Abstract
Background: The spleen is the largest secondary immune organ in the body. Knowledge regarding the normal splenic vascular anatomy and its anatomical variants is crucial in the medical practice of surgeons and radiologists and is useful for diagnostic evaluations and the guidance of various surgical procedures. Hence, in this research, we aim to characterize the behavior of the lineal or splenic artery in humans from an anatomoclinical point of view. Methods: A systematic search was carried out in electronic databases to compile the available literature on the research subject. Searches were undertaken in the following databases: Medline, Scielo, Wos, Cinahl, Scopus, and Google Scholar. The search terms were “Splenic artery”, “Splenic vascularization”, “Anatomical variations’’, “Splenic organ”, and “Clinical anatomy”. Results: From the 35 studies included in this review, clinical correlations of anatomical variations in the splenic artery with surgical procedures in the abdominal region were reported in 8 studies. These correlations are mainly associated with surgical procedures for the pancreas, liver, stomach, and bile ducts through imaging of the spleen. To verify our conclusions, the risk of bias of the anatomical studies was measured using the AQUA checklist. Conclusions: Recognition of the usual anatomy and anatomical variants of the splenic artery is crucial for both morphology professionals and clinicians addressing the abdominal region and its vascular components. In this review, we determined that the splenic artery could present a variation in its origin or entry into the splenic hilum, which could mean that in any abdominal intervention there may be complications if the splenic artery variation is overlooked. More anatomic clinical studies considering this variation in both diagnostic and surgical processes are suggested for further investigations.
1. Introduction
This review and meta-analysis has arisen from the need to update existing knowledge in respect of anatomical variants of the abdominal arteries, including cadaveric, imaging, and surgical samples. The spleen is the largest secondary immune organ in the body; it weighs 0.2% of the total body weight and uses 3% of the body’s cardiac output. It is also one of the most vascularized abdominal organs, consistent with the thickness of its blood vessels; this thickness is necessary for it to perform its main functions, including both innate and adaptive immune function and removing old and abnormal red blood cells from circulation, as well as cellular debris and circulating tumor cells [1].
Splenic circulation comprises arterial vessels that are part of the circulation that supplies the esophagus, stomach, proximal duodenum, liver, biliary system, and pancreas [2]. Generally, this circulation is facilitated by the celiac trunk, which originates in the abdominal aorta. This trunk, in most cases, gives rise to three branches: the common hepatic artery, the left gastric artery, and the splenic artery. The splenic artery has an average diameter of around five millimeters, constituting the largest branch of the celiac trunk. It originates at the level of the first lumbar vertebra, with an anteroinferior course, after a short oblique suprapancreatic segment downwards and to the left. Then, it is directed transversely, following a tortuous path along the superior edge of the pancreas posterior to the omental bursa. Next, it runs through the anterior of the pancreas tail, then passes between the splenorenal ligament leaves and reaches the hilum of the spleen, where it can be divided into two to five terminal branches. At this level, it gives rise to the short vessels of the stomach and the left gastro-omental (gastroepiploic) artery that penetrates the gastrosplenic ligament [3,4,5]. In the study by Pandey et al., 2004, it was found that the pattern described above was present in 237 (74.1%) of the 320 specimens studied [6].
Knowledge in respect of splenic vascular anatomy is crucial for both surgeons and radiologists as it is not only helpful for performing diagnostic evaluations but also for guiding surgical procedures. In relation to the above, the absence of anastomosis between the arterial vessels within the spleen is described; this determines the formation of vascular segments of the spleen, which allows the execution of subtotal splenectomies [7,8]. In this regard, some studies using radioisotopes in patients who underwent operations involving a type of disconnection technique have allowed the simplification of operative techniques at the level of the gastric vessels without ligating the splenic artery; this is the reason why some authors have dedicated themselves to the study of patterns of branching of the celiac trunk [9,10]. However, within abdominal vascular diseases, visceral aneurysms represent a smaller fraction and it is important to know about these because of the possibility of rupture, hemorrhage, and the consequent risk to life. Splenic artery aneurysm is a disease with a poorly understood incidence due to its asymptomatic nature. From the point of view of etiopathogenesis, it mainly affects women with an average age of 55 years, arterial hypertension with splenomegaly, atherosclerosis, infections, and trauma. These aneurysms are difficult to diagnose by clinical examination, so different imaging studies are required for their diagnosis [11]. If the artery’s pattern has a variation, surgical techniques will be used to avoid putting the patient’s life at risk. For this reason, the objective of this research was to characterize the behavior of the lineal or splenic artery in humans from both anatomical and clinical points of view.
2. Materials and Methods
In this systematic review, we sought to describe the characteristics of the anatomical variations of the splenic artery. The searches and the order of delivery of information were systematized based on the following methodological steps. Specific scientific articles and books on human anatomy, written in Spanish or English, published between 1970 and 2022, were considered. A systematic search was carried out in electronic databases to compile the available literature on the research topic. Searches were carried out in the following databases: Medline, Scielo, Wos, Cinahl, Scopus, and Google Scholar. We used the search terms “Splenic artery”, “Splenic vascularization of the spleen”, “Anatomical variations”, “Spleen”, and “Clinical anatomy”. These terms were entered with the Boolean connectors “AND”, “OR”, and “NOT”. Additionally, to analyze the bias of the articles, the quality assurance checklist in the performance of primary anatomical studies (AQUA) was used, which allows analyzing the methodological quality of the studies included in this review as it helps to verify the quality of the original anatomical reporting. The AQUA checklist was used to better analyze the quality of the original anatomical study reports. If an item was not reported or was not applicable to this study, we recorded it as “NA” (not applicable). The studies used in this research are listed in Table 1, while Table 2 shows the risk of bias reported by the studies in each of the domains [12] (http://www.eba.cm.uj.edu.pl/aqua (accessed 15 December 2022)); we have submitted the completed checklist form as a supplement to this manuscript.

Table 1.
Anatomical quality assurance checklist.
Table 2.
Details of the application and assessment of the AQUA tool.
The data extracted in the meta-analysis were interpreted to calculate the prevalence of splenic artery variants using the JAMOVI statistical tool. The DerSimonian–Laird model with a Freeman–Tukey double arcsine transformation was used to combine the summary data. In addition, a random effects model was used because of the highly heterogeneous splenic artery prevalence data. The heterogeneity degree between the included studies was assessed using the chi² test and the heterogeneity (I²) statistic. For the chi² test, the result was considered significant if the value of Q p proposed by the Cochrane collaboration was <0.10. Values of the I² statistic were interpreted as follows with a 95% confidence interval (CI): 0–40% might not be important, 30–60% might indicate moderate heterogeneity, 50–90% might represent substantial heterogeneity, and 75–100% could represent a significant amount of heterogeneity [45].
Data were extracted by four investigators (MO, DP, AB, JJV). For each study, the following information was extracted: last name of the first author, year of publication, type of study, sample size, prevalence and morphological characteristics of the splenic artery variants, statistical data presented by the studies, geographic region, and finally the sex of the patients in the sample. Any disagreement was resolved by consensus with a fifth investigator (PV). All articles analyzed in full-text form were evaluated through quality assessment and risk of bias analysis using the methodological quality assurance tool for anatomical studies (AQUA) proposed by the international evidence-based anatomy working group (IEBA) [12].
