
Association of Ground Reaction Force Measurements in Runners with Symptomatic Iliotibial Band Friction Syndrome: A Cross-Sectional Study
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcomes
2.3. Data Collection
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Recruitment and General Data
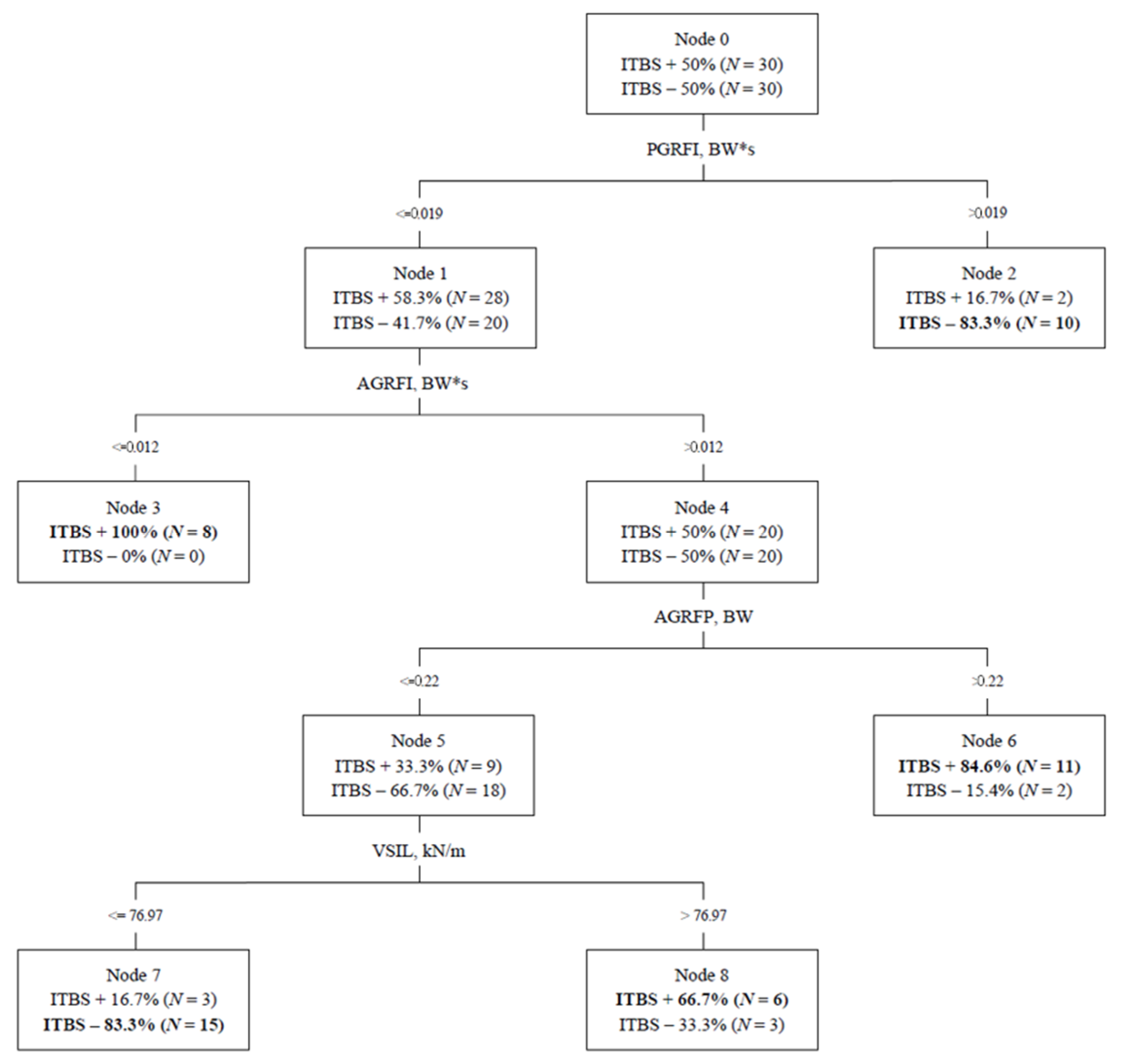
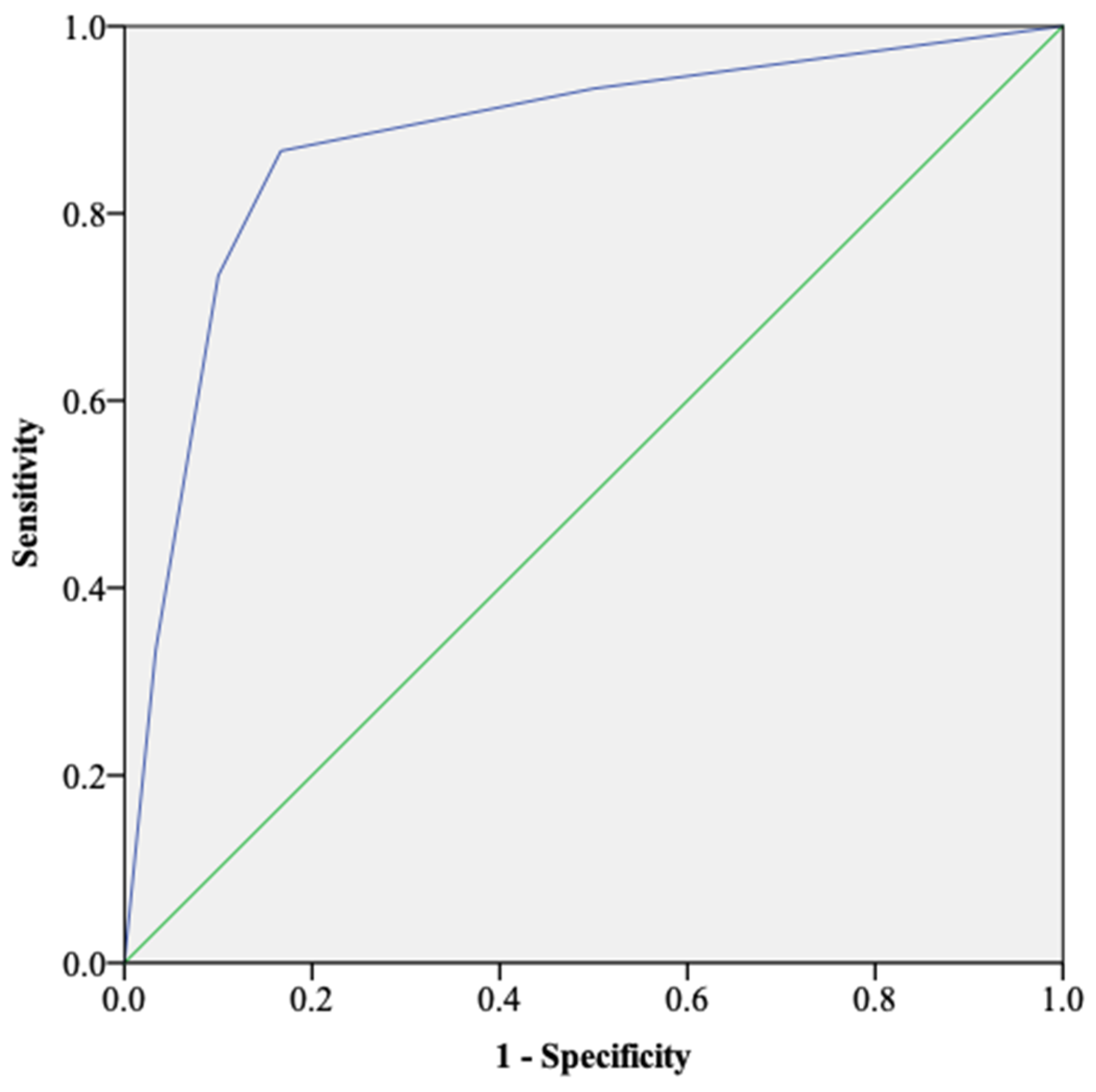
3.2. CART Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vitti, A.; Nikolaidis, P.T.; Villiger, E.; Onywera, V.; Knechtle, B. The “New York City Marathon”: Participation and performance trends of 1.2M runners during half-century. Res. Sport. Med. 2019, 28, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Oswald, F.; Campbell, J.; Williamson, C.; Richards, J.; Kelly, P. A Scoping Review of the Relationship between Running and Mental Health. Int. J. Environ. Res. Public Health 2020, 17, 8059. [Google Scholar] [CrossRef] [PubMed]
- Schnohr, P.; Marott, J.L.; Lange, P.; Jensen, G.B. Longevity in Male and Female Joggers: The Copenhagen City Heart Study. Am. J. Epidemiol. 2013, 177, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Pedisic, Z.; Shrestha, N.; Kovalchik, S.; Stamatakis, E.; Liangruenrom, N.; Grgic, J.; Titze, S.; Biddle, S.J.; Bauman, A.E.; Oja, P. Is running associated with a lower risk of all-cause, cardiovascular and cancer mortality, and is the more the better? A systematic review and meta-analysis. Br. J. Sport. Med. 2019, 54, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Lun, V.; Meeuwisse, W.H.; Stergiou, P.; Stefanyshyn, D. Relation between running injury and static lower limb alignment in recreational runners. Br. J. Sport. Med. 2004, 38, 576–580. [Google Scholar] [CrossRef]
- Kemler, E.; Blokland, D.; Backx, F.; Huisstede, B. Differences in injury risk and characteristics of injuries between novice and experienced runners over a 4-year period. Phys. Sportsmed. 2018, 46, 485–491. [Google Scholar] [CrossRef]
- Videbæk, S.; Bueno, A.M.; Nielsen, R.O.; Rasmussen, S. Incidence of Running-Related Injuries Per 1000 h of running in Different Types of Runners: A Systematic Review and Meta-Analysis. Sport. Med. 2015, 45, 1017–1026. [Google Scholar] [CrossRef]
