Abstract
Background: The aim of this study was to identify variations in the origins of the anterior branches of the external carotid artery (ECA) and to propose an update of the current classification. Methods: The study included 100 carotids arteries from fifty human donors. Classification of anterior branches of external carotid artery was performed according to Vaz’quez et al. (2009). Results: The configuration origins of anterior branches were found as follows: Type I, 82%; Type II, 1%; Type III, 16%. No Type IV was observed. The study identified seven subgroups of anterior branch variations in the external carotid artery. The most frequently observed variations were Subtype Ia in 40% (n = 20) of cases on the right side and Subtype Ib in 38% (n = 19) on the left side. In addition, a rare and previously unclassified configuration was observed in a 72-year-old male donor, where the carotid artery was pentafurcated on the left side. Conclusions: In conclusion, the presence of anatomical variants not previously included in the anterior external carotid artery branching classifications supports the consideration of a revision to the present classification system.
1. Introduction
Anatomy is the basis of any surgical, therapeutic and diagnostic procedure. Knowledge of the operative field is essential for the planning of any medical procedure. The main source of arterial supply to the head and neck regions is the common carotid artery (CCA). The CCA meets the carotid bifurcation (CB) at the level of the superior border of the thyroid cartilage [1], and then divides into the internal carotid artery (ICA) and external carotid artery (ECA). The ECA and its branches provide blood supply to the meninges, scalp, and face. Anterior branches of the ECA, including the superior thyroid artery (STA), lingual artery (LA), and facial artery (FA), arise from the ECA, following the CB. The complex anatomy of the ECA and its branches can pose a challenge, especially in radiology and surgery of the head and neck [2,3,4]. The risk of iatrogenic injury during surgical procedures increases when there is a lack of knowledge and experience in identifying the precise location and course of anterior branches of the ECA [5]. This is further compounded by variability of the anatomy of these blood vessels, making it easy to confuse one vessel for another one [6].
Two different classifications have been proposed for anterior branches of the ECA. Natsis et al. (2011) and Ozgur et al. (2008) classified them into four types based on origins of the STA, LA, and FA [7,8]. Type I is applied when they originate from separate branches, Type II is applied when STA and LA share a common thyrolingual trunk, Type III is applied when LA and FA share a common linguofacial trunk (LFT), and Type IV is applied when they originate from a common thyrolinguofacial trunk. On the other hand, Vazquez et al. (2009) divided the classification into three subtypes based on the origins of STA: (a) from the carotid bifurcation (50.2%); (b) from the common carotid artery (26.6%); (c) from the external carotid artery (23.2%) [9]. Several authors have already described variabilities in the anatomy of the ECA anterior branches (STA, LA, and FA) [1,2,3,4,6,8,10,11,12,13,14]. Natsis et al. (2011) and Zümre et al. (2005) have reported variations in the forms of the LFT, thyrolingual trunk (TLT), and thyrolinguofacial trunk (TLFT) [6,7]. Additionally, several studies have reported different origins for these branches, such as those arising from other carotid arteries or originating from the carotid arterial tree in combination with other arterial trunks [15,16,17,18]. Due to the heterogeneous nature and wide variability of the ECA and its branches, they are clinically significant in radiology and surgery procedures in the neck region [2,3,4,7,8,19].
The purpose of the anatomic dissections performed in this study was to examine various configurations of the origin of anterior branches of the ECA and to suggest a revision to the classification system to include anatomical variations. The findings of this study, along with a review of the literature, were used to develop this updated classification model.
