

Inotrope Analysis for Acute and Chronic Reduced-EF Heart Failure Using Fuzzy Multi-Criteria Decision Analysis



Abstract
1. Introduction
2. Methodology
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- The preference function of each criterion should be defined.
- Importance weights of each criterion where and should be defined aswhere K is the number of criteria.
- For each of the alternative pairs , ∈ , the outranking relation should be determined bywhere denotes the value of the jth criteria of the alternative and denotes the preference indices, which shows the preference intensity for an alternative in comparison to an alternative while counting all criteria simultaneously.
- The positive outranking flow and negative outranking flows should be determined as follows:A positive outranking flow of the alternative ,A negative outranking flow of the alternative ,denotes the number of alternatives. The defines the strength of alternative ∈ A, while the negative outranking flow defines the weakness of alternative ∈ A.
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria/Alternatives | Adrenaline (β1 > β2 > α) | Noradrenaline (β and α) | Dopamine (dopa1-2, α1, β1) | Dobutamine (β1 > β2 > α) | Milrinone (PDE3 Inhibitor) |
|---|---|---|---|---|---|
| Cost | 271 USD/30 mL (30 mg) | 120 USD/40 mL (40 mg) | 141 USD/3000 mL (4800 mg) | 136 USD/3000 mL (6000 mg) | 55.70 USD/200 mL (200 mg) |
| Steady-State Blood Concentration Reached In | 10–15 min | 5 min | 5 min | 10 min | 20 min |
| Half-Life | 3 min | 2.4 min | 2 min | 2 min | 2.5 h |
| Long-Term Use | Short (VL) | Short (VL) | Longer (L) | Longer (M) | Longer (M) |
| Vasodilator | VL | VL | Low Dose Yes | Low Dose Peripheral Yes | Yes |
| Vasopressor | Peripheral and Pulmonary Yes | Yes | High Dose Yes | Neutral–V. High Dose Peripheral Yes | Low |
| Inotropy | 3 (H) | 2 (M) | 3 (H) | 3 (H) | 2 |
| Chronotropic Effect | Positive | Minimal | Positive | Neutral | Minimal (L) |
| Myocardial Oxygen Demand | Tachycardia Increased | Tachycardia Increased | Slight Increase | Significant Increase | Lower |
| Causes Tachyarrhythmia | Yes | Yes | Yes | Yes Mild | Yes |
| Thrombogenic | Yes | No | No | No | No |
| Diuresis | 0 | 1 | 2 | 0 | 0 |
| Peripheral Organ Damage | 5 | 3 | 2 | 1 | 1 |
| Side Effects | 1. Lactic Acidosis 2. Myocardial Ischemia 3. Intracranial Bleeding 4. Hypertension 5. Pulmonary Congestion 6. Hyperglycemia | 1. Increased BP 2. Myocardial Toxicity 3. Hypertension 4. Headache | 1. +PCWP 2. ++Afterload 3. Hypertension | 1. Hypotension 2. Low Dose Reduced Afterload 3. May Build Tolerance 4. Myocarditis 5. Peripheral Eosinophilia | 1. Hypotension 2. Renal Funct. Consideration |
| Effectiveness with Beta Blockers | No | No | No | No | Yes |
| Criteria/Alternatives | Adrenaline (β1 > β2 > α) | Noradrenaline (β and α) | Dopamine (dopa1-2, α1, β1) | Dobutamine (β1 > β2 > α) | Milrinone (PDE3 Inhibitor) |
|---|---|---|---|---|---|
| Cost | 271 USD/30 mL (30 mg) | 120 USD/40 mL (40 mg) | 141 USD/3000 mL (4800 mg) | 136 USD/3000 mL (6000 mg) | 55.70 USD/200 mL (200 mg) |
| Steady-State Blood Concentration Reached In | 10–15 min | 5 min | 5 min | 10 min | 20 min |
| Half-Life | 3 min | 2.4 min | 2 min | 2 min | 2.5 h |
| Long-Term Use | VL | VL | L | M | M |
| Vasodilator | VL | VL | Low Dose Yes | Low Dose Peripheral Yes | Yes |
