indicates the likely range of true mean differences in the specific clinical population, considering the potential for random variation [71,72,73]. Nevertheless, the findings from a small sample size are less likely to capture the characteristics and variability of the overall population, mainly when statistical inferences are applied; therefore, caution is needed when generalizing conclusions.
- The presence of brain lesions and congenital condition or motion artifacts might lead to difficulties in accurately delineating the border between the brain and the skull, depending on their severity, location (e.g., near the border of the skull or affecting skull integrity and brain tissue characteristics), and BE method category [9]. When using BET2 [8,14], which is a deformable surface-based model approach, the presence of brain pathology and motion can pose challenges in the evolution of the mesh used to approximate the brain surface, primarily due to intensity and shape variations. However, the BE methods based on deep learning techniques are known to mitigate this constraint [9]. For instance, Isensee et al. [19] stated that HD-BET showed a robust performance in the presence of adult brain pathology- or treatment-induced tissue alterations. Additionally, Hoopes et al. [26] developed SynthStrip to be agnostic to MRI contrasts and acquisition schemes, and it was validated for age, health, resolution, and imaging modality factors. So, it is expected that deep learning methods behave similarly in a pathological neonatal context. Furthermore, motion artifacts can be present, especially in older infants, as it can be challenging to maintain their sleep during scanning [80]. Fortunately, since the typical protocols used in neonatal brain MRI (e.g., low magnetic field strengths and fast imaging sequences) do not provide high-resolution images, they are less sensitive to motion artifacts [81]. Nonetheless, special attention should be given when considering pathological cases with motion artifacts, because the performance of BE methods may vary considerably.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. BET2 Parameters
- Fractional intensity threshold (<f> parameter varied from 0 to 1 in steps of 0.05; 0.50 is the default value), where smaller values results in larger brain outline estimates, and higher values result in smaller brain outline estimates.
- Vertical gradient in fractional intensity threshold (<g> parameter varied from −1 to 1 in steps of 0.05; 0 is the default value), where positive values result in a larger brain outline at the bottom and a smaller one at the top of the scale, and negative values result in the opposite.
- Robust brain centre estimation (<R>), iterates BET2 several times with the purpose of improving the BE, when the input data contains a considerable amount of non-brain matter.
- Eye and optic nerve cleanup (<S>) attempts to clean up the residual eye and optic nerve voxels that are remaining after running standard BE using BET2.
- Bias field and neck cleanup (<B>) attempts to reduce image bias and residual neck voxels after running standard BE using BET2.

Appendix A.2. SynthStrip Parameters
Appendix B
| Metrics | Equations | Description | |
|---|---|---|---|
| Voxel-overlap-based metrics | Dice Coefficient (DC) [69,70,82,83,84] | DC describes the similarity level between the segmentation results (i.e., brain masks obtained with different automatic brain extraction methods) and ground truth (i.e., manual segmentation). It ranges from 0 (no overlap) to 1 (perfect match). DC is the most frequently used metric for accurate analysis of brain extraction and is also known as F1 score/measure or overlap index. | |
| Jaccard Coefficient (JC) [69,70,84,85] | JC is defined as the intersection between the automatic segmentation and the manual segmentation over their union. It ranges from 0 (no intersection) to 1 (full intersection). It is similar to DC regarding the measurement aspects and ranking. | ||
| Precision (Pr) [69,70,84] | Pr is also called the positive predictive value (PPV) or confidence. It is defined as the amount of overlap with respect to the automatic segmentation. | ||
| Sensitivity (Se) [69,70,84] | Se is also called recall or true positive rate (TPR). It is defined as the amount of overlap with respect to manual segmentation. | ||
