
Immediate Effects of Blood Flow Restriction Combined with Neuromuscular Electrical Stimulation in Female Amateur Football Players: A Pilot Trial

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
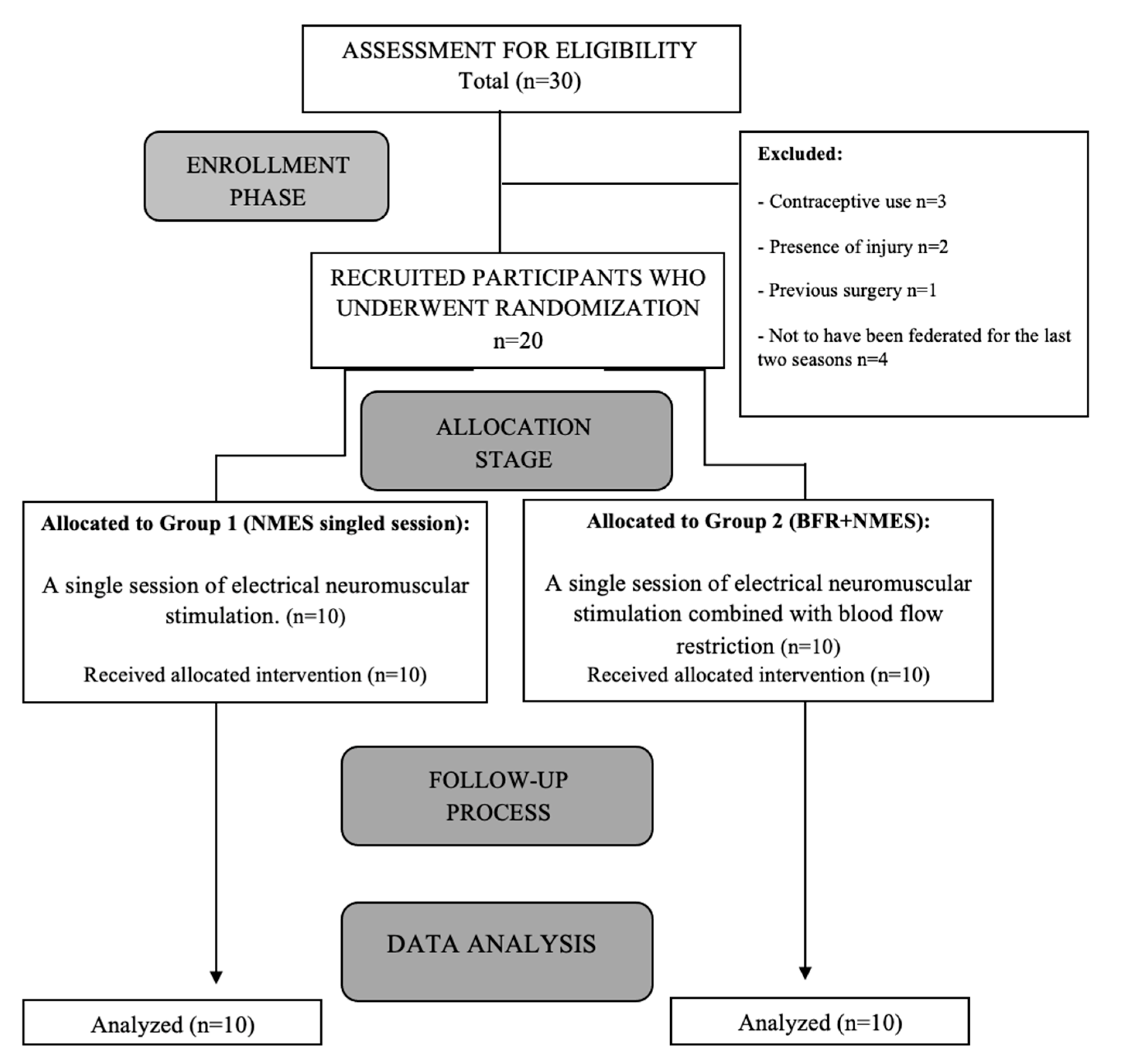
2.1. Design
2.2. Participants
2.3. Randomization
2.4. Procedure
2.5. Outcome Measures
2.5.1. Muscle Strength
2.5.2. Thigh Circumference
2.5.3. Knee Joint Position Sense Test
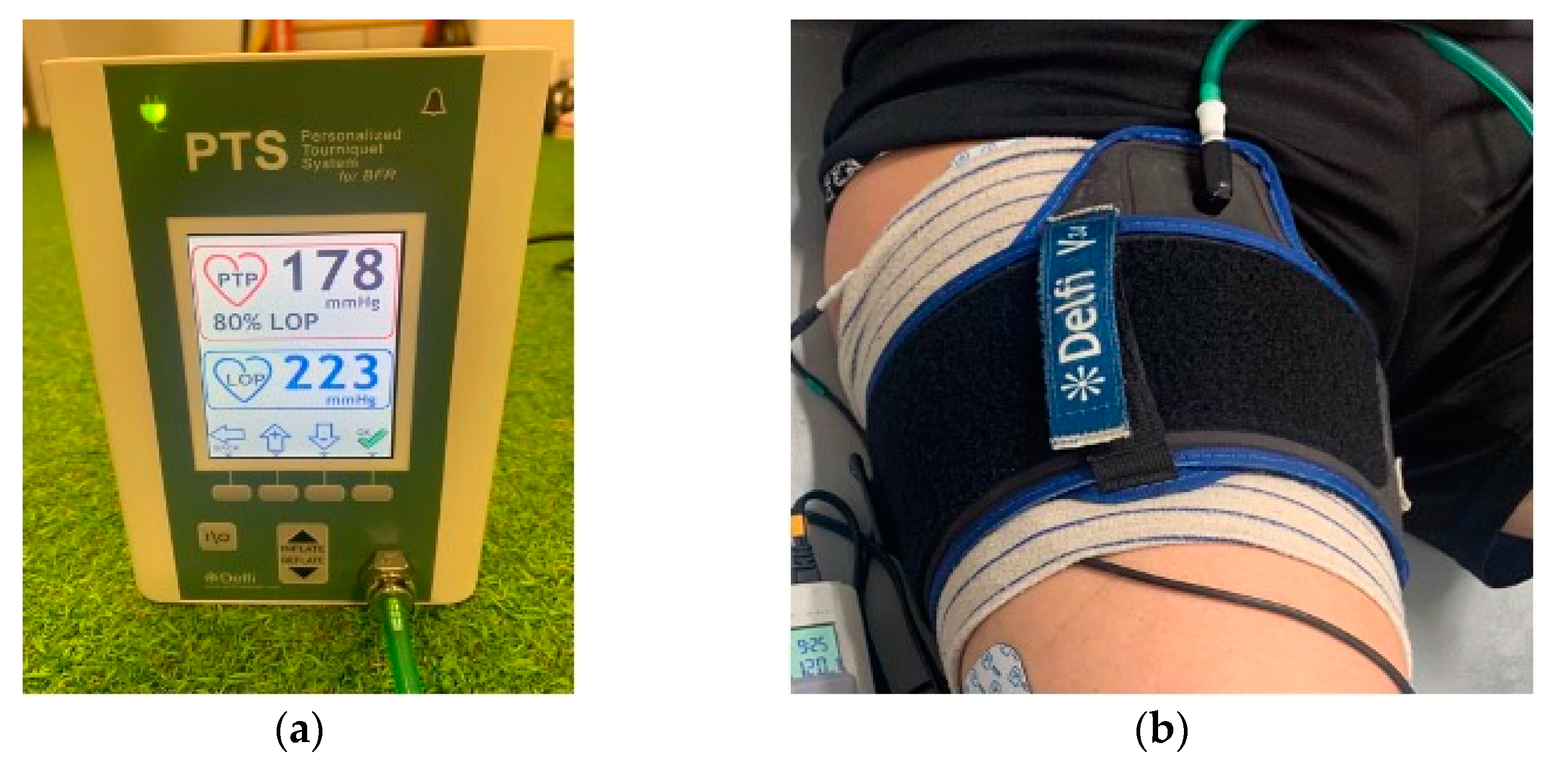
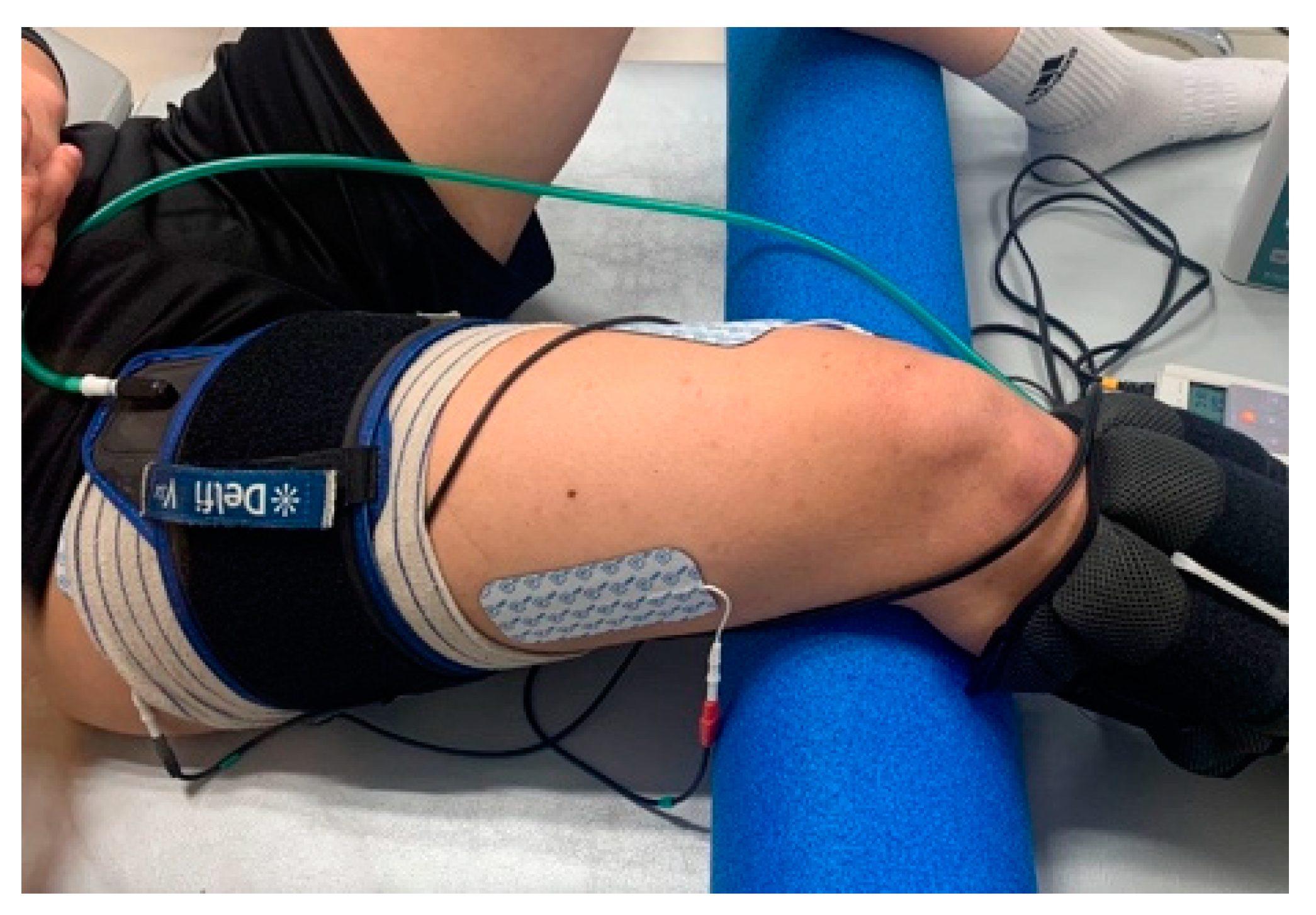
2.6. Intervention
2.7. Sample Size
2.8. Statistical Analysis
3. Results
4. Discussion
4.1. Practical Implications
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Exercise with Blood Flow Restriction: An Updated Evidence-Based Approach for Enhanced Muscular Development. Sports Med. 2015, 45, 313–325. [Google Scholar] [CrossRef]
- Wernbom, M.; Augustsson, J.; Raastad, T. Ischemic Strength Training: A Low-Load Alternative to Heavy Resistance Exercise? Scand. J. Med. Sci. Sports 2008, 18, 401–416. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Wilson, J.M.; Marín, P.J.; Zourdos, M.C.; Bemben, M.G. Low Intensity Blood Flow Restriction Training: A Meta-Analysis. Eur. J. Appl. Physiol. 2012, 112, 1849–1859. [Google Scholar] [CrossRef]
- Farup, J.; De Paoli, F.; Bjerg, K.; Riis, S.; Ringgard, S.; Vissing, K. Blood Flow Restricted and Traditional Resistance Training Performed to Fatigue Produce Equal Muscle Hypertrophy. Scand. J. Med. Sci. Sports 2015, 25, 754–763. [Google Scholar] [CrossRef]
- Saltin, B.; Rådegran, G.; Koskolou, M.D.; Roach, R.C. Skeletal Muscle Blood Flow in Humans and Its Regulation during Exercise. Acta. Physiol. Scand. 1998, 162, 421–436. [Google Scholar] [CrossRef]
- Grant Mouser, J.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Buckner, S.L.; Counts, B.R.; Loenneke, J.P. A Tale of Three Cuffs: The Hemodynamics of Blood Flow Restriction. Eur. J. Appl. Physiol. 2017, 117, 1493–1499. [Google Scholar] [CrossRef]
- Credeur, D.P.; Hollis, B.C.; Welsch, M.A. Effects of Handgrip Training with Venous Restriction on Brachial Artery Vasodilation. Med. Sci. Sports Exerc. 2010, 42, 1296–1302. [Google Scholar] [CrossRef]
