Abstract
Background: obstructive sleep apnoea is a common and burdensome condition, characterised by obstruction of the airway during sleep at the level of the pharynx, which may occur with symptoms or without any symptoms. The most common place for obstructive sleep apnoea management is in specialised sleep units. Aim: to identify what is known about nurses’ role in comprehensive management of obstructive sleep apnoea, and to determine the effectiveness of nurse-led interventions as well as the cost effectiveness of management of obstructive sleep apnoea in primary care settings. Methods: a scoping review was carried out by searching PubMed/Medline, CINAHL, Scopus, Cochrane Database of Systematic Reviews and ScienceDirect. The study findings were synthesised using a thematic analysis approach. Results: In this review, 12 articles were included, and three key themes emerged, namely the role of nurses in the diagnosis of obstructive sleep apnoea, role of nurses in the follow up and support of obstructive sleep apnoea patients, and role of nurses in the management of obstructive sleep apnoea in primary care and the cost-effectiveness. Conclusion: Nurses can play a critical role in obstructive sleep apnoea. There are many ways in which nurses can contribute, including screening, assessment, diagnosis, promotion of therapy adherence, and following up with patients, including monitoring for any side effects associated with the CPAP machine, such as irritation of the face. Additionally, nurses can provide patient education and coordinate with other health care providers. Nursing interventions such as patient education have been demonstrated to be highly effective in promoting adherence to PAP therapy in both sleep units and primary care settings. Based on the findings of this review, the primary care model is more cost-effective than the sleep unit model in the management of obstructive sleep apnoea patients. The role of nurses in managing Obstructive Sleep Apnoea in both paediatric and adult populations shares similarities, but also includes differences that should be carefully considered and explored. In this review, one article only explored the role of nurses in paediatric OSA care. Thus, there is a need to identify the potential role of nursing in the comprehensive management of paediatric obstructive sleep apnoea, as well as to explore alternative cost-effective approaches that include primary care settings.
1. Introduction
Obstructive sleep apnoea (OSA) is a common and burdensome condition, characterised by obstructions of the airway during sleep at the level of the pharynx that can present with or without symptoms [1,2]. This is in contrast to central sleep apnoea which is due to a dysregulation of breathing during sleep [2].
The individual with OSA has more than 5 events per hour of partial (hypopnoea) or total (apnoea) obstruction of the upper airway despite trying to breathe [3]. An apnoea is defined as a complete obstruction of the upper airway (>90%) lasting for more than 10 s, and hypopnoea is defined as a partial airway obstruction (>30%) sufficient to cause at least a 3% reduction in blood oxygen saturation or sleep arousals [3].
The apnoea–hypopnoea index (AHI) is the key measure used in sleep study monitoring to define and stratify OSA severity; however, this metric has inherent limitations, including not taking into account the degree of accompanying hypoxia, and the length of respiratory events [4]. The AHI levels of 5, 15, and 30 are used as cut points to determine mild, moderate, and severe OSA, respectively [4].
The International Classification of Sleep Disorders (ICSD-3) [5] encompasses a broad definition of OSA, defining it as: (1) clinical symptoms and complaints of diurnal sleepiness, or apnoeas witnessed by a partner, or cardiometabolic abnormalities and an AHI of >5 events per hour of sleep; or (2) 15 or more predominantly obstructive breathing events per hour of sleep (with no attendant symptoms or comorbidities specifically listed) [5].
As a result of OSA, individuals may experience daytime sleepiness, they may describe fatigue, lack of energy, tiredness, poor concentration, bad mood, morning headaches, snoring, and observed breathing pauses during sleep, according to their bed partner [6].
OSA prevalence varies by country and region [7]. Globally, it has been indicated that one billion adults aged 30 to 69 years may be suffering from OSA, with almost 425 million individuals suffering from moderate to severe cases based on an Apnoea-Hypopnoea (AHI) cut-off value, for which treatment is recommended [7]. Additionally, the prevalence of OSA in Europe was estimated in the year of 2018 to be around 175 million, including approximately 90 million individuals with moderate to severe OSA [8].
Paediatric with OSA have a different clinical picture from adults. The prevalence of OSA in children varies from 1% to 5% [9]. The incidence of this condition tends to peak between the ages of 2 and 8 years old [10]. In the majority of cases, OSA in children is diagnosed often as a result of complaints of snoring or they are referred for surgery due to adenoids or enlarged tonsils [11].
It is imperative that OSA-related risk factors and complications are identified for effective management in clinical practice. The development of OSA is influenced by several unmodifiable and modifiable risk factors. The unmodifiable factors include older age, male sex, race/ethnicity, family history of OSA, and cranofacial abnormalities [12,13,14]. Among the modifiable risk factors for OSA are obesity, smoking, and alcohol consumption [13,14]. OSA has been associated with increased risk of cardiovascular diseases [15,16], metabolic disturbances [15], cognitive impairment [17,18,19] and cancer [20,21,22,23]; a possible association between OSA and COVID-19 has also been examined [24,25,26,27].
A polysomnography (PSG) is considered the gold standard diagnostic tool, along with other assessment methods for determining the severity of symptoms and defining a clinical phenotype to guide treatment [28].
As most individuals change their sleeping position frequently during the night, there may be a difference in the proportion of time spent sleeping supine and non-supine. Accordingly, this might have implications for OSA diagnosis based on the AHI. It should be noted that the accuracy of this rating depends on the definition of hypopnoeas, along with other factors, while the criteria for defining mild, moderate, and severe disease are based on expert consensus rather than a clear correlation between grade and risk of adverse outcomes [29]. Consequently, the diagnosis should remain holistic in nature, incorporating simplified home sleep tests (e.g., respiratory polygraphy) with other tests, as needed, as well as symptomatic assessment. The importance of other signals to evaluate the severity of OSA has been highlighted [30]. There is a need for additional efforts to explore specific signals beyond the AHI [31].
The management of OSA typically revolves around positive airway pressure (PAP) therapy; the use of continuous positive airway pressure (CPAP) is considered the gold standard treatment. Additionally, lifestyle changes (i.e., weight loss, physical activity), mandibular advancement devices, and surgery may also be considered, although their application is largely dependent on the characteristics of the patient [32,33].
OSA is seen as a heterogeneous disease, which is characterised by a wide range of symptoms, anthropometric characteristics, polysomnographic patterns, long-term outcomes, and comorbid conditions [34]. In order to address these aspects, tailored treatment must be developed based on patient-reported outcome data, individual risk factors, and the available therapeutic options [33,34]. The optimal treatment of asymptomatic individuals with mild to moderate OSA remains challenging [35]. However, the management approach should be based upon the principle that individuals with different characteristics will be treated differently. Although each treatment option differs in its mode of action, it is common to all of these alternative approaches that efficacy tends to vary between individuals [33].
2. Obstructive Sleep Apnoea Management
OSA management varies by country and is determined by the patient’s symptoms. it is imperative that health care systems adopt effective diagnostic and management strategies in order to minimise the negative health outcomes caused by the condition [7]. There has been considerable progress in diagnosing and management of individuals with OSA in well-resourced settings [36]. It has been reported that the majority of cases of OSA are undiagnosed and untreated [37], even in countries where income levels are high. In low- and middle-income countries, there is little awareness about OSA, and diagnostic and treatment options are often unavailable or have not been adapted for these settings [36]. The low diagnosis rates of OSA can be partially explained by the fact that it is often asymptomatic. In view of the co-morbidities and potential public health implications as well as the economic burden of untreated OSA in the long term, it is imperative to identify and manage patients with OSA. However, the demand for specialised sleep units has been increasing as well as the wait lists for consultations for these services. Considering the chronicity of this disease, its prevalence and long-term consequences, it is imperative to manage it. There has been a proposal for a novel model for managing OSA in primary care settings [38]. A comprehensive approach to the management of OSA should encompass other clinical settings, similarly to the management of other prevalent chronic diseases [38].
The OSA management in specialised sleep units is commonplace. There is, however, a need to point out that the management of OSA in sleep units may not be feasible or necessary for many individuals, and there is also a distinct shortage of sleep specialists when it comes to the comprehensive care of this condition [39,40].
There is evidence to suggest that cost savings and comparable efficacy are achievable in the primary care setting [38,41,42].