| Specificity (Sp) [69,70,84] | Sp is also called true negative rate (TNR). It is defined as the fraction of pixels correctly labelled as “background” (i.e., non-brain tissue). | ||
| False Positive Rate (FPR) [69,70,84] | FPR is also called fallout. It can be considered an estimation of over-segmentation, indicating how many pixels identified as brain, by the automatic method, are outside of the manual mask. | ||
| False Negative Rate (FNR) [69,70,84] | FNR is also called miss rate. It can be considered an estimation of under-segmentation, indicating the falsely segmented pixels over the total number of pixels in manual segmentation. | ||
| Volume-based metrics | Volume Similarity (VS) [70,86] | VS represents the volume size difference (as a percentage) between the automatic and manual segmentations, whilst the overlap between brain masks is not considered. A negative VS means the volume is underestimated, and a positive VS means the volume is overestimated. | |
| Root Mean Square Error (RMSE) [87] | RMSE measures the volume (mL) deviations between the automatic and manual segmentations. It is the square root of the mean square error. A smaller RMSE value means better volume agreement between methods. | ||
| Coefficient of Variation of the Root Mean Square Error (CVRMSE) [87] | CVRMSE is also called normalized RMSE or percent RMS. Normalizing the RMSE by the mean value of the manual volume provides the coefficient of variation (%) of the automated volumes relative to the manual volumes. | ||
| Surface distance-based metrics | Hausdorff Distance (HD) [69,70,88,89] | where | HD measures the spatial consistency of the overlap between the automatic and manual segmentations by measuring the maximum surface-to-surface distance between the two brain masks. A smaller HD indicates a higher similarity between brain masks. |
| Hausdorff Distance 95% Percentile (HD95) [69,70,90] | HD95 is similar to the maximum HD but considers only the 95th percentile of the distances in order to overcome the impact of outliers. | ||
| Mean Surface Distance (MSD) [69,89] | MSD represents the average of all of the distances from pixels on the boundary of the automatic segmentation to the boundary of the manual segmentation, and vice versa. | ||
| Median Surface Distance (MDSD) [86] | MDSD represents the median of all of the distances from pixels on the boundary of the automatic segmentation to the boundary of the manual segmentation, and vice versa. | ||
| Standard Deviation Surface Distance (STDSD) [69,89] | STDSD represents the standard deviation of all of the distances from pixels on the boundary of the automatic segmentation to the boundary of the manual segmentation, and vice versa. |
Appendix C


References
- Volpe, J.J. Neurology of the Newborn, 5th ed.; Saunders: Philadelphia, PA, USA, 2008; pp. 172–177. [Google Scholar]
- Rutherford, M.A. Imaging the Neonatal Brain. In The Newborn Brain; Lagercrantz, H., Hanson, M.A., Ment, L.R., Peebles, D.M., Eds.; Cambridge University Press: Cambridge, UK, 2010; pp. 199–210. ISBN 978-0-511-71184-8. [Google Scholar]
- Dubois, J.; Alison, M.; Counsell, S.J.; Hertz-Pannier, L.; Hüppi, P.S.; Benders, M.J.N.L. MRI of the Neonatal Brain: A Review of Methodological Challenges and Neuroscientific Advances. J. Magn. Reason. Imaging 2021, 53, 1318–1343. [Google Scholar] [CrossRef]
- British Association of Perinatal Medicine. Neonatal Brain Magnetic Resonance Imaging: Clinical Indications, Acquisition and Reporting. 2023. Available online: https://www.bapm.org/resources/neonatal-brain-magnetic-resonance-imaging (accessed on 30 November 2023).
- Li, G.; Wang, L.; Yap, P.-T.; Wang, F.; Wu, Z.; Meng, Y.; Dong, P.; Kim, J.; Shi, F.; Rekik, I.; et al. Computational Neuroanatomy of Baby Brains: A Review. NeuroImage 2019, 185, 906–925. [Google Scholar] [CrossRef]
- Devi, C.N.; Chandrasekharan, A.; Sundararaman, V.K.; Alex, Z.C. Neonatal Brain MRI Segmentation: A Review. Comput. Biol. Med. 2015, 64, 163–178. [Google Scholar] [CrossRef]
- Kalavathi, P.; Prasath, V.B.S. Methods on Skull Stripping of MRI Head Scan Images—A Review. J. Digit. Imaging 2016, 29, 365–379. [Google Scholar] [CrossRef]
- Smith, S.M. Fast Robust Automated Brain Extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef]
- Fatima, A.; Shahid, A.R.; Raza, B.; Madni, T.M.; Janjua, U.I. State-of-the-Art Traditional to the Machine- and Deep-Learning-Based Skull Stripping Techniques, Models, and Algorithms. J. Digit. Imaging 2020, 33, 1443–1464. [Google Scholar] [CrossRef]
