




Considering the Consequences of Cybersickness in Immersive Virtual Reality Rehabilitation: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Searching Process
2.2. Data Analysis
3. Results
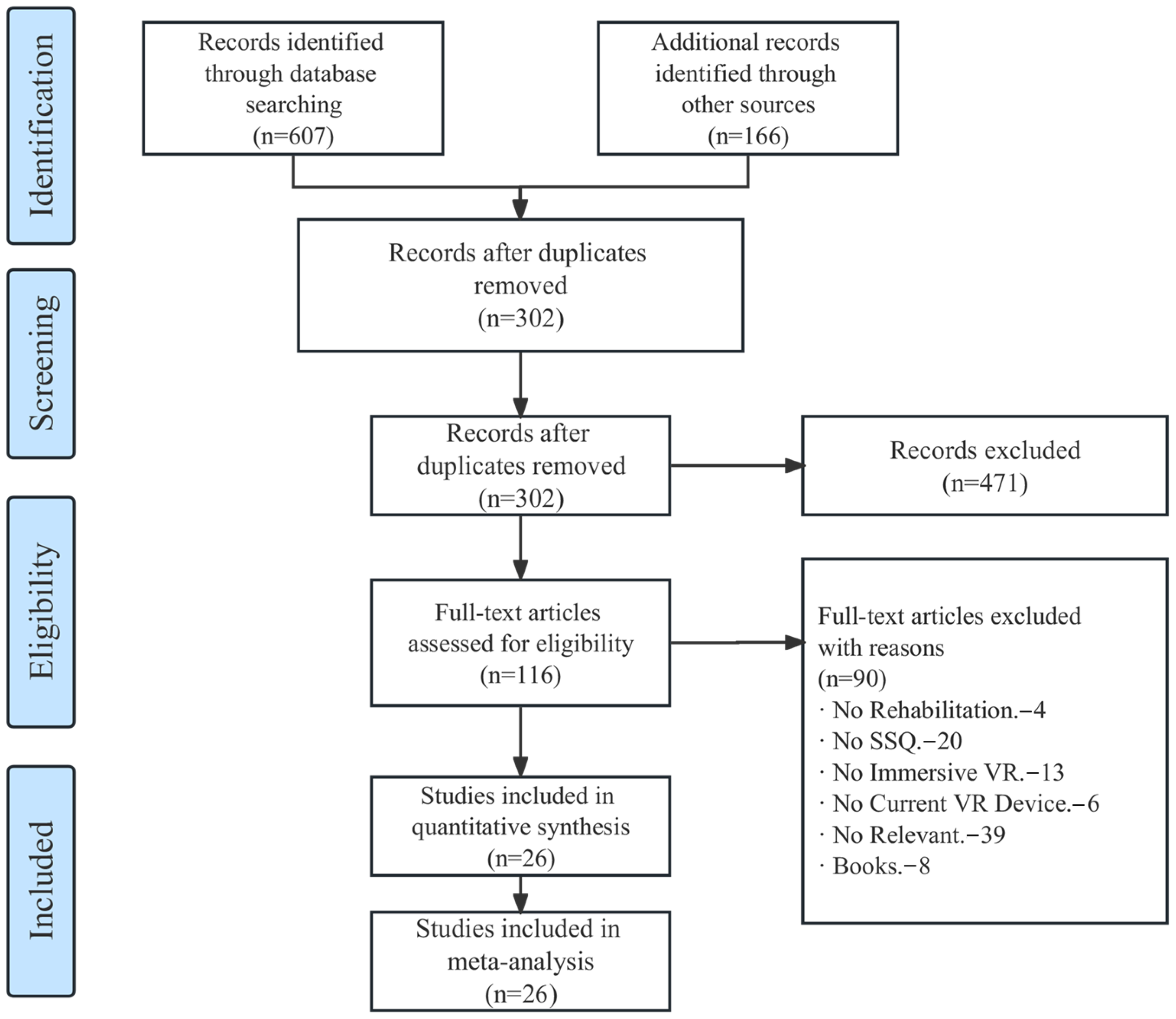
3.1. Study Identification
3.2. Study Details
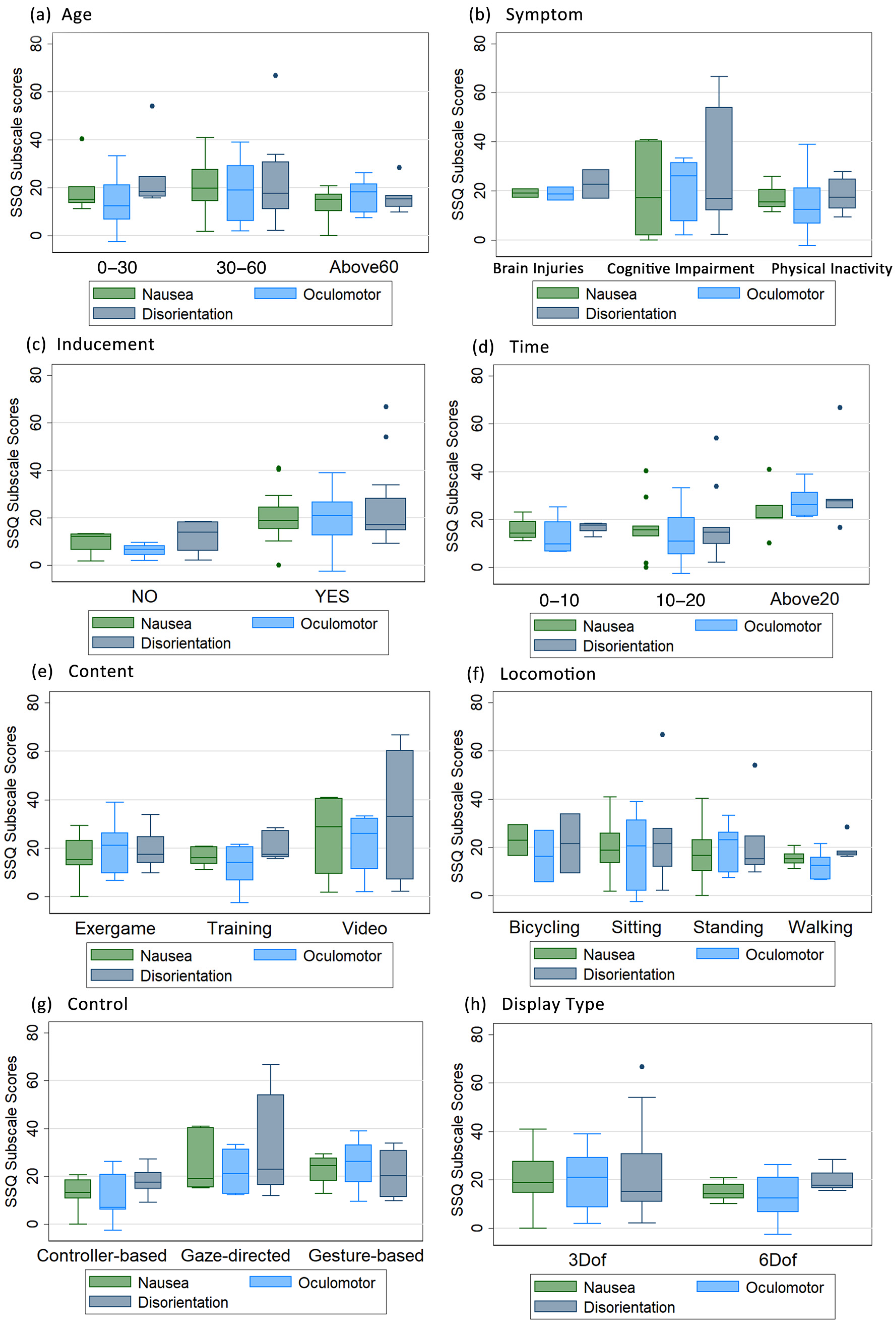
3.3. Subject Characters and VR Cybersickness
3.4. VR Software and Cybersickness
3.5. VR Hardware and Cybersickness
4. Discussion
4.1. Demographic of Cybersickness
4.2. Software Factors of Cybersickness
4.3. Hardware Factors of Cybersickness
4.4. Strengths, Limitations, and Future Works
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
| Abbreviations | Description | Abbreviations | Description |
| AD-ACL | Activation–Deactivation Adjective Check List | AES | Apathy Evaluation Scale |
| CCT | Computerized Cognitive Training | CERAD-K | A Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment |
| CET | Cognitive Evaluation Theory | DHI | Dizziness Handicap Inventory |
| IMI | Intrinsic Motivation Inventory | DOF | Degrees of Freedom |
| EDQ | Equipment and Display Questionnaire | GMS | Global Motivation Scale |
| ITC-SOPI | International Test Commission—Sense of Presence Inventory | ICU-VR | ICU-specific VR |
| HMD | Head-Mounted Display | KQOL-AD | Korean Version of Quality of Life—Alzheimer’s Disease |
| GEQ | Game Experience Questionnaire | GDS | Geriatric Depression Scale |
| MCI | Mild Cognitive Impairment | GSR | Galvanic Skin Response |
| NDI | Neck Disability Index | NASA-TLX | NASA Task Load Index |
| QoE | Quality of Experience | RAGT | Robot-Assisted Gait Training |
| VEQ | Virtual Embodiment Questionnaire | SoP | Sense of Presence |
| SP | Spatial Presence | RTLX | Raw Task Load Index |
| SMET | Submaximal Tourniquet Effort Test | PAS | Psychogeriatric Assessment Scale |
| QoE | Quality of Experience | SCR | Skin Conductance Response |
| PQ | Presence Questionnaire | VRSQ | Virtual Reality Symptom Questionnaire |
| UEQ | Experience Questionnaire | USEQ | User Satisfaction Evaluation Questionnaire |
| SS-VAS | Simulator Sickness Visual Analog Scale | VRISE | VR Sickness or Virtual Reality-Induced Symptoms and Effects |
| SSQ | Simulator Sickness Questionnaire | SUS | System Usability Scale |
| VSS | Visual Symptoms Scale | VRCT | Virtual Reality-Based Cognitive Therapy |
| VAS | Visual Analog Scale | TAM | Technology Acceptance Model |
Appendix B
| Section and Topic | Item | Checklist Item | Location Where Item Is Reported |
| TITLE | |||
| Title | 1 | Identify the report as both systematic review and meta-analysis. | Page 1 |
| ABSTRACT | |||
| Structure summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; conclusions and implications of key findings. | Page 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | Page 2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | Page 2–4 |
| METHODS | |||
| Eligibility criteria | 5 | Present the systematic review registration number. And specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 4 |
| Information sources | 6 | Specify all databases, registers, websites, organizations, reference lists and other sources searched or consulted to identify studies. | Page 4 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Page 4–5 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Page 5 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators. | Page 5 |
| Data items | 10 | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses). | Page 5 |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Page 5 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | Page 5 |
| Synthesis methods | 13 | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | Page 5–6 |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Page 5–6 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Page 6 |
| RESULTS | |||
| Study selection | 16 | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 7 Figure 2 |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Page 7 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for included study. | Page 14 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Table 2 and Table 3 |
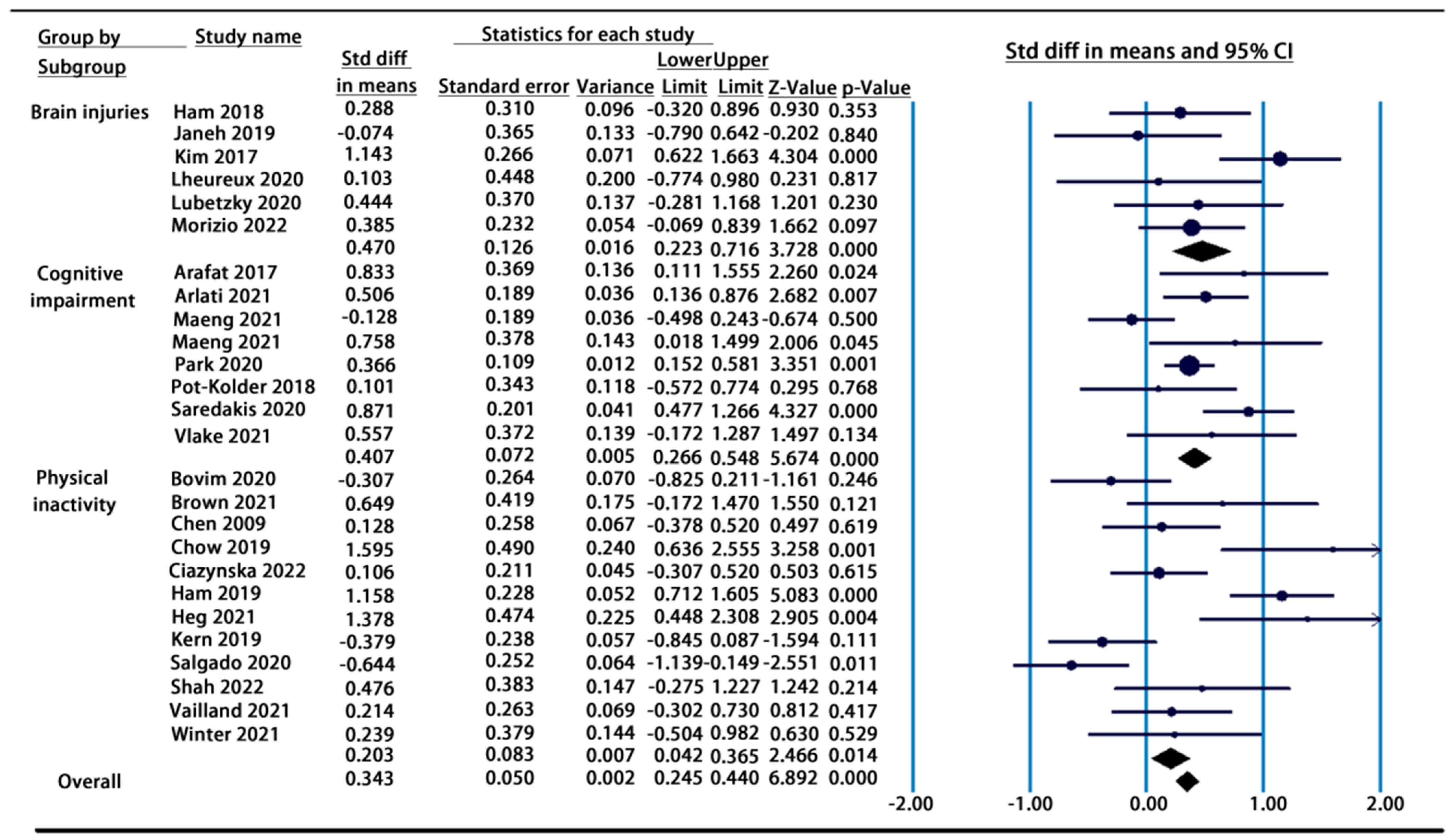
| Results of syntheses | 20 | Present results of all statistical syntheses conducted. As meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. Comparing the groups and describing the direction of the effect. | Figure 3 and Figure 4 Table 4, Table 5 and Table 6 |
| Reporting biases | 21 | Present results of any assessment of risk of bias across studies (see Item 18). | Page 14 |
| DISCUSSION | |||
| Discussion | 22 | Provide a general interpretation of the results in the context of other evidence and implications of the results for practice, policy, and future research. | Page 20 |
| OTHER INFORMATION | |||
| Registration and protocol | 23 | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | NA |
| Support | 24 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | NA |
| Competing interests | 25 | Declare any competing interests of review authors. | NA |
| Availability of data, code and other materials | 26 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | NA |