The prevalence, accessibility, and cost issues justify the study of more affordable and reliable but less expensive alternatives. It is therefore important to involve all levels of medical care in this process including primary care or specialists who are not directly involved in sleep, second-level hospitals that may be capable of performing simplified studies, and tertiary hospitals with complex equipment and multidisciplinary environment [43,44]. Through the involvement of primary care professionals, OSA underdiagnosis may be improved. This approach involves ambulatory diagnostic techniques and follow-ups that do not require hospitalisation [40]. A consensus document has been recently published that presents a potentially useful algorithm for primary care that allows patients with a high probability of disease due to excessive daytime symptoms (Epworth Sleepiness Scale ESS ≥ 12)) to be evaluated with single- or double-channel devices based on oximetry and/or nasal pressure [45]. The gold standard test for diagnosing OSA is an in-lab sleep study or PSG. If PSG is not feasible, out-of-centre sleep testing (OCST) or home sleep apnoea testing (HSAT) are acceptable alternatives [46]. It has been shown in multiple studies that HSAT is as effective as laboratory-based care [47,48,49,50,51]. These studies suggest that HSAT is also cost-effective, results in comparable treatment decisions, and is associated with similar compliance with PAP therapy. Further, patients reported improved sleepiness and quality of life. However, HSAT may have potential disadvantages over PSG due to the difference in the physiologic parameters collected and the lack of personnel available to adjust sensors as necessary [52]. HSAT devices have increased risk of technical failures due to a lack of real-time monitoring and have inherent limitations resulting from the inability of most devices to define sleep versus wake. A further potential disadvantage is that positive airway pressure (PAP) cannot be initiated during a HSAT but can be initiated during a PSG if needed [52]. It is, however, possible to use PAP therapy during an HSAT under certain circumstances. It is possible to initiate positive airway pressure therapy during the diagnostic process for sleep-disordered breathing using the auto-titrating positive airway pressure (APAP) in some HSAT devices [52,53].
The following research questions directed the review of the literature:
What is known about the role of nurses in comprehensive management of obstructive sleep apnoea?
What is known about the effectiveness of nurse-led interventions, as well as cost effectiveness of obstructive sleep apnoea management in primary care settings?
3. Methodology
As a result of the fragmented and scattered nature of the literature, a systematic review and meta-analysis was not feasible. Moreover, the subject is comparatively understudied and crosses several approaches and disciplines. This study maps current research on this topic based on scholarly publications, including qualitative and quantitative studies. Due to the nature of the task and the current state of research, a scoping review was considered appropriate [54]. The study follows the PRISMA 2020 guidelines for scoping reviews [55]. In order to conduct the search, the electronic databases PubMed/Medline, CINAHL, Scopus, Cochrane Database of Systematic Reviews, and ScienceDirect were searched with terms, syntaxes, and Boolean combinations. The following key search terms were used in the search: obstructive sleep apnoea, OSA, nurses, nurses’ roles, primary care, primary setting, management, intervention, and sleep units.
The inclusion criteria were peer-reviewed studies, including quantitative and qualitative studies, as well as mixed methods studies, studies focused on individuals with OSA of any age group and studies which displayed the nursing contribution to the management of obstructive sleep apnoea in primary care or in sleep units. Inclusion was restricted to English language publications published from January 2015.
This review excluded studies that had been published before 2015, were not in English, or were abstracts, conference papers, editorial studies, commentaries, or grey literature. Choosing 2015 as the year of publication was driven by the desire to present the most current knowledge about the topic rather than leaving the year of published articles unlimited/open.
To manage references, to look for duplicates, and eliminate them, EndNote 9.2 was used as a citation management tool. To maintain the precise numbers obtained from each database, the references were exported to the software. After deduplication, the references were exported to Rayyan using the Rayyan tool [56]. Using the inclusion and exclusion criteria, two reviewers independently examined the titles and abstracts of the references, and any disagreements between them were resolved by consensus. The complete texts of the articles were searched for relevant references. Full-text publications were screened using the same methods as title/abstract screening. Using a custom data charting form recommended by Arksey and O’Malley (2007) [57], the authors, title, publication year, country, study design and sample were collected from the publications. In June 2021, the five databases yielded a total of 566 articles. Following the removal of duplicates, 345 articles were selected for screening. Additionally, 300 studies were disregarded because they failed to present results particular to the role of nursing in OSA management. Of the 45 articles which were retrieved fully, only 10 met all the inclusion and exclusion criteria (Figure 1). The articles included were coded thematically and classified according to major themes and subthemes [58].
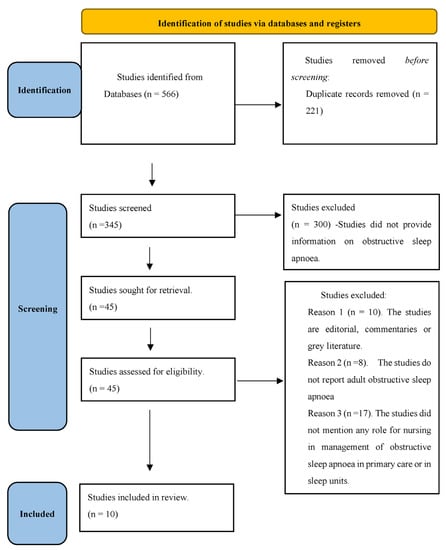
Figure 1.
PRISMA Flow Chart.
A new search of relevant articles was conducted in February 2023, and as a result two new articles were added to the review, as a result, the total of included articles is 12.
Critical analysis can assist researchers in focusing their attention on articles relevant to the research issue and substantiating their assertions with reliable evidence. Furthermore, it can assist them in finding high-quality research that is directly relevant to their practice [59]. A quality assessment was performed using design-specific frameworks provided by the Critical Appraisal Skills Program (CASP). The guiding quality questions were used as a guide to inform decisions about the risk of various systematic biases. They also helped to inform decisions about each study’s applicability to other contexts in light of the geographical setting, cohort characteristics, and the likelihood of selection bias (Appendix B) [60].
4. Results
Using the inclusion criteria, 12 articles were included which were identified as relevant to this review of the nursing role in the comprehensive management of OSA in sleep units or primary care settings. Appendix A summarises the main findings and characteristics of the included studies. The studies examined the role of nursing in adult patients with OSA, except for one study that examined the role of nurses in child patients with OSA [61].
The majority of the studies were quantitative in nature [38,41,42,62,63,64]; one qualitative study [65] was included, and four literature reviews [43,66,67,68]. In the quantitative studies, the main methodology used was randomised controlled trials, which provide a high-quality evidence base. Based on what was found in the literature, three key themes emerged: the role of nurses in the diagnosis of obstructive sleep apnoea, the role of nurses in the follow up and support of obstructive sleep apnoea patients, and the role of nurses in the management of obstructive sleep apnoea in primary care and issues of cost-effectiveness.
5. Role of Nurses in the Diagnosis of Obstructive Sleep Apnoea
Comprehensive patient history and the use of validated questionnaires: according to Suárez et al. (2016), it is imperative to begin OSA management and diagnosis in a primary care setting [43]. It is likely that nurses will screen the patients as they are the first point of contact within the healthcare system. The use of screening tools can reduce OSA-related mortality and morbidity rates. However, screening has several challenges, such as the lack of knowledge regarding how to identify OSA, the best OSA screening tool, how to diagnose OSA, and follow-up procedures for patients who are diagnosed with OSA in different settings [68]. It has been indicated that inadequate training and knowledge of OSA screening tools is a barrier to OSA screening in primary care settings [68]. As a result of the study, it was determined that nurses and primary care physicians would benefit from additional training about OSA detection and its impact on health [68]. The development of a number of OSA screening measures has been designed to facilitate the quick screening of patients for OSA either in hospital or primary care settings [68]. The use of sensitive and specific screening measures provides a cost-effective method of detecting OSA and determining whether to refer the patient to a sleep specialist [68].
The studies have demonstrated that the screening tools are effective in detecting OSA among high-risk patients. Primary care nurses and physicians have received training on OSA risk factors, symptoms, associated comorbidities, and treatment options, as well as using screening tools to ensure early diagnosis. Studies have shown that nurses employed a variety of screening tools/questionnaires in primary care settings as well as in sleep units including STOP-BANG [43], five-dimensions questionnaire (EQ-5D) [38,42], the SF-36 questionnaires [62,63,67] and the Epworth Sleepiness Scale [38,42,43,62,63,67,69]. A more comprehensive sleep history should be taken as soon as possible after a positive OSA screening or when the physician determines that further evaluation is necessary. In addition to the body mass index (BMI) and neck circumference, blood pressure is a measure of health that falls under the responsibility of nurses [68].
Facilitating the OSA diagnostic tests/sleep studies: It is generally acknowledged that PSG is the gold standard method for diagnosing OSA, although it must often be carried out in a controlled, specialist setting [64]. Indeed, PSG is an intricate and technical procedure that may be difficult to perform outside of specialised sleep units, which might prohibit its use in primary care or other settings. Therefore, suspected OSA patients may experience long wait times before being diagnosed and able to receive medical therapy [43].
In recent years, HSAT has become increasingly popular, as it provides a cost-effective and effective diagnostic tool, especially when combined with electroencephalography (EEG) readings [64]. It may be beneficial to refine algorithms using HSAT with or without EEG readings in order to facilitate simple and effective diagnosis of OSA, thus preventing the need for PSG and costly assessments in sleep clinics [64]. Home respiratory polygraphy (HRP) is a simplified, portable monitor that measures air flow, respiratory efforts, pulse oximetry, and body position. Furthermore, HRP has been shown to be a cost-effective alternative for detecting OSA especially in patients with high pre-test OSA suspicion [43]. It has been concluded, however, that some diagnostic procedures are difficult to carry out in primary care, but other procedures may be considered in patients without OSA comorbidities [43]. A further consideration has been that all levels of medical care must be involved. There must be coordination and collaboration between the healthcare team in primary care (i.e., nurses, physicians) as well as the healthcare team in sleep units [43].