- Natsume, T.; Ozaki, H.; Saito, A.I.; Abe, T.; Naito, H. Effects of Electrostimulation with Blood Flow Restriction on Muscle Size and Strength. Med. Sci. Sports Exerc. 2015, 47, 2621–2627. [Google Scholar] [CrossRef]
- Slysz, J.T.; Burr, J.F. The Effects of Blood Flow Restricted Electrostimulation on Strength and Hypertrophy. J. Sport Rehabil. 2018, 27, 257–262. [Google Scholar] [CrossRef]
- Cancio, J.M.; Sgromolo, N.M.; Rhee, P.C. Blood Flow Restriction Therapy after Closed Treatment of Distal Radius Fractures. J. Wrist Surg. 2019, 8, 288–294. [Google Scholar] [CrossRef]
- McEwen, J.A.; Owens, J.G.; Jeyasurya, J. Why Is It Crucial to Use Personalized Occlusion Pressures in Blood Flow Restriction (BFR) Rehabilitation? J. Med. Biol. Eng. 2019, 39, 173–177. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Timmons, M.K.; Dolbow, D.R.; Bengel, J.; Fugate-Laus, K.C.; Michener, L.A.; Gater, D.R. Electrical Stimulation and Blood Flow Restriction Increase Wrist Extensor Cross-Sectional Area and Flow Mediated Dilation Following Spinal Cord Injury. Eur. J. Appl. Physiol. 2016, 116, 1231–1244. [Google Scholar] [CrossRef]
- Wortman, R.; Brown, S.; Savage-Elliott, I.; Finley, Z.; Mulcahey, M. Blood Flow Restriction Training for Athletes: A Systematic Review. Am. J. Sports Med. 2020, 49, 1938–1944. [Google Scholar] [CrossRef]
- Luebbers, P.E.; Fry, A.C.; Kriley, L.M.; Butler, M.S. The Effects of a 7-Week Practical Blood Flow Restriction Program on Well-Trained Collegiate Athletes. J. Strength Cond. Res. 2014, 28, 2270–2280. [Google Scholar] [CrossRef]
- Yasuda, T.; Loenneke, J.P.; Thiebaud, R.S.; Abe, T. Effects of Blood Flow Restricted Low-Intensity Concentric or Eccentric Training on Muscle Size and Strength. PLoS ONE 2012, 7, E52843. [Google Scholar] [CrossRef]
- Yasuda, T.; Brechue, W.F.; Fujita, T.; Shirakawa, J.; Sato, Y.; Abe, T. Muscle Activation during Low-Intensity Muscle Contractions with Restricted Blood Flow. J. Sports Sci. 2009, 27, 479–489. [Google Scholar] [CrossRef]