| Vasopressor | Peripheral and Pulmonary Yes | Yes | High Dose Yes | Neutral—V. High Dose Peripheral Yes | Low |
| Inotropy | 3 | 2 | 3 | 3 | 2 |
| Chronotropic Effect | Positive | Minimal | Positive | Neutral | Minimal |
| Myocardial Oxygen Demand | Tachycardia Increased | Tachycardia Increased | Slight Increase | Significant Increase | Lower |
| Causes Tachyarrhythmia | Yes | Yes | Yes | Yes Mild | Yes |
| Thrombogenic | Yes | No | No | No | No |
| Diuresis | 0 | 1 | 2 | 0 | 0 |
| Peripheral Organ Damage | 5 | 3 | 2 | 1 | 1 |
| Side Effects | 1. Lactic Acidosis 2. Myocardial Ischemia 3. Intracranial Bleeding 4. Hypertension 5. Pulmonary Congestion 6. Hyperglycemia | 1. Increased BP 2. Myocardial Toxicity 3. Hypertension 4. Headache | 1. +PCWP 2. ++Afterload 3. Hypertension | 1. Hypotension 2. Low Dose Reduced Afterload 3. May Build Tolerance 4. Myocarditis 5. Peripheral Eosinophilia | 1. Hypotension 2. Renal Funct. Consideration |
| Effective With Beta Blockers | No | No | No | No | Yes |
References
- American Heart Association Editorial Staff. What is Heart Failure? American Heart Association: Dallas, TX, USA, 2017; Available online: https://www.heart.org/en/health-topics/heart-failure/what-is-heart-failure (accessed on 11 January 2022).
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [PubMed]
- American Heart Association Editorial Staff. Ejection Fraction Heart Failure Measurement; American Heart Association: Dallas, TX, USA, 2017; Available online: https://www.heart.org/en/health-topics/heart-failure/diagnosing-heart-failure/ejection-fraction-heart-failure-measurement (accessed on 11 January 2022).
- Harvard Health Publishing Editorial Staff. Heart Failure: Reduced vs Preserved Pumping; Harvard Health Publishing: Boston, MA, USA, 2020; Available online: https://www.health.harvard.edu/heart-health/heart-failure-reduced-vs-preserved-pumping (accessed on 11 January 2022).
- Murphy, S.P.; Ibrahim, N.E.; Januzzi, J.L. Heart Failure With Reduced Ejection Fraction: A Review. JAMA 2020, 324, 488–504. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Mentzer, G.; Hsich, E.M. Heart Failure with Reduced Ejection Fraction in Women: Epidemiology, Outcomes, and Treatment. Heart Fail. Clin. 2019, 15, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Christopher BOvergaard, C.B.; Džavík, V. Inotropes and Vasopressors. Circulation 2008, 118, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Bistola, V.; Arfaras-Melainis, A.; Polyzogopoulou, E.; Ikonomidis, I.; Parissis, J. Inotropes in Acute Heart Failure: From Guidelines to Practical Use: Therapeutic Options and Clinical Practice. Card. Fail. Rev. 2019, 5, 133–139. [Google Scholar] [CrossRef]
- Berry, W.; McKenzie, C. Use of Inotropes in Critical Care. Clin. Pharm. 2010, 395, 65353. [Google Scholar]
- Tariq, S.; Aronow, W.S. Use of Inotropic Agents in Treatment of Systolic Heart Failure. Int. J. Mol. Sci. 2015, 16, 29060–29068. [Google Scholar] [CrossRef] [PubMed]
- Cochran, J.J.; Cox, L.A., Jr.; Keskinocak, P.; Kharoufeh, J.P.; Smith, J.C.; Franco, L.A.; Montibeller, G. Problem Structuring for Multicriteria Decision Analysis Interventions. In Wiley Encyclopedia of Operations Research and Management Science; Cochran, J.J., Cox, L.A., Keskinocak, P., Kharoufeh, J.P., Smith, J.C., Eds.; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Jahan, A.; Edwards, K.L. Multi-criteria Decision-Making for Materials Selection. In Multi-criteria Decision Analysis for Supporting the Selection of Engineering Materials in Product Design; Elsevier Science: San Diego, CA, USA, 2013; pp. 31–41. [Google Scholar]