- Lopes, A.D.; Hespanhol, L.C.; Yeung, S.S.; Costa, L.O.P. What are the Main Running-Related Musculoskeletal Injuries? Sport. Med. 2012, 42, 891–905. [Google Scholar] [CrossRef]
- Taunton, J.E.; Ryan, M.B.; Clement, D.B.; McKenzie, D.C.; Lloyd-Smith, D.R.; Zumbo, B.D. A retrospective case-control analysis of 2002 running injuries. Br. J. Sport. Med. 2002, 36, 95–101. [Google Scholar] [CrossRef]
- Ceyssens, L.; Vanelderen, R.; Barton, C.; Malliaras, P.; Dingenen, B. Biomechanical Risk Factors Associated with Running-Related Injuries: A Systematic Review. Sport. Med. 2019, 49, 1095–1115. [Google Scholar] [CrossRef]
- van der Worp, M.P.; ten Haaf, D.S.M.; van Cingel, R.; de Wijer, A.; Nijhuis-van der Sanden, M.W.; Staal, J.B. Injuries in runners; a systematic review on risk factors and sex differences. PLoS ONE 2015, 10, e0114937. [Google Scholar] [CrossRef] [PubMed]
- Van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.A.; Koes, B.W. Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. Br. J. Sport. Med. 2007, 41, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Saragiotto, B.T.; Yamato, T.P.; Hespanhol Junior, L.C.; Rainbow, M.J.; Davis, I.S.; Lopes, A.D. What are the main risk factors for running-related injuries? Sport. Med. 2014, 44, 1153–1163. [Google Scholar] [CrossRef]
- Hutchinson, L.A.; Lichtwark, G.A.; Willy, R.W.; Kelly, L.A. The Iliotibial Band: A Complex Structure with Versatile Functions. Sport. Med. 2022, 52, 995–1008. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.J.; Kim, S.; Calcei, J.G.; Park, D. Iliotibial band syndrome: Evaluation and management. JAAOS 2011, 19, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, J.; Hayashi, K.; Toumi, H.; Lyons, K.; Bydder, G.; Phillips, N.; Best, T.M.; Benjamin, M. Is iliotibial band syndrome really a friction syndrome? J. Sci. Med. Sport 2007, 10, 74–76. [Google Scholar] [CrossRef]
- Orchard, J.W.; Fricker, P.A.; Abud, A.T.; Mason, B.R. Biomechanics of iliotibial band friction syndrome in runners. Am. J. Sport. Med. 1996, 24, 375–379. [Google Scholar] [CrossRef]
- Messier, S.P.; Edwards, D.G.; Martin, D.F.; Lowery, R.B.; Cannon, D.W.; James, M.K.; Curl, W.W.; Read, H.M., Jr.; Hunter, D.M. Etiology of iliotibial band friction syndrome in distance runners. Med. Sci. Sport. Exerc. 1995, 27, 951–960. [Google Scholar] [CrossRef]