- Queiros, V.; Dantas, M.; Neto, G.; Silva, L.; Assis, M.; Almeida-Neto, P.; Dantas, P.; Cabral, B. Application and Side Effects of Blood Flow Restriction Technique. Medicine 2021, 100, e25794. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Black, C.D.; Elder, C.P.; Dudley, G.A. Effects of Electrical Stimulation Parameters on Fatigue in Skeletal Muscle. J. Orthop. Sports Phys. Ther. 2009, 39, 684–692. [Google Scholar] [CrossRef]
- Takahashi, M.; Takeda, K.; Otaka, Y.; Osu, R.; Hanakawa, T.; Gouko, M.; Ito, K. Event-Related Desynchronization-Modulated Functional Electrical Stimulation System for Stroke Rehabilitation: A Feasibility Study. J. Neuroeng. Rehabil. 2012, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schardong, J.; Dipp, T.; Bozzeto, C.B.; da Silva, M.G.; Baldissera, G.L.; Ribeiro, R.D.C.; Valdemarca, B.P.; do Pinho, A.S.; Sbruzzi, G.; Plentz, R.D.M. Effects of Intradialytic Neuromuscular Electrical Stimulation on Strength and Muscle Architecture in Patients with Chronic Kidney Failure: Randomized Clinical Trial. Artif. Organs 2017, 41, 1049–1058. [Google Scholar] [CrossRef]
- Erickson, L.N.; Hickey Lucas, K.C.; Davis, K.A.; Jacobs, C.A.; Thompson, K.L.; Hardy, P.A.; Andersen, A.H.; Fry, C.S.; Noehren, B.W. Effect of Blood Flow Restriction Training on Quadriceps Muscle Strength, Morphology, Physiology, and Knee Biomechanics Before and After Anterior Cruciate Ligament Reconstruction: Protocol for a Randomized Clinical Trial. Phys. Ther. 2019, 99, 1010–1019. [Google Scholar] [CrossRef] [PubMed]
- Head, P.; Waldron, M.; Theis, N.; Patterson, S.D. Acute Neuromuscular Electrical Stimulation (NMES) With Blood Flow Restriction: The Effect of Restriction Pressures. J. Sport Rehabil. 