2. Materials and Methods
A group of fifty human donors (100 heminecks) was studied as part of an anatomy dissecting course for students of oral and maxillofacial surgery of the Sapienza University of Rome at the International Cadaver Lab Organization Teaching and Research center in Verona, Italy. The donated bodies used in the study were obtained from individuals who had given their informed consent for the use of their body for educational and scientific purposes after death. The preservation method used for each specimen involved fresh freezing at −20 °C, without the use of formalin fixation solution. Visualization of the vascular patterns was achieved through the use of vascular injection fluid (latex). The sample consisted of 38 male and 12 female cadavers, with ages ranging from 60 to 98 years. Although a detailed clinical history was available, there was no indication of any vascular surgical intervention. During the anatomy dissecting course, the common, external, and internal carotid arteries were dissected on both sides of the donor. The neurovascular fascicle was exposed by lifting up the sternocleidomastoid muscle. Each carotid artery was dissected from the carotid sheath in a preparatory way, with the didactic purpose of highlighting the course of the main vascular structures that flow into the oral cavity from the latero-cervical tract of the neck (Figure 1). Particular attention was given to the anatomical pathway of ECA’s anterior branches observed in each specimen and on each side in order to properly classify the specific type described by Vazquez e al. (2009). Data on type, side, and sex at birth were collected in a table for descriptive analysis.
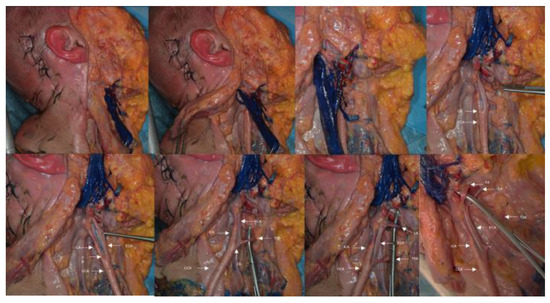
Figure 1.
Didactic dissection aimed at highlighting the anterior branches of the external carotid artery.
3. Results
The study investigated the branching patterns of carotid arteries in fifty cadavers, totaling 100 carotid arteries. The anterior branch variants of the ECA were classified into ten subgroups based on Vazquez et al.’s (2009) classification (Ia, Ib, and Ic; IIa, IIb, and IIc; IIIa, IIIb, IIIc, and IV), and the observed variants are recorded in Table 1 and described as follows: The most common grouping observed was Type I, where the STA, LA, and FA originated from separate branches, as depicted in Figure 2. This grouping was seen in 58.33% (n = 14) of the female patients and 89.47% (n = 68) of the male patients. When they were classified according to sides, type Ia was the most common on the right side at 40% (n = 20), while type Ib was the most common on the left side at 36% (n = 19).

Figure 2.
Type I: STA, LA, and FA originate from separate branches.
The type II group (TLT) (Figure 3) was found once only on the left side of a female donor, and the sample was assigned to subgroup a (Type IIa).
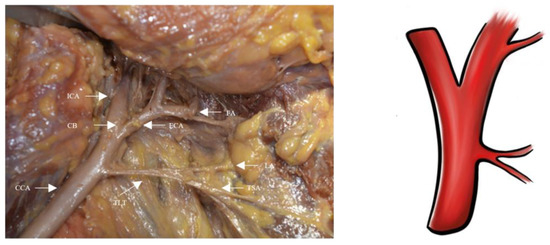
Figure 3.
Type II: STA and LA have a common thyrolingual trunk (TLT).
The study found that the type III group, in which the LA and FA share a common LFT (Figure 4), was present in 37.5% of female patients and 9.1% of male patients. In consideration of the subgroups within type III, type IIIa was found as often on both sides, with 12% prevalence, while type IIIb was not found, and type IIIc was only found on the left side, with a prevalence of 6%.
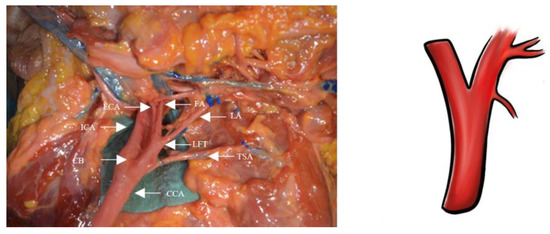
Figure 4.
Type III: LA and FA share a common linguofacial trunk (LFT).
No variant with TLFT was found in the group observed (Type IV). Moreover, we found a rare, unclassified configuration of a pentafurcated carotid artery on the left side of a male, 72-year-old donor. This finding was published as a “case report” by the authors in 2022 [20]. The authors observed that the STA, LA, and FA originated directly from the CCA at its terminal ramus just before the carotid bifurcation (CB), as shown in Figure 5.