- Mahapatra, D. Skull Stripping of Neonatal Brain MRI: Using Prior Shape Information with Graph Cuts. J. Digit. Imaging 2012, 25, 802–814. [Google Scholar] [CrossRef]
- Makropoulos, A.; Counsell, S.J.; Rueckert, D. A Review on Automatic Fetal and Neonatal Brain MRI Segmentation. NeuroImage 2018, 170, 231–248. [Google Scholar] [CrossRef]
- Eskildsen, S.F.; Coupé, P.; Fonov, V.; Manjón, J.V.; Leung, K.K.; Guizard, N.; Wassef, S.N.; Østergaard, L.R.; Collins, D.L.; Alzheimer’s Disease Neuroimaging Initiative. BEaST: Brain Extraction Based on Nonlocal Segmentation Technique. NeuroImage 2012, 59, 2362–2373. [Google Scholar] [CrossRef]
- Rex, D.E.; Shattuck, D.W.; Woods, R.P.; Narr, K.L.; Luders, E.; Rehm, K.; Stoltzner, S.E.; Rottenberg, D.A.; Toga, A.W. A Meta-Algorithm for Brain Extraction in MRI. NeuroImage 2004, 23, 625–637. [Google Scholar] [CrossRef]
- Jenkinson, M.; Pechaud, M.; Smith, S. BET2: MR-Based Estimation of Brain, Skull and Scalp Surfaces. In Proceedings of the Eleventh Annual Meeting of the Organization for Human Brain Mapping, Toronto, ON, Canada, 12–16 June 2005. [Google Scholar]
- Shattuck, D.W.; Sandor-Leahy, S.R.; Schaper, K.A.; Rottenberg, D.A.; Leahy, R.M. Magnetic Resonance Image Tissue Classification Using a Partial Volume Model. NeuroImage 2001, 13, 856–876. [Google Scholar] [CrossRef]
- Lucena, O.; Souza, R.; Rittner, L.; Frayne, R.; Lotufo, R. Convolutional Neural Networks for Skull-Stripping in Brain MR Imaging Using Silver Standard Masks. Artif. Intell. Med. 2019, 98, 48–58. [Google Scholar] [CrossRef]
- Kleesiek, J.; Urban, G.; Hubert, A.; Schwarz, D.; Maier-Hein, K.; Bendszus, M.; Biller, A. Deep MRI Brain Extraction: A 3D Convolutional Neural Network for Skull Stripping. NeuroImage 2016, 129, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Ségonne, F.; Dale, A.M.; Busa, E.; Glessner, M.; Salat, D.; Hahn, H.K.; Fischl, B. A Hybrid Approach to the Skull Stripping Problem in MRI. NeuroImage 2004, 22, 1060–1075. [Google Scholar] [CrossRef] [PubMed]
- Isensee, F.; Schell, M.; Pflueger, I.; Brugnara, G.; Bonekamp, D.; Neuberger, U.; Wick, A.; Schlemmer, H.-P.; Heiland, S.; Wick, W.; et al. Automated Brain Extraction of Multisequence MRI Using Artificial Neural Networks. Hum. Brain Mapp. 2019, 40, 4952–4964. [Google Scholar] [CrossRef]
- Doshi, J.; Erus, G.; Ou, Y.; Gaonkar, B.; Davatzikos, C. Multi-Atlas Skull-Stripping. Acad. Radiol. 2013, 20, 1566–1576. [Google Scholar] [CrossRef]
- Rehm, K.; Schaper, K.; Anderson, J.; Woods, R.; Stoltzner, S.; Rottenberg, D. Putting Our Heads Together: A Consensus Approach to Brain/Non-Brain Segmentation in T1-Weighted MR Volumes. NeuroImage 2004, 22, 1262–1270. [Google Scholar] [CrossRef]
- Iglesias, J.E.; Liu, C.-Y.; Thompson, P.M.; Tu, Z. Robust Brain Extraction across Datasets and Comparison with Publicly Available Methods. IEEE Trans. Med. Imaging 2011, 30, 1617–1634. [Google Scholar] [CrossRef]
- Roy, S.; Butman, J.A.; Pham, D.L. Robust Skull Stripping Using Multiple MR Image Contrasts Insensitive to Pathology. NeuroImage 2017, 146, 132–147. [Google Scholar] [CrossRef]
- Rohlfing, T.; Maurer, C.R. Shape-Based Averaging. IEEE Trans. Image Process. 2007, 16, 153–161. [Google Scholar] [CrossRef]
- Carass, A.; Cuzzocreo, J.; Wheeler, M.B.; Bazin, P.-L.; Resnick, S.M.; Prince, J.L. Simple Paradigm for Extra-Cerebral Tissue Removal: Algorithm and Analysis. NeuroImage 2011, 56, 1982–1992. [Google Scholar] [CrossRef][Green Version]
- Hoopes, A.; Mora, J.S.; Dalca, A.V.; Fischl, B.; Hoffmann, M. SynthStrip: Skull-Stripping for Any Brain Image. NeuroImage 2022, 260, 119474. [Google Scholar] [CrossRef]
- Cox, R.W. AFNI: Software for Analysis and Visualization of Functional Magnetic Resonance Neuroimages. Comput. Biomed. Res. 1996, 29, 162–173. [Google Scholar] [CrossRef]
- Hwang, H.; Rehman, H.Z.U.; Lee, S. 3D U-Net for Skull Stripping in Brain MRI. Appl. Sci. 2019, 9, 569. [Google Scholar] [CrossRef]
- Serag, A.; Blesa, M.; Moore, E.J.; Pataky, R.; Sparrow, S.A.; Wilkinson, A.G.; Macnaught, G.; Semple, S.I.; Boardman, J.P. Accurate Learning with Few Atlases (ALFA): An Algorithm for MRI Neonatal Brain Extraction and Comparison with 11 Publicly Available Methods. Sci. Rep. 2016, 6, 23470. [Google Scholar] [CrossRef]
- Wang, L.; Wu, Z.; Chen, L.; Sun, Y.; Lin, W.; Li, G. iBEAT V2.0: A Multisite-Applicable, Deep Learning-Based Pipeline for Infant Cerebral Cortical Surface Reconstruction. Nat. Protoc. 2023, 18, 1488–1509. [Google Scholar] [CrossRef]