6. Role of Nurses in the Follow Up and Support of Obstructive Sleep Apnoea Patients
Obstructive sleep apnoea treatment and strategies to upscale therapy adherence: The treatment of OSA is often multimodal in nature and involves PAP therapy, behavioural interventions, medical device use, and surgical procedures, depending on the patient symptoms and clinical status. Behavioural interventions include weight loss approaches, exercise and sleep position. These may provide benefits in a proportion of patients, although results of interventions may not be realised immediately [66,68]. The use of strategies to enhance adherence to PAP therapy and to promote remote management of patients with OSA are gathering interest, including pharmacological therapies, telemedicine approaches to care provision and supplemental oxygen use. Fields et al. [63] found that a telemedicine-based approach to supporting PAP device use in the community was associated with similar outcomes to standard care, including benefits for mental health and functional outcomes of patients. Telemedicine may provide a basis for remote support, with a high level of satisfaction, in the long-term management of OSA, although further studies are needed to build on this pilot study which only lasted three months and included 60 patients [63].
The role of nurses in follow up and support including patient education: In three randomised controlled trials, patient-reported sleepiness and PAP therapy adherence were comparable at 6 months between primary care unit and specialist sleep care unit [38,41,42].
For instance, a study was conducted to evaluate whether primary care providers could provide follow-up for patients with OSA undergoing PAP therapy [42]. The patients with OSA were randomly assigned to either the specialised sleep unit or primary care units for follow-up over the course of six months. The primary outcome was adherence with PAP therapy at six months [42]. Additionally, the secondary outcomes were Epworth Sleep Scale (ESS) score, EuroQoL, patient satisfaction, BMI, blood pressure and cost-effectiveness. Based on the results, primary care management of patients with OSA was not associated with poorer outcomes than sleep unit management and was shown to be more cost-effective than sleep unit specialist management.
This study involved nurses in the follow-up of patients in the sleep unit, as well as patients undergoing primary care as described below [42].
In the primary care centres that collaborated in this study, one primary care physician and one nurse participated in an educational programme (6 h) that covered both theoretical and practical aspects of managing patients with OSA. The education was delivered by a sleep physician and specialist nurse from the sleep unit who were responsible for managing PAP therapy treatment for the patients in this study who were assigned to the sleep unit group. The patients were followed up in person by a primary care physician or a primary care nurse to review patients’ progress, provide support for the PAP device setup, advice regarding managing PAP-related adverse effects and encouragement to comply with PAP therapy and adhere to its use, education and lifestyle modification. Furthermore, the patients were asked to complete relevant research questionnaires. During the course of the study, the patients were followed at 1, 3, and 6 months. Patients could also consult with the primary care physician or nurse who performed the follow-up visits via telephone if necessary. Sleep unit management was performed by the sleep unit specialist nurse in a similar manner to the way it was previously performed by the primary care nurse [42].
Follow up of child/paediatric patients with OSA: This review identified only one study regarding the management of paediatric OSA [61].
The purpose of the study was to determine the effectiveness and satisfaction of a nurse-led phone follow-up service in children following surgery for sleep disordered breathing SDB or OSA in a tertiary paediatric hospital. Nursing follow-up via telephone consultation was provided to patients who underwent adenotonsillectomy in lieu of the traditional 4-to-8-week clinic visit following surgery. Parents were contacted by telephone for six weeks post-operatively by a nurse specialist. The T-14 validated questionnaire was utilised to assess post-operative outcomes. The experience of these nurse-led telephone consultations was subsequently evaluated by parents between June 2016 and April 2017. The study concluded that a nurse-led telephone service provided postoperatively to patients undergoing an adenotonsillectomy is an effective method for managing post-operative care for these patients without compromising safety or satisfaction [61].
7. Effectiveness of Nursing Led Interventions
Clarification of the role of the nurse in the diagnosis and management of OSA may be derived from studies evaluating the effectiveness of nurse-led interventions and management approaches.
Effectiveness of nurse led interventions: studies in Spain have found that patients with OSA treated by primary care physicians and nurses in a primary care setting have similar outcomes to those treated by sleep unit specialists [38,42]. In a study conducted by the Spanish Sleep Network, PAP therapy adherence was similar between primary care and sleep units, and primary care settings demonstrated consistent overall effectiveness of care. It is noteworthy, however, that patient satisfaction and sleepiness scores were higher in the sleep unit setting [42]. A number of studies have demonstrated the importance of nursing care in specialist and primary care settings [62,65,66,67]. It was found that nurse-led interventions could improve symptoms, mood, quality of life, and compliance with PAP therapy in an evaluation of 80 patients [62].
A meta-analysis by Gong et al. [67] found that nurse-led interventions were not inferior to physician-led interventions in terms of symptomatic improvement, cost effectiveness, and quality of life. Additionally, it was found that nursing-led interventions, particularly educational strategies, could improve adherence to PAP therapy in particular, highlighting the important role that nurses can play both in specialist and primary care settings to educate patients. An educational and personalised follow-up intervention conducted via telephone after discharge from a sleep unit was found to be efficient, safe, and well received by patients [66]. Nurse-led interventions have been shown to improve adherence to PAP therapy compared with usual care [62]. Furthermore, it has been shown in a systematic review of eight RCTs that education programmes can improve PAP therapy adherence in the community setting, while evidence for other approaches remains limited, including pharmacological interventions [66].
Among nursing interventions is the provision of patient education that emphasises lifestyle modification strategies such as providing them with advice about improving their diet, reducing consumption of high-calorie foods, maintaining a healthy lifestyle, and increasing their physical activity [62]. Further, it has been suggested that a family member should be included in the education, as this will strengthen the intervention at home [66]. This highlights the value of nurse-led interventions in promoting follow-up, reducing complications, and reducing unnecessary physical follow-up in practice.
Using a qualitative approach, a study explored the perspectives of patients and providers regarding OSA management in primary care [65].
The study identified several barriers, including a lack of access to specialists, a lack of knowledge of OSA among primary care providers, and a lack of clarity regarding the roles of providers in OSA management. In this context, it is suggested that the integration of primary care and specialist services as well as improved system navigation may be crucial to improving OSA management. According to the analysis of qualitative responses, nurses can play a significant role in educating, providing information, and providing holistic support to patients [65].
8. Cost Effectiveness of Obstructive Sleep Apnoea in Primary Care Settings
The evidence suggests that specialist services/sleep units are not necessary for all patients and should instead be focused on patients with greater severity. The value of primary care services in management of OSA is noted in the included studies.
Cost-effectiveness of OSA management in primary care setting: several studies suggest that comprehensive management of OSA in primary care is a cost-effective and feasible alternative to standard management performed in specialised sleep units [38,41,42,67].
A multicentre, noninferiority, randomised, controlled trial with two open parallel arms and a cost-effectiveness analysis was conducted in Spain in which 20 primary care centres corresponding to six tertiary hospitals sequentially screened patients for suspected OSA. The aim was to compare primary health care areas (PHA) and in-laboratory specialised management protocols during a 6-month follow-up [41]. The results indicated a significant cost in sleep-related care per patient in the laboratory arm compared to the primary healthcare practice arm, primarily due to the higher cost of PSG. In terms of cost-effectiveness, the PHA arm was more cost-effective, with a cost difference of €537 per patient. As a result, the researchers conclude that primary care management utilising a prescribed protocol may provide an alternative to in-lab management for patients with high probability of OSA [41]. Participants who were randomised to the primary care practice arm underwent a home sleep study, and the general practitioner determined whether or not to recommend PAP therapy treatment based on the apnoea–hypopnoea index and clinical symptoms. The primary care nurse provided follow-up management [41]. A noteworthy contribution of this study is the use of a prescribed clinical algorithm in primary care practices that did not require extensive training of primary care nurses.
Accordingly, the findings are consistent with those of another randomised clinical trial conducted to evaluate the cost-effectiveness and effectiveness of primary care and sleep unit models for the management of subjects with suspected OSA [38]. The results showed that among patients with suspected OSA, the primary care model did not result in a worse ESS score or Health Utilities Index than the specialist sleep unit model. The cost analysis revealed a median savings of €558 per patient when comparing the primary care setting to the sleep unit setting [38]. It is noteworthy that the follow-up visits were conducted by specialised nurses at the sleep unit, and in the primary care setting by general practitioners or nurses; all patients were followed up for 6 months [38].
9. Discussion
The literature suggests that standards for diagnosis, management, and nurse-led care for patients with OSA have improved over recent years, as well as suggesting that nurses can play a critical role throughout this journey. As a result of the literature review, it appears that nurses play a variety of roles in the diagnosis, assessment, management, and follow-up of patients with OSA. An overview of these roles can be found in Figure 2. This role includes providing high-quality standards of care and expertise in promoting the wellbeing of patients, educating patients and implementing evidence-based practices across all care settings [70].