2020, 30, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Wohlfahrt, H.W.; Haensel, L.; Mithoefer, K.; Ekstrand, J.; English, B.; McNally, S. Terminology and Classification of Muscle Injuries in Sport: The Munich Consensus Statement. Br. J. Sports Med. 2013, 47, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.; Aitchison, T.; Henderson, E.; Christie, J.; Zare, S.; McMurray, J.; Dargie, H. A Comparison of the Reproducibility and the Sensitivity to Change of Visual Analogue Scales, Borg Scales, and Likert Scales in Normal Subjects during Submaximal Exercise. Chest 1999, 116, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, D.; Cahalane, E.; Conroy, R.; Fitzgerald, D.; Hardiman, O. Maximum Voluntary Isometric Contraction: Reference Values and Clinical Application. Amyotroph. Lateral. Scler. 2007, 8, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.C.P.; Caserotti, P.; Carvalho, C.M.P.; Abade, E.A.; Sampaio, A.J.E. Reliability of Concentric, Eccentric and Isometric Knee Extension and Flexion When Using the REV9000 Isokinetic Dynamometer. J. Hum. Kinet. 2013, 37, 47–53. [Google Scholar] [CrossRef]
- Chamorro, C.; Armijo-Olivo, S.; De La Fuente, C.; Fuentes, J.; Chirosa, L.J. Absolute Reliability and Concurrent Validity of Hand Held Dynamometry and Isokinetic Dynamometry in the Hip, Knee and Ankle Joint: Systematic Review and Meta-Analysis. Open Med. Wars 2017, 12, 359–375. [Google Scholar] [CrossRef] [PubMed]
- Zaharieva, E. Asymmetry of Limb Circumferences in Female Athletes. In The Female Athlete; Karger Publishers: Basel, Switzerland, 1981; Volume 15, pp. 142–149. [Google Scholar]
- Santonja Medina, F.; Alberto Peña Ramírez, W.; Medina Leal, D.; Ferrer-López, V. Metodología y Fiabilidad de La Medición Del Perímetro de Muslo. Rev. Act. Fis Des. Hum. 2012, 4, 150–154. [Google Scholar]
- Bragança, S.; Arezes, P.; Carvalho, M.; Ashdown, S.P.; Castellucci, I.; Leão, C. A Comparison of Manual Anthropometric Measurements with Kinect-Based Scanned Measurements in Terms of Precision and Reliability. Work 2018, 59, 325–339. [Google Scholar] [CrossRef]
- Salgado, E.; Ribeiro, F.; Oliveira, J. Joint-Position Sense Is Altered by Football Pre-Participation Warm-up Exercise and Match Induced Fatigue. J. Knee 2005, 22, 243–248. [Google Scholar] [CrossRef]