3. Results
A systematized search of the literature was carried out, where a total of 390 studies were found in the databases reviewed; no studies were found in the gray literature. After applying the exclusion criteria to the searches (articles that did not relate to the anatomical variations of the splenic artery with clinical complications, neither in the title nor in the abstract), a total of 95 studies were analyzed in full-text form and exclusion criteria corresponding to the type of study were applied (systematic reviews, literature reviews, letters to the editor). Another exclusion criterion was articles in respect of animals, which left us with 35 studies included in this review (Figure 1).
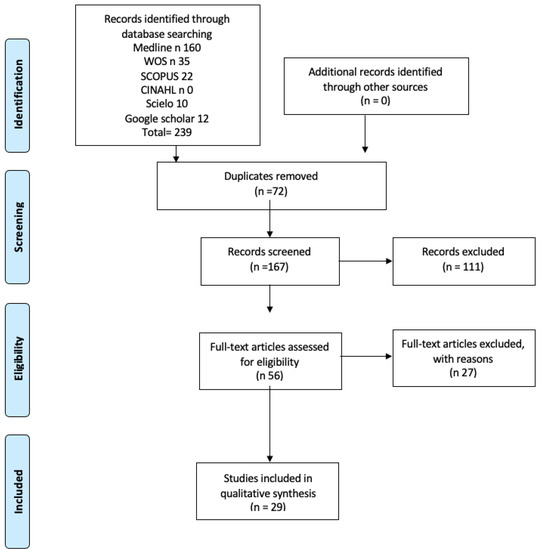
Figure 1.
The search flowchart is shown in the image.
The articles were analyzed through an interpretation guide, which was used to assess their individual quality, based on studies by Greenhalgh et al. (1997) [46] and adapted by MacDermid et al. (2009) [47].
The anatomical variations of the splenic artery found in the literature review are detailed below. These variations are explained in the following order: (1) variations in the origin of the splenic artery, (2) variations in the course of the splenic artery, (3) variations in its entry into the splenic hilum, (4) other anatomical variations, and (5) associated clinical considerations.
3.1. Variations at The Splenic Artery’s Origin
The hepatosplenic trunk is an anatomical variation defined as the fusion of the splenic artery with the common hepatic artery (Figure 2). This variation can present as a single branch of the celiac trunk; in these cases, the left gastric artery originates from the abdominal aorta artery [48,49,50,51]. Alternatively, it may originate directly from the abdominal aorta and the left gastric artery arises from the abdominal aorta, the common hepatic artery, or the splenic artery (Figure 3) [52]. In this review, four studies were found that reported the presence of the hepatosplenic trunk [3,34,51,53]. The first two articles are case studies, which are reports of accidental findings [51,53]. The third study aimed to look for anatomical variations in the splenic artery and the presence of three hepatosplenic (HTS) trunks was reported in a total of 26 cadavers studied, which translates into an incidence of 11.5% [3]. The study by Ekingen et al. (2019) found 35 cases of an HTS trunk in 750 patients (4.67%) [54].
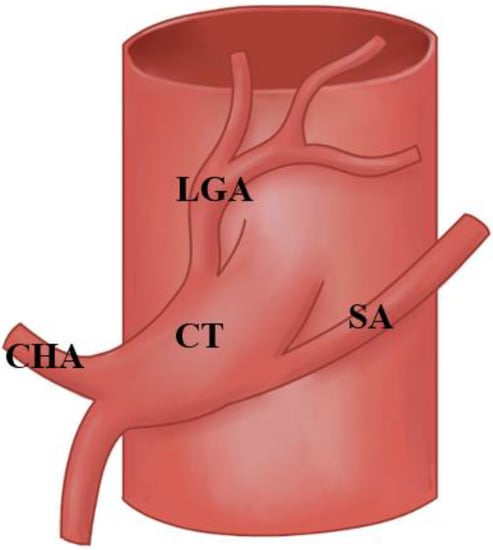
Figure 2.
The image shows the hepatosplenic trunk. Abbreviations: celiac trunk (CT), splenic artery (SA), common hepatic artery (CHA), left gastric artery (LGA).
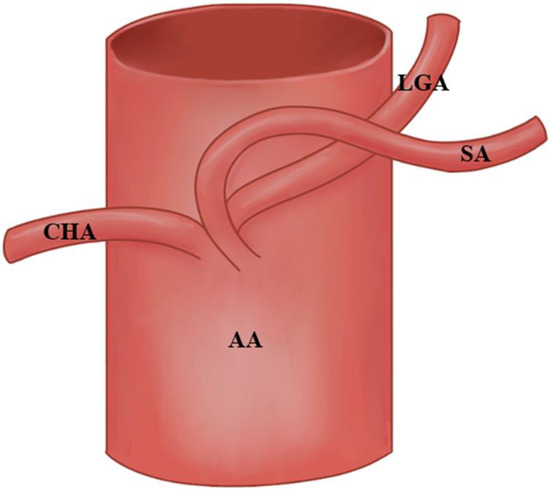
Figure 3.
The image shows the splenic artery arising from the abdominal aorta. Abbreviations: abdominal aortic (AA), splenic artery (SA), common hepatic artery (CHA), left gastric artery (LGA).
The hepato-spleno-mesenteric trunk is an anatomical variation in which the hepatosplenic trunk and the superior mesenteric artery arise from a common vessel, while the left gastric artery originates directly from the abdominal aorta slightly superior to the hepato-spleno-mesenteric trunk. Its prevalence is estimated at 0.40% [55]. In this review, seven studies were found that reported the presence of the hepato-spleno-mesenteric trunk [4,33,51,56,57]. These studies are case studies, reporting a similar origin to that described in the study by Liu et al. (2009). That study had a N of 6 patients; the authors found an SA arising directly from the superior mesenteric artery (SMA) and the common hepatic artery arose from the abdominal aorta [43]. Moreover, the study by Redmond et al. (1989) found that in 126 patients (99.2%) out of 127, the SA arose as a single trunk from the coeliac axis in all but one case, where a second splenic artery was found arising directly from the aorta and supplying the upper pole [44]. Additionally, Bacallao et al. (2017) reported on 15 anatomical preparations: 5 in adult humans, 3 of the male sex and 2 of the female sex, with ages ranging between 48 and 63 years, and 10 human fetuses, between 20 and 29 weeks of age, 6 female and 4 male. They found that three adult human spleens had an SA origin at the celiac trunk and the remaining 40% of adult spleens had a direct tripod origin from the anterior aspect of the abdominal aorta. Regarding the sample of fetuses, it was found that in fetuses between 20 and 24 weeks, the AS originated in the celiac trunk in three (75%), while the remaining fetus showed an AS originating in the form of a direct tripod from the anterior wall of the abdominal aorta (25%). In fetuses from 25 to 29 weeks, five (83.3%) had an SA originating from the celiac trunk and one (16.7%) from the tripod shape, in which the SA was the longest [16].
The celiac–mesenteric trunk is an extremely rare anatomical variant in which the celiac trunk and the superior mesenteric artery originate from the abdominal aorta through a common trunk. According to the study carried out by Poynter, the celiac–mesenteric trunk represents less than 1.4% of all anomalies in the origin of the splenic artery [58]. Ekingen et al. (2019) found eight (1.07%) (two females, six males) instances of SA originating from the celiacomesenteric trunk (CMT), which they described as type 5 CMTs [34].