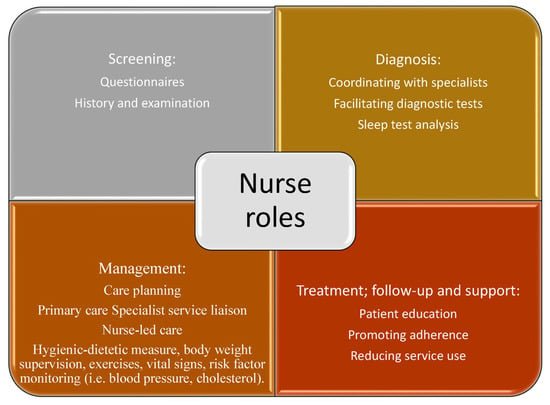
Figure 2.
Conceptualisation of nurse roles in care of patients with OSA.
These findings provide an important update on nurses’ roles in the care of patients with OSA, and their implications should be considered in the context of the wider evidence base and current practice guidelines. The potential role of nursing in paediatric OSA has been explored in a limited number of studies. Further studies are needed to identify the potential role of nursing in the comprehensive management of paediatric OSA and to explore cost-effective alternatives, including other clinical settings such as primary care units. There are many differences between nursing roles in paediatric care and nursing care in adults that should be considered.
The symptoms and treatment of OSA in paediatric and adult patients are unique. For example, paediatric patients may experience behavioural problems, academic difficulties, and growth abnormalities that require additional nursing care attention [71,72,73,74]. Paediatric OSA nurses play a crucial role in identifying these symptoms, educating patients and their families regarding OSA, and providing comprehensive care to patients.
A noteworthy difference in nursing roles between paediatric and adult OSA care relates to the treatment options. Care for paediatric OSA may require a different level of specialisation and skill compared to adult nursing care. This is because the management of OSA in paediatric patients often involves adenotonsillectomy surgery as a treatment option [75,76,77], which demands specific expertise in the care of paediatric patients undergoing surgery. On the other hand, adult patients with OSA usually have a more established care plan that typically involves the use of PAP therapy as the gold standard of care [32,33].
Additionally, paediatric patients with OSA may require a different approach to education and care than adults. Nursing care for children with OSA may require creative and interactive methods for educating them on the importance of treatment adherence as well as involving family members more heavily than in care for adults. On the other hand, adults may require a different and maybe more straightforward explanation of OSA and its treatment [78,79].
It is also important to note that the emotional and psychological support provided to patients and their families varies in paediatric and adult OSA care. It is possible for paediatric patients with OSA to feel anxious and fearful regarding their condition, especially if surgery is required [75,76,77].
Based on the previously mentioned, there are some differences between nursing roles in paediatric and adult OSA care, which highlights the importance of specialised care and attention for patients of different ages who have OSA. In light of this, there is a need to conduct research into different strategies for managing OSA in children and adults and the roles of nurses in this context. For example, the screening of OSA in adult and paediatric settings may involve using different validated questionnaires.
The nursing profession should be prepared to actively participate in the diagnostic and therapeutic process of patients with chronic diseases such as OSA. It will be necessary for nurses to receive training in the proper use of screening tools to ensure an accurate and timely diagnosis and referral of individuals suffering from sleep apnoea.
The nursing profession is capable of administering these questionnaires effectively in hospital/sleep unit settings as well as in the primary care settings; they can supervise patients while they self-administer the questionnaires. In accordance with Williams et al. (2015), nurses and physicians are the most appropriate healthcare professionals to evaluate a patient’s sleep history, refer the patient to a sleeping unit specialist, and initiate treatment, if needed [80].
However, Chapman et al., argue that screening tools/questionnaires will not be of significant benefit in improving disease prediction when primary care professionals are provided with adequate training/education to identify important clinical risk factors for OSA [81]. Nevertheless, the questionnaires may provide useful input in identifying individuals who are suffering from OSA until nursing educational programmes are further developed to integrate OSA as a chronic disease into primary care.
According to the current review, there has been a shift away from specialised sleep units and interventions to a primary care management model. This in in line with a previous study that found the primary care model to be comparable to the sleep unit model in terms of patient-reported sleepiness and PAP therapy adherence at six months; the primary care providers were responsible for performing OSA counselling and therapy decisions [82].
As one example, a randomised, controlled, noninferiority study conducted between September 2008 and June 2010 in Adelaide, Australia included individuals with obstructive sleep apnoea who were treated in primary care practices or at a university hospital sleep medicine centre [82]. Regarding primary care management, the patients were overseen by primary care physicians and nurses who attended a 6-h education programme on obstructive sleep apnoea. The patients were reviewed by a nurse in person to evaluate their progress. They were provided advice regarding managing adverse effects associated with PAP therapy, encouraged to adhere to therapy and advised to discuss alternative treatment options with their primary care physician, if necessary. The patients were educated regarding lifestyle changes that could improve obstructive sleep apnoea, and asked to complete relevant research questionnaires [82].
As the transition from specialist sleep unit care to primary care advances in OSA management and follow-up, nurses will be increasingly involved in the management of these patients [83]. In order for patients to benefit from this transition, nurses must be supported and trained in OSA management and follow-up. The evidence base that underlies nurse-led interventions should also be improved. Moreover, there is a need to coordinate specialist and primary care services regarding OSA, so that the role of primary care nurses can be contextualised within the multidisciplinary model of OSA management [84].
The use of PAP therapy for OSA continues to be a standard of care, which can be delivered in a community setting. However, it is important to ensure that adherence to CPAP is optimised in this setting so that the treatment is effective [85]. It has been demonstrated in this literature that nurse-led follow-up, patient education, and telemedicine and e-health approaches may be helpful in increasing PAP therapy adherence. The application of these strategies may promote evidence-based nursing care in the community and may reduce the need for specialist services and treatment escalation, even as there continues to be debate over effectiveness of e-health tools on PAP therapy adherence [86,87,88]. The American Academy of Sleep Medicine Task Force on sleep medicine supports telemedicine and e-health but emphasises the need for a clear understanding of its application and maintaining clinical standards of care that encompass all aspects of diagnosis and treatment [89].
This review supports the findings of other studies published prior to 2015. There were three trials comparing nurse-led management with sleep unit specialist management [90,91,92]. Two studies were conducted in which patients were randomly assigned to receive sleep apnoea care from a nurse or a physician sleep specialist [91,92]. One study randomised individuals with OSA diagnosis to nurse home visits or annual clinic-based specialist appointments [90]. All the studies found that sleep symptoms and PAP adherence were comparable between groups [90,91,92]; additionally, the nurse-led primary care was associated with lower costs [91,92]. Based on the findings of this review, nurses play a crucial role in OSA management, and primary care models are cost-effective [38,41,42,67].
It should be noted that some trials excluded patients with important medical comorbidities including heart failure, chronic obstructive pulmonary diseases, stroke, and severe psychiatric disease [38,42]. This highlights the complexity of OSA and raises questions regarding the appropriateness of the primary care model in which nurses manage the disease; however, sufficient advanced training could result in nurses gaining more knowledge and skills related to OSA. Additionally, the included studies primarily focused on PAP therapy, whereas non-PAP therapies were largely excluded.
10. Implications
From a research perspective, studies are needed to improve the standardisation of methods used to diagnose OSA in practice through direct comparisons of tools used in different practice settings and a thorough evaluation of their value. Based on the results of these studies, it may be possible to streamline OSA diagnosis in practice, including outside of specialist sleep units, as appropriate, thereby reducing diagnostic costs [84].
Further, super-simplified methods can be utilised, which rely on one or two channels (pulse oximetry and/or respiratory flow) and automatic analysis for interpretation. This method has been proposed as a useful diagnostic tool in primary care [45]. As an alternative to PSG for diagnosing OSA, respiratory polygraphy has been shown to be cost-effective [93], and should be considered as the first option for diagnosing OSA in patients with high pre-test probability (patients with referred symptoms of OSA and/or risk factors such as obesity, hypertension, and snoring).
In addition, further research is required to determine the most effective approaches to improving PAP therapy adherence as well as to supporting PAP therapy withdrawal in patients with OSA. Nurse-led interventions should be considered specifically in this context, given the key role of nurses in the primary care management of OSA [92]. It is clear that nurses play an essential role in supporting adherence to PAP therapy, and more should be done to support nurses in this role by providing evidence-based strategies and facilitating primary care staff engagement with patients in the primary care settings. There should be nursing involvement in services devoted to OSA diagnosis, patient follow up, and educating patients about OSA [94].
The use of telemedicine to facilitate follow-up in the community and to promote assessment of treatment efficacy provides nurses with the opportunity to guide care of patients with OSA in the community, thus reducing the need for specialist care [95]. E-health technology can be used by nurses to monitor and motivate patients with OSA through virtual educational programmes, visits, and remote monitoring; however, more research needs to be conducted to find out whether e-health technologies are cost-effective, whether patient education via e-health tools is effective, and whether patients accept receiving education and monitoring via e-health tools. Furthermore, research is necessary to support the role of nurses in caring for patients with OSA, including qualitative evaluations of barriers to care as well as quantitative evaluations of nurse-led care over the long- and medium-term, focusing on clinically significant outcomes [86].
There are important implications for nurses working in both specialist and primary care settings as a result of the transition. Specialist services may benefit from nurse-led care and assessments as they become more standardised, and there is evidence supporting comparisons between nurse-led and physician-led care. In primary health care, nurses appear to be best positioned to provide effective patient follow-up and education, using diverse techniques such as telemedicine to facilitate patient assessment and prevent treatment escalation. It is necessary, however, to raise concerns regarding the global shortage of nurses as well as whether nurses are prepared to cope with the growing number of patients.