- Pelletier, F.; Hájek, P. Metamathematics of Fuzzy Logic; Trends in logic; Kluwer Academic Publishers: Dordrecht, The Netherlands; Boston, MA, USA; London, UK, 1998; Volume 4, 297p. [Google Scholar] [CrossRef]
- Brans, J.P.; Vincke, P. A preference ranking organisation method: The PROMETHEE method for MCDM. Manag. Sci. 1985, 31, 647656. [Google Scholar]
- Uzun, B.; Almasri, A.; Uzun Ozsahin, D. Preference Ranking Organization Method for Enrichment Evaluation (Promethee). In Application of Multi-Criteria Decision Analysis in Environmental and Civil Engineering. Professional Practice in Earth Sciences; Uzun Ozsahin, D., Gökçekuş, H., Uzun, B., LaMoreaux, J., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Yildirim, F.; Sayan, M.; Sanlidag, T.; Uzun, B.; Ozsahin, D.; Ozsahin, I. Comparative Evaluation of the Treatment of COVID-19 with Multicriteria Decision-Making Techniques. J. Healthc. Eng. 2021, 2021, 8864522. [Google Scholar] [CrossRef] [PubMed]
- Sayan, M.; Sarigul Yildirim, F.; Sanlidag, T.; Uzun, B.; Uzun Ozsahin, D.; Ozsahin, I. Capacity Evaluation of Diagnostic Tests For COVID-19 Using Multicriteria Decision-Making Techniques. Comput. Math. Methods Med. 2020, 2020, 1560250. [Google Scholar] [CrossRef]
- Drugs.com. Norepinephrine Prices, Coupons & Patient Assistance Programs—Drugs.com. 2021. Available online: https://www.drugs.com/price-guide/norepinephrine (accessed on 26 August 2021).
- Drugs.com. Dopamine Prices, Coupons & Patient Assistance Programs—Drugs.com. 2021. Available online: https://www.drugs.com/price-guide/dopamine (accessed on 26 August 2021).
- Drugs.com. Dobutamine Prices, Coupons & Patient Assistance Programs—Drugs.com. 2021. Available online: https://www.drugs.com/price-guide/dobutamine (accessed on 26 August 2021).
- Drugs.com. Milrinone Prices, Coupons & Patient Assistance Programs—Drugs.com. 2021. Available online: https://www.drugs.com/price-guide/milrinone (accessed on 26 August 2021).
- Drugs.com. Adrenalin Prices, Coupons & Patient Assistance Programs—Drugs.com. 2021. Available online: https://www.drugs.com/price-guide/adrenalin (accessed on 26 August 2021).
- Guglin, M.; Kaufman, M. Inotropes do not increase mortality in advanced heart failure. Int. J. Gen. Med. 2014, 7, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Belletti, A.; Castro, M.L.; Silvetti, S.; Greco, T.; Biondi-Zoccai, G.; Pasin, L.; Zangrillo, A.; Landoni, G. The Effect of inotropes and vasopressors on mortality: A meta-analysis of randomized clinical trials. Br. J. Anaesth. 2015, 115, 656–675. [Google Scholar] [CrossRef] [PubMed]
- Morici, N.; Sacco, A.; Oliva, F.; Ferrari, S.; Paino, R.; Milazzo, F.; Frigerio, M.; Pirola, R.; Klugmann, S.; Mafrici, A. Epinephrine for acute decompensated heart failure and low output state: Friend or foe? Int. J. Cardiol. 2011, 149, 384–385. [Google Scholar] [CrossRef] [PubMed]
- Accessdata.fda.gov. 2021. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/020201s036lbl.pdf (accessed on 21 September 2021).