Figure 5.
Pentafurcated carotid artery: STA, LA, and FA detached directly from the CCA at the terminal ramus just before the carotid bifurcation.
Figure 5.
Pentafurcated carotid artery: STA, LA, and FA detached directly from the CCA at the terminal ramus just before the carotid bifurcation.


Table 1.
Anterior branch variants of the ECA by sides and sex.
Table 1.
Anterior branch variants of the ECA by sides and sex.
| Variation Type | Right n (%) (n = 50) | Left n (%) (n = 50) | Female n (%) (n = 24) | Male n (%) (n = 76) | Total n (%) (n = 100) | |
|---|---|---|---|---|---|---|
| Ia | 20 (40) | 18 (36) | Type I | 14 (58.33) | 68 (89.47) | 82 (82) |
| Ib | 14 (28) | 19 (38) | ||||
| Ic | 7 (14) | 4 (8) | ||||
| IIa | - | 1 (2) | Type II | 1 (4.16) | - | 1 (1) |
| IIb | - | - | ||||
| IIc | - | - | ||||
| IIIa | 6 (12) | 6 (12) | Type III | 9 (37.5) | 7 (9.21) | 16 (16) |
| IIIb | - | 1 (2) | ||||
| IIIc | 3 (6) | - | ||||
| IV | - | - | - | - | - | |
| Unclassified | - | 1 (2) | Unclassified | - | 1 (1.32) | 1 (1) |
4. Discussion
Understanding variations in the origins and locations of branches of the ECA can help to guide surgeons in planning and performing neck surgeries, as these branches serve as important landmarks for adequate exposure and dissection of the carotid artery. Therefore, knowledge of these variations can help to minimize the risk of complications during surgical procedures in the neck region.
Understanding the prevalence and existence of anatomical variations is crucial, particularly for oral and oncologic procedures that may require ligation of the LA or TLT to prevent excessive bleeding.
As compared to the existing literature, our study’s findings showed that the Type I configuration was the most common variation (82%), which is consistent with previous studies by Herrera-Núñez et al. (2020), Devadas et al. (2018) and Zümre et al. (2005) [2,4,10]. Authors of reports, however, have reported both a higher prevalence (90%) and a lower (65%) prevalence of this variation (Özgür et al. (2008) and Shintani et al. (1999), respectively) [8,19]. The prevalence of a common trunk arising from the anterior ECA branches also varies significantly in the literature [4,7].
Previous studies have reported that type II (TLT) occurs in 1 to 3% of cases [3,5,6,7,8,21,22,23,24,25]. In our study, we also observed a prevalence of 1%, which is consistent with the literature.
Previous studies have described type III (LFT) as the most common variation in the common trunk, with an incidence ranging from 7.5% to 31% [3,4,7,8,18,20,24]. In our study, we observed a 16% incidence of type III, which is similar to the findings reported by other studies such as those of Devadas et al. (2018) (20%), Ito et al. (2006) (19.9%), and Zümre et al. (2005) (20%) [2,21,26].
Unfortunately, we did not find any TLFTs (Type IV). According to the literature, this is the rarest configuration of the variations described by Vaz’quez [2,4,6,7,27].
We encountered a unique instance of carotid artery branching that was not covered by existing classification systems. Specifically, we observed pentafurcation, in which the superior thyroid artery (STA), the lingual artery (LA), and the facial artery (FA) arose directly from the common carotid artery (CCA) just prior to the carotid bifurcation (CB) (Figure 4 and Figure 5).