- Fredericson, M.; Wolf, C. Iliotibial band syndrome in runners: Innovations in treatment. Sport. Med. 2005, 35, 451–459. [Google Scholar] [CrossRef]
- Willwacher, S.; Kurz, M.; Robbin, J.; Thelen, M.; Hamill, J.; Kelly, L.; Mai, P. Running-Related Biomechanical Risk Factors for Overuse Injuries in Distance Runners: A Systematic Review Considering Injury Specificity and the Potentials for Future Research. Sport. Med. 2022, 52, 1863–1877. [Google Scholar] [CrossRef]
- van der Worp, M.P.; van der Horst, N.; de Wijer, A.; Backx, F.J.; Nijhuis-van der Sanden, M.W. Iliotibial band syndrome in runners: A systematic review. Sport. Med. 2012, 42, 969–992. [Google Scholar] [CrossRef]
- Johnson, C.D.; Tenforde, A.S.; Outerleys, J.; Reilly, J.; Davis, I.S. Impact-Related Ground Reaction Forces Are More Strongly Associated with Some Running Injuries Than Others. Am. J. Sport. Med. 2020, 48, 3072–3080. [Google Scholar] [CrossRef]
- Suárez, L.B.; Rueda, O.J.; Collazo, G.C.; Veiga, F.S.; Navarro, C.E. Kinematics of recreational runners with iliotibial band injury. J. Hum. Sport Exerc. 2018, 13, 698–709. [Google Scholar]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br. J. Sport. Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, S.T.; Souza, T.R.; Verhagen, E.; van Emmerik, R.; Bittencourt, N.F.N.; Mendonça, L.D.M.; Andrade, A.G.P.; Resende, R.A.; Ocarino, J.M. Sports Injury Forecasting and Complexity: A Synergetic Approach. Sport. Med. 2020, 50, 1757–1770. [Google Scholar] [CrossRef] [PubMed]
- Beals, C.; Flanigan, D. A Review of Treatments for Iliotibial Band Syndrome in the Athletic Population. J. Sport. Med. 2013, 2013, 367169. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Futrell, E.E.; Jamison, S.T.; Tenforde, A.S.; Davis, I.S. Relationships between Habitual Cadence, Footstrike, and Vertical Load Rates in Runners. Med. Sci. Sport. Exerc. 2018, 50, 1837–1841. [Google Scholar] [CrossRef]
- Hollander, K.; Johnson, C.D.; Outerleys, J.; Davis, I.S. Multifactorial Determinants of Running Injury Locations in 550 Injured Recreational Runners. Med. Sci. Sport. Exerc. 2020, 53, 102–107. [Google Scholar] [CrossRef]
- Cavagna, G.A. Force platforms as ergometers. J. Appl. Physiol. 1985, 39, 174–179. [Google Scholar] [CrossRef]