- Shi, F.; Wang, L.; Dai, Y.; Gilmore, J.H.; Lin, W.; Shen, D. LABEL: Pediatric Brain Extraction Using Learning-Based Meta-Algorithm. NeuroImage 2012, 62, 1975–1986. [Google Scholar] [CrossRef]
- Warfield, S.K.; Zou, K.H.; Wells, W.M. Simultaneous Truth and Performance Level Estimation (STAPLE): An Algorithm for the Validation of Image Segmentation. IEEE Trans. Med. Imaging 2004, 23, 903–921. [Google Scholar] [CrossRef]
- Péporté, M.; Ilea Ghita, D.E.; Twomey, E.; Whelan, P.F. A Hybrid Approach to Brain Extraction from Premature Infant MRI. In Lecture Notes in Computer Science, Proceedings of the Image Analysis: 17th Scandinavian Conference, SCIA 2011, Ystad, Sweden, 23–25 May 2011; Heyden, A., Kahl, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6688, pp. 719–730. [Google Scholar]
- Yamaguchi, K.; Fujimoto, Y.; Kobashi, S.; Wakata, Y.; Ishikura, R.; Kuramoto, K.; Imawaki, S.; Hirota, S.; Hata, Y. Automated Fuzzy Logic Based Skull Stripping in Neonatal and Infantile MR Images. In Proceedings of the International Conference on Fuzzy Systems, Barcelona, Spain, 18–23 July 2010; pp. 1–7. [Google Scholar]
- Kobashi, S.; Udupa, J.K. Fuzzy Connectedness Image Segmentation for Newborn Brain Extraction in MR Images. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 7136–7139. [Google Scholar]
- Gousias, I.S.; Edwards, A.D.; Rutherford, M.A.; Counsell, S.J.; Hajnal, J.V.; Rueckert, D.; Hammers, A. Magnetic Resonance Imaging of the Newborn Brain: Manual Segmentation of Labelled Atlases in Term-Born and Preterm Infants. Neuroimage 2012, 62, 1499–1509. [Google Scholar] [CrossRef]
- Plaisier, A.; Govaert, P.; Lequin, M.H.; Dudink, J. Optimal Timing of Cerebral MRI in Preterm Infants to Predict Long-Term Neurodevelopmental Outcome: A Systematic Review. AJNR Am. J. Neuroradiol. 2014, 35, 841–847. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reason. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Eritaia, J.; Wood, S.J.; Stuart, G.W.; Bridle, N.; Dudgeon, P.; Maruff, P.; Velakoulis, D.; Pantelis, C. An Optimized Method for Estimating Intracranial Volume from Magnetic Resonance Images. Magn. Reson. Med. 2000, 44, 973–977. [Google Scholar] [CrossRef]
- Mai, J.; Majtanik, M.; Paxinos, G. Atlas of the Human Brain, 4th ed.; Academic Press: Cambridge, MA, USA, 2015; pp. 7–40. [Google Scholar]
- Griffiths, P.D.; Morris, J.; Larroche, J.-C.; Reeves, M. Atlas of Fetal and Postnatal Brain MR Imaging, 1st ed.; Mosby: Philadelphia, PA, USA, 2010; pp. 35–157. [Google Scholar]
- Beare, R.J.; Chen, J.; Kelly, C.E.; Alexopoulos, D.; Smyser, C.D.; Rogers, C.E.; Loh, W.Y.; Matthews, L.G.; Cheong, J.L.Y.; Spittle, A.J.; et al. Neonatal Brain Tissue Classification with Morphological Adaptation and Unified Segmentation. Front. Neuroinform. 2016, 10, 12. [Google Scholar] [CrossRef]
- Merkel, D. Docker: Lightweight Linux Containers for Consistent Development and Deployment. Linux J. 2014, 239, 2. [Google Scholar]
- Jenkinson, M.; Beckmann, C.F.; Behrens, T.E.J.; Woolrich, M.W.; Smith, S.M. FSL. NeuroImage 2012, 62, 782–790. [Google Scholar] [CrossRef]
- Penny, W.D.; Friston, K.J.; Ashburner, J.T.; Kiebel, S.J.; Nichols, T.E. Statistical Parametric Mapping: The Analysis of Functional Brain Images, 1st ed.; Academic Press: Cambridge, MA, USA, 2006; p. 689. [Google Scholar]
- MATLAB Version: 9.14.0 (R2023a); The MathWorks Inc.: Natick, MA, USA, 2023.
- Fischl, B. FreeSurfer. NeuroImage 2012, 62, 774–781. [Google Scholar] [CrossRef]
- Alexander, B.; Kelly, C.E.; Adamson, C.; Beare, R.; Zannino, D.; Chen, J.; Murray, A.L.; Loh, W.Y.; Matthews, L.G.; Warfield, S.K.; et al. Changes in Neonatal Regional Brain Volume Associated with Preterm Birth and Perinatal Factors. NeuroImage 2019, 185, 654–663. [Google Scholar] [CrossRef]
- Thompson, D.K.; Kelly, C.E.; Chen, J.; Beare, R.; Alexander, B.; Seal, M.L.; Lee, K.J.; Matthews, L.G.; Anderson, P.J.; Doyle, L.W.; et al. Characterisation of Brain Volume and Microstructure at Term-Equivalent Age in Infants Born across the Gestational Age Spectrum. Neuroimage Clin. 2019, 21, 101630. [Google Scholar] [CrossRef]
- Alexander, B.; Loh, W.Y.; Matthews, L.G.; Murray, A.L.; Adamson, C.; Beare, R.; Chen, J.; Kelly, C.E.; Anderson, P.J.; Doyle, L.W.; et al. Desikan-Killiany-Tourville Atlas Compatible Version of M-CRIB Neonatal Parcellated Whole Brain Atlas: The M-CRIB 2.0. Front. Neurosci. 2019, 13, 34. [Google Scholar] [CrossRef]
