
Stretching and Eccentric Exercises Normalize Gait Parameters in Gastrocnemius Tightness Subjects

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria
2.2. Stanish Protocol
2.3. Examinations
2.4. Assessment Criteria
2.5. Statistics
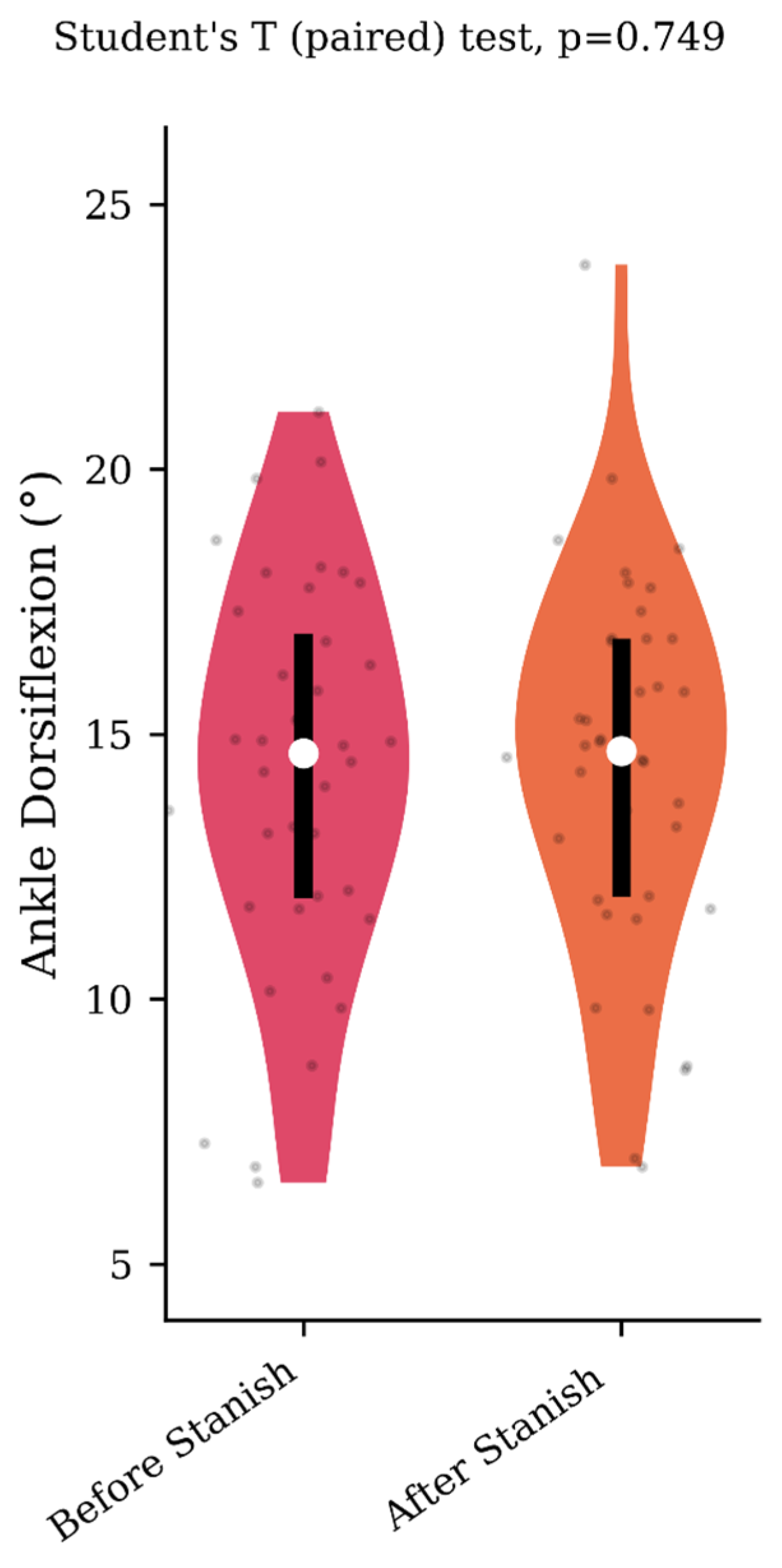
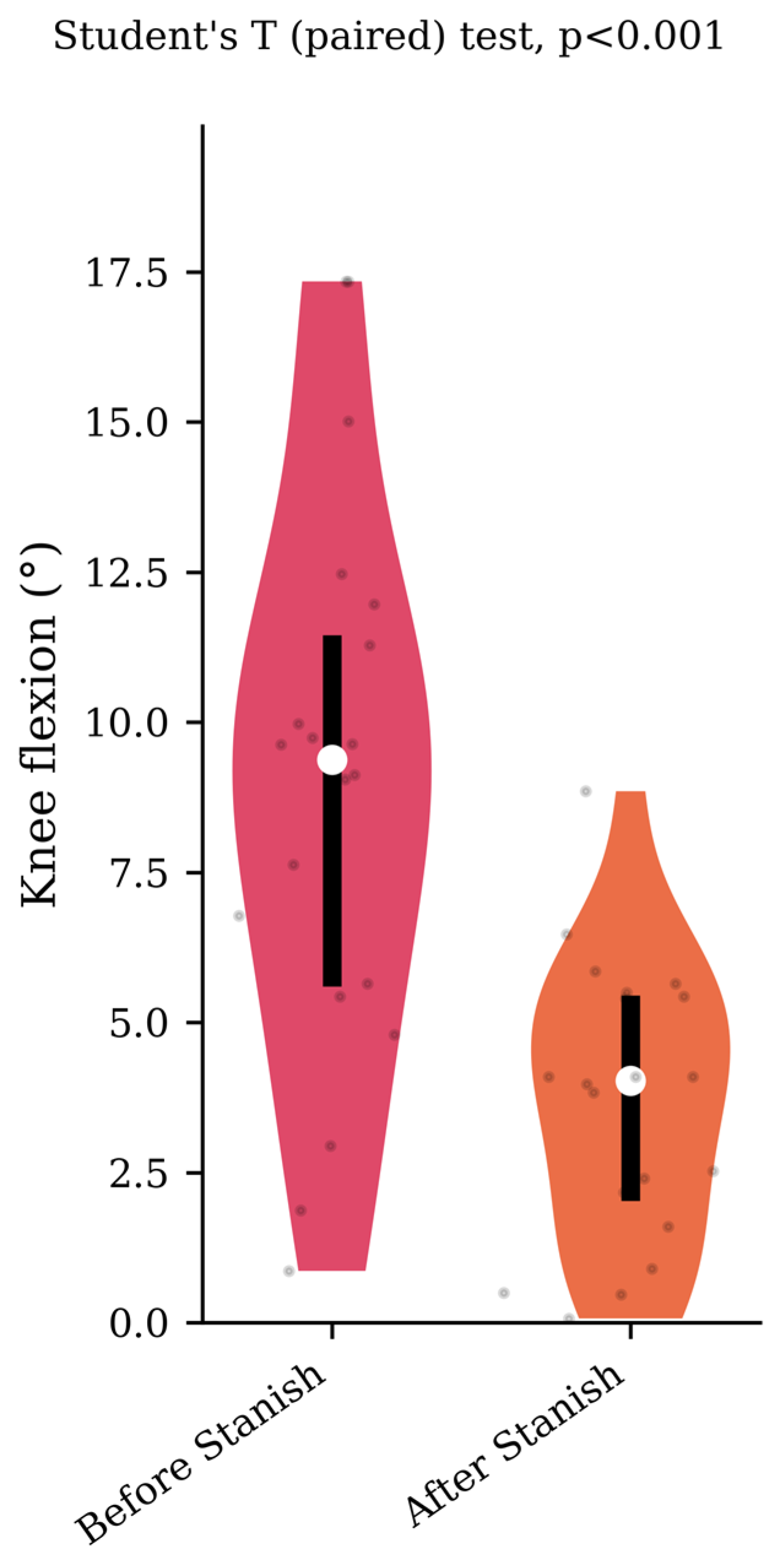
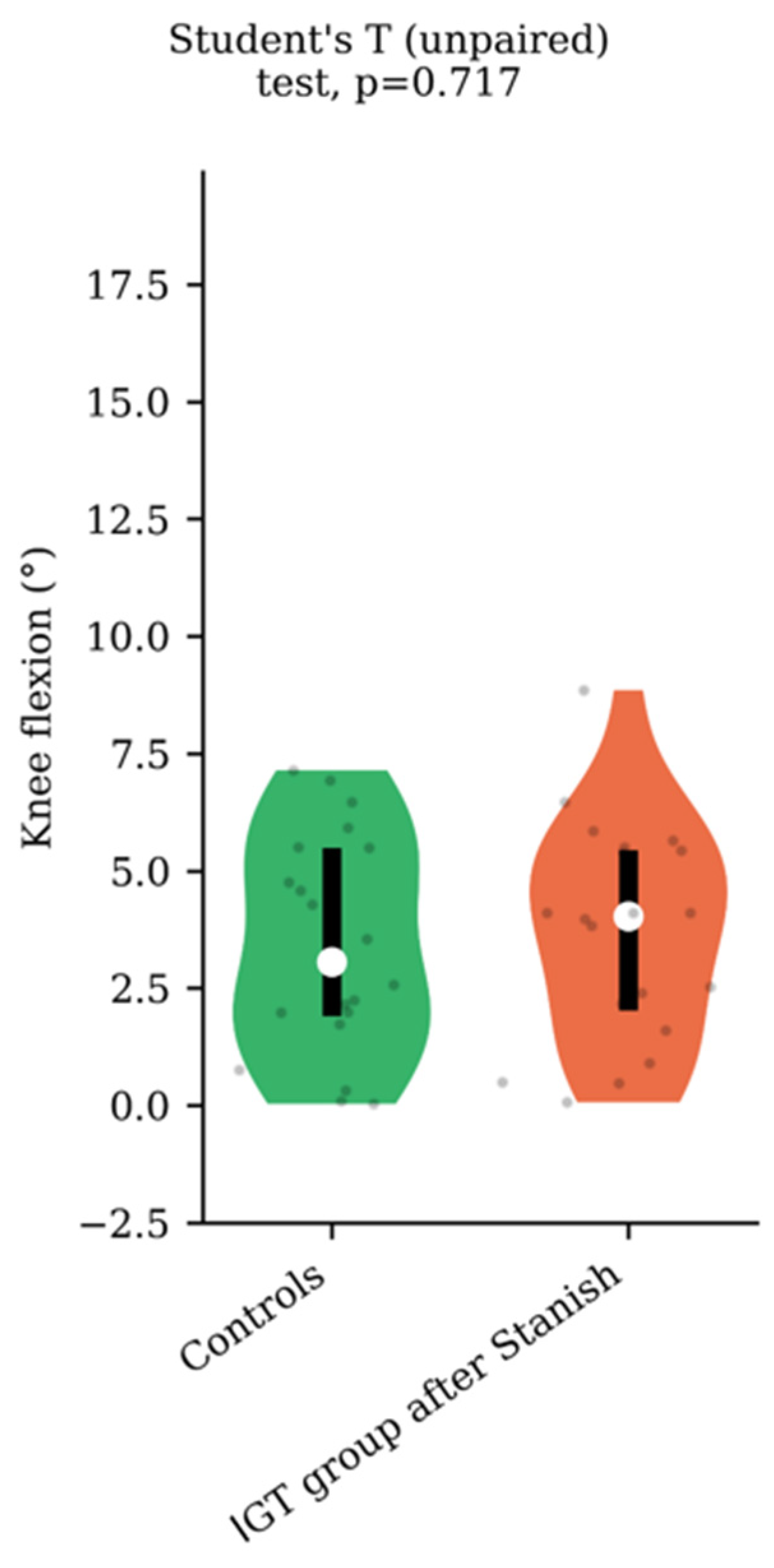
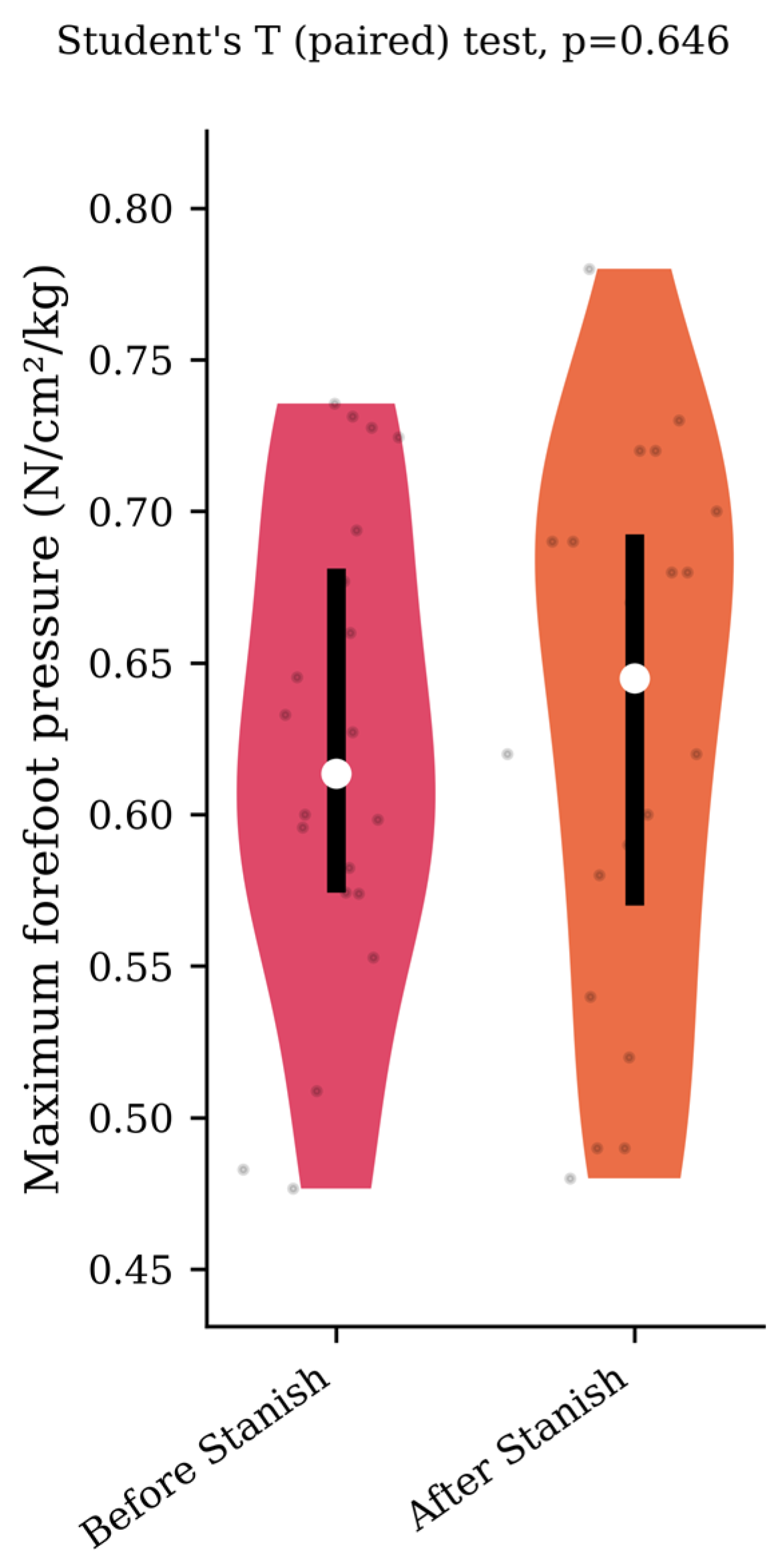
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DiGiovanni, C.W.; Kuo, R.; Tejwani, N.; Price, R.; Hansen, S.T.J.; Cziernecki, J.; Sangeorzan, B.J. Isolated Gastrocnemius Tightness. JBJS 2002, 84, 962. [Google Scholar] [CrossRef] [PubMed]
- Jastifer, J.R.; Marston, J. Gastrocnemius Contracture in Patients With and Without Foot Pathology. Foot Ankle Int. 2016, 37, 1165–1170. [Google Scholar] [CrossRef]
- Antończak, P.P.; Hartman-Petrycka, M.; Garncarczyk, A.; Adamczyk, K.; Wcisło-Dziadecka, D.; Błońska-Fajfrowska, B. The Effect of Callus and Corns Removal Treatments on Foot Geometry Parameters, Foot Pressure, and Foot Pain Reduction in Women. Appl. Sci. 2023, 13, 4319. [Google Scholar] [CrossRef]