- Ferreira, A.G.; Duarte, M.; Maldonado, E.P.; Burke, T.N.; Marques, A.P. Postural Assessment Software (PAS/SAPO): Vadilidation and Reliability. Clinics 2010, 65, 675–681. [Google Scholar] [CrossRef] [PubMed]
- De Almeida Paz, I.; Rigo, G.T.; Sgarioni, A.; Baroni, B.M.; Frasson, V.B.F.; Vaz, M.A. Alternating Current Is More Fatigable Than Pulsed Current in People Who Are Healthy: A Double-Blind, Randomized Crossover Trial. Phys. Ther. 2021, 101, Pzab056. [Google Scholar] [CrossRef]
- Tennent, D.J.; Hylden, C.M.; Johnson, A.E.; Burns, T.C.; Wilken, J.M.; Owens, J.G. Blood Flow Restriction Training After Knee Arthroscopy: A Randomized Controlled Pilot Study. Clin. J. Sport Med. 2017, 27, 245–252. [Google Scholar] [CrossRef]
- Callanan, M.C.; Plummer, H.A.; Chapman, G.L.; Opitz, T.J.; Rendos, N.K.; Anz, A.W. Blood Flow Restriction Training Using the Delfi System Is Associated with a Cellular Systemic Response. Arthrosc. Sports Med. Rehabil. 2020, 27, E189–E198. [Google Scholar] [CrossRef]
- Madarame, H.; Kurano, M.; Takano, H.; Iida, H.; Sato, Y.; Ohshima, H.; Abe, T.; Ishii, N.; Morita, T.; Nakajima, T. Effects of Low-Intensity Resistance Exercise with Blood Flow Restriction on Coagulation System in Healthy Subjects. Clin. Physiol. Funct. Imaging 2010, 30, 210–213. [Google Scholar] [CrossRef]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R.; Beck, B.; Bennell, K.; Brosseau, L.; Costa, L.; Cramp, F.; Cup, E. Consensus on Exercise Reporting Template (CERT): Modified Delphi Study. Phys. Ther. 2016, 96, 1514–1524. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences Lawrence Earlbaum Associates; Academic Press: Cambridge, MA, USA, 1988. [Google Scholar]
- Beato, M.; Maroto-Izquierdo, S.; Turner, A.N.; Bishop, C. Implementing Strength Training Strategies for Injury Prevention in Soccer: Scientific Rationale and Methodological Recommendations. Int. J. Sports Physiol. Perform. 2021, 16, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Konrad, A.; Kasahara, K.; Yoshida, R.; Yahata, K.; Sato, S.; Murakami, Y.; Aizawa, K.; Nakamura, M. Relationship between Eccentric-Exercise-Induced Loss in Muscle Function to Muscle Soreness and Tissue Hardness. Healthcare 2022, 10, 96. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A. Physiological and Methodological Considerations for the Use of Neuromuscular Electrical Stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–239. [Google Scholar] [CrossRef]