- Thompson, D.K.; Kelly, C.E.; Chen, J.; Beare, R.; Alexander, B.; Seal, M.L.; Lee, K.; Matthews, L.G.; Anderson, P.J.; Doyle, L.W.; et al. Early Life Predictors of Brain Development at Term-Equivalent Age in Infants Born across the Gestational Age Spectrum. NeuroImage 2019, 185, 813–824. [Google Scholar] [CrossRef]
- Kelly, C.E.; Thompson, D.K.; Spittle, A.J.; Chen, J.; Seal, M.L.; Anderson, P.J.; Doyle, L.W.; Cheong, J.L.Y. Regional Brain Volumes, Microstructure and Neurodevelopment in Moderate-Late Preterm Children. Arch. Dis. Child.-Fetal Neonatal Ed. 2020, 105, 593–599. [Google Scholar] [CrossRef]
- Ding, Y.; Acosta, R.; Enguix, V.; Suffren, S.; Ortmann, J.; Luck, D.; Dolz, J.; Lodygensky, G.A. Using Deep Convolutional Neural Networks for Neonatal Brain Image Segmentation. Front. Neurosci. 2020, 14, 207. [Google Scholar] [CrossRef]
- Alexander, B.; Yang, J.Y.-M.; Yao, S.H.W.; Wu, M.H.; Chen, J.; Kelly, C.E.; Ball, G.; Matthews, L.G.; Seal, M.L.; Anderson, P.J.; et al. White Matter Extension of the Melbourne Children’s Regional Infant Brain Atlas: M-CRIB-WM. Hum. Brain Mapp. 2020, 41, 2317–2333. [Google Scholar] [CrossRef]
- Mongerson, C.R.L.; Wilcox, S.L.; Goins, S.M.; Pier, D.B.; Zurakowski, D.; Jennings, R.W.; Bajic, D. Infant Brain Structural MRI Analysis in the Context of Thoracic Non-Cardiac Surgery and Critical Care. Front. Pediatr. 2019, 7, 315. [Google Scholar] [CrossRef]
- Collins, S.E.; Thompson, D.K.; Kelly, C.E.; Gilchrist, C.P.; Matthews, L.G.; Pascoe, L.; Lee, K.J.; Inder, T.E.; Doyle, L.W.; Cheong, J.L.Y.; et al. Development of Regional Brain Gray Matter Volume across the First 13 Years of Life Is Associated with Childhood Math Computation Ability for Children Born Very Preterm and Full Term. Brain Cogn. 2022, 160, 105875. [Google Scholar] [CrossRef]
- Treyvaud, K.; Thompson, D.; Kelly, C.; Loh, W.; Inder, T.; Cheong, J.; Doyle, L.; Anderson, P. Early Parenting Is Associated with the Developing Brains of Children Born Very Preterm. Clin. Neuropsychol. 2021, 35, 885–903. [Google Scholar] [CrossRef]
- Monson, B.B.; Anderson, P.J.; Matthews, L.G.; Neil, J.J.; Kapur, K.; Cheong, J.L.Y.; Doyle, L.W.; Thompson, D.K.; Inder, T.E. Examination of the Pattern of Growth of Cerebral Tissue Volumes From Hospital Discharge to Early Childhood in Very Preterm Infants. JAMA Pediatr. 2016, 170, 772–779. [Google Scholar] [CrossRef]
- Granger, C.; Spittle, A.J.; Walsh, J.; Pyman, J.; Anderson, P.J.; Thompson, D.K.; Lee, K.J.; Coleman, L.; Dagia, C.; Doyle, L.W.; et al. Histologic Chorioamnionitis in Preterm Infants: Correlation with Brain Magnetic Resonance Imaging at Term Equivalent Age. BMC Pediatr. 2018, 18, 63. [Google Scholar] [CrossRef]
- Strahle, J.M.; Triplett, R.L.; Alexopoulos, D.; Smyser, T.A.; Rogers, C.E.; Limbrick, D.D.; Smyser, C.D. Impaired Hippocampal Development and Outcomes in Very Preterm Infants with Perinatal Brain Injury. NeuroImage Clin. 2019, 22, 101787. [Google Scholar] [CrossRef]
- Matthews, L.G.; Smyser, C.D.; Cherkerzian, S.; Alexopoulos, D.; Kenley, J.; Tuuli, M.G.; Michael Nelson, D.; Inder, T.E. Maternal Pomegranate Juice Intake and Brain Structure and Function in Infants with Intrauterine Growth Restriction: A Randomized Controlled Pilot Study. PLoS ONE 2019, 14, e0219596. [Google Scholar] [CrossRef]
- Rudisill, S.S.; Wang, J.T.; Jaimes, C.; Mongerson, C.R.L.; Hansen, A.R.; Jennings, R.W.; Bajic, D. Neurologic Injury and Brain Growth in the Setting of Long-Gap Esophageal Atresia Perioperative Critical Care: A Pilot Study. Brain Sci. 2019, 9, 383. [Google Scholar] [CrossRef]
- Vanderhasselt, T.; Naeyaert, M.; Watté, N.; Allemeersch, G.-J.; Raeymaeckers, S.; Dudink, J.; de Mey, J.; Raeymaekers, H. Synthetic MRI of Preterm Infants at Term-Equivalent Age: Evaluation of Diagnostic Image Quality and Automated Brain Volume Segmentation. AJNR Am. J. Neuroradiol. 2020, 41, 882–888. [Google Scholar] [CrossRef]
- GilchristKelly, C.P.; Thompson, D.K.; Alexander, B.; Kelly, C.E.; Treyvaud, K.; Matthews, L.G.; Pascoe, L.; Zannino, D.; Yates, R.; Adamson, C.; et al. Growth of Prefrontal and Limbic Brain Regions and Anxiety Disorders in Children Born Very Preterm. Psychol. Med. 2023, 53, 759–770. [Google Scholar] [CrossRef]