- Chan, O.; Malhotra, K.; Buraimoh, O.; Cullen, N.; Welck, M.; Goldberg, A.; Singh, D. Gastrocnemius Tightness: A Population Based Observational Study. Foot Ankle Surg. 2019, 25, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, C. Rôle pathogénique de la brièveté du gastrocnémien dans les métatarsalgies. Médecine Chir. Pied 2004, 20, 3–5. [Google Scholar] [CrossRef]
- Hill, R.S. Ankle Equinus. Prevalence and Linkage to Common Foot Pathology. J. Am. Podiatr. Med. Assoc. 1995, 85, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Cazeau, C.; Stiglitz, Y. Effects of Gastrocnemius Tightness on Forefoot During Gait. Foot Ankle Clin. 2014, 19, 649–657. [Google Scholar] [CrossRef]
- Chen, G.; Liao, Q.; Luo, W.; Li, K.; Zhao, Y.; Zhong, D. Triceps-Sparing versus Olecranon Osteotomy for ORIF: Analysis of 67 Cases of Intercondylar Fractures of the Distal Humerus. Injury 2011, 42, 366–370. [Google Scholar] [CrossRef]
- Crisco, J.J.; Halilaj, E.; Moore, D.C.; Patel, T.; Weiss, A.-P.C.; Ladd, A.L. In Vivo Kinematics of the Trapeziometacarpal Joint during Thumb Extension-Flexion and Abduction-Adduction. J. Hand Surg. 2015, 40, 289–296. [Google Scholar] [CrossRef]
- Lavery, L.A.; Armstrong, D.G.; Boulton, A.J.M. Ankle Equinus Deformity and Its Relationship to High Plantar Pressure in a Large Population with Diabetes Mellitus. J. Am. Podiatr. Med. Assoc. 2002, 92, 479–482. [Google Scholar] [CrossRef]