- Umbel, J.D.; Hoffman, R.L.; Dearth, D.J.; Chleboun, G.S.; Manini, T.M.; Clark, B.C. Delayed-Onset Muscle Soreness Induced by Low-Load Blood Flow-Restricted Exercise. Eur. J. Appl. Physiol. 2009, 107, 687–695. [Google Scholar] [CrossRef]
- Wernbom, M.; Paulsen, G.; Nilsen, T.S.; Hisdal, J.; Raastad, T. Contractile Function and Sarcolemmal Permeability after Acute Low-Load Resistance Exercise with Blood Flow Restriction. Eur. J. Appl. Physiol. 2012, 112, 2051–2063. [Google Scholar] [CrossRef] [PubMed]
- Egner, I.M.; Bruusgaard, J.C.; Eftestøl, E.; Gundersen, K. A Cellular Memory Mechanism Aids Overload Hypertrophy in Muscle Long after an Episodic Exposure to Anabolic Steroids. J. Physiol. 2013, 591, 6221–6230. [Google Scholar] [CrossRef]
- Pedersen, J.; Lonn, J.; Hellstrom, F.; Djupsjobacka, M.; Johansson, H. Localized Muscle Fatigue Decreases the Acuity of the Movement Sense in the Human Shoulder. Med. Sci. Sports Exerc. 1999, 31, 1047–1052. [Google Scholar] [CrossRef]
- Miura, K.; Ishibashi, Y.; Tsuda, E.; Okamura, Y.; Otsuka, H.; Toh, S. The Effect of Local and General Fatigue on Knee Proprioception. Arthroscopy 2004, 20, 414–418. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Load | 20% of MVCC |
| Volume | 75 repetitions in 4 sets: 30-15-15-15. |
| Rest periods | 30 s between sets, without stopping the application of techniques. |
| Total Sample (n = 20) | NMES Group (n = 10) | NMES + BFR (n = 10) | p Value * | |
|---|---|---|---|---|
| Age (years) | 20.4 ± 2.58 | 20.5 ± 3 | 20.3 ± 2.32 | 0.87 |
| Weight (kg) | 52 ± 0 | 52 ± 0 | 52 ± 0 | 0.87 |
| Height (cm) | 1.64 ± 0.76 | 1.64 ± 0.73 | 1.64 ± 0.82 | |
| BMI (kg/m2) | 7.05 ± 1.89 | 22.11 ± 2.43 | 21.37 ± 1.13 | 0.4 |
| Exercise (h/week) | 7.05 ± 2.93 | 7.2 ± 3.01 | 6.9 ± 3 | 0.83 |