Based on the discovery of this unique branching pattern, it may be appropriate to consider updating the current classification system. We propose adding a new subtype for each type of configuration, in which all the anterior branches (STA, LA, and FA) arise directly from the common carotid artery before the carotid bifurcation (CB). Additionally, Kaneko et al. (1996) previously reported a similar configuration in which the LA and FA originated as a common trunk (LFT) before the CB [28]. These findings support the introduction of a new subgroup for each type of configuration: Subtype Id for configurations in which STA, LA, and FA arise as separate branches before the CB, Subtype IId for configurations in which the TLT and FA originate before the CB, Subtype IIId for configurations in which STA and LFT originate before the CB, and Subtype IVb for configurations in which the TLFT originates before the CB. To aid in the understanding of these different anatomical types, including our proposed update, we have provided original illustrations in Figure 6.
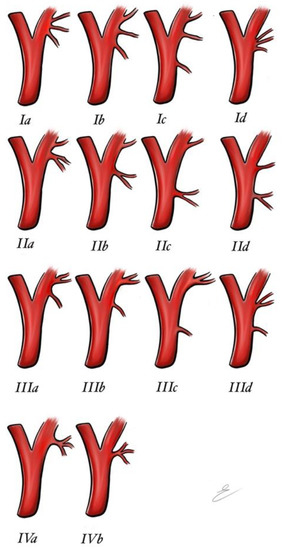
Figure 6.
Anterior branch variant classification updated with a new subtype for each type.
Updating the current anatomical classifications will allow the comparison of results of researchers from all over the world revising the incidence of variations.
Revising and updating the current anatomical classifications will enable researchers from around the world to compare their findings and assess the incidence of anatomical variations more accurately.
According to various authors, anatomical dissection has high educational relevance and should always be included in the training of each and every surgeon [29,30]. Even with the continuous updating of imaging technologies and surgical procedures, direct anatomical observation and dissection are the cornerstones of teaching and learning gross anatomy [30].
Aziz et al. (2002) reviewed the advantages of cadaveric dissection, which can be summarized as follows: (1) prioritizing patient care, (2) gaining a three-dimensional understanding of the human body, (3) developing tactile skills for patient examination, (4) studying anatomical variations, (5) mastering the fundamental skills of medicine, (6) acquiring proficiency in diagnostic imaging, (7) using computer-assisted learning tools that focus on the patient, (8) facilitating group learning, and (9) providing training for medical specialties [30].
5. Conclusions
This study aimed to determine the incidence of the STA–LA–FA configuration variant according to Vazquez et al.’s (2009) classification in a sample of fifty heads. The collected data were compared with the existing literature to confirm the previously reported percentages. The evidence of anatomical variants supports the need to revise the current classification system to include anatomical variations. Moreover, based on the variant origin configuration found in this study and the literature, it may be appropriate to update the terminology used for the anterior branches of the external carotid artery to the more accurate term “anterior branches of the carotid artery”, as suggested by Natsis et al. (2011).
Author Contributions
Conceptualization, F.Z. and G.P.; methodology, A.C., A.G. and G.T; software, A.P.; validation, G.T., A.M. and F.Z.; formal analysis, G.P.; investigation, F.Z.; resources, A.C.; data curation, A.C.; writing—original draft preparation, F.Z. and G.P.; writing—review and editing, A.C.; visualization, A.M. and M.E.C.; supervision, A.C.; project administration, G.T.; funding acquisition, A.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The authors state that every effort was made to follow all local and international ethical guidelines and laws that pertain to the use of human cadaveric donors in anatomical research. The reference legislation on the matter is Italian law nr. 10/2020. (The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Nicola’s Foundation Onlus (protocol code 001-11/01/2023).
Informed Consent Statement
All human cadaveric specimens were derived from donors who gave their written consent for the post-mortem use of their body for educational and scientific purpose. Attached official donor informed consent was issued.
Data Availability Statement
Data available on request from the authors.