- El-Hawary, R.; Karol, L.A.; Jeans, K.A.; Richards, B.S. Gait Analysis of Children Treated for Clubfoot with Physical Therapy or the Ponseti Cast Technique. J. Bone Joint Surg. Am. 2008, 90, 1508–1516. [Google Scholar] [CrossRef] [PubMed]
- Lofterød, B.; Fosdahl, M.A.; Terjesen, T. Can Persistent Drop Foot After Calf Muscle Lengthening Be Predicted Preoperatively? J. Foot Ankle Surg. 2009, 48, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Chimera, N.J.; Castro, M.; Davis, I.; Manal, K. The Effect of Isolated Gastrocnemius Contracture and Gastrocnemius Recession on Lower Extremity Kinematics and Kinetics during Stance. Clin. Biomech. 2012, 27, 917–923. [Google Scholar] [CrossRef] [PubMed]
- You, J.-Y.; Lee, H.-M.; Luo, H.-J.; Leu, C.-C.; Cheng, P.-G.; Wu, S.-K. Gastrocnemius Tightness on Joint Angle and Work of Lower Extremity during Gait. Clin. Biomech. 2009, 24, 744–750. [Google Scholar] [CrossRef]
- Lalevée, M.; Menez, C.; Roussignol, X.; Hue, A.G.; Dujardin, F.; Dodelin, D.; Dechelotte, B.; Lintz, F. A Comparative Study between Isolated Gastrocnemius Tightness Patients and Controls by Quantitative Gait Analysis and Baropodometry. Foot Ankle Surg. 2021, 27, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Cychosz, C.C.; Phisitkul, P.; Belatti, D.A.; Glazebrook, M.A.; DiGiovanni, C.W. Gastrocnemius Recession for Foot and Ankle Conditions in Adults: Evidence-Based Recommendations. Foot Ankle Surg. 2015, 21, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Knapik, D.M.; LaTulip, S.; Salata, M.J.; Voos, J.E.; Liu, R.W. Impact of Routine Gastrocnemius Stretching on Ankle Dorsiflexion Flexibility and Injury Rates in High School Basketball Athletes. Orthop. J. Sports Med. 2019, 7, 2325967119836774. [Google Scholar] [CrossRef] [PubMed]
- Barouk, P. Technique, Indications, and Results of Proximal Medial Gastrocnemius Lengthening. Foot Ankle Clin. 2014, 19, 795–806. [Google Scholar] [CrossRef] [PubMed]
- Riiser, M.O.; Husebye, E.E.; Hellesnes, J.; Molund, M. Outcomes After Proximal Medial Gastrocnemius Recession and Stretching vs Stretching as Treatment of Chronic Plantar Fasciitis at 6-Year Follow-Up. Foot Ankle Int. 2023, 10711007231205559, Epub ahead of print. [Google Scholar] [CrossRef]
- Stanish, W.D.; Rubinovich, R.M.; Curwin, S. Eccentric Exercise in Chronic Tendinitis. Clin. Orthop. 1986, 208, 65–68. [Google Scholar] [CrossRef]
- Fyfe, I.; Stanish, W.D. The Use of Eccentric Training and Stretching in the Treatment and Prevention of Tendon Injuries. Clin. Sports Med. 1992, 11, 601–624. [Google Scholar] [CrossRef] [PubMed]