| From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/, accessed on 9 January 2023. | |||
References
- Tan, T.F.M.; Li, Y.; Lim, J.S.F.; Gunasekeran, D.V.M.; Teo, Z.L.M.; Ng, W.Y.F.; Ting, D.S. Metaverse and Virtual Health Care in Ophthalmology: Opportunities and Challenges. Asia-Pac. J. Ophthalmol. 2022, 11, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Kye, B.; Han, N.; Kim, E.; Park, Y.; Jo, S. Educational applications of metaverse: Possibilities and limitations. J. Educ. Evaluation Health Prof. 2021, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Monardo, G.; Pavese, C.; Giorgi, I.; Godi, M.; Colombo, R. Evaluation of Patient Motivation and Satisfaction During Technology-Assisted Rehabilitation: An Experiential Review. Games Health J. 2021, 10, 13–27. [Google Scholar] [CrossRef]
- Petri, K.; Feuerstein, K.; Folster, S.; Bariszlovich, F.; Witte, K. Effects of Age, Gender, Familiarity with the Content, and Exposure Time on Cybersickness in Immersive Head-mounted Display Based Virtual Reality. Am. J. Biomed. Sci. 2020, 12, 107–121. [Google Scholar] [CrossRef]
- Burdea, G.C. Virtual rehabilitation–benefits and challenges. Methods Inf. Med. 2003, 42, 519–523. [Google Scholar]
- Rose, T.; Nam, C.S.; Chen, K.B. Immersion of virtual reality for rehabilitation—Review. Appl. Ergon. 2018, 69, 153–161. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Cerasa, A.; Ciancarelli, I.; Pignolo, L.; Tonin, P.; Iosa, M.; Morone, G. The arrival of the metaverse in neurorehabilitation: Fact, fake or vision? Biomedicines 2022, 10, 2602. [Google Scholar] [CrossRef]
- Kurz, A.; Pohl, C.; Ramsenthaler, M.; Sorg, C. Cognitive rehabilitation in patients with mild cognitive impairment. Int. J. Geriatr. Psychiatry A J. Psychiatry Late Life Allied Sci. 2009, 24, 163–168. [Google Scholar] [CrossRef]
- Teasell, R.; Bayona, N.; Marshall, S.; Cullen, N.; Bayley, M.; Chundamala, J.; Villamere, J.; Mackie, D.; Rees, L.; Hartridge, C.; et al. A systematic review of the rehabilitation of moderate to severe acquired brain injuries. Brain Inj. 2007, 21, 107–112. [Google Scholar] [CrossRef]
- Zelle, D.M.; Klaassen, G.; Van Adrichem, E.; Bakker, S.J.; Corpeleijn, E.; Navis, G. Physical inactivity: A risk factor and target for intervention in renal care. Nat. Rev. Nephrol. 2017, 13, 152–168. [Google Scholar] [CrossRef]
- Kim, O.; Pang, Y.; Kim, J.-H. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry 2019, 19, 219. [Google Scholar] [CrossRef]
- Cullen, N.; Chundamala, J.; Bayley, M.; Jutai, J. The efficacy of acquired brain injury rehabilitation. Brain Inj. 2007, 21, 113–132. [Google Scholar] [CrossRef]
- Dębska, M.; Polechoński, J.; Mynarski, A.; Polechoński, P. Enjoyment and Intensity of Physical Activity in Immersive Virtual Reality Performed on Innovative Training Devices in Compliance with Recommendations for Health. Int. J. Environ. Res. Public Health 2019, 16, 3673. [Google Scholar] [CrossRef]
- Takkouche, B.; Norman, G. Prisma statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Rebenitsch, L.; Owen, C. Individual variation in susceptibility to cybersickness. In Proceedings of the 27th annual ACM Symposium on User Interface Software and Technology, Honolulu, HI, USA, 5–8 October 2014; pp. 309–317. [Google Scholar]
- Bruck, S.; Watters, P.A. Estimating Cybersickness of Simulated Motion Using the Simulator Sickness Questionnaire (SSQ): A Controlled Study. In Proceedings of the 2009 6th International Conference on Computer Graphics, Imaging and Visualization, Tianjin, China, 11–14 August 2009; pp. 486–488. [Google Scholar] [CrossRef]
- Arafat, I.M. Cybersickness in Persons with Multiple Sclerosis. Ph.D. Thesis, The University of Texas at San Antonio, San Antonio, TX, USA, 2019. [Google Scholar]
- Arlati, S.; Di Santo, S.G.; Franchini, F.; Mondellini, M.; Filiputti, B.; Luchi, M.; Ratto, F.; Ferrigno, G.; Sacco, M.; Greci, L. Acceptance and Usability of Immersive Virtual Reality in Older Adults with Objective and Subjective Cognitive Decline. J. Alzheimer’s Dis. 2021, 80, 1025–1038. [Google Scholar] [CrossRef]
- Bovim, L.P.; Gjesdal, B.E.; Mæland, S.; Aaslund, M.K.; Bogen, B. The impact of motor task and environmental constraints on gait patterns during treadmill walking in a fully immersive virtual environment. Gait Posture 2020, 77, 243–249. [Google Scholar] [CrossRef]
- Brown, P.; Powell, W. Pre-Exposure Cybersickness Assessment Within a Chronic Pain Population in Virtual Reality. Front. Virtual Real. 2021, 2, 67. [Google Scholar] [CrossRef]
- Chen, C.-H.; Jeng, M.-C.; Fung, C.-P.; Doong, J.-L.; Chuang, T.-Y. Psychological benefits of virtual reality for patients in rehabilitation therapy. J. Sport Rehabil. 2009, 18, 258–268. [Google Scholar] [CrossRef]
- Chowdhury, T.; Ferdous, S.; Peck, T.; Quarles, J. Virtual ability simulation: Applying rotational gain to the leg to increase confidence during physical rehabilitation. In Proceedings of the ICAT-EGVE 2019-International Conference on Artificial Reality and Telexistence and Eurographics Symposium on Virtual Environments, Tokyo, Japan, 11–13 September 2019. [Google Scholar]