The gastrosplenic trunk is an anatomical variant described as a common trunk of origin for the left gastric artery and the splenic artery. This trunk is a branch of the abdominal aorta, while the common hepatic artery may originate from the abdominal aorta or the superior mesenteric artery [59]. Oliveros reported this variation in 5.5% of cases [60]. Nakamura reported it in one of three cases studied, showing 33.3% incidence [14]. Iacob et al. (2018) reported one case [19] and Selaru et al. (2020) reported one case [29]. In the study by Ekingen et al. (2019), they found 26 (3.47%) (12 females, 14 males) cases of an SA originating from the GST and they classified these as a type 4 SA variation [34]. Additionally, García-Porrero and Lemes (1988) found a GST in 37.04% of a total of 188 cases that originated in the SA [41].
The origin of the splenic artery has also been described as a branch of the abdominal aorta, arising between the celiac trunk and the superior mesenteric artery, as reported by six studies included in this review [5,6,16,47,61]. Of these studies, four were case reports (5, 15, 35, 39) [5,19,47,62]. A fifth study analyzed 320 cadaveric splenic arteries, of which 26 originated from the abdominal aorta, with an incidence of 8.1% [41]. A sixth study analyzed five cadaveric splenic arteries and reported that two arteries had their origin in the abdominal aorta, with an incidence of 40% [16].
However, the study by Vandame et al. (1986) identified 156 abdominal preparations, of which it was found that 66% had a common splenico-gastro-omentalis trunk from which the SA originated. It was also found that 26% of the preparations had a left gastro-omental artery (LGOA) emerging from them and, in the remaining 8%, the SA divided simultaneously into two splenic rami and the LGOA [38]. In the study by Daisy et al. (2003), in 90% of instances, the SPLA was the largest of the three branches. In the remaining specimens, the CHA was the largest and, in 68% of specimens, the LGA arose as the first branch of the CT, which then bifurcated into the CHA and SPLA; in 30% of dissections the CT divided into three branches at the same point; lastly, in the remaining 2% of instances, the SA and the LGA arose via a common trunk from the CT [39].
3.2. Variations in the Splenic Artery’s Trajectory
The splenic artery is described as the most extensive artery originating in the celiac trunk and its tortuosity is due to its large irrigation territory [5]; therefore, if its path is straight, it represents an anatomical variant. Bacallao et al. (2017) reported two cases of five specimens studied with an incidence of this variation of 40% [16]. Casado et al. reported four cases out of a total of 26 specimens studied with an incidence of this variation of 15.3% [9]. Moreover, Zheng et al. (2015) found a tortuous trajectory in 22 cases (6.9%) [36]. The splenic artery courses anterior to the splenic vein towards the spleen [5]; the study by Casado et al. (2018) described a splenic artery that runs towards the spleen posterior to the splenic vein in 11 of 26 cadavers studied, with an incidence of 42.3% [3]. There are described cases in which the splenic artery follows an antero-pancreatic course. In this anatomical variation, the proximal portion of the splenic artery can be divided into two branches: an upper branch that follows the course usually described by the upper edge of the pancreas and a lower branch that runs along the anterior face of the pancreas. Pandey et al. (2004) studied 320 cadavers, of which 59 presented this variation, with an incidence of 18.4% [6]. There were also cases described in which the splenic artery followed an intrapancreatic course. In this anatomical variation, the proximal end of the splenic artery divides into multiple branches that run within the parenchyma of the body and tail of the pancreas [6,15,18,37,38]. In this review, three studies were found that describe this anatomical variation. One study analyzed 320 specimens, of which 15 presented this variation, with an incidence of 4.6% [6], while the remaining 2 were case report studies [15,18,37]. The splenic artery can also follow a retro-pancreatic course towards the spleen, passing over the posterior surface of the pancreas (6) (Figure 4). One study analyzed 320 specimens, of which 15 presented this variation, with an incidence of 4.6% [6]. Wada et al. (2020) found 25 (83%) type-S cases, where the SA curves and runs suprapancreatically, and 5 (17%) type-D SA cases, where the SA runs straight and dorsal to the pancreas [37]. Another rare anatomical variation of the splenic artery course found in the literature was that the proximal portion of the splenic artery loops on the neck of the pancreas and then embeds itself in the pancreatic parenchyma and the distal end of the loop divides into four branches. Pandey et al. (2004) reported the presence of this loop in two cases of 320 specimens studied, with an incidence of 0.6% [6]. Regarding the branches of the splenic artery, the gastroduodenal artery usually has its origin in the common hepatic artery. In this review, one report of an anatomical variation was found where the gastroduodenal artery was a branch of the splenic artery [31]. The accessory right hepatic artery is an anatomic variation of the right hepatic artery. This variant may originate from the superior mesenteric artery [63] or from the splenic artery [20,21,26]. Kervacionglu et al. (2013) and Al Zahrani et al. (2016) presented case reports [20,21,26]. In the study of Caruso at al. (2016), one case was reported out of a total of 74 specimens studied, which shows an incidence of 1.4% [8]. Ekingen et al. (2019) found 1 male (0.13%) type-13 SA that ran to the spleen as two branches; 25 (3.33%) (10 females, 15 males) type-14 SAs that divided into the replaced left gastric artery (RLGA) and replaced the gastroduodenal artery (RGDA); 15 (2%) (9 females, 6 males) type-15 SAs that divided into the RLGA and replaced the left hepatic artery (RLHA); 5 (0.67%) (1 female, 4 males) type-16 SAs that divided into the RLGA and replaced the common hepatic artery (RCHA); 1 male (0.13%) type-17 SA that divided into the RLGA and a common root of the RLHA and RGDA; 4 (0.53%) (3 females, 1 male) type-18 SAs that divided into the RLGA, the replaced right hepatic artery (RRHA), and a common root of the RLHA and RGDA; 6 (0.80%) (3 females, 1 male) type-19 SAs that divided into the RLGA and a common root of the RRHA and RGDA; 3 males (0.40%) [36].
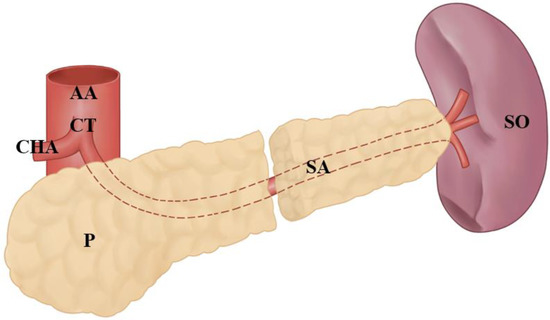
Figure 4.
The image shows the retro-pancreatic splenic artery. Abbreviations: abdominal aortic (AA), splenic artery (SA), common hepatic artery (CHA), celiac trunk pancreas (P), splenic organ (SO).
3.3. Splenic Artery’s Variations at the Entrance to the Splenic Hilum
There are 22 cases (6.9%) of the single-branch SA type (SA passes tortuously through the splenic hilar without dividing into terminal branches), 250 cases (78.9%) of the two-branched type (the SA divides into the superior and inferior lobar arteries), 43 cases (13.6%) of the three-branched type (the SA divides into the superior, middle, and inferior lobar arteries of the spleen), and 2 cases (0.6%) of a multiple-branched SA type (the SA branches into four–seven branches). In 78.43% of cases, the splenic artery divides into two terminal branches (upper and lower) and in 21.57% of cases it divides into three branches (upper, middle, and lower), with the presence of a superior polar collateral branch in 33.33% of cases [1]. We found two studies that reported this anatomical variation [35].