- Barouk, P.; Barouk, L.S. Clinical Diagnosis of Gastrocnemius Tightness. Foot Ankle Clin. 2014, 19, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Silfverskiold, N. Reduction of the Uncrossed Two-Joints Muscles of the Leg to One-Joint Muscles in Spastic Conditions. Acta Chir Scandinav 1924, 56, 315–330. [Google Scholar]
- Lalevée, M.; Barbachan Mansur, N.S.; Schmidt, E.; Carvalho, K.; Vandelune, C.; Bernasconi, A.; Wilken, J.; de Cesar Netto, C. Does Tibialis Posterior Dysfunction Correlate with a Worse Radiographic Overall Alignment in Progressive Collapsing Foot Deformity? A Retrospective Study. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2022, 28, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Martinez, L.; Lalevée, M.; Beldame, J.; L’Hermette, M.; Brunel, H.; Dujardin, F.; Billuart, F. Reliability of a New Computerized Equinometer Based on Silfverskiöld Test to Measure Gastrocnemius Tightness. PLoS ONE 2023, 18, e0284279. [Google Scholar] [CrossRef]
- Lower Body Modeling with Plug-in Gait-Nexus 2.5 Documentation-Vicon Documentation. Available online: https://docs.vicon.com/display/Nexus25/Lower+body+modeling+with+Plug-in+Gait (accessed on 25 June 2023).