- Chester, R.; Khondoker, M.; Shepstone, L.; Lewis, J.S.; Jerosch-Herold, C. Self-efficacy and risk of persistent shoulder pain: Results of a Classification and Regression Tree (CART) analysis. Br. J. Sport. Med. 2019, 53, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Lemon, S.C.; Roy, J.; Clark, M.A.; Friedmann, P.D.; Rakowski, W. Classification and regression tree analysis in public health: Methodological review and comparison with logistic regression. Ann. Behav. Med. 2003, 26, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.L.M.; Oliveira, R.R.; Nazareno, T.S.; Freitas, L.V.; Mendonça, L.D. Interaction of foot and hip factors identifies Achilles tendinopathy occurrence in recreational runners. Phys. Ther. Sport 2020, 45, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Branco, G.R.; Resende, R.A.; Bittencourt, N.F.N.; Mendonça, L.D. Interaction of hip and foot factors associated with anterior knee pain in mountain bikers. Phys. Ther. Sport 2022, 55, 139–145. [Google Scholar] [CrossRef]
- Fältström, A.; Kvist, J.; Bittencourt, N.F.N.; Mendonça, L.D.; Hägglund, M. Clinical Risk Profile for a Second Anterior Cruciate Ligament Injury in Female Soccer Players After Anterior Cruciate Ligament Reconstruction. Am. J. Sport. Med. 2021, 49, 1421–1430. [Google Scholar] [CrossRef]
- Napier, C.; MacLean, C.L.; Maurer, J.; Taunton, J.E.; Hunt, M.A. Kinetic risk factors of running-related injuries in female recreational runners. Scand. J. Med. Sci. Sport. 2018, 28, 2164–2172. [Google Scholar] [CrossRef]
- Noehren, B.; Schmitz, A.; Hempel, R.; Westlake, C.; Black, W. Assessment of strength, flexibility, and running mechanics in men with iliotibial band syndrome. J. Orthop. Sport. Phys. Ther. 2014, 44, 217–222. [Google Scholar] [CrossRef]
- Baker, R.L.; Souza, R.B.; Rauh, M.J.; Fredericson, M.; Rosenthal, M.D. Differences in Knee and Hip Adduction and Hip Muscle Activation in Runners with and without Iliotibial Band Syndrome. PMR 2018, 10, 1032–1039. [Google Scholar] [CrossRef]
- Almeida, M.O.; Davis, I.S.; Lopes, A.D. Biomechanical Differences of Foot-Strike Patterns During Running: A Systematic Review with Meta-analysis. J. Orthop. Sport. Phys Ther. 2015, 45, 738–755. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (N = 60) | ITBS+ (N = 30) | ITBS− (N = 30) | Mean Difference (95% CI) | p | d |