| KJPS 90° Seated (°) | 88.79 ± 8.56 | 86.13 ± 9.08 | 91.45 ± 7.53 | 0.17 |
| KJPS 90° Prone (°) | 81.32 ± 9.74 | 79.19 ± 11.22 | 83.45 ± 8.03 | 0.34 |
| KJPS 135° Seated (°) | 143.48 ± 11.56 | 148.06 ± 5.84 | 138.89 ± 14.18 | 0.06 |
| KJPS 135° Prone (°) | 135.39 ± 6.33 | 134.63 ± 6.75 | 136.15 ± 6.14 | 0.61 |
| Thigh circumference 5 (cm) | 41.3 ± 3.76 | 41.75 ± 4.39 | 40.85 ± 3.17 | 0.61 |
| Thigh circumference 10 (cm) | 45.95 ± 4.37 | 46.65 ± 5.18 | 45.25 ± 3.52 | 0.49 |
| Thigh circumference 15 (cm) | 50.56 ± 4.51 | 50.77 ± 5.34 | 50.35 ± 3.79 | 0.84 |
| Thigh circumference 20 (cm) | 54.81 ± 4.23 | 54.82 ± 5.07 | 54.8 ± 3.47 | 0.99 |
| MVEC (N) | 207.3 ± 76.8 | 204.7 ± 51.1 | 215 ± 35.4 | 0.77 |
| MVCC (N) | 209.9 ± 43.1 | 201.9 ± 63.1 | 212.6 ± 91.8 | 0.61 |
| Group | Baseline | Post-Intervention | Pre-/Post-Differences | Between-Group Mean Changes Post-Intervention | |
|---|---|---|---|---|---|
| KJPS 90° seated (°) | NMES | 86.13 ± 9.08 | 85.33 ± 8.79 | 0.79 [−6.08–7.66] | 6.58 [−15.08–1.93] |
| NMES + BFR | 91.45 ± 7.53 | 91.92 ± 9.32 | −0.47 [−6.59–5.64] | ||
| KJPS 90° prone (°) | NMES | 79.19 ± 11.22 | 76.85 ± 10.25 | 2.34 [−4.05–8.72] | −4.54 [−13.99–4.9] |
| NMES + BFR | 83.45 ± 8.03 | 81.39 ± 9.86 | 2.06 [−3.57–7.69] | ||
| KJPS 135° seated (°) | NMES | 148.06 ± 5.84 | 146.18 ± 8.25 | 1.88 [−4.35–8.12] | 3.45 [−3.77–10.66] |
| NMES + BFR | 138.89 ± 14.18 | 142.73 ± 7.07 | −3.84 [−15.72–8.05] | ||
| KJPS 135° prone (°) | NMES | 134.63 ± 6.75 | 136.85 ± 8.86 | −2.21 [−7.36–2.94] | 3.64 [−4.19–11.48] |
| NMES + BFR | 136.15 ± 6.14 | 133.2 ± 7.79 | 2.94 [−1.13–7.02] | ||
| Thigh circumference 5 (cm) | NMES | 41.75 ± 4.39 | 42.35 ± 4.55 | −0.6 [−0.93–−0.27] * | 0.6 [−3.1–4.3] |
| NMES + BFR | 40.85 ± 3.17 | 41.75 ± 3.22 | −0.9 [−1.23–−0.57] * | ||
| Thigh circumference 10 (cm) | NMES | 46.65 ± 5.18 | 47.35 ± 5.27 | −0.7 [−0.95–−0.45] * | 1.43 [−2.72–5.58] |
| NMES + BFR | 45.25 ± 3.53 | 45.92 ± 3.36 | −0.67 [−0.99–−0.35] * | ||
| Thigh circumference 15 (cm) | NMES | 50.77 ± 5.34 | 51.55 ± 5.18 | −0.78 [−1.27–−0.29] * | 0.38 [−3.9–4.66] |