| Criteria/Alternatives | Aim/Imp. | Weights | Adrenaline (β1 > β2 > α) | Noradrenaline (β and α) | Dopamine (dopa1-2, α1, β1) | Dobutamine (β1 > β2 > α) | Milrinone (PDE3 Inhibitor) |
|---|---|---|---|---|---|---|---|
| Cost | Min | VL | 271 USD/30 mL (30 mg) | 120 USD/40 mL (40 mg) | 141 USD/3000 mL (4800 mg) | 136 USD/3000 mL (6000 mg) | 55.70 USD/200 mL (200 mg) |
| Steady-State Blood Concentration Reached In | Min | VH | 10–15 min | 5 min | 5 min | 10 min | 20 min |
| Half-Life | Min | M | 3 min | 2.4 min | 2 min | 2 min | 2.5 h |
| Long-Term Use | Max | M | VL | VL | L | M | M |
| Vasodilator | Min | H | VL | VL | L | L | H |
| Vasopressor | Max | VH | VH | VH | H | M | L |
| Inotropy | Max | VH | H | M | H | H | M |
| Chronotropic Effect | Min | M | H | L | H | VL | L |
| Myocardial Oxygen Demand | Min | VH | H | H | M | VH | VL |
| Causes Tachyarrhythmia | Min | VH | VH | H | H | M | H |
| Thrombogenic | Min | H | Yes | No | No | No | No |
| Diuresis | Max | H | VL | M | H | VL | VL |