- Bell, K.A.; Cherkerzian, S.; Drouin, K.; Matthews, L.G.; Inder, T.E.; Prohl, A.K.; Warfield, S.K.; Belfort, M.B. Associations of Macronutrient Intake Determined by Point-of-Care Human Milk Analysis with Brain Development among Very Preterm Infants. Children 2022, 9, 969. [Google Scholar] [CrossRef]
- Whitwell, J.L.; Crum, W.R.; Watt, H.C.; Fox, N.C. Normalization of Cerebral Volumes by Use of Intracranial Volume: Implications for Longitudinal Quantitative MR Imaging. Am. J. Neuroradiol. 2001, 22, 1483–1489. [Google Scholar]
- Van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Yeghiazaryan, V.; Voiculescu, I. Family of Boundary Overlap Metrics for the Evaluation of Medical Image Segmentation. J. Med. Imaging 2018, 5, 015006. [Google Scholar] [CrossRef]
- Taha, A.A.; Hanbury, A. Metrics for Evaluating 3D Medical Image Segmentation: Analysis, Selection, and Tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef]
- Portney, L.G. Foundations of Clinical Research: Applications to Evidence-Based Practice, 4th ed.; FA Davis: Philadelphia, PA, USA, 2020; ISBN 978-0-8036-6113-4. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring Agreement in Method Comparison Studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Beare, R.; Chen, J.; Adamson, C.L.; Silk, T.; Thompson, D.K.; Yang, J.Y.M.; Anderson, V.A.; Seal, M.L.; Wood, A.G. Brain Extraction Using the Watershed Transform from Markers. Front. Neuroinform. 2013, 7, 32. [Google Scholar] [CrossRef]
- Dimitrova, R.; Arulkumaran, S.; Carney, O.; Chew, A.; Falconer, S.; Ciarrusta, J.; Wolfers, T.; Batalle, D.; Cordero-Grande, L.; Price, A.N.; et al. Phenotyping the Preterm Brain: Characterizing Individual Deviations From Normative Volumetric Development in Two Large Infant Cohorts. Cerebral Cortex 2021, 31, 3665–3677. [Google Scholar] [CrossRef]
- Mewes, A.U.J.; Hüppi, P.S.; Als, H.; Rybicki, F.J.; Inder, T.E.; McAnulty, G.B.; Mulkern, R.V.; Robertson, R.L.; Rivkin, M.J.; Warfield, S.K. Regional Brain Development in Serial Magnetic Resonance Imaging of Low-Risk Preterm Infants. Pediatrics 2006, 118, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Gui, L.; Loukas, S.; Lazeyras, F.; Hüppi, P.S.; Meskaldji, D.E.; Borradori Tolsa, C. Longitudinal Study of Neonatal Brain Tissue Volumes in Preterm Infants and Their Ability to Predict Neurodevelopmental Outcome. Neuroimage 2019, 185, 728–741. [Google Scholar] [CrossRef]
- Zacharia, A.; Zimine, S.; Lovblad, K.O.; Warfield, S.; Thoeny, H.; Ozdoba, C.; Bossi, E.; Kreis, R.; Boesch, C.; Schroth, G.; et al. Early Assessment of Brain Maturation by MR Imaging Segmentation in Neonates and Premature Infants. AJNR Am. J. Neuroradiol. 2006, 27, 972–977. [Google Scholar]
- Lu, M.-J.; Zhong, W.-H.; Liu, Y.-X.; Miao, H.-Z.; Li, Y.-C.; Ji, M.-H. Sample Size for Assessing Agreement between Two Methods of Measurement by Bland-Altman Method. Int. J. Biostat. 2016, 12, 20150039. [Google Scholar] [CrossRef]
- Howell, B.R.; Styner, M.A.; Gao, W.; Yap, P.-T.; Wang, L.; Baluyot, K.; Yacoub, E.; Chen, G.; Potts, T.; Salzwedel, A.; et al. The UNC/UMN Baby Connectome Project (BCP): An Overview of the Study Design and Protocol Development. Neuroimage 2019, 185, 891–905. [Google Scholar] [CrossRef]
- Havsteen, I.; Ohlhues, A.; Madsen, K.H.; Nybing, J.D.; Christensen, H.; Christensen, A. Are Movement Artifacts in Magnetic Resonance Imaging a Real Problem?—A Narrative Review. Front. Neurol. 2017, 8, 232. [Google Scholar] [CrossRef]
- Sørensen, T. A Method of Establishing Groups of Equal Amplitude in Plant Sociology Based on Similarity of Species Content and Its Application to Analyses of the Vegetation on Danish Commons. K. Dan. Vidensk. Selsk. 1948, 5, 1–34. [Google Scholar]
- Dice, L.R. Measures of the Amount of Ecologic Association Between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Powers, D.M.W. Evaluation: From Precision, Recall and F-Measure to ROC, Informedness, Markedness and Correlation. Int. J. Mach. Learn. 2011, 2, 37–63. [Google Scholar] [CrossRef]
- Jaccard, P. The Distribution of the Flora in the Alpine Zone. New Phytol. 1912, 11, 37–50. [Google Scholar] [CrossRef]
- Segmentation Evaluation. Available online: http://insightsoftwareconsortium.github.io/SimpleITK-Notebooks/Python_html/34_Segmentation_Evaluation.html (accessed on 26 August 2023).
- Root-Mean-Square Deviation. Wikipedia. 2023. Available online: https://en.wikipedia.org/w/index.php?title=Root-mean-square_deviation&oldid=1171599164 (accessed on 16 September 2023).