11. Limitations
The review process recognised that there was a relative paucity of literature on the effectiveness of nurses in delivering OSA care in the community, including studies comparing nurse-led care with other approaches. The potential role of nursing in paediatric OSA has been explored in a limited number of studies. There is a need to identify the potential role of nursing in the comprehensive management of paediatric obstructive sleep apnoea, as well as to explore alternative cost-effective approaches that include primary care settings. Nursing-led care is often supported by clinical trials rather than actual practice in patients with OSA, and it is therefore necessary to conduct further research on nurse-led care strategies in practice as well as using other research methodologies, such as qualitative studies.
Over time, however, the evidence base has become increasingly practice-focused and suggests that nurses across settings may be positioned to take a more active role in OSA management, reflecting broader shifts in specialist-primary care divisions. The review included articles published between 2015 and 2023, but the specific time period may have reduced the number of articles included, thereby limiting our ability to identify more comprehensive roles for nurses in OSA management.
12. Conclusions
Nurses can play a critical role in the management of OSA through a variety of roles, such as screening, assessment, diagnosis, follow-up, promotion of therapy adherence, follow-up, patient education, as well as collaborative and coordinated efforts with other healthcare professionals. Nurse-led interventions have been shown to be highly effective in promoting patient adherence to PAP therapy in both sleep units and primary care settings. In this review, the primary care model is found to be more cost-effective than the sleep unit model for the management of OSA patients.
Author Contributions
R.A.E.A.: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Writing—Original Draft, Writing—review & editing. M.S.-d.-l.-T.: Conceptualization, Methodology, Writing—review & editing Validation, and Supervision. F.V.-P.: Methodology, Validation, Writing—review & editing, and Supervision. O.M.-N.: Data curation, Formal analysis. O.M.: Conceptualization, Writing—review & editing Validation. E.R.-A., J.B.-B., F.R.-C. and M.G.-S.: Review, Editing, and Critically reviewed the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
ISCIII (PI21/00337), ERDF/ESF, SES, SEPAR. MS has received financial support from a “Ramón y Cajal” grant (RYC2019-027831-I) from the “Ministerio de Ciencia e Innovación—Agencia Estatal de Investigación” co-funded by the European Social Fund (ESF)/“Investing in your future”. RA is a predoctoral researcher in the University of Lleida, Faculty of Nursing and Physiotherapy.
Acknowledgments
The authors would like to thank Joel Somerville for his efforts in proofreading this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Summary of the Included Studies
| Author and Date | Design | Population | Intervention | Key Findings | Critical Analysis |
| Sabil et al. (2019) [64] | Prospective cohort study | 160 patients investigated by PSG for OSA | Evaluation of a novel sleep/wake cycle algorithm combining EEG and HSAT signals versus PSG | Sensitivity of the algorithm was 76.5%; specificity was 95.5%; compared with HSAT alone, the combined HSAT/EEG algorithm improved detection of AHI by 22.1% | Important evaluation of combined methods for home assessment of OSA; short-term analysis and no direct comparison of diagnostic strategies in a randomised context |
| Pendharkar et al. (2020) [65] | Qualitative survey | 119 primary care providers (surveys) and focus groups/interviews with patients with OSA (n = 28); workshop feedback with primary care and sleep providers (n = 36) | Survey to explore perspectives on barriers and facilitators to optimal, patient centred OSA management in primary care | Poor specialist access, variable knowledge of OSA in primary care providers and lack of clarity about roles were key barriers and led to poorly informed patients and reduced trust; improvements included integration of providers into a model of care, technology, and navigation across the health service | Multiple data sets permit triangulation; limited evaluation of nurse role in primary care context |
| Fields et al. (2016) [63] | Prospective randomised pilot study | 60 veterans with OSA | Telemedicine feasibility and effects versus usual care | Functional outcomes, patient satisfaction and CPAP adherence were consistent in both groups over three months; mental health scores and positive feedback was more likely with telemedicine | Small evaluation: focus on veterans may limit generalisability; limited evaluation of outcomes and over the short-term only (pilot study) |
| Lopez-Lopez et al. (2020) [66] | Literature review | Eight RCTs on methods to improve CPAP adherence | Education, technological, pharmacological, and multidimensional interventions | Educational programmes were the only interventions associated with the potential to improve CPAP adherence; these were generally delivered by nurses in specialist and primary care settings | Systematic review (i.e., not primary data); no meta-analysis of the literature’s relatively small sample of studies included |
| Chen et al. (2015) [62] | Randomised trial | n = 80 patients with OSA | Nurse-led interventions versus usual support at hospital and home | After 12 months of treatment intensive support by nurses was associated with higher CPAP usage and greater improvements in symptoms and mood, including quality of life (p < 0.05) | Relatively small sample size: potential for confounding to influence group outcomes |
| Sanchez-de-la-Torre et al. (2015) [42] | RCT | 210 patients with OSA treated in a sleep clinic | Follow-up at sleep units or in primary care over 6 months | CPAP adherence was similar in both groups (p = 0.18); Epworth Sleepiness scores improved more so in the sleep unit group, along with patient satisfaction (p < 0.05); effectiveness, blood pressure and cost savings were noted in the primary care arm (p < 0.05) | The study is based on a single sleep unit and eight primary care settings, increasing generalisability; factors influenced outcomes, including body mass index |
| Tarraubella et al. (2018) [38] | RCT | 302 patients with suspected OSA and/or resistant hypertension | Comprehensive OSA diagnosis and treatment in primary care or sleep units over 6 months | In patients diagnosed with OSA, the primary care model was associated with an improvement in the mean of ESS score; cost savings were seen with primary care | Detailed evaluation of practice settings; limited appreciation of nurse role specifically |
| Gong et al. (2018) [67] | Meta-analysis | Four studies | Nurse-led versus physician-led care | Nurse-led care is non-inferior to physician-led care in terms of CPAP adherence, sleep outcomes, quality of life and physical function | Few studies included in the analysis; focus on studies where CPAP was the primary treatment strategy |
| Suarez et al. (2016) [43] | Literature review | Four studies | Effectiveness between primary care management of OSA versus traditional sleep unit management (involving primary care physicians and trained nurses) | Functional improvements on sleep questionnaires CPAP adherence and cost-effectiveness | Few studies included in the analysis |
| Ángeles Sánchez-Quiroga M et al.(2018) [41] | RCT | 307 patients were randomised and 303 included in the intention-to-treat analysis. | Effectiveness between primary health care area and specialized management protocols | Primary care management can be an alternative to in laboratory management for patients with an intermediate to high OSA probability | The researchers and the patients were not blinded |
| Miller JN, Berger AM (2015) [68] | Literature review | 17 studies | Evaluating the screening and assessment for OSA in primary care settings | Primary care screening for OSA is fragmented and ineffective. | Nurses are not adequately appreciated for their role in practice settings |
| Walijee et al. (2020) [61] | Prospective observational uncontrolled trial | N = 535 with OSA and discharged from hospital/specialist treatment setting | Nurse-led telephone follow-up | The nurse-led telephone follow-up was associated with efficiency | No direct comparison between usual care and nurse-led intervention; paediatric care setting may limit application to adults |
| ACS, acute coronary syndrome; CAD, coronary artery disease; EEG, electro encephalography; HSAT, home sleep apnoea testing; OSA, obstructive sleep apnoea; PSG, polysomnography; RCT, randomised controlled trial. | |||||
Appendix B. Results of the Critical Appraisal Using the CASP Toolkit
The results of the CASP appraisal checklists are presented for individual study design, including systematic reviews (n = 4), randomised controlled trials (n = 5), cohort studies (n = 1) and qualitative studies (n = 1).

Table A1.
Systematic review/meta-analysis checklist.
Table A1.
Systematic review/meta-analysis checklist.
| Questions | Suarez et al. [43] | Lopez-Lopez et al. [66] | Miller J, Berger A. [68] | Gong et al. [67] |
|---|---|---|---|---|
| Focused question? | Y | Y | Y | Y |
| Right type of papers? | Y | Y | Y | Y |
| Relevant studies included? | Y | Y | Y | Y |
| Quality assessed? | Y | Y | Y | Y |
| Results combined appropriately? | Y | Y | Y | Y |
| Overall results | Discussed in paper | Discussed in paper | Discussed in paper | Discussed in paper |
| Precise? | Y | Y | Y | Y |
| Local application? | ? | ? | ? | ? |
| Important outcomes considered? | Y | Y | Y | Y |
| Benefits worth harms and costs? | Y | ? | Y | Y |
Y = yes; N = no; ? = uncertain.
Table A2.
Randomised controlled trial checklist.
Table A2.