| Peripheral Organ Damage | Min | L | VH | M | L | VL | VL |
| Side Effects | Min | H | VH | H | M | L | M |
| Effectiveness with Beta Blockers | Max | M | No | No | No | No | Yes |
| Criteria/Alternatives | Aim/Imp. | Weights | Adrenaline (β1 > β2 > α) | Noradrenaline (β and α) | Dopamine (dopa1-2, α1, β1) | Dobutamine (β1 > β2 > α) | Milrinone (PDE3 Inhibitor) |
|---|---|---|---|---|---|---|---|
| Cost | Min | VL | 271 USD/30 mL (30 mg) | 120 USD/40 mL (40 mg) | 141 USD/3000 mL (4800 mg) | 136 USD/3000 mL (6000 mg) | 55.70 USD/200 mL (200 mg) |
| Steady-State Blood Concentration Reached In | Min | H | 10–15 min | 5 min | 5 min | 10 min | 20 min |
| Half-Life | Max | M | 3 min | 2.4 min | 2 min | 2 min | 2.5 h |
| Long-Term Use | Max | H | VL | VL | L | M | M |
| Vasodilator | Max | H | VL | VL | L | L | H |
| Vasopressor | Min | VH | VH | VH | H | M | L |
| Inotropy | Max | VH | H | M | H | H | M |
| Chronotropic Effect | Min | M | H | H | VL | L | |
| Myocardial Oxygen Demand | Min | VH | H | H | M | VH | VL |