- Birsan, T.; Tiba, D. One Hundred Years Since the Introduction of the Set Distance by Dimitrie Pompeiu. In System Modeling and Optimization: Proceedings of the 22nd IFIP TC7 Conference, Turin, Italy, 18–22 July 2005; Ceragioli, F., Dontchev, A., Futura, H., Marti, K., Pandolfi, L., Eds.; Springer: Boston, MA, USA, 2006; pp. 35–39. [Google Scholar]
- Heimann, T.; van Ginneken, B.; Styner, M.A.; Arzhaeva, Y.; Aurich, V.; Bauer, C.; Beck, A.; Becker, C.; Beichel, R.; Bekes, G.; et al. Comparison and Evaluation of Methods for Liver Segmentation From CT Datasets. IEEE Trans. Med. Imaging 2009, 28, 1251–1265. [Google Scholar] [CrossRef]
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The Multimodal Brain Tumor Image Segmentation Benchmark (BRATS). IEEE Trans. Med. Imaging 2015, 34, 1993–2024. [Google Scholar] [CrossRef]



| All Infants (GA < 32 Weeks) | Extremely Preterm (EP) (GA < 28 Weeks) | Very Preterm (VP) (GA 28–31 Weeks) | |
|---|---|---|---|
| Study population | 22 | 8 | 14 |
| Gestational age (GA) in weeks (mean ± standard deviation (range)) | 28.4 ± 2.1 (25–31) | 26.0 ± 0.3 (25–27) | 29.9 ± 0.3 (28–31) |
| Gender (female, male) | 13, 9 | 5, 3 | 6, 8 |
| Median [IQR] of Voxel-Overlap-Based Metrics | |||||||
|---|---|---|---|---|---|---|---|
| DC | JC | Pr | Se | Sp | FPR | FNR | |
| BET2 | 0.937 [0.933; 0.941] | 0.881 [0.874; 0.889] | 0.906 [0.896; 0.912] | 0.971 [0.959; 0.980] | 0.989 [0.988; 0.990] | 0.011 [0.010; 0.012] | 0.029 [0.020; 0.041] |
| SWS | 0.966 [0.963; 0.969] | 0.934 [0.929; 0.939] | 0.977 [0.961; 0.981] | 0.959 [0.954; 0.962] | 0.998 [0.996; 0.998] | 0.003 [0.002; 0.005] | 0.041 [0.038; 0.046] |
| HD-BET | 0.968 [0.965; 0.971] | 0.938 [0.932; 0.944] | 0.958 [0.948; 0.962] | 0.983 [0.974; 0.987] | 0.995 [0.994; 0.996] | 0.005 [0.004; 0.006] | 0.017 [0.013; 0.026] |
| SynthStrip | 0.957 [0.952; 0.961] | 0.917 [0.909; 0.925] | 0.958 [0.944; 0.964] | 0.961 [0.947; 0.969] | 0.996 [0.994; 0.996] | 0.005 [0.004; 0.006] | 0.039 [0.031; 0.053] |
| Median [IQR] of Volume-Based Metrics | Median [IQR] of Surface-Distance-Based Metrics (In mm) | |||||
|---|---|---|---|---|---|---|
| VS (%) | HD | HD95 | MSD | MDSD | STDSD | |
| BET2 | 7.185 [5.512; 8.310] | 32.357 [31.318; 33.586] | 3.600 [3.600; 4.438] | 1.382 [1.282; 1.582] | 0.884 [0.625; 0.975] | 1.940 [1.748; 2.166] |
| SWS | −2.033 [−2.874; 0.028] | 27.339 [11.027; 33.370] | 3.600 [3.125; 3.600] | 0.651 [0.571; 0.794] | 0.000 [0.000; 0.000] | 1.471 [1.106; 1.837] |
| HD-BET | 2.609 [1.320; 4.007] | 7.200 [6.063; 8.975] | 3.156 [2.500; 3.600] | 0.596 [0.463; 0.653] | 0.000 [0.000; 0.000] | 1.008 [0.863; 1.142] |
| SynthStrip | 0.083 [−1.773; 2.945] | 7.500 [7.218; 9.674] | 3.600 [3.125; 3.600] | 0.720 [0.654; 0.941] | 0.000 [0.000; 0.000] | 1.127 [1.032; 1.281] |
| Median [IQR] of Dice Coefficient | |||
|---|---|---|---|
| Bottom Mask (Slices 1 to 11) | Middle Mask (Slices 12 to 22) | Top Mask (Slices 23 to 33) | |
| BET2 | 0.874 [0.857; 0.883] | 0.961 [0.959; 0.963] | 0.915 [0.904; 0.921] |
| SWS | 0.897 [0.877; 0.905] | 0.983 [0.980; 0.985] | 0.960 [0.947; 0.961] |
| HD-BET | 0.944 [0.935; 0.947] | 0.979 [0.976; 0.980] | 0.962 [0.949; 0.961] |
| SynthStrip | 0.926 [0.913; 0.930] | 0.968 [0.966; 0.970] | 0.948 [0.937; 0.952] |
| HD-BET vs. BET2 | HD-BET vs. SWS | HD-BET vs. SynthStrip | SWS vs. BET2 | SWS vs. SynthStrip | SynthStrip vs. BET2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | ||
| Voxel-overlap-based metrics | DC | 2.545 | 0.000 | 0.273 | 1.000 | 1.364 | 0.003 | 2.273 | 0.000 | 1.091 | 0.030 | 1.182 | 0.014 |