- Zvetkova, E.; Koytchev, E.; Ivanov, I.; Ranchev, S.; Antonov, A. Biomechanical, Healing and Therapeutic Effects of Stretching: A Comprehensive Review. Appl. Sci. 2023, 13, 8596. [Google Scholar] [CrossRef]
- Stecco, C.; Pirri, C.; Fede, C.; Yucesoy, C.A.; De Caro, R.; Stecco, A. Fascial or Muscle Stretching? A Narrative Review. Appl. Sci. 2021, 11, 307. [Google Scholar] [CrossRef]
- Jung, J.-Y.; Yang, C.-M.; Kim, J.-J. Effectiveness of Combined Stretching and Strengthening Exercise Using Rehabilitation Exercise System with a Linear Actuator and MR Damper on Static and Dynamic Sitting Postural Balance: A Feasibility Study. Appl. Sci. 2021, 11, 7329. [Google Scholar] [CrossRef]
- Marouvo, J.; Sousa, F.; Fernandes, O.; Castro, M.A.; Paszkiel, S. Gait Kinematics Analysis of Flatfoot Adults. Appl. Sci. 2021, 11, 7077. [Google Scholar] [CrossRef]
- Steinberg, N.; Tenenbaum, G.; Zeev, A.; Witchalls, J.; Waddington, G. The Relationship between the Ability to Cope with Unexpected Perturbations and Mechanical and Functional Ankle Instability. Appl. Sci. 2022, 12, 11119. [Google Scholar] [CrossRef]