- Ciążyńska, J.; Janowski, M.; Maciaszek, J. Effects of a Modern Virtual Reality 3D Head-Mounted Display Exergame on Simulator Sickness and Immersion Under Specific Conditions in Young Women and Men: Experimental Study. JMIR Serious Games 2022, 10, e41234. [Google Scholar] [CrossRef]
- Hamzeheinejad, N.; Straka, S.; Gall, D.; Weilbach, F.; Latoschik, M.E. Immersive Robot-Assisted Virtual Reality Therapy for Neurologically-Caused Gait Impairments. In Proceedings of the 2018 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Tuebingen/Reutlingen, Germany, 18–22 March 2018; pp. 565–566. [Google Scholar] [CrossRef]
- Hamzeheinejad, N.; Roth, D.; Götz, D.; Weilbach, F.; Latoschik, M.E. Physiological effectivity and user experience of immersive gait rehabilitation. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 1421–1429. [Google Scholar]
- Høeg, E.R.; Bruun-Pedersen, J.R.; Cheary, S.; Andersen, L.K.; Paisa, R.; Serafin, S.; Lange, B. Buddy biking: A user study on social collaboration in a virtual reality exergame for rehabilitation. Virtual Real. 2021, 27, 1–18. [Google Scholar] [CrossRef]
- Janeh, O.; Fründt, O.; Schönwald, B.; Gulberti, A.; Buhmann, C.; Gerloff, C.; Steinicke, F.; Pötter-Nerger, M. Gait Training in Virtual Reality: Short-Term Effects of Different Virtual Manipulation Techniques in Parkinson’s Disease. Cells 2019, 8, 419. [Google Scholar] [CrossRef] [PubMed]
- Kern, F.; Winter, C.; Gall, D.; Kathner, I.; Pauli, P.; Latoschik, M.E. Immersive Virtual Reality and Gamification Within Procedurally Generated Environments to Increase Motivation During Gait Rehabilitation. In Proceedings of the 26th IEEE Conference on Virtual Reality and 3D User Interfaces, VR 2019, Osaka, Japan, 25–29 March 2017; pp. 500–509. [Google Scholar] [CrossRef]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lubetzky, A.V.; Kelly, J.; Wang, Z.; Gospodarek, M.; Fu, G.; Sutera, J.; Hujsak, B.D. Contextual sensory integration training via head mounted display for individuals with vestibular disorders: A feasibility study. Disabil. Rehabil. Assist. Technol. 2020, 17, 74–84. [Google Scholar] [CrossRef]
- Lheureux, A.; LeBleu, J.; Frisque, C.; Sion, C.; Stoquart, G.; Warlop, T.; Detrembleur, C.; Lejeune, T. Immersive Virtual Reality to Restore Natural Long-Range Autocorrelations in Parkinson’s Disease Patients’ Gait During Treadmill Walking. Front. Physiol. 2020, 11, 572063. [Google Scholar] [CrossRef]
- Maeng, S.; Hong, J.P.; Kim, W.-H.; Kim, H.; Cho, S.-E.; Kang, J.M.; Na, K.-S.; Oh, S.-H.; Park, J.W.; Bae, J.N.; et al. Effects of Virtual Reality-Based Cognitive Training in the Elderly with and without Mild Cognitive Impairment. Psychiatry Investig. 2021, 18, 619–627. [Google Scholar] [CrossRef]
- Morizio, C.; Compagnat, M.; Boujut, A.; Labbani-Igbida, O.; Billot, M.; Perrochon, A. Immersive Virtual Reality during Robot-Assisted Gait Training: Validation of a New Device in Stroke Rehabilitation. Medicina 2022, 58, 1805. [Google Scholar] [CrossRef]
- Park, S.; Lee, G. Full-immersion virtual reality: Adverse effects related to static balance. Neurosci. Lett. 2020, 733, 134974. [Google Scholar] [CrossRef]
- Pot-Kolder, R.; Veling, W.; Counotte, J.; Van Der Gaag, M. Anxiety Partially Mediates Cybersickness Symptoms in Immersive Virtual Reality Environments. Cyberpsychology Behav. Soc. Netw. 2018, 21, 187–193. [Google Scholar] [CrossRef]
- Salgado, D.P.; Flynn, R.; Naves, E.L.M.; Murray, N. The Impact of Jerk on Quality of Experience and Cybersickness in an Immersive Wheelchair Application. In Proceedings of the 2020 Twelfth International Conference on Quality of Multimedia Experience, Athlone, Ireland, 26–28 May 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Saredakis, D.; Keage, H.A.; Corlis, M.; Loetscher, T. Using Virtual Reality to Improve Apathy in Residential Aged Care: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e17632. [Google Scholar] [CrossRef]
- Shah, S.H.H.; Karlsen, A.S.T.; Solberg, M.; Hameed, I.A. A social vr-based collaborative exergame for rehabilitation: Codesign, development and user study. Virtual Real. 2022, 1–18. [Google Scholar] [CrossRef]
- Tyrrell, R.; Sarig-Bahat, H.; Williams, K.; Williams, G.; Treleaven, J. Simulator sickness in patients with neck pain and vestibular pathology during virtual reality tasks. Virtual Real. 2017, 22, 211–219. [Google Scholar] [CrossRef]
- Vailland, G.; Devigne, L.; Pasteau, F.; Nouviale, F.; Fraudet, B.; Leblong, E.; Babel, M.; Gouranton, V. VR based Power Wheelchair Simulator: Usability Evaluation through a Clinically Validated Task with Regular Users. In Proceedings of the 2021 IEEE Virtual Reality and 3D User Interfaces, Lisbon, Portugal, 27 March–1 April 2021; pp. 420–427. [Google Scholar] [CrossRef]
- Vlake, J.H.B.; Wils, E.-J.M.; van Bommel, J.M.; Korevaar, T.I.M.M.; Gommers, D.M.; van Genderen, M.E.M. Virtual Reality Tailored to the Needs of Post-ICU Patients: A Safety and Immersiveness Study in Healthy Volunteers. Crit. Care Explor. 2021, 3, e0388. [Google Scholar] [CrossRef]
- Winter, C.; Kern, F.; Gall, D.; Latoschik, M.E.; Pauli, P.; Käthner, I. Immersive virtual reality during gait rehabilitation increases walking speed and motivation: A usability evaluation with healthy participants and patients with multiple sclerosis and stroke. J. Neuroeng. Rehabil. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Tallarida, R.J.; Murray, R.B.; Tallarida, R.J.; Murray, R.B. Chi-square test. Man. Pharmacol. Calc. Comput. Programs 1987, 140–142. [Google Scholar]