|---|---|---|---|---|---|---|
| Sex F M | 34 (56.7%) 26 (43.3%) | 15 (50%) 15 (50%) | 11 (36.7%) 19 (63.3%) | - | 0.297 | - |
| Age, years | 33.63 (11.19) | 35.20 (11.49) | 32.07 (10.85) | 3.13 (−2.64 to 8.90) | 0.178 | 0.28 |
| Height, m | 1.69 (0.10) | 1.70 (0.10) | 1.67 (0.10) | 0.03 (−0.02 to 0.08) | 0.300 | 0.30 |
| Weight, kg | 67.81 (12.84) | 66.15 (12.07) | 69.48 (13.56) | −3.33 (−9.96 to 3.31) | 0.320 | 0.26 |
| Body mass index, kg/m2 | 22.95 (2.62) | 22.56 (2.27) | 23.35 (2.92) | −0.79 (−2.14 to 0.55) | 0.487 | 0.30 |
| Self-selected speed, m/s | 2.52 (0.25) | 2.53 (0.33) | 2.51 (0.15) | 0.02 (−0.11 to 0.14) | 0.847 | 0.08 |
| Variables | Total (N = 60) | ITBS+ (N = 30) | ITBS− (N = 30) | Mean Difference (95% CI) | p | d |
|---|---|---|---|---|---|---|
| Ground Reaction Force Impulses, BW*s | ||||||
| Vertical | 0.36 (0.02) | 0.36 (0.01) | 0.36 (0.02) | 0 (−0.009 to 0.013) | 0.836 | - |
| Anterior | 0.015 (0.002) | 0.014 (0.002) | 0.015 (0.001) | −0.001 (−0.001 to 0.001) | 0.303 | 0.50 |
| Posterior | 0.017 (0.002) | 0.016 (0.002) | 0.017 (0.002) | −0.001 (−0.002 to −0.001) | 0.049 * | 0.50 |
| Medial | 0.009 (0.004) | 0.009 (0.004) | 0.009 (0.003) | 0 (−0.002 to 0.002) | 0.858 | - |
| Lateral | 0.002 (0.001) | 0.002 (0.002) | 0.001 (0.001) | 0.001 (−0.001 to 0.001) | 0.086 | 0.63 |
| Instantaneous Loading Rates Peaks, BW/s | ||||||
| Vertical | 67.78 (21.72) | 70.35 (19.35) | 65.20 (23.91) | 5.15 (−6.08 to 16.39) | 0.363 | 0.20 |
| Posterior | 9.81 (3.27) | 9.51 (2.95) | 10.11 (3.59) | −0.60 (−2.29 to 1.10) | 0.359 | 0.18 |
| Medial | 7.86 (3.64) | 7.59 (3.37) | 8.12 (3.93) | −0.53 (−2.42 to 1.36) | 0.756 | 0.14 |
| Lateral | 8.24 (4.20) | 8.34 (3.76) | 8.14 (4.66) | 0.20 (−1.98 to 2.39) | 0.564 | 0.05 |
| Ground Reaction Force Peaks, BW | ||||||
| Vertical | 2.26 (0.20) | 2.25 (0.21) | 2.27 (0.20) | −0.02 (−0.13 to 0.08) | 0.658 | 0.10 |
| Anterior | 0.19 (0.03) | 0.19 (0.04) | 0.20 (0.03) | −0.01 (−0.02 to 0.01) | 0.627 | 0.28 |
| Posterior | 0.25 (0.05) | 0.24 (0.05) | 0.26 (0.05) | −0.02 (−0.04 to 0.01) | 0.168 | 0.40 |
| Medial | 0.09 (0.03) | 0.09 (0.02) | 0.10 (0.03) | −0.01 (−0.02 to 0.01) | 0.779 | 0.39 |
| Lateral | 0.05 (0.03) | 0.06 (0.03) | 0.05 (0.04) | 0.01 (−0.01 to 0.02) | 0.352 | 0.28 |