- Lalevée, M.; Anderson, D.D.; Wilken, J.M. Current Challenges in Chronic Ankle Instability. Foot Ankle Clin. 2023, 28, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Križaj, L.; Kozinc, Ž.; Šarabon, N. The Outcomes of Conservative Nonpharmacological Treatments for Achilles Tendinopathy: An Umbrella Review. Appl. Sci. 2022, 12, 12132. [Google Scholar] [CrossRef]
- Agostini, F.; Mangone, M.; Finamore, N.; Di Nicola, M.; Papa, F.; Alessio, G.; Vetrugno, L.; Chiaramonte, A.; Cimbri, G.; Bernetti, A.; et al. The Efficacy of Instrumental Physical Therapy through Extracorporeal Shock Wave Therapy in the Treatment of Plantar Fasciitis: An Umbrella Review. Appl. Sci. 2022, 12, 2841. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 20) Mean ± SD (95% CI) | IGT Group (n = 20) Mean ± SD (95% CI) | p-Value | ||
|---|---|---|---|---|
| Age | 37.8 ± 14.5 (31–44.6) | 42.2 ± 15.8 (34.8–49.7) | 0.16 | |
| Weight | 65.7 ± 13.4 (59.5–71.9) | 65.3 ± 10.6 (60.3–70.3) | 0.76 | |
| Gender | Male | 8 (40%) | 16 (80%) | 0.02 |
| Female | 12 (60%) | 4 (20%) | ||
| Ankle dorsiflexion with the knee in extension (in degrees) | 2.2 ± 2.6 (0.9–3.4) | −6.5 ± 7.1 (−9.8–−3.2) | <0.001 | |