- Kennedy, R.; Drexler, J.; Compton, D.; Stanney, K.; Lanham, D.; Harm, D. Configural scoring of simulator sickness, cybersickness and space adaptation syndrome: Similarities and differences. Virtual Adapt. Environ. Appl. Implic. Hum. Perform. Issues 2003, 2003, 247. [Google Scholar]
- Dilanchian, A.T.; Andringa, R.; Boot, W.R. A Pilot Study Exploring Age Differences in Presence, Workload, and Cybersickness in the Experience of Immersive Virtual Reality Environments. Front. Virtual Real. 2021, 2, 736793. [Google Scholar] [CrossRef]
- Xu, W.; Liang, H.-N.; Yu, K.; Baghaei, N. Effect of gameplay uncertainty, display type, and age on virtual reality exergames. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; pp. 1–14. [Google Scholar]
- Pietrzak, E.; Pullman, S.; McGuire, A. Using Virtual Reality and Videogames for Traumatic Brain Injury Rehabilitation: A Structured Literature Review. Games Health J. 2014, 3, 202–214. [Google Scholar] [CrossRef]
- Rose, F.D.; Brooks, B.M.; Rizzo, A.A. Virtual Reality in Brain Damage Rehabilitation: Review. CyberPsychology Behav. 2005, 8, 241–262. [Google Scholar] [CrossRef]
- Patel, M.; Snyder, A.R.; Baham, M.; Sheridan, C.A.; Brown, A.; Asarnow, R.; Babikian, T.; Choe, M.; Giza, C. Brief Autonomic Assessment in Concussion Clinic. Neurology 2020, 95, S4–S5. [Google Scholar] [CrossRef]
- Huang, H.-M.; Rauch, U.; Liaw, S.-S. Investigating learners’ attitudes toward virtual reality learning environments: Based on a constructivist approach. Comput. Educ. 2010, 55, 1171–1182. [Google Scholar] [CrossRef]
- Moraes, T.M.; Zaninotto, A.L.; Neville, I.S.; Hayashi, C.Y.; Paiva, W.S. Immersive virtual reality in patients with moderate and severe traumatic brain injury: A feasibility study. Health Technol. 2021, 11, 1035–1044. [Google Scholar] [CrossRef]
- Coyle, H.; Traynor, V.; Solowij, N. Computerized and Virtual Reality Cognitive Training for Individuals at High Risk of Cognitive Decline: Systematic Review of the Literature. Am. J. Geriatr. Psychiatry 2014, 23, 335–359. [Google Scholar] [CrossRef] [PubMed]
- Cushman, L.A.; Stein, K.; Duffy, C.J. Detecting navigational deficits in cognitive aging and Alzheimer disease using virtual reality. Neurology 2008, 71, 888–895. [Google Scholar] [CrossRef]
- Tuena, C.; Serino, S.; Stramba-Badiale, C.; Pedroli, E.; Goulene, K.M.; Stramba-Badiale, M.; Riva, G. Usability of an Embodied CAVE System for Spatial Navigation Training in Mild Cognitive Impairment. J. Clin. Med. 2023, 12, 1949. [Google Scholar] [CrossRef]
- Mondellini, M.; Arlati, S.; Gapeyeva, H.; Lees, K.; Märitz, I.; Pizzagalli, S.L.; Otto, T.; Sacco, M.; Teder-Braschinsky, A. User Experience during an Immersive Virtual Reality-Based Cognitive Task: A Comparison between Estonian and Italian Older Adults with MCI. Sensors 2022, 22, 8249. [Google Scholar] [CrossRef]
- García-Muñoz, C.; Cortés-Vega, M.-D.; Heredia-Rizo, A.M.; Martín-Valero, R.; García-Bernal, M.-I.; Casuso-Holgado, M.J. Effectiveness of vestibular training for balance and dizziness rehabilitation in people with multiple sclerosis: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 590. [Google Scholar] [CrossRef]
- Norouzi-Gheidari, N.; Hernandez, A.; Archambault, P.S.; Higgins, J.; Poissant, L.; Kairy, D. Feasibility, Safety and Efficacy of a Virtual Reality Exergame System to Supplement Upper Extremity Rehabilitation Post-Stroke: A Pilot Randomized Clinical Trial and Proof of Principle. Int. J. Environ. Res. Public Health 2019, 17, 113. [Google Scholar] [CrossRef]
- Risi, D.; Palmisano, S. Effects of postural stability, active control, exposure duration and repeated exposures on HMD induced cybersickness. Displays 2019, 60, 9–17. [Google Scholar] [CrossRef]
- Servotte, J.-C.; Goosse, M.; Campbell, S.H.; Dardenne, N.; Pilote, B.; Simoneau, I.L.; Guillaume, M.; Bragard, I.; Ghuysen, A. Virtual reality experience: Immersion, sense of presence, and cybersickness. Clin. Simul. Nurs. 2020, 38, 35–43. [Google Scholar] [CrossRef]
- Chandra, A.N.R.; El Jamiy, F.; Reza, H. A Systematic Survey on Cybersickness in Virtual Environments. Computers 2022, 11, 51. [Google Scholar] [CrossRef]
- Saint-Aubert, J.; Cogné, M.; Bonan, I.; Launey, Y.; Lécuyer, A. Influence of user posture and virtual exercise on impression of locomotion during vr observation. IEEE Trans. Vis. Comput. Graph. 2022, 14, 8. [Google Scholar] [CrossRef]
- Mittelstaedt, J.; Wacker, J.; Stelling, D. Effects of display type and motion control on cybersickness in a virtual bike simulator. Displays 2018, 51, 43–50. [Google Scholar] [CrossRef]
- Petrigna, L.; Musumeci, G. The Metaverse: A New Challenge for the Healthcare System: A Scoping Review. J. Funct. Morphol. Kinesiol. 2022, 7, 63. [Google Scholar] [CrossRef]
- Yang, J.O.; Lee, J.S. Utilization exercise rehabilitation using metaverse (vr· ar· mr· xr). Korean J. Sport Biomech. 2021, 31, 249–258. [Google Scholar]