| NMES + BFR | 50.35 ± 3.79 | 51.17 ± 3.83 | −0.82 [−1.09–−0.55] * | ||
| Thigh circumference 20 (cm) | NMES | 54.82 ± 5.07 | 55.4 ± 5.31 | −0.58 [−0.92–−0.24] * | −0.25 [−4.42–3.92] |
| NMES + BFR | 54.8 ± 3.47 | 55.65 ± 3.34 | −0.85 [−1.09–−0.61] * | ||
| MVEC (N) | NMES | 204.7 ± 51.2 | 218 ± 46.3 | −13.3 [−28.3–1.8] | 11 [−61.8–83.8] |
| NMES + BFR | 215.0 ± 35.4 | 205.9 ± 41.8 | 9.1 [−3.8–22] | ||
| MVCC (N) | NMES | 201.9 ± 63.1 | 220.1 ± 76.3 | −18.2 [−57.7–21.3] | 12.1 [−29.4–53.6] |
| NMES + BFR | 212.6 ± 91.8 | 209.1 ± 78.5 | 3.5 [−25.1–32.1] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afán-Argüín, I.; Fernández-Morales, C.; Espejo-Antúnez, L.; Albornoz-Cabello, M.; León-Morillas, F.; Cardero-Durán, M.d.l.Á. Immediate Effects of Blood Flow Restriction Combined with Neuromuscular Electrical Stimulation in Female Amateur Football Players: A Pilot Trial. Appl. Sci. 2023, 13, 13131. https://doi.org/10.3390/app132413131
Afán-Argüín I, Fernández-Morales C, Espejo-Antúnez L, Albornoz-Cabello M, León-Morillas F, Cardero-Durán MdlÁ. Immediate Effects of Blood Flow Restriction Combined with Neuromuscular Electrical Stimulation in Female Amateur Football Players: A Pilot Trial. Applied Sciences. 2023; 13(24):13131. https://doi.org/10.3390/app132413131
Chicago/Turabian StyleAfán-Argüín, Irene, Carlos Fernández-Morales, Luis Espejo-Antúnez, Manuel Albornoz-Cabello, Felipe León-Morillas, and María de los Ángeles Cardero-Durán. 2023. "Immediate Effects of Blood Flow Restriction Combined with Neuromuscular Electrical Stimulation in Female Amateur Football Players: A Pilot Trial" Applied Sciences 13, no. 24: 13131. https://doi.org/10.3390/app132413131
APA StyleAfán-Argüín, I., Fernández-Morales, C., Espejo-Antúnez, L., Albornoz-Cabello, M., León-Morillas, F., & Cardero-Durán, M. d. l. Á. (2023). Immediate Effects of Blood Flow Restriction Combined with Neuromuscular Electrical Stimulation in Female Amateur Football Players: A Pilot Trial. Applied Sciences, 13(24), 13131. https://doi.org/10.3390/app132413131