Randomised controlled trial checklist.
| Questions | Chen et al. [62] | Fields et al. [63] | Sanchez-de-la-Torre et al. [42] | Tarraubella et al. [38] | Ángeles Sánchez-Quiroga M et al. [41] |
|---|---|---|---|---|---|
| Focused question? | Y | Y | Y | Y | Y |
| Randomised? | Y | Y | Y | Y | Y |
| Participants followed to conclusion? | Y | Y | Y | Y | Y |
| Blinding? | N | N | N | N | N |
| Baseline similarity? | Y | Y | Y | Y | Y |
| Treated consistently? | Y | Y | Y | Y | Y |
| Comprehensive reporting of outcomes? | Y | Y | Y | Y | Y |
| Precise? | Y | Y | Y | Y | Y |
| Benefits worth harms and costs? | ? | ? | Y | ? | ? |
| Local application? | ? | Y | ? | Y | Y |
| Superior to existing interventions? | ? | ? | Y | ? | ? |
Table A3.
Cohort study checklist.
Table A3.
Cohort study checklist.
| Questions | Sabil et al. [64] | Walijee et al. [61] |
|---|---|---|
| Focused question? | Y | Y |
| Recruited acceptably? | Y | Y |
| Exposure accurate? | Y | Y |
| Outcome measured? | Y | Y |
| Confounding considered? | Y | Y |
| Follow-up complete and long enough? | Y | Y |
| Results | Discussed in paper | Discussed in paper |
| Precise? | Y | Y |
| Believable? | Y | Y |
| Local application | Y | Y |
| Fit with other evidence? | Y | Y |
| Implications for practice? | Y | Y |
Table A4.
Qualitative study checklist.
Table A4.
Qualitative study checklist.
| Questions | Pendharkar et al. [65] |
|---|---|
| Aims stated? | Y |
| Appropriate qualitative methodology? | Y |
| Appropriate design? | Y |
| Appropriate recruitment? | Y |
| Appropriate data collection? | Y |
| Research participant relationship considered? | Y |
| Ethical? | Y |
| Rigorous analysis? | ? |
| Findings clearly stated? | Y |
| Valuable? | Y |
References
- Malhotra, A.; Orr, J.E.; Owens, R.L. On the cutting edge of obstructive sleep apnoea: Where next? Lancet Respir. Med. 2015, 3, 397–403. [Google Scholar] [CrossRef]
- Jun, J.C.; Chopra, S.; Schwartz, A.R. Sleep apnoea. Eur. Respir. Rev. 2016, 25, 12–18. [Google Scholar] [CrossRef]
- Feltner, C.; Wallace, I.F.; Aymes, S.; Middleton, J.C.; Hicks, K.L.; Schwimmer, M.; Baker, C.; Balio, C.P.; Moore, D.; Voisin, C.E.; et al. Screening for Obstructive Sleep Apnea in Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2022, 328, 1951–1971. [Google Scholar] [CrossRef] [PubMed]
- Won, C.H.J. When will we ditch the AHI? J. Clin. Sleep Med. 2020, 16, 1001–1003. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Riha, R.L. Defining obstructive sleep apnoea syndrome: A failure of semantic rules. Breathe 2021, 17, 210082. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.-L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Heinzer, R.; Morrell, M.J.; Penzel, T.; Pepin, J.-L.; Valentine, K.; Nunez, C.; Benjafield, A. Late Breaking Abstract—European prevalence of OSA in adults: Estimation using currently available data. Eur. Respir. J. 2018, 52, OA4961. [Google Scholar] [CrossRef]
- Fagundes, N.; Fagundes, F.; Perez-Garcia, A.; Graf, D.; Flores-Mir, C.; Heo, G. Orthodontic interventions as a management option for children with residual obstructive sleep apnea: A cohort study protocol. BMJ Open 2022, 12, 61651. [Google Scholar] [CrossRef]
- Sánchez-De-La-Torre, M.; Barbé, F. Cellular heterogeneity insights and molecular signatures in paediatric sleep apnoea. Eur. Respir. J. 2023, 61, 2202316. [Google Scholar] [CrossRef]
- Jennum, P.; Ibsen, R.; Kjellberg, J. Morbidity and mortality in children with obstructive sleep apnoea: A controlled national study. Thorax 2013, 68, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Jehan, S.; Masters-Isarilov, A.; Salifu, I.; Zizi, F.; Jean-Louis, G.; Pandi-Perumal, S.R.; Gupta, R.; Brzezinski, A.; McFarlane, S.I. Sleep Disorders in Postmenopausal Women. J. Sleep Disord.Ther. 2015, 4, 212. [Google Scholar]
- Rundo, J.V. Obstructive sleep apnea basics. Cleve. Clin. J. Med. 2019, 86, 2–9. [Google Scholar] [CrossRef]
- Young, T.; Skatrud, J.; Peppard, P.E. Risk Factors for Obstructive Sleep Apnea in Adults. JAMA 2004, 291, 2013–2016. [Google Scholar] [CrossRef] [PubMed]
- Almendros, I.; Basoglu, Ö.K.; Conde, S.V.; Liguori, C.; Saaresranta, T. Metabolic dysfunction in OSA: Is there something new under the sun? J. Sleep Res. 2022, 31, e13418. [Google Scholar] [CrossRef]
- Sánchez-De-La-Torre, M.; Barbé, F. Sleep disorders and cardiovascular disease. Med. Clínica (Engl. Ed.) 2022, 158, 73–75. [Google Scholar] [CrossRef]
- Nikodemova, M.; Finn, L.; Mignot, E.; Salzieder, N.; Peppard, P.E. Association of sleep disordered breathing and cognitive deficit in APOE ε4 carriers. Sleep 2013, 36, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Gaeta, A.M.; Benítez, I.D.; Jorge, C.; Torres, G.; Dakterzada, F.; Minguez, O.; Huerto, R.; Pujol, M.; Carnes, A.; Dalmases, M.; et al. Prevalence of obstructive sleep apnea in Alzheimer’s disease patients. J. Neurol. 2020, 267, 1012–1022. [Google Scholar] [CrossRef] [PubMed]
- Jorge, C.; Targa, A.; Benítez, I.D.; Dakterzada, F.; Torres, G.; Minguez, O.; Carnes, A.; Pujol, M.; Gibert, A.; López, R.; et al. Obstructive sleep apnoea and cognitive decline in mild-to-moderate Alzheimer’s disease. Eur. Respir. J. 2020, 56, 2000523. [Google Scholar] [CrossRef]
- Huang, T.; Lin, B.M.; Stampfer, M.J.; Schernhammer, E.S.; Saxena, R.; Tworoger, S.S.; Redline, S. Associations of self-reported obstructive sleep apnea with total and site-specific cancer risk in older women: A prospective study. Sleep 2021, 44, zsaa198. [Google Scholar] [CrossRef] [PubMed]
- Santamaria-Martos, F.; Sánchez-De-La-Torre, M.; Martínez-García, M.A. Sleep and Cancer: Clinical Studies and Opportunities for Personalized Medicine. Curr. Sleep Med. Rep. 2017, 3, 11–21. [Google Scholar] [CrossRef]
- Martínez-García, M.Á.; Campos-Rodriguez, F.; Barbé, F. Cancer and OSA: Current Evidence From Human Studies. Chest 2016, 150, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-De-La-Torre, M.; Cubillos, C.; Veatch, O.J.; Garcia-Rio, F.; Gozal, D.; Martinez-Garcia, M.A. Potential Pathophysiological Pathways in the Complex Relationships between OSA and Cancer. Cancers 2023, 15, 1061. [Google Scholar] [CrossRef] [PubMed]
- Labarca, G.; Henríquez-Beltrán, M.; Lamperti, L.; Nova-Lamperti, E.; Sanhueza, S.; Cabrera, C.; Quiroga, R.; Antilef, B.; Ormazábal, V.; Zúñiga, F.; et al. Impact of Obstructive Sleep Apnea (OSA) in COVID-19 Survivors, Symptoms Changes Between 4-Months and 1 Year After the COVID-19 Infection. Front. Med. 2022, 9, 1700. [Google Scholar] [CrossRef]
- Peker, Y.; Celik, Y.; Arbatli, S.; Isik, S.R.; Balcan, B.; Karataş, F.; Uzel, F.I.; Tabak, L.; Çetin, B.; Baygül, A.; et al. Effect of High-Risk Obstructive Sleep Apnea on Clinical Outcomes in Adults with Coronavirus Disease 2019. Ann. Am. Thorac. Soc. 2021, 18, 1548–1559. [Google Scholar] [CrossRef]
- Maas, M.B.; Kim, M.; Malkani, R.G.; Abbott, S.M.; Zee, P.C. Obstructive Sleep Apnea and Risk of COVID-19 Infection, Hospitalization and Respiratory Failure. Sleep Breath 2021, 25, 1155–1157. [Google Scholar] [CrossRef] [PubMed]
- Strausz, S.; Kiiskinen, T.; Broberg, M.; Ruotsalainen, S.; Koskela, J.; Bachour, A.; Palotie, A.; Palotie, T.; Ripatti, S.; Ollila, H.M.; et al. Sleep apnoea is a risk factor for severe COVID-19. BMJ Open Respir. Res. 2021, 8, e000845. [Google Scholar] [CrossRef]
- Štengl, M.; Hirani, R.; Smiley, A. A Scoping Review of Sleep Apnea: Where Do We Stand? Life 2023, 13, 387. [Google Scholar] [CrossRef]
- Gottlieb, D.J.; Punjabi, N.M. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA 2020, 323, 1380–1400. [Google Scholar] [CrossRef] [PubMed]