- Garavand, A.; Aslani, N. Metaverse phenomenon and its impact on health: A scoping review. Inform. Med. Unlocked 2022, 32, 101029. [Google Scholar] [CrossRef]
- Garrido, L.E.; Frías-Hiciano, M.; Moreno-Jiménez, M.; Cruz, G.N.; García-Batista, Z.E.; Guerra-Peña, K.; Medrano, L.A. Focusing on cybersickness: Pervasiveness, latent trajectories, susceptibility, and effects on the virtual reality experience. Virtual Real. 2022, 26, 1347–1371. [Google Scholar] [CrossRef]
- Stanney, K.; Lawson, B.D.; Rokers, B.; Dennison, M.; Fidopiastis, C.; Stoffregen, T.; Weech, S.; Fulvio, J.M. Identifying Causes of and Solutions for Cybersickness in Immersive Technology: Reformulation of a Research and Development Agenda. Int. J. Human-Comput. Interact. 2020, 36, 1783–1803. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Details |
|---|---|
| Nausea | General discomfort, increased salivation, sweating, nausea, difficulty concentrating, stomach awareness, burping |
| Oculomotor | General discomfort, fatigue, headache, eyestrain, difficulty focusing |
| Disorientation | Difficulty focusing, nausea, fullness of the head, blurred vision, dizzy (eyes open), dizzy (eyes closed) |
| No. | Author | N | M | F | Age | Symptom | Induce | Time | Content | Locomotion | Control | Display Type | Equipment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Arafat 2017 [18] | 16 | 3 | 13 | 37–67 M = 55 (9) | Cognitive impairment | YES | ≤15 | Exergame | Bicycling | Gesture-based | 360° Simulator, 3 DoF | Oculus Rift DK2 |
| 2 | Arlati 2021 [19] | 58 | 11 22 | 13 9 | M = 72.45 (5.83) M = 70.67 (5.62) | Cognitive impairment | YES | ≤15 | Exergame | Standing | Controller-based | 360° Simulator, 3 DoF | HTC Vive Pro |
| 3 | Bovim 2020 [20] | 29 | 6 | 23 | 19–40 M = 28.9 (4.8) | Physical inactivity | NO | ≤5 | Training | Walking | Controller-based | 360° Simulator, 6 DoF | HTC Vive |
| 4 | Brown 2021 [21] | 12 | 5 | 7 | 39–70 M = 56 (9.36) | Physical inactivity | YES | ≤5 | Exergame | Standing | Gesture-based | 360° Simulator, 3 DoF | Oculus Rift CV1 |
| 5 | Chen 2009 [22] | 30 | 14 | 16 | 27–70 M = 53 (2) | Physical inactivity | NO | ≤10 | Exergame | Walking | Controller-based | 360° Simulator, 6 DoF | - |
| 6 | Chowdhury 2019 [23] | 11 | 4 | 7 | M = 53.30 (4.87) | Physical inactivity | YES | ≤45 | Exergame | Sitting | Gesture-based | 360° Simulator, 3 DoF | HTC Vive |
| 7 | Ciaynska 2022 [24] | 45 | 23 | 22 | 19–28 M = 21.69 (2.76) | Physical inactivity | YES | ≤30 | Exergame | Standing | Controller-based | 360° Simulator, 3 DoF | Oculus Quest 1 |
| 8 | Ham 2018 [25] | 21 | 10 | 11 | 19–35 M = 24.19 (4.38) | Brain injuries | YES | n/a | Scene | Walking | Gaze-directed | 360° Simulator, 6 DoF | HTC Vive |
| 9 | Ham 2019 [26] | 45 | 23 | 22 | 19–26 M = 21.82 (1.84) | Physical inactivity | NO | ≤15 | Training | Walking | Gesture-based | 360° Simulator, 6 DoF | HTC Vive |
| 10 | Heg 2021 [27] | 11 | 7 | 4 | M = 60 (11) | Physical inactivity | YES | ≤15 | Scene | Bicycling | Controller-based | 360° Simulator, 3 DoF | Oculus Rift CV1 |
| 11 | Janeh 2019 [28] | 15 | 15 | 0 | M = 67.6 (7) | Brain injuries | YES | ≤20 | Training | Walking | Controller-based | 360° Simulator, 3 DoF | HTC Vive |
| 12 | Kern 2019 [29] | 36 | 20 | 16 | 19–30 M = 22.68 (2.64) | Physical inactivity | YES | ≤15 | Training | Walking | Gaze-directed | 360° Simulator, 6 DoF | HTC Vive |
| 13 | Kim 2017 [30] | 33 | 5 3 3 | 6 8 8 | M = 28 (7) M = 66 (3) M = 65 (7) | Brain injuries | YES | ≤30 | Training | Walking | Gaze-directed | 360° Simulator, 6 DoF | Oculus Rift DK2 |
| 14 | Lhbetzky 2020 [31] | 15 | 10 | 5 | M = 57 (13.5) | Brain injuries | YES | ≤20 | Exergame | Walking | Gaze-directed | 360° Simulator, 3 DoF | HTC Vive |
| 15 | Lheureux 2020 [32] | 10 | 6 | 4 | M = 63.7 (10.6) | Brain injuries | YES | ≤15 | Training | Walking | - | 360° Simulator, 3 DoF | HTC Vive |
| 16 | Maeng 2021 [33] | 31 25 | 8 3 | 23 22 | M = 73.2 (7.3) M = 71.6 (4.4) | Cognitive impairment | YES | ≤30 | Exergame | Standing | Controller-based | 360° Simulator, 6 DoF | Samsung HMD Odyssey |
| 17 | Morizio 2022 [34] | 38 | 18 | 20 | 19–53 M = 25.2 (8.4) | Brain injuries | NO | ≤20 | Video | Walking | Gaze-directed | 360° Simulator, 3 DoF | HTC Vive |
| 18 | Park 2020 [35] | 15 | 6 | 9 | M = 22.60 (1.06) | Cognitive impairment | YES | ≤15 | Exergame | Standing | Gesture-based | 360° Simulator, 3 DoF | PlayStation® VR headset |
| 19 | Pot-Kolder 2018 [36] | 170 | 97 | 73 | 18–35 M = 25.4 (4.6) | Cognitive impairment | YES | ≤20 | Video | Standing | Gaze-directed | 360° Simulator, 3 DoF | Sony HMZ-T1 |
| 20 | Salgado 2020 [37] | 33 | 10 8 | 7 8 | M = 30.29 (1.77) M = 30.12 (3.17) | Physical inactivity | YES | ≤15 | Training | Sitting | Controller-based | 360° Simulator, 6 DoF | Oculus Rift DK2 |
| 21 | Saredakis 2020 [38] | 17 | 7 | 10 | 72–95 M = 87.3 (6.3) | Cognitive impairment | YES | ≤20 | Video | Sitting | Gaze-directed | 360° Simulator, 3 DoF | Oculus Go |
| 22 | Shah 2022 [39] | 14 | 7 | 7 | 60–88 M = 77.57 (7.08) | Physical inactivity | NO | ≤15 | Exergame | Standing | Gesture-based | 360° Simulator, 3 DoF | Oculus Quest 1 |
| 23 | Tyrrell 2017 [40] | 20 14 20 | 6 11 11 | 14 8 9 | M = 47.15 (11.6) M = 49.64 (13.2) M = 46.5 (12) | Cognitive impairment | YES | ≤30 | Video | Sitting | Gaze-directed | 360° Simulator, 3 DoF | Oculus Rift DK2 |