| JC | 2.545 | 0.000 | 0.273 | 1.000 | 1.364 | 0.003 | 2.273 | 0.000 | 1.091 | 0.030 | 1.182 | 0.014 | |
| Pr | 1.500 | 0.001 | 1.227 | 0.010 | 0.273 | 1.000 | 2.727 | 0.000 | 0.955 | 0.085 | 1.773 | 0.000 | |
| Se | 1.227 | 0.010 | 2.000 | 0.000 | 2.045 | 0.000 | 0.773 | 0.283 | 0.045 | 1.000 | 0.818 | 0.213 | |
| Sp | 1.455 | 0.001 | 1.318 | 0.004 | 0.318 | 1.000 | 2.773 | 0.000 | 1.000 | 0.061 | 1.773 | 0.000 | |
| FPR | 1.455 | 0.001 | 1.318 | 0.004 | 0.318 | 1.000 | 2.773 | 0.000 | 1.000 | 0.061 | 1.773 | 0.000 | |
| FNR | 1.227 | 0.010 | 2.000 | 0.000 | 2.045 | 0.000 | 0.773 | 0.283 | 0.045 | 1.000 | 0.818 | 0.213 | |
| Volume-based metrics | VS | 1.182 | 0.014 | 1.455 | 0.001 | 1.000 | 0.061 | 2.636 | 0.000 | 0.455 | 1.000 | 2.182 | 0.000 |
| Surface-distance-based metrics | HD | 2.568 | 0.000 | 1.727 | 0.000 | 0.614 | 0.690 | 0.841 | 0.184 | 1.114 | 0.025 | 1.955 | 0.000 |
| HD95 | 2.318 | 0.000 | 0.545 | 0.967 | 0.682 | 0.479 | 1.773 | 0.000 | 0.136 | 1.000 | 1.636 | 0.000 | |
| MSD | 2.545 | 0.000 | 0.591 | 0.774 | 1.045 | 0.043 | 1.955 | 0.000 | 0.455 | 1.000 | 1.500 | 0.001 | |
| MDSD | 2.159 | 0.000 | 0.068 | 1.000 | 0.409 | 1.000 | 2.091 | 0.000 | 0.341 | 1.000 | 1.750 | 0.000 | |
| STDSD | 2.364 | 0.000 | 1.318 | 0.004 | 0.500 | 1.000 | 1.045 | 0.043 | 0.818 | 0.213 | 1.864 | 0.000 | |
| HD-BET vs. BET2 | HD-BET vs. SWS | HD-BET vs. SynthStrip | SWS vs. BET2 | SWS vs. SynthStrip | SynthStrip vs. BET2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | |Z| | adj. p | ||
| Bottom mask (slices 1 to 11) | 7.123 | 0.000 | 5.488 | 0.000 | 2.335 | 0.117 | 1.635 | 0.612 | 3.153 | 0.010 | 4.788 | 0.000 | |
| Middle mask (slices 12 to 22) | 5.021 | 0.000 | 1.868 | 0.370 | 2.919 | 0.021 | 6.890 | 0.000 | 4.788 | 0.000 | 2.102 | 0.213 | |
| Top mask (slices 23 to 33) | 5.839 | 0.000 | 0.117 | 1.000 | 1.985 | 0.283 | 5.722 | 0.000 | 1.868 | 0.370 | 3.854 | 0.001 | |
| 95% Confidence Interval for Mean | ||||||
|---|---|---|---|---|---|---|
| Brain Extraction Method | Mean | Standard Deviation | Minimum | Maximum | Lower Bound | Upper Bound |
| Manual | 463.0 | 50.1 | 388.7 | 575.6 | 440.8 | 485.3 |
| BET2 | 495.4 | 47.0 | 423.2 | 610.8 | 474.6 | 516.3 |
| SWS | 456.5 | 52.2 | 377.1 | 571.2 | 433.4 | 479.6 |
| HD-BET | 475.2 | 46.0 | 403.9 | 581.2 | 454.8 | 495.6 |
| SynthStrip | 464.8 | 40.2 | 395.7 | 554.4 | 447.0 | 482.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaz, T.F.; Canto Moreira, N.; Hellström-Westas, L.; Naseh, N.; Matela, N.; Ferreira, H.A. Brain Extraction Methods in Neonatal Brain MRI and Their Effects on Intracranial Volumes. Appl. Sci. 2024, 14, 1339. https://doi.org/10.3390/app14041339
Vaz TF, Canto Moreira N, Hellström-Westas L, Naseh N, Matela N, Ferreira HA. Brain Extraction Methods in Neonatal Brain MRI and Their Effects on Intracranial Volumes. Applied Sciences. 2024; 14(4):1339. https://doi.org/10.3390/app14041339
Chicago/Turabian StyleVaz, Tânia F., Nuno Canto Moreira, Lena Hellström-Westas, Nima Naseh, Nuno Matela, and Hugo A. Ferreira. 2024. "Brain Extraction Methods in Neonatal Brain MRI and Their Effects on Intracranial Volumes" Applied Sciences 14, no. 4: 1339. https://doi.org/10.3390/app14041339
APA StyleVaz, T. F., Canto Moreira, N., Hellström-Westas, L., Naseh, N., Matela, N., & Ferreira, H. A. (2024). Brain Extraction Methods in Neonatal Brain MRI and Their Effects on Intracranial Volumes. Applied Sciences, 14(4), 1339. https://doi.org/10.3390/app14041339