3.4. Other Anatomical Variations of the Splenic Artery
The accessory splenic artery is a rare anatomical variation described in the literature consisting of an accessory splenic branch with three origins. It might be a branch of the left gastroepiploic artery [64], a left gastric artery branch [26], or a branch of the right gastric artery [28]. In this review we found four studies that reported the presence of an accessory splenic artery [4,52,56,60]. All the studies that reported this variation were case report studies. Additionally, an intrahilar and intraparenchymatous anastomosis were shown in a single specimen in the study by Vandamme et al. (1986) [38].
3.5. Clinical Considerations
Anatomical variations of the splenic artery are commonly inspected as an incidental finding during routine cadaveric dissection. Therefore, a clinical implication is often not established as there is no history of any pathology or previous surgical intervention related to death. In our review, we found fourteen studies that reported a clinical correlation with some type of variation in the splenic artery [2,4,8,17,29,35,40,42,43,46,54,58,59].
Next, we will detail the clinical correlations found in the reviewed literature, dividing them into two groups: surgical clinical correlation and clinical correlation with diagnostic and therapeutic study.
3.6. Quantitative Results
Of the 35 included studies (Table 3), 4 were from North America [3,16,24,28], 1 was from South America [46], 13 were from Asia [5,6,13,14,17,18,20,23,27,36,37,39,40,43], 16 were from Europe [3,15,19,23,24,26,29,30,31,32,35,38,39,41,42,44], and 1 was from Africa [45]. In relation to the type of study, nineteen reviewed works corresponded to case studies [5,10,13,15,17,18,19,20,21,22,23,24,25,26,28,29,30,31,33], four were descriptive studies [3,6,32,61], and one was a retrospective study [18]. The last five studies had n > 1 [3,6,14,32,33]. The total number of specimens in the 24 studies analyzed was 684. In relation to gender, five studies did not report the gender of the individuals analyzed [3,14,25,27,33], eleven studies analyzed individuals of the male gender [13,15,17,18,20,22,23,24,26,28,33] and five of the female gender [19,23,29,30,31], and three [3,6,9,32] studies included individuals of both genders. The percentage of men in studies with n > 1 fluctuated between 55.2% and 82.5%, with a mean of 67.7%. The percentage of women in studies with n > 1 fluctuated between 17.5% and 44.8%, with a mean of 32.3%. For the calculation of the incidence of anatomical variations, only studies with n greater than 1 [6,14,16,32] were included. The variation in the origin of the splenic artery was between 1.1% and 40% (origin in the abdominal aorta, hepatomesenteric trunk, and gastrosplenic trunk). Path variations fluctuated between 2.6% and 40% (anterior, retro, or intrapancreatic) (Figure 5). Of the studies included in this review, only one reported the incidence of anatomical variation in the entry of the splenic artery to the spleen (42.3%) [3].
Table 3.
Summary of articles included in the review.
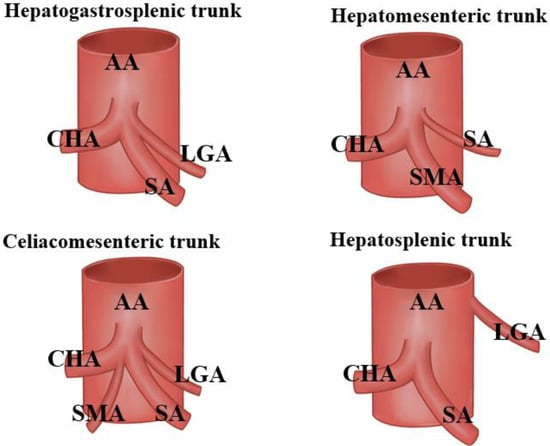
Figure 5.
Celiac trunk trifurcation types according to Adachi. Abbreviations: common hepatic artery (CHA), left gastric artery (LGA), splenic artery (SA), superior mesenteric artery (SMA).
Of the nineteen studies included with n = 1 [3,10,13,15,17,18,19,20,22,23,24,25,26,27,29,30,33,58], sixteen reported variations in the origin of the splenic artery [2,3,6,13,14,16,19,19,20,21,22,23,24,29,30,31] and described the presence of a hepatosplenic trunk [9], a mesenteric hepatosplenic trunk [4,33,54,56,57,63], a gastrosplenic trunk [14,19,29], and an origin of the splenic artery from the abdominal aorta artery [6,16,31]. Only one study showed statistical significance in its results, finding no statistically significant difference in splenic artery tortuosity between the genders (p:0,1) [57]. The results found in this review are summarized in Table 3, Table 4, Table 5 and Table 6.
Table 4.
Summary of the described variations and their clinical correlations of the included articles.
Table 5.
Splenic artery prevalence data of the included studies.
Table 6.
Splenic artery prevalence data heterogeneity of the included studies.
3.7. Surgical Clinical Correlation
Eight studies reported clinical correlations of anatomical variations in the splenic artery with surgical procedures in the abdominal region (Table 4), which were mostly associated with surgeries of the pancreas, liver, stomach, and bile ducts. The main surgical complications presented in the literature are those that occur during surgeries for tumors of the tail and body of the pancreas. This is mainly because, for the resection of the tumor mass, in the presence of SA variants, there could be intrasurgical complications, which are argued in cases of a carcinogenic-type tumor due to its rich vascularization and the different SA route patterns that it can present for this type of pathology. Although there are changes in the position superior to the pancreas, these route variants will always present in an intrapancreatic, inferopancreatic, anteropancreatic, or intrapancreatic route, the latter being the one with the worst prognosis if it is not investigated early. For pyloroduodenal junction and bile duct surgeries, greater caution should be taken for variants associated with the origin of the splenic artery, since, as detailed in the results of this study, the number of possible origins of the artery are varied and before a surgical procedure in this area it is important to determine the patterns and different origins to avoid adverse or iatrogenic phenomena during the intervention. Finally, for variants in the entrance to the hepatic hilum, caution has been detailed in complete splenectomy surgeries or in left colic flexure surgeries, which could also have some type of proximity to the area of the variant [3,6,13,16,17,33,51,56].
3.8. Clinical Correlation with Diagnostic and Therapeutic Study
Eight studies reported clinical correlations of the anatomical variations in the splenic artery with the diagnostic and therapeutic study through images of the abdominal region. This is because, depending on the type of SA variant, different SA origin dispositions could be observed, such as an aberrant trajectory or an arrival in disposition that is different from the splenic hilum; any of these variants could cause confusion in the diagnosis of both vascular pathologies, as well as those of the spleen. This could include greater curvature of the stomach, the upper portion of the duodenum, or pathologies of the pancreas, mainly in respect of the body and tail, since in imaging the diagnosis could otherwise depend on the diagnostic criteria and the patient’s symptoms, which could lead to erroneous diagnoses and/or overestimation or underestimation of different pathologies of the aforementioned regions. Regarding the intervention of therapeutic studies, the same patterns mentioned for diagnosis should be considered [5,13,17,22,27,29,30,31].