| 24 | Vailland 2021 [41] | 29 | - | - | M = 65 | Physical inactivity | YES | n/a | Training | Sitting | Controller-based | 360° Simulator, 6 DoF | HTC Vive Pro |
| 25 | Vlake 2021 [42] | 15 | 4 | 11 | 45–65 M = 54 | Cognitive impairment | NO | ≤15 | Video | Sitting | - | 360° Simulator, 3 DoF | - |
| 26 | Winter 2021 [43] | 14 | - | - | M = 52.6 (7.5) | Physical inactivity | YES | ≤15 | Exergame | Walking | Gaze-directed | 360° Simulator, 6 DoF | HTC Vive |
| No. | Author | Measures | Groups | Total SSQ (SD) | Nausea (SD) | Oculomotor (SD) | Disorientation (SD) | Objectives | Results |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Arafat 2017 [18] | MS, GSR, MSSQ, SSQ | Pre Post | 13.090 (12.251) 33.125 (31.730) | 10.221 (9.513) 29.301 (29.096) | 14.618 (15.581) 27.071 (22.781) | 6.960 (11.899) 33.805 (43.922) | How persons with sclerosis experience cybersickness. | Virtual environment-induced cybersickness. |
| 2 | Arlati 2021 [19] | SSQ, ITC-SOPI, TAM3 | MCI SCD | 3.74 (9.35) 11.22 (18.70) | 0 (9.54) 0 (9.54) | 0 (9.48) 7.58 (18.95) | 0 (13.92) 13.92 (27.84) | Evaluating the acceptance and usability of VR environment. | Immersive VR was acceptable and enjoyable for older adults. |
| 3 | Bovim 2020 [20] | SSQ, DT | Pre Post | 18.2 (22.4) 12.4 (14.6) | 11.8 (20.8) 11.3 (16.4) | 17.5 (19.1) 6.7 (13.4) | 18.4 (26.9) 7.2 (14.5) | Investigating the impact of constraints on gait during treadmill walking in VE. | VE training on a treadmill improved gait and balance control. |
| 4 | Brown 2021 [21] | SSQ | Pre Post | 10.29 (11.44) 19.39 (6.19) | 15.105 (13.184) 23.055 (11.327) | 18.318 (19.439) 25.267 (18.908) | 2.32 (7.695) 12.76 (34.781) | Investigating cybersickness baseline recordings among a chronic pain population. | Significant differences were found. |
| 5 | Chen 2009 [22] | AD-ACL, SSQ | Pre Post | 10.54 (9.58) 11.59 (6.47) | 14.74 (11.58) 13.36 (11.20) | 7.52 (10.17) 6.82 (7.54) | 15.19 (24.47) 18.10 (20.80) | Investigating the psychological benefits of VR in rehabilitation. | There were no significant differences between the VR and non-VR groups. |
| 6 | Chowdhury 2019 [23] | EDSS, SSQ | Pre Post | 13.352 (16.845) 36.876 (12.297) | 8.204 (8.586) 25.853 (10.618) | 16.221 (24.142) 38.961 (19.784) | 7.934 (10.955) 27.84 (11.359) | Investigating a concept called Virtual Ability Simulation (VAS) for people with disability. | VAS enabled participants to perceive the difficulty of the same task more easily. |
| 7 | Ciaynska 2022 [24] | SSQ, BioHarness 3.0 | Before After | 13.65 (10.68) (M) 15.47 (11.41) (F) 15.13 (16.60) (M) 32.98 (17.30) (F) | 10.37 (9.22) (M) 9.54 (9.74) (F) 22.40 (12.87) (M) 20.38 (13.05) (F) | 14.5 (12.25) (M) 18.26 (14.18) (F) 21.09 (15.33) (M) 34.11 (18.80) (F) | 7.87 (10.05) (M) 11.39 (11.42) (F) 15.13 (10.65) (M) 24.68 (22.80) (F) | Examining the differences in the effects of VR 3D HMD gaming on genders. | Significant differences between genders were observed. |
| 8 | Ham 2018 [25] | IMI, NASA-TLX, UEQ, SSQ | Pre Post | 23.69 (29.76) 33.30 (36.54) | - | - | - | Presenting an immersive VR system for gait rehabilitation after neurological impairments. | The results demonstrated an encouraging user experience and acceptance. |
| 9 | Ham 2019 [26] | SSQ, NASA-TLX, IMI, UEQ | Day 1 Day 3 | 2.89 (3.26) 5.86 (1.59) | - | - | - | Introducing an immersive VR system for gait rehabilitation. | Figuring out the requirements, such as enhancing social communication, interactivity. |
| 10 | Heg 2021 [27] | SSQ, SUS, IMI, VEQ, IPI | Pre-test Post-test | 4.8 (3.8) 14.5 (9.2) | 6.1 (9.8) 25.4 (16.1) | 4.1 (5.2) 11.8 (11.3) | 5.1 (9.4) 9.3 (13.6) | Encouraging player collaboration on a virtual tandem bike. | Nearly all participants would like to use the system again. |
| 11 | Janeh 2019 [28] | MoCA, SSQ, SUS, PDQ-39 | Pre Post | 16.45 (16.59) 15.21 (17.04) | - | - | - | Finding a VR-based gait manipulation strategy to improve gait symmetry. | Providing rehabilitative training strategies to achieve gait symmetry and prevent FOG. |
| 12 | Kern 2019 [29] | SSQ, SAM, IMI, RTLX, UEQ, USEQ, STAI | Pre Post | 21.19 (20.87) 14.23 (15.45) | 15.63 (16.15) 15.10 (14.49) | 21.68 (20.59) 12.42 (16.32) | 16.23 (27.54) 11.21 (16.57) | Using VR to enhance motivation during gait rehabilitation. | Providing critical content features in gait rehabilitation. |
| 13 | Kim 2017 [30] | Mini-BESTest, CoP, SSQ | Healthy young Healthy old Parkinson’s disease | 8.3 (10.5) 6.5 (13.0) 27.5 (22.5) | 5.8 (7.4) 6.1 (11.2) 20.8 (18.3) | 10.2 (12.4) 12.1 (13.2) 21.5 (16.6) | 6.5 (13.6) 4.4 (12.4) 28.5 (29.3) | Evaluating the safety of using an HMD for longer bouts of walking. | Older adults with PD were able to use immersive VR during walking without adverse effects. |
| 14 | Lhbetzky 2020 [31] | VVAS, DHI, ABC, FSST | (VM) Pre (VM) Post (mTBI) Pre (mTBI) Post | 4.75 (4.22) 4.17 (5.06) 13 (11.3) 18.5 (13.4) | - | - | - | Testing the feasibility of a novel VR application (app) for patients with vestibular disorders. | HMD training appeared to be a promising adjunct modality for vestibular rehabilitation. |