| Causes Tachyarrhythmia | Min | VH | VH | H | H | M | H |
| Thrombogenic | Min | VH | Yes | No | No | No | No |
| Diuresis | Max | H | VL | M | H | VL | VL |
| Peripheral Organ Damage | Min | VH | VH | M | L | VL | VL |
| Side Effects | Min | VH | VH | H | M | L | M |
| Effective With Beta Blockers | Max | M | No | No | No | No | Yes |
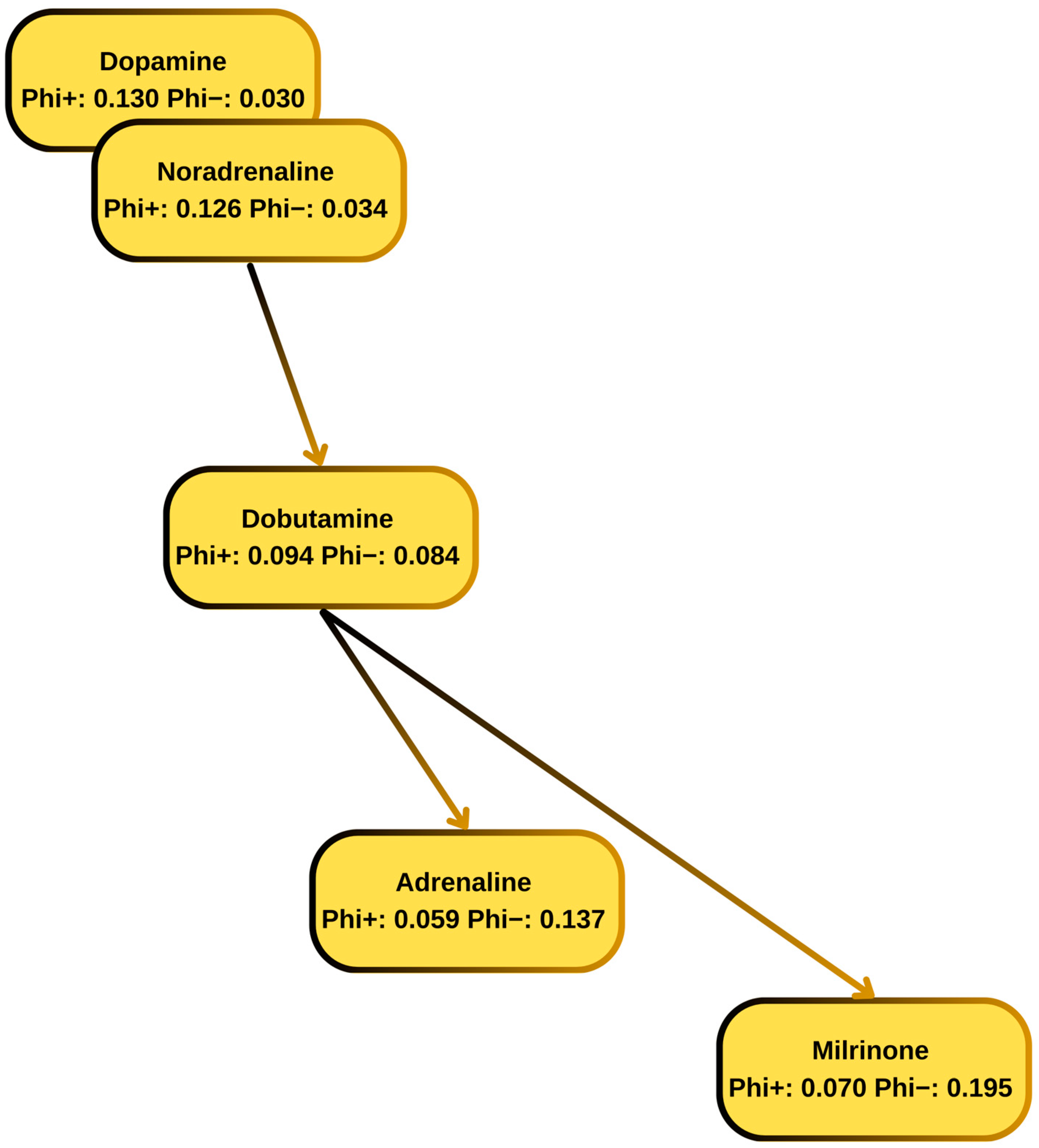
| Rank | Inotrope | |||
|---|---|---|---|---|
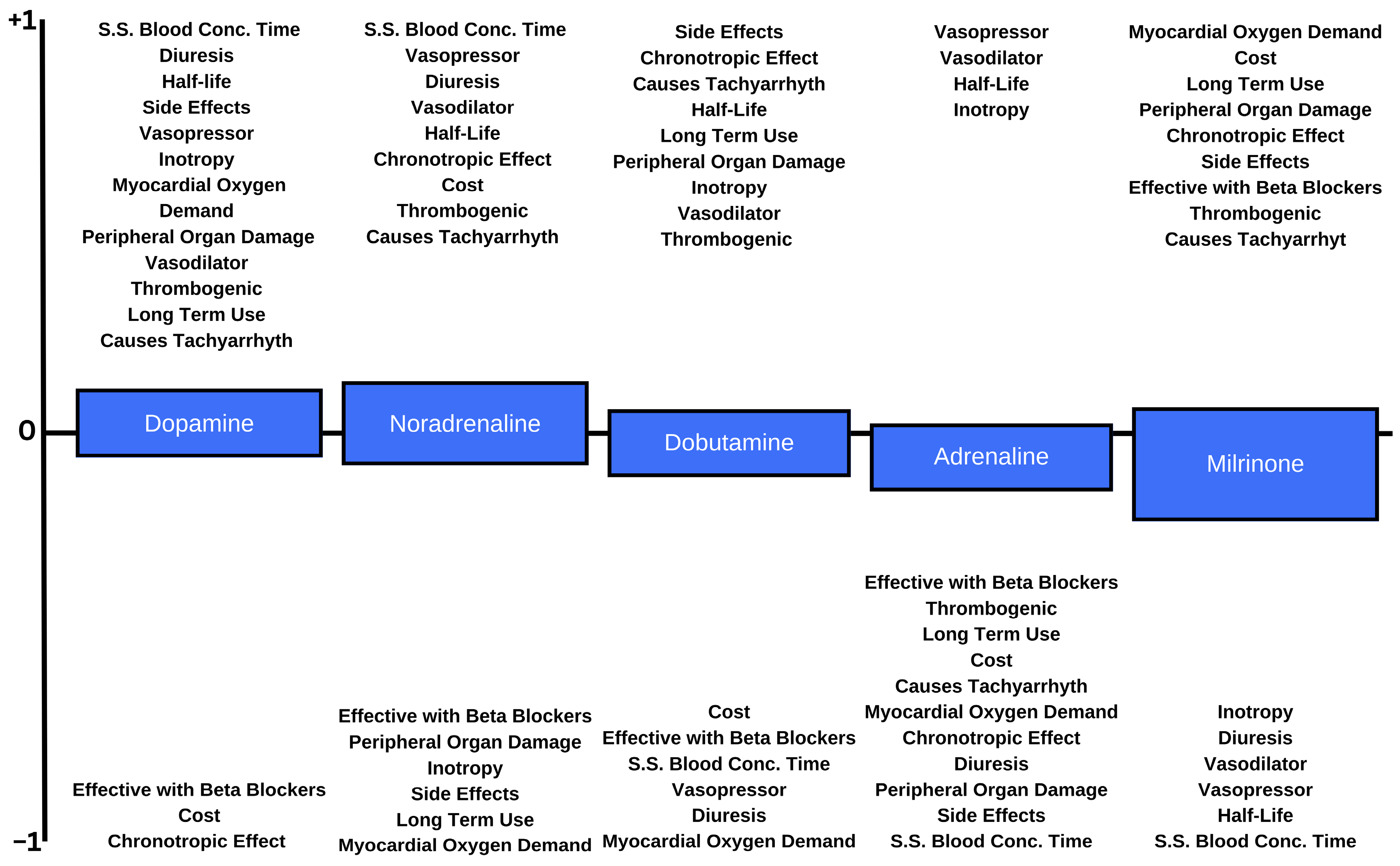
| 1 | Dopamine | 0.0999 | 0.1296 | 0.0297 |
| 2 | Noradrenaline | 0.0923 | 0.1264 | 0.0341 |
| 3 | Dobutamine | 0.0103 | 0.0942 | 0.0840 |
| 4 | Adrenaline | −0.0778 | 0.0588 | 0.1366 |
| 5 | Milrinone | −0.1246 | 0.0703 | 0.1950 |
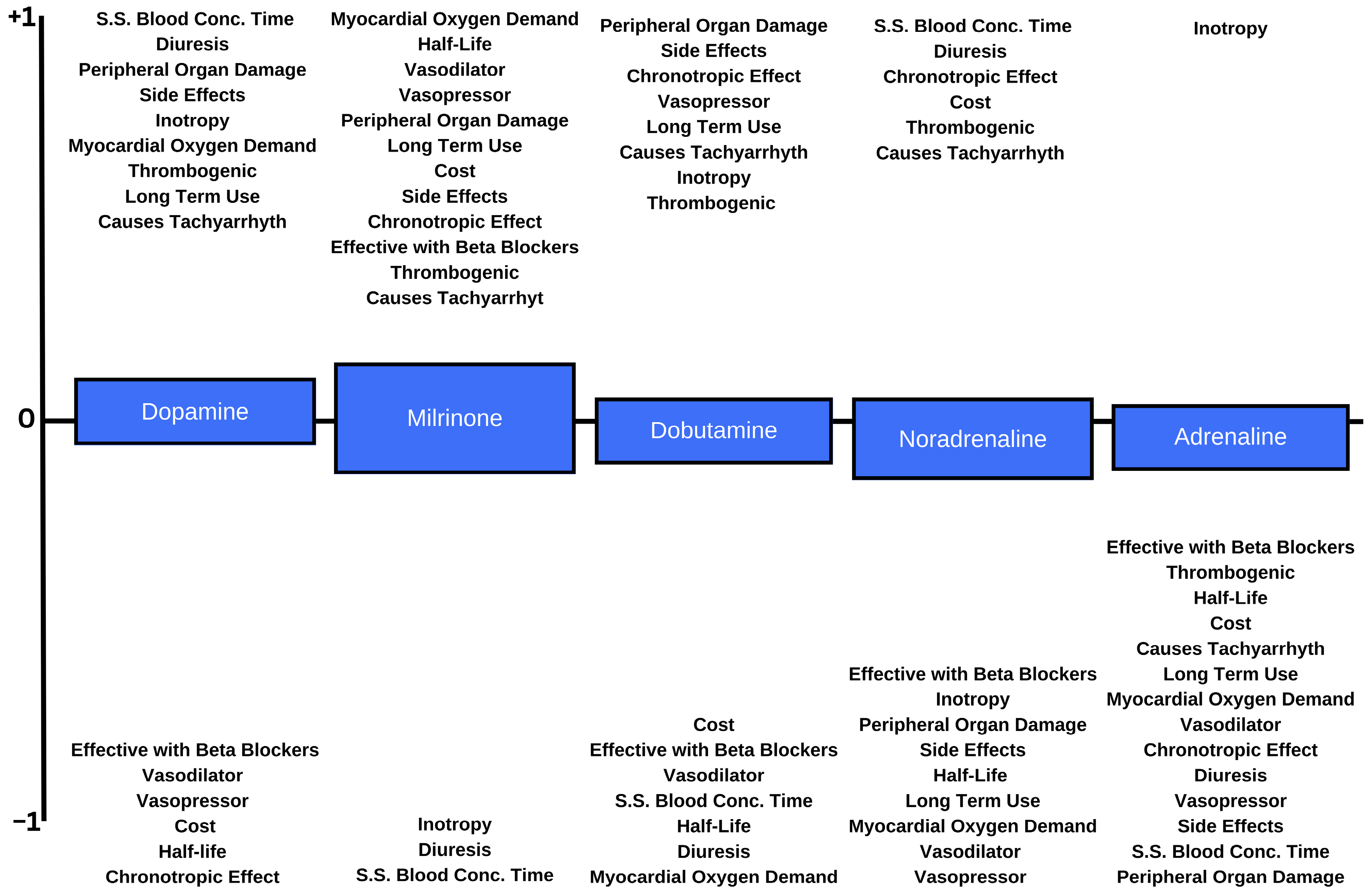
| Rank | Inotrope | |||
|---|---|---|---|---|
| 1 | Dopamine | 0.0632 | 0.1037 | 0.0405 |
| 2 | Milrinone | 0.0565 | 0.1485 | 0.0921 |
| 3 | Dobutamine | 0.0285 | 0.0983 | 0.0698 |
| 4 | Noradrenaline | 0.0081 | 0.0782 | 0.0701 |