4. Discussion
Regarding the study of the variations in the splenic artery, there can be a wide range of possibilities. In relation to what was reported by the reviewed investigations, the splenic artery may present variation in its origin [3,5,6,14,16,19,20,22,23,24,25,29,31,33,62], in its course [3,6,15,16,17,18,32], or in its entrance to the splenic hilum [3,6], and could also present one or more variations [3,6,21,26,37]. This suggests that there could be multiple factors that can influence the development of anatomical variation, including geographic region, gender, and age. As the geographical distribution was relatively homogeneous, with a slight inclination towards the European continent (Table 3), we do not believe it is possible to determine that this criterion has an influence on the higher incidence of anatomical variations in the splenic artery. However, we believe that it may be associated with article search bias or a higher number of studies of the splenic artery that have been carried out in this continent. Regarding gender, the studies included in this review showed that 68.8% of patients were men, while 31.2% were women. These percentages were taken from sixteen case studies [5,6,13,15,17,19,22,23,24,28,29,30,31,33] in which gender was reported. We believe that it is not representative to attribute the variation to this aspect. Only three [6,28,32] studies included men and women, where the results presented means of 67% men and 32.3% women. If we consider these data, we can say that two-thirds were men and one-third were women, which could be an indication that these variations have a greater incidence in male subjects; however, we believe, that to better support this theory, more studies should be carried out that measure this relationship. Regarding age, most of the studies did not report age since they were mostly cadaveric studies and these tend not to mention age. In relation to the above, we believe that age is not a factor that influences directly the variation of the splenic artery, considering that its variation comes from embryonic development [65], but this could be analyzed in relation to the appearance of some associated comorbidities in different age cycles.
In relation to the variation in the splenic artery’s origin, we found that it has an incidence between 1.1 and 40%. Within these variations, its origin in the abdominal aorta artery [5,19,31] was most frequently mentioned, specifically under the celiac trunk and with an inclination to the left. Another reported origin was the hepatomesenteric trunk [19,63], from which the superior mesenteric artery, the common hepatic artery, and the splenic artery arose directly. Finally, this artery can also originate in the gastrosplenic trunk [14,19,29], which has been described as inferior to the celiac trunk, and the splenic artery will have its origin in the left part of the gastrosplenic trunk. However, variation in the course can present many patterns of variation, with the pancreas being the main relation to consider, for which the main variation was the intrapancreatic trajectory [6,15,18] (Figure 6). Later, we will comment on its clinical correlation, which could be very important. Finally, the variation in the entrance to the splenic hilum [3,6] is mainly associated with the multiple branches of the splenic arteries in the hilum of the spleen or with their entrance in the superior or inferior poles of the spleen.
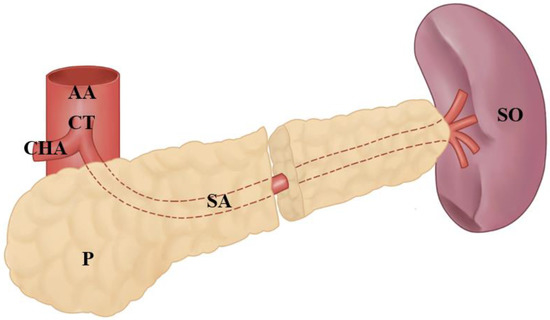
Figure 6.
The image shows the intrapancreatic splenic artery. Abbreviations: abdominal aortic (AA), splenic artery (SA), common hepatic artery (CHA), celiac trunk pancreas (P), splenic organ (SO).
Notably, 42% of the studies reviewed showed that variations in the splenic artery should be considered for surgical approaches to surrounding organs [3,13,17,20,21,22,23,24,31]. Ignoring these variations could cause a hemorrhage in the area, which, if it is not handled quickly, could present a serious risk to the patient’s life. Additionally, 36% of the studies reviewed highlighted the importance of knowing these variants for the diagnosis of certain abdominal pathologies [13,20,23,24,25,30,33], mainly pancreatitis or other conditions of the pancreas, in which the position of the splenic artery could have some type of diagnostic and therapeutic consideration; to a lesser extent, the studies also suggested considering the variants in the approach to stomach or large intestine pathologies.
These results support the importance of a thorough understanding of the normal anatomy and its variations in the practice of clinical and therapeutic medicine to avoid possible complications. We believe that this study will contribute to the current knowledge to enable better performance in surgical intervention in the abdominal region and in angiographic practice generally.
Of the studies included in this review, to analyze their methodological quality, they were subjected to the quality assessment of anatomical studies bias analysis [12]; the results reported the five domains covered by this tool and the criteria of the objectives and the characteristics of the studies. Studies and anatomical descriptions of the risk of bias were uncommon. For all domains, more than a 30% risk of bias was found. Particularly for the domain “objective(s) and characteristics of the studies”, 18 studies (51%) [5,6,10,13,18,19,20,23,24,25,26,27,29,32,34,35,38,40] are at high risk of bias, while in the domain “ study design”, 24 studies (69%) [3,4,5,8,13,14,15,17,18,19,24,28,29,30,33,34,36,38,39,52,53,59,60,64] have a high risk of bias. In the domain “characterization of the methodology”, 18 studies (51%) [5,6,15,18,22,25,26,27,29,30,32,33,34,38,39,42,54,55] have a high risk of bias. With respect to the “descriptive anatomy” domain, 21 (60%) [3,4,5,6,13,14,16,17,18,19,20,21,24,27,28,29,30,31,32,33,37,42,59,60] studies presented a high risk of bias. Lastly, for the domain “outcome report”, the risk of bias was high in 11 (31%) studies [13,20,21,22,23,24,25,26,27,38,56]. The foregoing suggests that the results reported by several of the studies should be taken with caution, but we should also highlight that in some domains the level of risk of bias is increased by case studies that may not have a rigorous methodological quality [5,6,15,18,24,25,26,27,28,29,30,31,32,33,34,38,39,42]. Regarding the prevalence of the SA variant, we excluded 19 studies that had N equal to 1 and all studies in which its prevalence was 100% [5,13,15,18,19,20,21,23,24,26,27,28,29,30,31,33,41,57], since, in this case, the sample was chosen intentionally or for convenience and therefore gave this result. With respect to the 15 studies [3,14,16,16,34,35,36,37,38,39,40,41,42,43,44] that met the criteria to be meta-analyzed based on the prevalence variable, these presented high heterogeneity, which indicates that they were very disparate in their sample; however, in the same way, they met the criteria defined by the research group for meta-analysis based on their prevalence (Table 5). The results obtained in the meta-analysis show that the prevalence of the SA variant was 0.29, with a CI of 0.17 to 0.41, which, from the theoretical point of view of the definition of the anatomical variant, would exclude it and represent it as a variability of AS. We believe that this is due to the fact that six [3,6,16,36,42,44] of the meta-analyzed studies presented a prevalence above 20%, which is represented as our standard error (0.00598); this suggests that the reported prevalence data should be analyzed individually and with caution, since some other factor may have intentionally or accidentally influenced the prevalence in each of the included studies. However, the meta-analysis shows us that the prevalence results were statistically significant in relation to the comparison between the different samples p < 0.001. Finally, for the meta-analysis, the weight of the included studies fluctuated between 4.83% and 7.03%, which correlates with the high heterogeneity of the studies included for the meta-analysis, supported by the differences in the total N included. For the forest plot, where the prevalence of SA and the prevalence of SA variations are compared, the data are reported as the prevalence or number of variants reported by each of the studies in relation to the total N of the SA (Figure 7). The foregoing was applied to all the studies that met the condition of declaring the AS variant in their sample jointly. Although the heterogeneity reported in the forest plot is high, the aforementioned results show us that, in studies that showed the SA variants, there was high statistically significant heterogeneity (I2) (p < 0.001) (Table 6). The clinical considerations reported by the included studies mention both surgery and diagnostic and interventional radiology, such as, for example, the development of transarterial treatment of liver tumors [13,20], and allow the surgeon to select a proper surgery approach and prevent potential iatrogenic blood loss [17,23,24,42,43]. However, there were two studies that showed the correlation of an SA originating from the superior mesenteric artery and distal aneurysms [22,25] of the supramesocolic region. For this reason, we emphasize the importance of determining how the variants of SA could structurally or functionally influence the correct functioning of the spleen and whether this variant and association present some type of characteristic clinical picture or a type of symptomatology that indicates this anatomo–clinical relationship. Our review comprehensively addressed AS variants, taking as samples studies that included cadavers, imaging studies, and studies with individual intra-operative findings for patients with these variants, and we believe that our review is different from that carried out by Manatakis et al. (2020). Although they carried out an exhaustive systematic review of SA variations (including the following aspects: year of publication; country of origin; type of investigation (cadaver dissection, corrosion cast and/or arteriogram); sample size; demographic characteristics (gender, age, and ethnicity); number of SA terminal branches; SA origin and course; distance of SA terminal division point from the splenic hilum; type of SA branching pattern at the hilum; polar artery (PA) [66], prevalence; origin, and length; number of splenic lobes and segments; prevalence of intrasplenic anastomoses), we also considered, in addition to these aspects, the clinical correlation of each of the SA variants, if any. It should be noted that this systematic review and meta-analysis, unlike other previously published studies, shows the prevalence of different studies in addition to including various study types and also includes cadaveric and imaging samples, increasing the sample spectrum and methodological and statistical scope of our results. However, the study by Manatakis et al. (2020) only considered studies in English conducted on cadavers whether they involved dissection, corrosion casts, and/or arteriograms up to the year 2018, while we considered studies in English and Spanish and also considered articles up to the year 2022, considering seven papers after 2018 [17,23,29,34,35,37] that were not considered in the previously described article [67]. Finally, we performed a prevalence meta-analysis to account for the prevalence of each of the anatomical variants of AS, which methodologically demonstrates greater rigor. Taking into consideration the differences expressed above, we hope our review and meta-analysis provides a contribution and a broader analysis of the SA variants and may provide assistance for medical or rehabilitation professionals in respect of the supramesocolic region through an anatomical translational study.