| 15 | Lheureux 2020 [32] | SSQ | TW (Pre) iVRTW (Post) | 15.0 (19.7) 16.8 (14.8) | 11.5 (12.6) 17.2 (11.7) | 12.1 (15.7) 15.9 (17.7) | 16.7 (29.2) 8.4 (9.7) | Comparing PD gait during different conditions. | iVRTW could enhance the effectiveness of TW. |
| 16 | Maeng 2021 [33] | CERAD-K, KQOL-AD, GDS, SSQ | Normal group MCI group | 16.45 (24.42) 19.90 (29.45) | 10.30 (17.61) 14.46 (21.17) | 26.16 (37.76) 32.33 (46.91) | 10.91 (17.10) 11.24 (19.26) | Introducing a virtual reality-based cognitive training (VRCT) program. | Both groups showed a reduction in discomfort as the VRCT program progressed. |
| 17 | Morizio 2022 [34] | SSQ, PQ, SUS | Pre Sess 1 Post Sess 1 Pre Sess 2 Post Sess 2 | 1.31 (2.53) 3.33 (6.98) 0.80 (2.00) 2.32 (5.53) | - | - | - | Assessing the onset of cybersickness in the health before testing in stroke patients. | The usage of this VR device for gait rehabilitation did not lead to cybersickness. |
| 18 | Park 2020 [35] | VRSQ, SSQ | Fixed Moving | 7.98 (11.03) 24.43 (28.62) | - | - | - | Investigating how full-immersion VR games cause changes. | Paying a VR game had negative effects on static balance. |
| 19 | Pot-Kolder 2018 [36] | SSQ, SUD | Pre Post | 32.7 (37.7) 46.7 (38.7) | 23.3 (29.2) 40.3 (36.1) | 32.7 (33.3) 33.3 (30.6) | 27.8 (46.5) 54.0 (51.9) | Investigating the relationship between VR and CS. | CS is expected to decline during treatment. |
| 20 | Salgado 2020 [37] | QoE, SSQ, SCR, IBI, HRV | Low (Pre) High (Post) | 2.8 (11.2) 16.28 (27.4) | 7.75 (16.0) 13.47 (23.6) | −2.36 (12.0) 9.8 (24.4) | 2.39 (9.54) 15.71 (21.0) | Presenting a QoE and cybersickness study of wheelchair training simulator. | Simulator with low jerk effect reduced simulator sickness symptoms. |
| 21 | Saredakis 2020 [38] | AES, SSQ | Pre Post | 12.22 (13.07) 13.46 (11.38) | 15.90 (15.99) 17.17 (17.74) | 18.70 (21.98) 20.72 (20.75) | 7.42 (15.67) 12.06 (14.76) | Assessing whether VR using HMDs could be used to deliver tailored reminiscence therapy. | It is feasible to use VR for therapy to treat symptoms of apathy in older adults. |
| 22 | Shah 2022 [39] | SUS, SSQ, GEQ, IMI, VEQ | Pre-test Post-test Change Score | 9.08 (11.19) 14.43 (11.29) 5.34 (6.74) | 4.77 (10.66) 17.71 (15.23) 12.94 (12.28) | 9.75 (10.88) 9.75 (9.25) 0 (4.96) | 8.95 (14.51) 9.94 (14.34) 0.99 (3.58) | Motivating elderly individuals to participate in physical exercise and social connectedness. | The participants found the social VR gameplay enjoyable. |
| 23 | Tyrrell 2017 [40] | NDI, VSS, VAS, DHI, SS-VAS, SSQ | Control Neck pain Vestibular | 21.88 (29.7) 43.20 (31.5) 49.42 (33.4) | 24.33 (30.9) 32.91 (29.3) 40.89 (23.5) | 12.13 (17.8) 34.11 (21.7) 31.40 (27.1) | 23.66 (37.0) 50.11 (46.2) 66.62 (49.5) | This was a cross-sectional, observational study with three populations sought. | Neck pain and vestibular pathology similarly increased rating of SS. |
| 24 | Vailland 2021 [41] | SSQ, USE, IPQ | Pre Post | 20.44 (22.45) 25.58 (25.52) | 13.63 (16.3) 20.61 (25.49) | 20.84 (22.84) 20.62 (22.48) | 17.9 (25.09) 27.28 (34.69) | Developing a virtual reality-based power wheelchair simulator. | The simulator provoked only slight to moderate cybersickness discomforts. |
| 25 | Vlake 2021 [42] | SSQ, IPQ | 2D Group VR Group | 0.9 (0.3) 3.7 (2.1) | 0.9 (0.5) 1.8 (3.8) | 0.1 (0.1) 2.1 (1.2) | 0.1 (0.1) 2.3 (5.3) | To describe and evaluate the safety and immersiveness of an ICU-specific VR module. | ICU-VR is safe and more immersive than 2D. |
| 26 | Winter 2021 [43] | IPQ, SSQ, RTLX, SUS | Pre Post | 13.19 (13.34) 17.04 (18.46) | 10.34 (11.49) 15.37 (11.47) | 12.63 (14.61) 12.84 (19.58) | 10.83 (17.00) 17.40 (26.07) | Comparison for VR via HMD, VR via monitor, treadmill training without VR. | Study demonstrated the feasibility of combining treadmill training with VR. |
| Total SSQ Score | Nausea | Oculomotor | Disorientation | |
|---|---|---|---|---|
| Age | Q-value = 0.362 | Q-value = 6.103 | Q-value = 8.870 | Q-value = 1.045 |
| p = 0.835 | p = 0.107 | p = 0.031 | p = 0.790 | |
| Symptom | Q-value = 6.628 | Q-value = 8.472 | Q-value = 8.552 | Q-value = 10.724 |
| p = 0.036 | p = 0.037 | p = 0.014 | p = 0.005 | |
| Inducement | Q-value = 0.744 | Q-value = 6.602 | Q-value = 10.284 | Q-value = 14.920 |
| p = 0.388 | p = 0.037 | p = 0.001 | p = 0.000 | |
| Time | Q-value = 10.181 | Q-value = 14.032 | Q-value = 7.160 | Q-value = 18.070 |
| p = 0.017 | p = 0.003 | p = 0.067 | p = 0.000 | |
| Content | Q-value = 9.594 | Q-value = 12.536 | Q-value = 7.990 | Q-value = 26.937 |
| p = 0.048 | p = 0.014 | p = 0.018 | p = 0.000 | |
| Locomotion | Q-value = 7.864 | Q-value = 9.355 | Q-value = 7.340 | Q-value = 8.396 |
| p = 0.020 | p = 0.053 | p = 0.059 | p = 0.015 | |
| Control | Q-value = 21.936 | Q-value = 14.530 | Q-value = 3.726 | Q-value = 9.222 |
| p = 0.000 | p = 0.002 | p = 0.293 | p = 0.026 | |
| Display type | Q-value = 7.660 | Q-value = 21.058 | Q-value = 16.903 | Q-value = 31.741 |
| p = 0.006 | p = 0.000 | p = 0.000 | p = 0.000 |
| Attribute | Total SSQ | |||
|---|---|---|---|---|
| n | % | Mean | 95% CI | |
| Age | ||||
| 0–30 | 8 | 30.7 | 20.508 | [13.086, 27.931] |
| 30–60 | 9 | 34.6 | 20.853 | [14.138, 27.569] |
| Above 60 | 8 | 30.7 | 16.036 | [12.699, 19.372] |