| 5 | Adrenaline | −0.1563 | 0.0206 | 0.1769 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozgocmen, C.; Balcioglu, O.; Uzun, B.; Uzun Ozsahin, D. Inotrope Analysis for Acute and Chronic Reduced-EF Heart Failure Using Fuzzy Multi-Criteria Decision Analysis. Appl. Sci. 2024, 14, 4431. https://doi.org/10.3390/app14114431
Ozgocmen C, Balcioglu O, Uzun B, Uzun Ozsahin D. Inotrope Analysis for Acute and Chronic Reduced-EF Heart Failure Using Fuzzy Multi-Criteria Decision Analysis. Applied Sciences. 2024; 14(11):4431. https://doi.org/10.3390/app14114431
Chicago/Turabian StyleOzgocmen, Cemre, Ozlem Balcioglu, Berna Uzun, and Dilber Uzun Ozsahin. 2024. "Inotrope Analysis for Acute and Chronic Reduced-EF Heart Failure Using Fuzzy Multi-Criteria Decision Analysis" Applied Sciences 14, no. 11: 4431. https://doi.org/10.3390/app14114431
APA StyleOzgocmen, C., Balcioglu, O., Uzun, B., & Uzun Ozsahin, D. (2024). Inotrope Analysis for Acute and Chronic Reduced-EF Heart Failure Using Fuzzy Multi-Criteria Decision Analysis. Applied Sciences, 14(11), 4431. https://doi.org/10.3390/app14114431