- Azarbarzin, A.; Sands, S.A.; Stone, K.L.; Taranto-Montemurro, L.; Messineo, L.; Terrill, P.I.; Ancoli-Israel, S.; Ensrud, K.; Purcell, S.; White, D.P.; et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: The Osteoporotic Fractures in Men Study and the Sleep Heart Health Study. Eur. Heart. J. 2019, 40, 1149–1157. [Google Scholar] [CrossRef]
- Pevernagie, D.A.; Gnidovec-Strazisar, B.; Grote, L.; Heinzer, R.; McNicholas, W.T.; Penzel, T.; Randerath, W.; Schiza, S.; Verbraecken, J.; Arnardottir, E.S. On the rise and fall of the apnea-hypopnea index: A historical review and critical appraisal. J. Sleep Res. 2020, 29, e13066. [Google Scholar] [CrossRef]
- Randerath, W.J.; Heise, M.; Hinz, R.; Ruehle, K.H. An individually adjustable oral appliance vs continuous positive airway pressure in mild-to-moderate obstructive sleep apnea syndrome. Chest 2002, 122, 569–575. [Google Scholar] [CrossRef]
- Lim, D.C.; Sutherland, K.; Cistulli, P.A.; Pack, A.I. P4 medicine approach to obstructive sleep apnoea. Respirology 2017, 22, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.; de Lange, J.; Hedner, J.; Ho, J.P.T.F.; Marklund, M.; Schiza, S.; Steier, J.; Verbraecken, J. Current and novel treatment options for obstructive sleep apnoea. ERJ Open Res. 2022, 8, 00126–02022. [Google Scholar] [CrossRef] [PubMed]
- Lee-Iannotti, J.K.; Parish, J.M. Exercise as a treatment for sleep apnea. J. Clin. Sleep Med. 2020, 16, 1005–1006. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, S.; Owens, R.; Malhotra, A. Raising awareness about sleep disorders. Lung India 2017, 34, 262–268. [Google Scholar] [CrossRef]
- Laratta, C.R.; Ayas, N.T.; Povitz, M.; Pendharkar, S.R. Diagnosis and treatment of obstructive sleep apnea in adults. CMAJ 2017, 189, E1481–E1488. [Google Scholar] [CrossRef]
- Tarraubella, N.; Sánchez-De-La-Torre, M.; Nadal, N.; de Batlle, J.; Benítez, I.; Cortijo, A.; Urgelés, M.C.; Sanchez, V.; Lorente, I.; Lavega, M.M.; et al. Management of obstructive sleep apnoea in a primary care vs sleep unit setting: A randomised controlled trial. Thorax 2018, 73, 1152–1160. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A.; Campos-Rodriguez, F.; Barbé, F.; Gozal, D.; Agustí, A. Precision medicine in obstructive sleep apnoea. Lancet Respir. Med. 2019, 7, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Donovan, L.M.; Shah, A.; Chai-Coetzer, C.L.; Barbé, F.; Ayas, N.T.; Kapur, V.K. Redesigning Care for OSA. Chest 2020, 157, 966–976. [Google Scholar] [CrossRef]
- Ángeles Sánchez-Quiroga, M.; Corral, J.; Gómez-de-Terreros, F.J.; Carmona-Bernal, C.; Isabel Asensio-Cruz, M.; Cabello, M.; Martínez-Martínez, M.Á.; Egea, C.J.; Ordax, E.; Barbe, F.; et al. Primary care physicians can comprehensively manage patients with sleep apnea a noninferiority randomized controlled trial. Am. J. Respir. Crit. Care Med. 2018, 198, 648–656. [Google Scholar] [CrossRef]
- Sánchez-De-La-Torre, M.; Nadal, N.; Cortijo, A.; Masa, J.; Duran-Cantolla, J.; Valls, J.; Serra, S.; Gracia, M.; Ferrer, F.; Lorente, I.; et al. Role of primary care in the follow-up of patients with obstructive sleep apnoea undergoing CPAP treatment: A randomised controlled trial. Thorax 2015, 70, 346–352. [Google Scholar] [CrossRef]
- Suárez, M.; Osorio, J.; Torres, M.; Montserrat, J.M. Should the diagnosis and management of OSA move into general practice? Breathe 2016, 12, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Simonds, A.; de Backer, W. ERS Handbook of Respiratory Sleep Medicine; European Respiratory Society: Lausanne, Switzerland, 2012. [Google Scholar]
- Mediano, O.; González Mangado, N.; Montserrat, J.M.; Alonso-Álvarez, M.L.; Almendros, I.; Alonso-Fernández, A.; Barbé, F.; Borsini, E.; Caballero-Eraso, C.; Cano-Pumarega, I.; et al. [Translated article] International consensus document on obstructive sleep apnea. Arch. Bronconeumol. 2022, 58, T52–T68. [Google Scholar] [CrossRef]
- Goyal, M.; Johnson, J. Obstructive Sleep Apnea Diagnosis and Management. Mo. Med. 2017, 114, 120–124. [Google Scholar] [PubMed]
- Rosen, C.L.; Auckley, D.; Benca, R.; Foldvary-Schaefer, N.; Iber, C.; Kapur, V.; Rueschman, M.; Zee, P.; Redline, S. A Multisite Randomized Trial of Portable Sleep Studies and Positive Airway Pressure Autotitration Versus Laboratory-Based Polysomnography for the Diagnosis and Treatment of Obstructive Sleep Apnea: The HomePAP Study. Sleep 2012, 35, 757–767. [Google Scholar] [CrossRef]
- Masa, J.F.; Jiménez, A.; Durán, J.; Capote, F.; Monasterio, C.; Mayos, M.; Terán, J.; Hernández, L.; Barbé, F.; Maimó, A.; et al. Alternative methods of titrating continuous positive airway pressure: A large multicenter study. Am. J. Respir. Crit. Care Med. 2004, 170, 1218–1224. [Google Scholar] [CrossRef]
- Kuna, S.T.; Gurubhagavatula, I.; Maislin, G.; Hin, S.; Hartwig, K.C.; McCloskey, S.; Hachadoorian, R.; Hurley, S.; Gupta, R.; Staley, B.; et al. Noninferiority of functional outcome in ambulatory management of obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2011, 183, 1238–1244. [Google Scholar] [CrossRef]
- Berry, R.B.; Hill, G.; Thompson, L.; McLaurin, V. Portable monitoring and autotitration versus polysomnography for the diagnosis and treatment of sleep apnea. Sleep 2008, 31, 1423–1431. [Google Scholar] [CrossRef]
- Corral, J.; Sánchez-Quiroga, M.A.; Carmona-Bernal, C.; Sánchez-Armengol, A.; de la Torre, A.S.; Durán-Cantolla, J.; Egea, C.J.; Salord, N.; Monasterio, C.; Terán, J.; et al. Conventional polysomnography is not necessary for the management of most patients with suspected obstructive sleep apnea noninferiority, randomized controlled trial. Am. J. Respir. Crit. Care Med. 2017, 196, 1181–1190. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Rosen, I.M.; Kirsch, D.B.; Carden, K.A.; Malhotra, R.K.; Ramar, K.; Aurora, R.N.; Kristo, D.A.; Martin, J.L.; Olson, E.J.; Rosen, C.L.; et al. Clinical Use of a Home Sleep Apnea Test: An Updated American Academy of Sleep Medicine Position Statement. J. Clin. Sleep Med. 2018, 14, 2075–2077. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, N71. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2007, 8, 19–32. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Davies, A. Carrying out systematic literature reviews: An introduction. Br. J. Nurs. 2019, 28, 1008–1014. [Google Scholar] [CrossRef]
- Nadelson, S.; Nadelson, L.S. Evidence-Based Practice Article Reviews Using CASP Tools: A Method for Teaching EBP. Worldviews Evid.-Based Nurs. 2014, 11, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Walijee, H.; Sood, S.; Markey, A.; Krishnan, M.; Lee, A.; De, S. Is nurse-led telephone follow-up for post-operative obstructive sleep apnoea patients effective? A prospective observational study at a paediatric tertiary centre. Int. J. Pediatr. Otorhinolaryngol. 2020, 129, 109766. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Chen, W.; Hu, W.; Huang, K.; Huang, J.; Zhou, Y. Nurse-led intensive interventions improve adherence to continuous positive airway pressure therapy and quality of life in obstructive sleep apnea patients. Patient Prefer. Adherence 2015, 9, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.G.; Behari, P.P.; McCloskey, S.; True, G.; Richardson, D.; Thomasson, A.; Korom-Djakovic, D.; Davies, K.; Kuna, S.T. Remote Ambulatory Management of Veterans with Obstructive Sleep Apnea. Sleep 2016, 39, 501–509. [Google Scholar] [CrossRef]
- Sabil, A.; Vanbuis, J.; Baffet, G.; Feuilloy, M.; Le Vaillant, M.; Meslier, N.; Gagnadoux, F. Automatic identification of sleep and wakefulness using single-channel EEG and respiratory polygraphy signals for the diagnosis of obstructive sleep apnea. J. Sleep Res. 2019, 28, e12795. [Google Scholar] [CrossRef] [PubMed]