Acknowledgments
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. The results from this research can potentially increase humankind’s overall knowledge, which can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lo, A.; Oehley, M.; Bartlett, A.; Adams, D.; Blyth, P.; Al-Ali, S. Anatomical variations of the common carotid artery bifurcation. ANZ J. Surg. 2006, 76, 970–972. [Google Scholar] [CrossRef]
- Devadas, D.; Pillay, M.; Sukumaran, T.T. A cadaveric study on variations in branching pattern of external carotid artery. Anat. Cell Biol. 2018, 51, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, N.; Hori, E.; Ohtani, Y.; Ohtani, O.; Kuwayama, N.; Endo, S. Surgical anatomy of the cervical carotid artery for carotid endarterectomy. Neurol. Med. Chir. 2005, 45, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Núñez, M.; Menchaca-Gutiérrez, J.L.; Pinales-Razo, R.; Elizondo-Riojas, G.; Quiroga-Garza, A.; Fernandez-Rodarte, B.A.; Elizondo-Omaña, R.E.; Guzmán-López, S. Origin variations of the superior thyroid, lingual, and facial arteries: A computed tomography angiography study. Surg. Radiol. Anat. 2020, 42, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Heltzel, S.; Jelinek, L.; Jaynes, D. Variation in the caudal branches of the external carotid artery: Comparison of sex and side. Med. Res. Arch. 2015, 1, 1–10. [Google Scholar] [CrossRef]
- Zümre, O.; Salbacak, A.; Ciçekcibaşi, A.E.; Tuncer, I.; Seker, M. Investigation of the bifurcation level of the common carotid artery and variations of the branches of the external carotid artery in human fetuses. Ann. Anat. Anat. Anz. 2005, 187, 361–369. [Google Scholar] [CrossRef]
- Natsis, K.; Raikos, A.; Foundos, I.; Noussios, G.; Lazaridis, N.; Njau, S.N. Superior thyroid artery origin in Caucasian Greeks: A new classification proposal and review of the literature. Clin. Anat. 2011, 24, 699–705. [Google Scholar] [CrossRef]
- Ozgur, Z.; Govsa, F.; Ozgur, T. Assessment of origin characteristics of the front branches of the external carotid artery. J. Craniofacial Surg. 2008, 19, 1159–1166. [Google Scholar] [CrossRef]
- Vazquez, T.; Cobiella, R.; Maranillo, E.; Valderrama, F.J.; McHanwell, S.; Parkin, I.; Sañudo, J.R. Anatomical variations of the superior thyroid and superior laryngeal arteries. Head Neck 2009, 31, 1078–1085. [Google Scholar] [CrossRef]
- Fazan, V.P.; da Silva, J.H.; Borges, C.T.; Ribeiro, R.A.; Caetano, A.G.; Filho, O.A. An anatomical study on the lingual-facial trunk. Surg. Radiol. Anat. 2009, 31, 267–270. [Google Scholar] [CrossRef]
- Thwin, S.S.; Soe, M.M.; Myint, M.; Than, M.; Lwin, S. Variations of the origin and branches of the external carotid artery in a human cadaver. Singap. Med. J. 2010, 51, e40–e42. [Google Scholar]
- Troupis, T.; Michalinos, A.; Dimovelis, I.; Demesticha, T.; Vlasis, K.; Skandalakis, P. Bilateral abnormal origin of the anterior branches of the external carotid artery. Ann. Vasc. Surg. 2014, 28, 494.e5–494.e7. [Google Scholar] [CrossRef]
- Murlimanju, B.V.; Prabhu, L.V.; Pai, M.M.; Jayaprakash, D.; Saralaya, V.V. Variant origins of arteries in the carotid triangle—A case report. Chang Gung Med. J. 2012, 35, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Espalieu, P.; Cottier, M.; Relave, M.; Youvarlakis, P.; Cuilleret, J. Radio-anatomic study of the carotid axis with regard to the implantation of microsurgical vascular anastomoses. Surg. Radiol. Anat. 1986, 8, 257–263. [Google Scholar] [CrossRef]
- Poisel, S.; Golth, D. Zur Variabilität der grossen Arterien im Trigonum caroticum [Variability of large arteries in the carotid trigone]. Wien. Med. Wochenschr. 1974, 124, 229–232. [Google Scholar] [PubMed]