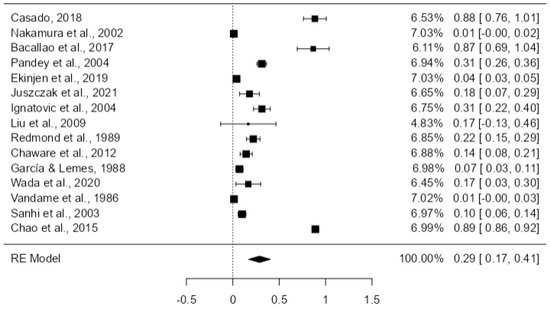
Figure 7.
Forest plot of prevalence of the variations of the SA of the included studies [3,6,10,14,16,34,36,37,38,39,40,41,42,43,44].
5. Limitations
The limitations that we report for this review comprise the publication bias of the included studies (since studies with different results that were found in the non-indexed literature in the selected databases may have been excluded and our results could have changed), the probability of not having carried out the most sensitive and specific search on the topic to be studied, and, finally, the personal selection criteria of the authors for the article filter.
6. Conclusions
Determining the normal anatomy and the anatomical variants of the splenic artery is crucial both for the knowledge of professionals with respect to the morphological area and for clinical professionals who deal with the abdominal region and its vascular components. In this review, we discovered that the variation in the splenic artery can be at its origin, along its path, or at its entrance to the splenic hilum, which leads us to understand that any abdominal intervention in the territory adjacent to the normal path of this artery could cause complications if the possible variations of this artery are not taken into consideration. For this reason, it is suggested that new clinical anatomy studies should be carried out that consider these variations in both diagnostic and surgical processes. Finally, we propose that in future primary studies, the AQUA questionnaire should be applied before writing the research paper so that the results of the study are replicable and more reliable, thus reducing the risk of bias.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank the team that allowed us to successfully carry out this investigation, as well as our families, who gave us time to finish this investigation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sirio, M.; Herrera, N.; Rodríguez, M.; Antonetti, C. Contribución De La Ar-teria Esplénica En La Irrigación Del Bazo; Revista de la Facultad de Medicina; Facultad de Medicina de la Universidad Central de Venezuela: Caracas, Venezuela, 2023; Available online: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S0798-04692008000200003&lng=es (accessed on 15 January 2023).
- Keith, L.M.; Agur, A.M.R.; Dalley, A.F. Clinically Oriented Anatomy 7E; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Casado, M.; Rafael, P. Variantes Anatómicas De La Arteria Esplénica; Revista Médica Electrónica; Centro Provincial de Información de Ciencias Médicas de Matanzas—FCMM: Matanzas, Cuba, 1997; Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242018000200011&lng=es (accessed on 15 January 2023).
- Hirai, Y.; Yamaki, K.-I.; Saga, T.; Hirata, T.; Yoshida, M.; Soejima, H.; Kanazawa, T.; Araki, Y.; Yoshizuka, M. An Anomalous Case of the Hepato-spleno-mesenteric and the Gastro-phrenic Trunks Independently Arising from the Abdominal Aorta. Kurume Med. J. 2000, 47, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ren, Z.F. Gastroduodenal-splenic trunk: An anatomical vascular variant. Rom. J. Morphol. Embryol. 2011, 52, 1385–1387. [Google Scholar] [PubMed]
- Pandey, S.; Bhattacharya, S.; Mishra, R.; Shukla, V. Anatomical variations of the splenic artery and its clinical implications. Clin. Anat. 2004, 17, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Susan, S.; Gray, H. Gray’s Anatomy: The Anatomical Basis of Clinical Practice; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Richard, M.; Levine, M. Textbook of Gastrointestinal Radiology; Elsevier: Philadelphia, PA, USA, 2022. [Google Scholar]
- Drake, R.L.; Vogl, W.; Maw, M.; Gray, H.; Tibbitts, R.; Richardson, P. Gray’s Anatomy for Students; Elsevier: New Delhi, India, 2020. [Google Scholar]
- Covantev, S.; Mazuruc, N.; Drangoi, I.; Belic, O. Unusual development of the celiac trunk and its clinical significance. J. Vasc. Bras. 2021, 20, e20200032. [Google Scholar] [CrossRef]
- Díaz Mesa, J.; Domínguez Cordovés, J.; González Sosa, G.; Madrigal Batista, G.; Queral Gómez Quintero, R.; Collera Rodríguez, S.; Alfonso Sabatier, C.; de Armas Fernández, M.C. Aneurisma De La Arteria Esplénica; Revista Cubana de Cirugía; Editorial Ciencias Médicas: La Habana, Cuba, 2002; Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-74932008000200010 (accessed on 15 January 2023).