| Vertical Stiffness at Initial Loading, kN/m | 69.49 (22.13) | 71.95 (21.86) | 67.02 (22.49) | 4.93 (−6.53 to 16.39) | 0.237 | 0.22 |
| Risk Profiles | PR (95% CI) |
|---|---|
| Node 3 Posterior Ground Reaction Force Impulse <= 0.019 BW*s Anterior Ground Reaction Force Impulse <= 0.012 BW*s | - |
| Node 6 Posterior Ground Reaction Force Impulse <= 0.019 BW*s Anterior Ground Reaction Force Impulse > 0.012 BW*s Anterior Ground Reaction Force Peak > 0.22 BW | 8.10 (1.61 to 40.76) * |
| Node 8 Posterior Ground Reaction Force Impulse <= 0.019 BW*s Anterior Ground Reaction Force Impulse > 0.012 BW*s Anterior Ground Reaction Force Peak <= 0.22 BW Vertical Stiffness at Initial Loading > 76.97 kN/m | 2.25 (0.50 to 9.99) |
| Protective Profiles | |
| Node 2 Posterior Ground Reaction Force Impulse > 0.019 BW*s | 0.14 (0.02 to 0.72) * |
| Node 7 Posterior Ground Reaction Force Impulse <= 0.019 BW*s Anterior Ground Reaction Force Impulse > 0.012 BW*s Anterior Ground Reaction Force Peak <= 0.22 BW Vertical Stiffness at Initial Loading <= 76.97 kN/m | 0.11 (0.02 to 0.44) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Souza Júnior, J.R.; Bradach, M.M.; Gaudette, L.W.; Tenforde, A.S. Association of Ground Reaction Force Measurements in Runners with Symptomatic Iliotibial Band Friction Syndrome: A Cross-Sectional Study. Appl. Sci. 2023, 13, 3441. https://doi.org/10.3390/app13063441
de Souza Júnior JR, Bradach MM, Gaudette LW, Tenforde AS. Association of Ground Reaction Force Measurements in Runners with Symptomatic Iliotibial Band Friction Syndrome: A Cross-Sectional Study. Applied Sciences. 2023; 13(6):3441. https://doi.org/10.3390/app13063441
Chicago/Turabian Stylede Souza Júnior, José Roberto, Molly M. Bradach, Logan W. Gaudette, and Adam S. Tenforde. 2023. "Association of Ground Reaction Force Measurements in Runners with Symptomatic Iliotibial Band Friction Syndrome: A Cross-Sectional Study" Applied Sciences 13, no. 6: 3441. https://doi.org/10.3390/app13063441
APA Stylede Souza Júnior, J. R., Bradach, M. M., Gaudette, L. W., & Tenforde, A. S. (2023). Association of Ground Reaction Force Measurements in Runners with Symptomatic Iliotibial Band Friction Syndrome: A Cross-Sectional Study. Applied Sciences, 13(6), 3441. https://doi.org/10.3390/app13063441