- Pendharkar, S.R.; Blades, K.; Kelly, J.E.; Tsai, W.H.; Lien, D.C.; Clement, F.; Woiceshyn, J.; McBrien, K.A. Perspectives on primary care management of obstructive sleep apnea: A qualitative study of patients and health care providers. J. Clin. Sleep Med. 2021, 17, 89–98. [Google Scholar] [CrossRef] [PubMed]
- López-López, L.; Torres-Sánchez, I.; Cabrera-Martos, I.; Ortíz-Rubio, A.; Granados-Santiago, M.; Valenza, M.C. Nursing Interventions Improve Continuous Positive Airway Pressure Adherence in Obstructive Sleep Apnea With Excessive Daytime Sleepiness: A Systematic Review. Rehabil. Nurs. 2020, 45, 140–146. [Google Scholar] [CrossRef]
- Gong, F.; Chen, X.; Wu, Y.; Yao, D.; Xie, L.; Ouyang, Q.; Wang, P.; Niu, G. Nurse vs. physician-led care for obstructive sleep apnoea: A systematic review and meta-analysis of randomized trials. J. Adv. Nurs. 2018, 74, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.N.; Berger, A.M. Screening and assessment for obstructive sleep apnea in primary care. Sleep Med. Rev. 2016, 29, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, C.D.; Sen, D.; Kohler, M.; Petousi, N.; Stradling, J.R. Effect of Supplemental Oxygen on Blood Pressure in Obstructive Sleep Apnea (SOX). A Randomized Continuous Positive Airway Pressure Withdrawal Trial. Am. J. Respir. Crit. Care Med. 2019, 199, 211–219. [Google Scholar] [CrossRef]
- Nursing and Midwifery Council. The Code Professional Standards of Practice and Behaviour for Nurses, Midwives and Nursing Associates; Nursing and Midwifery Council: London, UK, 2018. [Google Scholar]
- Kang, M.; Mo, F.; Witmans, M.; Santiago, V.; Tablizo, M.A. Trends in Diagnosing Obstructive Sleep Apnea in Pediatrics. Children 2022, 9, 306. [Google Scholar] [CrossRef]
- Owens, J.A. Neurocognitive and behavioral impact of sleep disordered breathing in children. Pediatr. Pulmonol. 2009, 44, 417–422. [Google Scholar] [CrossRef]
- Churchill, S.S.; Kieckhefer, G.M.; Bjornson, K.F.; Herting, J.R. Relationship between sleep disturbance and functional outcomes in daily life habits of children with Down syndrome. AcademicOupCom. Sleep 2015, 38, 61–71. [Google Scholar] [CrossRef]
- Verhulst, S.; Kaditis, A. Obstructive sleep apnoea in children. Breathe 2011, 7, 240–247. [Google Scholar] [CrossRef]
- Kaditis, A.G.; Alvarez, M.L.A.; Boudewyns, A.; Alexopoulos, E.I.; Ersu, R.; Joosten, K.; Larramona, H.; Miano, S.; Narang, I.; Trang, H.; et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: Diagnosis and management. Eur. Respir. J. 2016, 47, 69–94. [Google Scholar] [CrossRef] [PubMed]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; De Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int. J. Environ. Res. Public Health 2019, 16, 3235. [Google Scholar] [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N. Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics 2012, 130, 576–584. [Google Scholar] [CrossRef]
- Smith, B.M.; Sharma, R.; Das, A.; Aboumatar, H.; Pitts, S.I.; Day, J.; Holzhauer, K.; Bass, E.; Bennett, W.L. Patient and family engagement strategies for children and adolescents with chronic diseases: A review of systematic reviews. Patient Educ. Couns. 2021, 104, 2213–2223. [Google Scholar] [CrossRef]
- Marcus, C. Strategies for improving the quality of verbal patient and family education: A review of the literature and creation of the EDUCATE model. Health Psychol. Behav. Med. 2014, 2, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.J.; Nunes, J.V.; Zizi, F.; Okuyemi, K.; Airhihenbuwa, C.O.; Ogedegbe, G.; Jean-Louis, G. Factors Associated with Referrals for Obstructive Sleep Apnea Evaluation among Community Physicians. J. Clin. Sleep Med. 2015, 11, 23–26. [Google Scholar] [CrossRef]
- Chapman, J.L.; Hoyos, C.M.; Killick, R.; Sutherland, K.; Cistulli, P.A.; Zwar, N.; Yee, B.J.; Marks, G.; Grunstein, R.R.; Wong, K.K.H.; et al. Development and validation of a model for diagnosis of obstructive sleep apnoea in primary care. Respirology 2021, 26, 989–996. [Google Scholar] [CrossRef]
- Chai-Coetzer, C.L.; Antic, N.A.; Rowland, L.S.; Reed, R.; Esterman, A.; Catcheside, P.; Eckermann, S.; Vowles, N.; Williams, H.; Dunn, S.; et al. Primary Care vs Specialist Sleep Center Management of Obstructive Sleep Apnea and Daytime Sleepiness and Quality of Life: A Randomized Trial. JAMA 2013, 309, 997–1004. [Google Scholar] [CrossRef]
- Rosen, I.M. Nurse Practitioners and Physician Assistants Are Important to the Sleep Team. J. Clin. Sleep Med. 2018, 14, 295. [Google Scholar] [CrossRef]
- Chai-Coetzer, C.L.; Redman, S.; McEvoy, R.D. Can primary care providers manage obstructive sleep apnea? J. Clin. Sleep Med. 2021, 17, 1–2. [Google Scholar] [CrossRef]
- Cistulli, P.A.; Armitstead, J.; Pépin, J.L.; Woehrle, H.; Nunez, C.M.; Benjafield, A.; Malhotra, A. Short-term CPAP adherence in obstructive sleep apnea: A big data analysis using real world data. Sleep Med. 2019, 59, 114–116. [Google Scholar] [CrossRef]
- Weaver, T.E. Novel Aspects of CPAP Treatment and Interventions to Improve CPAP Adherence. J. Clin. Med. 2019, 8, 2220. [Google Scholar] [CrossRef] [PubMed]
- Aardoom, J.J.; Loheide-Niesmann, L.; Ossebaard, H.C.; Riper, H. Effectiveness of eHealth Interventions in Improving Treatment Adherence for Adults With Obstructive Sleep Apnea: Meta-Analytic Review. J. Med. Internet Res. 2020, 22, e16972. [Google Scholar] [CrossRef]
- Labarca, G.; Schmidt, A.; Dreyse, J.; Jorquera, J.; Barbe, F. Telemedicine interventions for CPAP adherence in obstructive sleep apnea patients: Systematic review and meta-analysis. Sleep Med. Rev. 2021, 60, 101543. [Google Scholar] [CrossRef]
- Singh, J.; Badr, M.S.; Diebert, W.; Epstein, L.; Hwang, D.; Karres, V.; Khosla, S.; Mims, K.N.; Shamim-Uzzaman, A.; Kirsch, D.; et al. American Academy of Sleep Medicine (AASM) Position Paper for the Use of Telemedicine for the Diagnosis and Treatment of Sleep Disorders. J. Clin. Sleep Med. 2015, 11, 1187–1198. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.; Selvaraj, S.; Dunn, C.; Osman, L.M.; Cairns, J.; Franklin, D.; Hulks, G.; Godden, D.J. Annual review of patients with sleep apnea/hypopnea syndrome—A pragmatic randomised trial of nurse home visit versus consultant clinic review. Sleep Med. 2004, 5, 61–65. [Google Scholar] [CrossRef]
- Andreu, A.L.; Chiner, E.; Sancho-Chust, J.N.; Pastor, E.; Llombart, M.; Gomez-Merino, E.; Senent, C.; Barbé, F. Effect of an ambulatory diagnostic and treatment programme in patients with sleep apnoea. Eur. Respir. J. 2012, 39, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Antic, N.A.; Buchan, C.; Esterman, A.; Hensley, M.; Naughton, M.T.; Rowland, S.; Williamson, B.; Windler, S.; Eckermann, S.; McEvoy, R.D. A randomized controlled trial of nurse-led care for symptomatic moderate-severe obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2009, 179, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Masa, J.F.; Corral, J.; Pereira, R.; Duran-Cantolla, J.; Cabello, M.; Hernández-Blasco, L.; Monasterio, C.; Alonso, A.; Chiner, E.; Rubio, M.; et al. Effectiveness of home respiratory polygraphy for the diagnosis of sleep apnoea and hypopnoea syndrome. Thorax 2011, 66, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Chaiard, J.; Weaver, T.E. Update on Research and Practices in Major Sleep Disorders: Part, I. Obstructive Sleep Apnea Syndrome. J. Nurs. Sch. 2019, 51, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Giron, M.; Bonsignore, M.R.; Montserrat, J.M. New organisation for follow-up and assessment of treatment efficacy in sleep apnoea. Eur. Respir. Rev. 2019, 28, 190059. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).