- Tomaszewski, K.; Henry, B.M.; Ramakrishnan, P.K.; Roy, J.; Vikse, J.; Loukas, M.; Tubbs, R.S.; Walocha, J.A. Development of the Anatomical Quality Assurance (AQUA) Checklist: Guidelines for reporting original anatomical studies. Clin. Anat. 2016, 30, 14–20. [Google Scholar] [CrossRef]
- Aljahani, J.; Alaklabi, A.; Almalki, W.; Alfaleh, H.; Alzahrani, Y. Splenic artery arising from hepatic artery proper in a patient with celiacomesenteric trunk: A rare anatomical variant. Surg. Radiol. Anat. 2019, 41, 1391–1394. [Google Scholar] [CrossRef]
- Nakamura, Y.; Miyaki, T.; Hayashi, S.; Iimura, A.; Itoh, M. Three cases of the gastrosplenic and the hepatomesenteric trunks. Okajimas Folia Anat. Jpn. 2003, 80, 71–76. [Google Scholar] [CrossRef]
- Ozan, H.; Önderoglu, S. Intrapancreatic course of the splenic artery with combined pancreatic anomalies. Surg. Radiol. Anat. 1997, 19, 409–411. [Google Scholar] [CrossRef]
- Bacallao Cabreras, I.S.; Quesada Molina, D.; Fong Rodríguez, V.; Serrano González, L.M.; Cuba Yordi, O.L.; Almaguer Rodríguez, C. Comportamiento anatómico de la arteria lienal o esplénica en el humano. Rev. Arch. Médico Camagüey 2017, 21, 842–853. [Google Scholar]
- Ramakrishnan, R.; Viswakumar, D.K.; Goriparthi, B.P. Anomalous Course of Accessory Splenic Arteries in Gastrosplenic Ligament: Case Report and Clinico-Embryological Basis. Acta Med. 2020, 63, 133–136. [Google Scholar] [CrossRef]
- Srinivas, M.; Kataria, R.; Bhatnagar, V.; Tandon, N.; Iyer, K.V.; Gupta, A.K.; Mitra, D.K. Intra-pancreatic splenic artery pseudoaneurysm. Pediatr. Surg. Int. 1998, 13, 171–174. [Google Scholar] [CrossRef]
- Iacob, N.; Pusztai, A.M.; Miclăuş, G.D.; Pop, E.; Matusz, P. An anomalous origin of the gastrosplenic trunk and common hepatic artery arising independently from the abdominal aorta: A case report using MDCT angiography. Rom. J. Morphol. Embryol. 2018, 59, 353–357. [Google Scholar]
- Al Zahrani, Y.; AlMat’Hami, A.; Alobaidi, H.; Wiseman, D.; Mujoomdar, A. Accessory Right Hepatic Artery Arising from Splenic Artery Supplying Hepatocellular Carcinoma Identified by Computed Tomography Scan and Conventional Angiography: A Rare Anatomic Variant. Ann. Vasc. Surg. 2017, 38, 316.e1–316.e5. [Google Scholar] [CrossRef]
- Caruso, F.; Dondossola, D.; Fornoni, G.; Caccamo, L.; Rossi, G. Right hepatic artery from splenic artery: The four-leaf clover of hepatic surgery. Surg. Radiol. Anat. 2016, 38, 867–871. [Google Scholar] [CrossRef]
- Facy, O.; Naouri, A.; Dugas, B.; Kadji, M.; Bernard, P.; Gabrielle, F. Anévrisme de l’artère splénique naissant de l’artère mésentérique supérieure: Stratégie thérapeutique. Ann. Chir. 2006, 131, 401–404. [Google Scholar] [CrossRef]
- Felli, E.; Wakabayashi, T.; Mascagni, P.; Cherkaoui, Z.; Faucher, V.; Pessaux, P. Aberrant splenic artery rising from the superior mesenteric artery: A rare but important anatomical variation. Surg. Radiol. Anat. 2019, 41, 339–341. [Google Scholar] [CrossRef]
- Fiorello, B.; Corsetti, R. Splenic Artery Originating from the Superior Mesenteric Artery: An Unusual but Important Anatomic Variant. Ochsner J. 2015, 15, 476–478. [Google Scholar]
- Kanoun, H.; Boulanouar, D.; Djenas, M.; Ghecham, R.; Ben Ziada, N.; Rehimat, S.E.; Djamel, F.; Mehyaoui, R. Aneurysm of a splenic artery originating from the superior mesenteric artery.About a case. Tunis. Med. 2018, 96, 317–320. [Google Scholar]
- Kervancioglu, S.; Yilmaz, F.G.; Gulsen, M. Massive upper gastrointestinal bleeding from an accessory splenic artery mimicking isolated gastric varices. Folia Morphol. 2013, 72, 366–370. [Google Scholar] [CrossRef]
- Patil, J. Atypical Arterial Supply to the Spleen by Polar Branches of Splenic Artery and Accessory Splenic Artery—A Case Report. J. Clin. Diagn. Res. 2014, 8, AD03–AD04. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Lowe, S. Accessory Splenic Artery: A Rare Cause of Upper Gastrointestinal Bleeding. Cardiovasc. Interv. Radiol. 2017, 40, 1115–1117. [Google Scholar] [CrossRef] [PubMed]
- Șelaru, M.; Rusu, M.C.; Jianu, A.M.; Bîrsășteanu, F.; Manta, B.A. Hepatomesenteric trunk, gastrosplenic trunk, coiled splenic and hepatic arteries, and a variant of Bühler’s arc. Folia Morphol. 2021, 80, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Slaba, S.; Sfeir, S.; Nassar, J.; Noun, R.; Checrallah, A.; Tamraz, J. Variante originale de l’artère splénique. J. de Radiol. 2005, 86, 657–658. [Google Scholar] [CrossRef]
- Slaba, S.; Assaf, S. Aberrant gastroduodenal artery with splenic origin. Surg. Radiol. Anat. 2018, 40, 1437–1440. [Google Scholar] [CrossRef]
- Sylvester, P.A.; Stewart, R.; Ellis, H. Tortuosity of the human splenic artery. Clin. Anat. 1995, 8, 214–218. [Google Scholar] [CrossRef]
- Del-Sol, M.; Ottone, N.E.; Vásquez, B. Tronco Hepato-Espleno-Mesentérico. Descripción de una Disposición Anómala del Tronco Celíaco. Int. J. Morphol. 2018, 36, 1525–1528. [Google Scholar] [CrossRef]
- Ekingen, A.; Hatipoğlu, E.S.; Hamidi, C.; Tuncer, M.C.; Ertuğrul, Ö. Splenic artery angiography: Clinical classification of origin and branching variations of splenic artery by multi-detector computed tomography angiography method. Folia Morphol. 2020, 79, 236–246. [Google Scholar] [CrossRef]
- Juszczak, A.; Mazurek, A.; Walocha, J.A.; Pasternak, A. Coeliac trunk and its anatomic variations: A cadaveric study. Folia Morphol. 2021, 80, 114–121. [Google Scholar] [CrossRef]
- Zheng, C.-H.; Xu, M.; Huang, C.-M.; Li, P.; Xie, J.-W.; Wang, J.-B.; Lin, J.-X.; Lu, J.; Chen, Q.-Y.; Cao, L.-L.; et al. Anatomy and influence of the splenic artery in laparoscopic spleen-preserving splenic lymphadenectomy. World J. Gastroenterol. 2015, 21, 8389–8397. [Google Scholar] [CrossRef]
- Wada, Y.; Aoki, T.; Murakami, M.; Fujimori, A.; Koizumi, T.; Kusano, T.; Matsuda, K.; Nogaki, K.; Hakozaki, T.; Shibata, H.; et al. Individualized procedures for splenic artery dissection during laparoscopic distal pancreatectomy. BMC Surg. 2020, 20, 2–3. [Google Scholar] [CrossRef]
- Vandamme, J.; Bonte, J. Systematisation of the Arteries in the Splenic Hilus. Cells Tissues Organs 1986, 125, 217–224. [Google Scholar] [CrossRef]
- Daisy Sahni, A.; Indar Jit, B.; Gupta, C.N.M.; Gupta, D.M.; Harjeet, E. Branches of the splenic artery and splenic arterial segments. Clin. Anat. 2003, 16, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Chaware, P.N.; Belsare, S.M.; Kulkarni, Y.R.; Pandit, S.V.; Ughade, J.M. Variational Anatomy of the Segmental Branches of the Splenic Artery. J. Clin. Diagn. Res. 2012, 6, 336–338. [Google Scholar]
- Garcia-Porrero, J.; Lemes, A. Arterial Segmentation and Subsegmentation in the Human Spleen. Cells Tissues Organs 1988, 131, 276–283. [Google Scholar] [CrossRef]
- Ignatovic, D.; Stimec, B.; Zivanovic, V. The basis for splenic segmental dearterialization: A post-mortem study. Surg. Radiol. Anat. 2004, 27, 15–18. [Google Scholar] [CrossRef]
- Liu, Q.; Lu, J.P.; Wang, F.; Wang, L.; Jin, A.G.; Wang, J.; Tian, J.M. Detection of anomalous splenic artery aneurysms with three-dimensional contrast-enhanced MR angiography. Abdom. Imaging 2008, 34, 772–776. [Google Scholar] [CrossRef]
- Redmond, H.P.; Redmond, J.M.; Rooney, B.P.; Duignan, J.P.; Bouchier-Hayes, D.J. Surgical anatomy of the human spleen. Br. J. Surg. 1989, 76, 198–201. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Training: London, UK, 2023; Available online: https://training.cochrane.org/handbook (accessed on 15 January 2023).