- Czerwiński, F. Variability of the course of external carotid artery and its rami in man in the light of anatomical and radiological studies. Folia Morphol. 1981, 40, 449–453. [Google Scholar]
- Lucev, N.; Bobinac, D.; Maric, I.; Drescik, I. Variations of the great arteries in the carotid triangle. Otolaryngol. Head Neck Surg. 2000, 122, 590–591. [Google Scholar] [PubMed]
- Demirtaş, İ.; Ayyıldız, B.; Demirbaş, A.T.; Ayyıldız, S.; Sönmez Topcu, F.; Kuş, K.C.; Kurt, M.A. Geometric morphometric study of anterior branches of external carotid artery and carotid bifurcation by 3D-CT angiography. Surg. Radiol. Anat. 2022, 44, 1029–1036. [Google Scholar] [CrossRef]
- Shintani, S.; Terakado, N.; Alcalde, R.E.; Tomizawa, K.; Nakayama, S.; Ueyama, Y.; Matsumura, T. An anatomical study of the arteries for intraarterial chemotherapy of head and neck cancer. Int. J. Clin. Oncol. 1999, 4, 327–330. [Google Scholar] [CrossRef]
- Zaccheo, F.; Mariotti, F.; Guttadauro, A.; Passaretti, A.; Campogrande, M.E.; Petroni, G.; Cicconetti, A. A Rare Configuration origin of the Superior Thyroid, Lingual and Facial Arteries in a Pentafurcated Common Carotid Artery. Anatomia 2022, 1, 204–209. [Google Scholar] [CrossRef]
- Acar, M.; Salbacak, A.; Sakarya, M.E.; Zararsiz, I.; Ulusoy, M. The Morphometrical Analysis of the External Carotid Artery and its Branches with Multidetector Computerized Tomography Angiography Technique. Int. J. Morphol. 2013, 31, 1407–1414. [Google Scholar] [CrossRef]
- Cappabianca, S.; Scuotto, A.; Iaselli, F.; Pignatelli di Spinazzola, N.; Urraro, F.; Sarti, G.; Rotondo, A. Computed tomography and magnetic resonance angiography in the evaluation of aberrant origin of the external carotid artery branches. Surg. Radiol. Anat. 2012, 34, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Delić, J.; Savković, A.; Bajtarević, A.; Isaković, E. Variations of ramification of external carotid artery–common trunks of collateral branches. Period. Biol. 2010, 112, 117–119. [Google Scholar]
- Dessie, M.A. Variations of the origin of superior thyroid artery and its relationship with the external branch of superior laryngeal nerve. PLoS ONE 2018, 13, e0197075. [Google Scholar] [CrossRef] [PubMed]
- Jitpun, E.; Wattanasen, Y.; Tirakotai, W. Do Asians have Higher Carotid Bifurcation? A Computed Tomographic Angiogram Study of the Common Carotid Artery Bifurcation and External Carotid Artery Branching Patterns. Asian J. Neurosurg. 2019, 14, 1082–1088. [Google Scholar] [CrossRef]
- Ito, H.; Mataga, I.; Kageyama, I.; Kobayashi, K. Clinical anatomy in the neck region--the position of external and internal carotid arteries may be reversed. Okajimas Folia Anat. Jpn. 2006, 82, 157–167. [Google Scholar] [CrossRef]
- Klosek, S.K.; Rungruang, T. Topography of carotid bifurcation: Considerations for neck examination. Surg. Radiol. Anat. 2008, 30, 383–387. [Google Scholar] [CrossRef]
- Kaneko, K.; Akita, M.; Murata, E.; Imai, M.; Sowa, K. Unilateral anomalous left common carotid artery; a case report. Ann. Anat. Anat. Anz. 1996, 178, 477–480. [Google Scholar] [CrossRef]
- Aziz, M.A.; McKenzie, J.C.; Wilson, J.S.; Cowie, R.J.; Ayeni, S.A.; Dunn, B.K. The human cadaver in the age of biomedical informatics. Anat. Rec. 2002, 269, 20–32. [Google Scholar] [CrossRef]
- Ghosh, S.K. Cadaveric dissection as an educational tool for anatomical sciences in the 21st century. Anat. Sci. Educ. 2017, 10, 286–299. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).