| Symptom | ||||
| Brain injuries | 7 | 26.9 | 21.058 | [15.357, 26.760] |
| Cognitive impairment | 7 | 26.9 | 19.242 | [11.294, 27.189] |
| Physical inactivity | 12 | 46.2 | 18.156 | [12.778, 23.534] |
| Inducement | ||||
| YES | 19 | 73.1 | 19.430 | [15.678, 23.181] |
| NO | 7 | 26.9 | 8.519 | [5.599, 11.438] |
| Time | ||||
| 0–10 min | 3 | 11.5 | 14.474 | [9.165, 19.784] |
| 10–20 min | 16 | 61.5 | 15.695 | [11.559, 19.830] |
| Above 20 min | 5 | 19.2 | 26.862 | [13.883, 39.841] |
| Content | ||||
| Exergame | 11 | 42.3 | 21.090 | [15.695, 26.484] |
| Training | 8 | 30.7 | 16.258 | [10.063, 22.453] |
| Video | 4 | 15.4 | 35.964 | [15.833, 56.095] |
| Scene | 3 | 11.6 | 14.446 | [6.548, 22.345] |
| Locomotion | ||||
| Sitting | 6 | 23.1 | 23.044 | [10.847, 35.240] |
| Standing | 7 | 26.9 | 24.122 | [14.779, 33.464] |
| Walking | 11 | 42.3 | 13.686 | [10.173, 17.199] |
| Bicycling | 2 | 7.7 | 22.330 | [14.310, 30.349] |
| Control | ||||
| Controller-based | 9 | 34.6 | 17.537 | [12.274, 22.800] |
| Gesture-based | 6 | 23.1 | 21.451 | [11.341, 31.562] |
| Gaze-directed | 9 | 34.6 | 23.953 | [12.580, 35.326] |
| Display Type | ||||
| 3 DoF | 16 | 61.5 | 21.307 | [14.402, 28.213] |
| 6 DoF | 10 | 38.5 | 19.114 | [14.7005, 23.523] |
| All studies | 26 | 100 | 19.430 | [15.678, 23.181] |
| Attribute | n (%) | Nausea | Oculomotor | Disorientation | |||
|---|---|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | ||
| Age | |||||||
| 0–30 | 5 (25) | 20.212 | [15.977, 24.447] | 14.222 | [8.583, 19.862] | 25.868 | [15.636, 36.101] |
| 30–60 | 8 (40) | 19.918 | [14.020, 25.816] | 17.143 | [11.752, 22.533] | 20.765 | [9.722, 31.807] |
| Above 60 | 6 (30) | 12.806 | [8.683, 16.929] | 15.859 | [12.802, 18.915] | 15.527 | [10.389, 20.665] |
| Symptom | |||||||
| Brain injuries | 2 (10) | 15.543 | [10.253, 20.833] | 22.216 | [17.006, 27.426] | 25.111 | [14.646, 35.575] |
| Cognitive impairment | 7 (35) | 22.651 | [14.995, 30.306] | 24.051 | [15.766, 32.336] | 26.615 | [10.778, 42.452] |
| Physical inactivity | 11 (55) | 17.014 | [14.225, 19.803] | 13.333 | [7.970, 18.696] | 18.174 | [14.046, 22.302] |
| Inducement | |||||||
| YES | 16 (80) | 20.429 | [13.553, 27.306] | 19.366 | [13.124, 25.609] | 23.395 | [16.733, 30.056] |
| NO | 4 (20) | 9.597 | [5.295, 13.900] | 6.136 | [3.138, 9.134] | 11.602 | [5.156, 18.048] |
| Time | |||||||
| 0–10 min | 3 (15) | 17.834 | [12.723, 22.946] | 10.842 | [5.741, 15.943] | 17.757 | [12.083, 23.430] |
| 10–20 min | 11 (55) | 15.871 | [10.636, 21.107] | 12.828 | [5.655, 20.001] | 17.779 | [8.491, 27.049] |
| Above 20 min | 5 (25) | 24.701 | [20.793, 28.610] | 24.558 | [19.764, 29.351] | 27.633 | [19.786, 35.480] |
| Content | |||||||
| Exergame | 9 (45) | 16.209 | [11.132, 21.286] | 18.204 | [11.981, 24.428] | 18.992 | [14.131, 23.852] |
| Training | 6 (30) | 16.009 | [13.015, 19.002] | 12.121 | [6.825, 17.417] | 19.866 | [15.226, 24.507] |
| Video | 4 (20) | 32.671 | [20.795, 44,546] | 21.590 | [10.274, 32.907] | 31.916 | [12.709, 51.123] |
| Locomotion | |||||||
| Sitting | 6 (30) | 19.449 | [11.394, 27.504] | 17.452 | [10.191, 24.712] | 21.809 | [9.512, 34.106] |
| Standing | 6 (30) | 21.466 | [15.633, 27.299] | 20.162 | [10.883, 29.441] | 22.378 | [12.316, 32.440] |
| Walking | 6 (30) | 15.077 | [12.680, 17.475] | 13.443 | [7.806, 19.080] | 19.384 | [15.276, 23.491] |
| Bicycling | 2 (10) | 21.491 | [14.254, 28.727] | 15.803 | [10.315, 31.921] | 19.435 | [10.218, 27.089] |
| Control | |||||||
| Controller-based | 8 (40) | 13.000 | [8.309, 17.691] | 10.591 | [4.771, 16.410] | 17.572 | [13.724, 21.421] |
| Gesture-based | 4 (20) | 21.888 | [15.095, 28.681] | 24.669 | [10.800, 38.538] | 20.369 | [8.010, 32.727] |
| Gaze-directed | 5 (25) | 21.820 | [11.675, 31.966] | 19.530 | [9.979, 29.081] | 30.953 | [14.490, 47.416] |
| Display Type | |||||||
| 3 DoF | 12 (60) | 19.964 | [12.113, 27.814] | 19.264 | [12.019, 26.509] | 22.301 | [12.089, 32.513] |
| 6 DoF | 7 (35) | 14.722 | [12.084, 17.360] | 12.133 | [6.164, 18.102] | 17.781 | [14.277, 21.286] |
| All studies | 20 (100) | 17.834 | [12.723, 22.946] | 16.365 | [11.512, 21.218] | 21.096 | [14.059, 28.133] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Luh, D.-B.; Xu, R.-H.; An, Y. Considering the Consequences of Cybersickness in Immersive Virtual Reality Rehabilitation: A Systematic Review and Meta-Analysis. Appl. Sci. 2023, 13, 5159. https://doi.org/10.3390/app13085159
Li X, Luh D-B, Xu R-H, An Y. Considering the Consequences of Cybersickness in Immersive Virtual Reality Rehabilitation: A Systematic Review and Meta-Analysis. Applied Sciences. 2023; 13(8):5159. https://doi.org/10.3390/app13085159
Chicago/Turabian StyleLi, Xin, Ding-Bang Luh, Ruo-Hui Xu, and Yi An. 2023. "Considering the Consequences of Cybersickness in Immersive Virtual Reality Rehabilitation: A Systematic Review and Meta-Analysis" Applied Sciences 13, no. 8: 5159. https://doi.org/10.3390/app13085159
APA StyleLi, X., Luh, D.-B., Xu, R.-H., & An, Y. (2023). Considering the Consequences of Cybersickness in Immersive Virtual Reality Rehabilitation: A Systematic Review and Meta-Analysis. Applied Sciences, 13(8), 5159. https://doi.org/10.3390/app13085159