- Greenhalgh, T. How to read a paper: Assessing the methodological quality of published papers. BMJ 1997, 315, 305–308. [Google Scholar] [CrossRef]
- MacDermid, J.C.; Walton, D.M.; Avery, S.; Blanchard, A.; Etruw, E.; McAlpine, C.; Goldsmith, C.H. Measurement Properties of the Neck Disability Index: A Systematic Review. J. Orthop. Sports Phys. Ther. 2009, 39, 400–412. [Google Scholar] [CrossRef]
- Banda, A.B., II. Das Arteriensystem Der Japaner; Hasebe, K., Kyoto, T.D., Eds.; Kaiserlich-Japanische Universitat: Kyoto, Japan, 1928; pp. 20–71. [Google Scholar]
- Chen, H.; Yano, R.; Emura, S.; Shoumura, S. Anatomic variation of the celiac trunk with special reference to hepatic artery patterns. Ann. Anat.-Anat. Anz. 2009, 191, 399–407. [Google Scholar] [CrossRef]
- Sankar, K.D.; Bhanu, P.S.; Susan, P.J. Variant Anatomy of the Celiac Trunk and its Branches. Int. J. Morphol. 2011, 23, 581–584. [Google Scholar] [CrossRef]
- Loukas, M.; Fergurson, A.; Louis, R.G.; Colborn, G.L. Multiple variations of the hepatobiliary vasculature including double cystic arteries, accessory left hepatic artery and hepatosplenic trunk: A case report. Surg. Radiol. Anat. 2006, 28, 525–528. [Google Scholar] [CrossRef]
- Michels, N.A. Variational anatomy of the hepatic, cystic, and retroduodenal arteries. A.M.A. Arch. Surg. 1953, 66, 20–34. [Google Scholar] [CrossRef]
- Sirasanagandla, S.R.; Kumar, N.; Shetty, S.D.; Badagabettu, S.N. Hepatosplenic Trunk Associated with Tortuous Course of Right Hepatic Artery Forming Caterpillar Hump. North Am. J. Med. Sci. 2012, 4, 376–378. [Google Scholar] [CrossRef]
- Bolintineanu, L.A.; Costea, A.N.; Iacob, N.; Pusztai, A.M.; Pleş, H.; Matusz, P. Hepato-spleno-mesenteric trunk, in association with an accessory left hepatic artery, and common trunk of right and left inferior phrenic arteries, independently arising from left gastric artery: Case report using MDCT angiography. Rom. J. Morphol. Embryol. 2019, 60, 1323–1331. [Google Scholar]
- Panagouli, E.; Venieratos, D.; Lolis, E.; Skandalakis, P. Variations in the anatomy of the celiac trunk: A systematic review and clinical implications. Ann. Anat.-Anat. Anz. 2013, 195, 501–511. [Google Scholar] [CrossRef]
- Hemanth, K.; Garg, S.; Yadav, T.D.; Sahni, D.; Singh, R. Hepato-gastro-phrenic trunk and hepato-spleno-mesenteric trunk: A rare anatomic variation. Trop. Gastroenterol. 2011, 32, 56–59. [Google Scholar]
- Varma, K.S.; Pamidi, N.; Vollala, V.R.; Bolla, S.R. Hepato-spleno-mesenteric trunk: A case report. Rom. J. Morphol. Embryol. 2010, 51, 401–402. [Google Scholar]
- Poynter, C.W.M.; Hicks, J.D. Congenital Anomalies of the Arteries and Veins of the Human Body: With Bibliography, 1st ed.; The University Studies of the University of Nebraska: Lincoln, NE, USA, 1922; Volume 22, p. 106. [Google Scholar]
- Michels, N.A. The variational anatomy of the spleen and splenic artery. Am. J. Anat. 1942, 70, 21–72. [Google Scholar] [CrossRef]
- Oliveros Viamontes, G.; Durán Matos, M.; Almaguer Rodríguez, C. Variantes anatómicas de las arterias que irrigan al estómago. Revisión bibliográfica. Rev. Arch. Médico Camagüey 2001, 5, 346–359. [Google Scholar]
- Higashi, N.; Hirai, K. A case of the three branches of the celiac trunk arising directly from the abdominal aorta. Anat. Sci. Int. 1995, 70, 349–352. [Google Scholar]
- Raikos, A.; Paraskevas, G.K.; Natsis, K.; Tzikas, A.; Njau, S.N. Multiple variations in the branching pattern of the abdominal aorta. Rom. J. Morphol. Embryol. 2010, 51, 585–587. [Google Scholar] [PubMed]
- Losanoff, J.E.; Millis, M.J.; Harland, R.C.; Testa, G. Hepato-spleno-mesenteric trunk. J. Am. Coll. Surg. 2007, 204, 511. [Google Scholar] [CrossRef]
- Padmalath, K.; Ramesh, B.R.; Balachandra, N.; Mamatha, Y. Accessory splenic artery from left gastric artery from the left gastric artery. Int. J. Anat. Var. 2010, 3, 106–107. [Google Scholar]
- Iacob, N.; Sas, I.; Joseph, S.C.; Pleş, H.; Miclăuş, G.D.; Matusz, P.; Tubbs, R.S.; Loukas, M. Anomalous pattern of origin of the left gastric, splenic, and common hepatic arteries arising independently from the abdominal aorta. Rom. J. Morphol. Embryol. 2014, 55, 1449–1453. [Google Scholar]
- Covantsev, S.; Alieva, F.; Mulaeva, K.; Mazuruc, N.; Belic, O. Morphological Evaluation of the Splenic Artery, Its Anatomical Variations and Irrigation Territory. Life 2023, 13, 195. [Google Scholar] [CrossRef]
- Manatakis, D.K.; Piagkou, M.; Loukas, M.; Tsiaoussis, J.; Delis, S.G.; Antonopoulos, I.; Chytas, D.; Natsis, K. A systematic review of splenic artery variants based on cadaveric studies. Surg. Radiol. Anat. 2021, 43, 1337–1347. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).