| Silfverskiöld test: ankle dorsiflexion gain after 90° knee flexion (in degrees) | 4.2 ± 2.5 (3–5.4) | 16.4 ± 4.7 (14.2–18.5) | <0.001 | |
| Control Group (n = 20) Mean ± SD (95% CI) | Study Group (n = 20) Mean ± SD (95% CI) | Effect Size | p-Value | |
|---|---|---|---|---|
| Maximum ankle dorsiflexion (in degrees) | 14.9 ± 3.0 (13.5–16.4) | 13.5 ± 4.1 (11.6–15.5) | 0.39 | 0.2 |
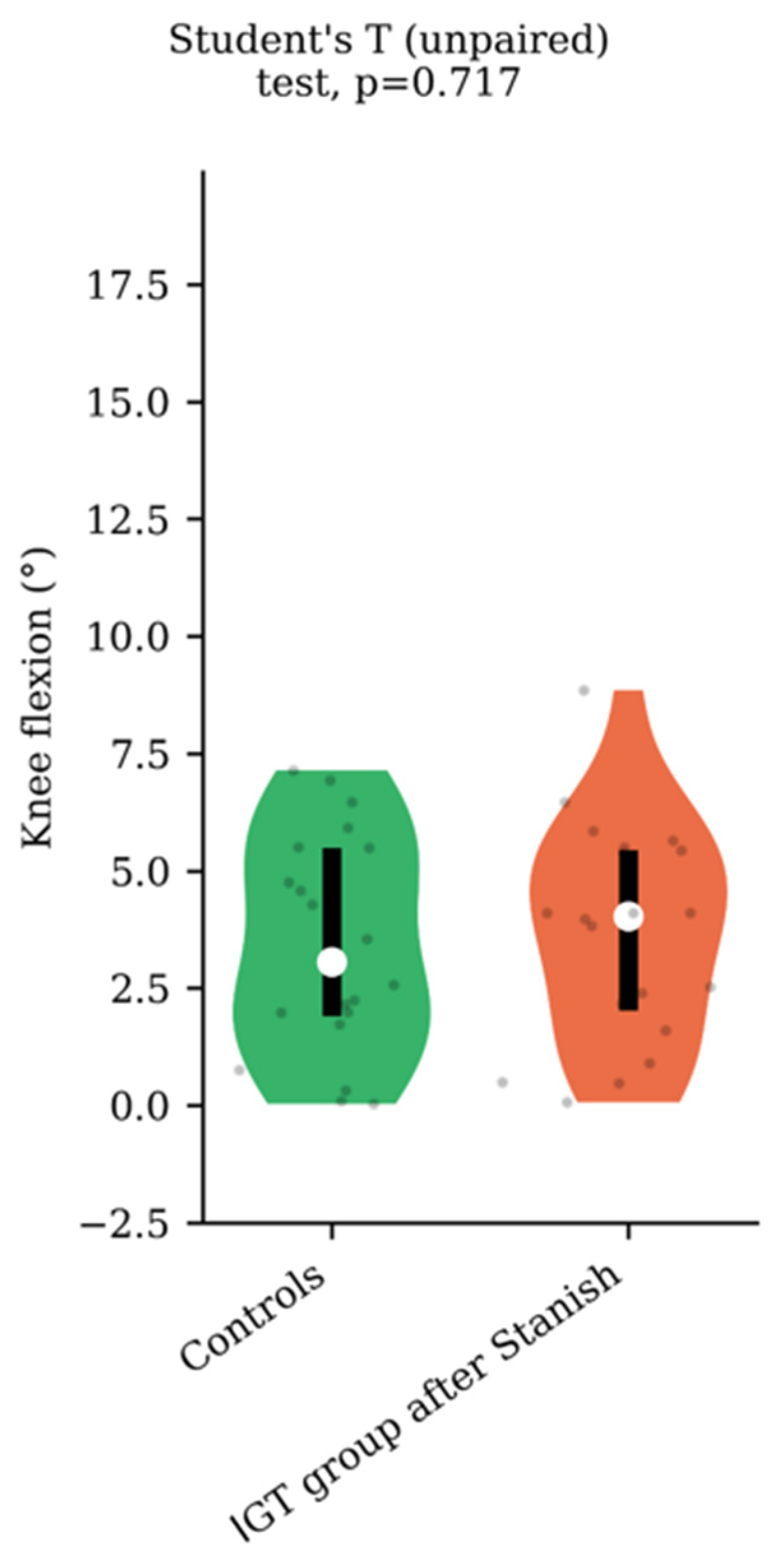
| Corresponding knee flexion (in degrees) | 3.4 ± 2.3 (2.3–4.5) | 8.9 ± 4.6 (6.8–11.1) | 1.21 | <0.001 |
| Maximum forefoot pressure (newton/cm2/kg) | 0.69 ± 0.18 (0.61–0.79) | 0.62 ± 0.08 (0.58–0.66) | 0.5 | 0.073 |
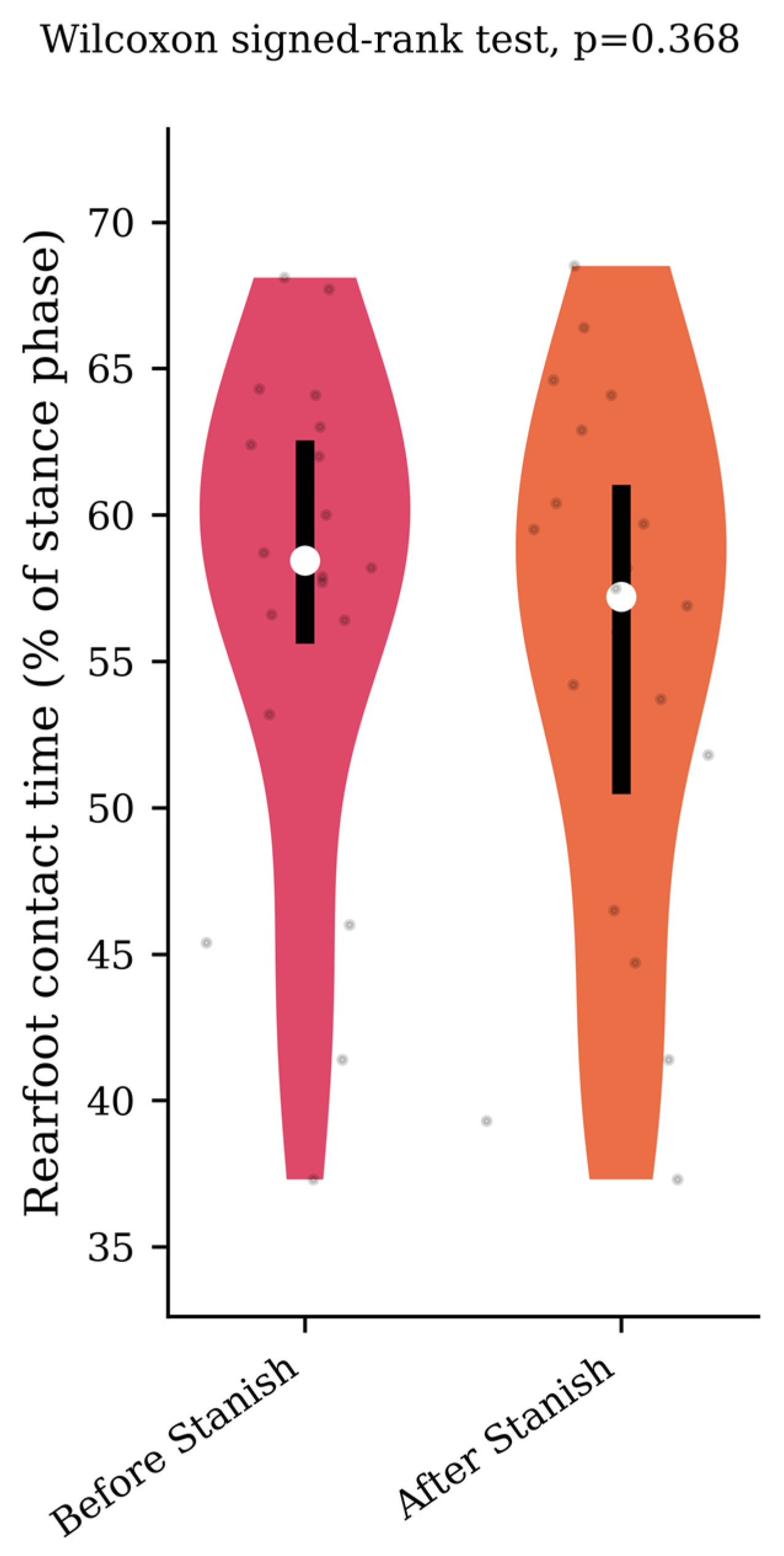
| Rearfoot contact time (% stance phase) | 57.9 ± 4.8 (55.9–60.4) | 57 ± 8.4 (53.1–60.9) | 0.13 | 0.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamza, A.; Martinez, L.; Sacco, R.; Amouyel, T.; Held, E.; Beldame, J.; Billuart, F.; Lalevée, M. Stretching and Eccentric Exercises Normalize Gait Parameters in Gastrocnemius Tightness Subjects. Appl. Sci. 2023, 13, 12494. https://doi.org/10.3390/app132212494
Hamza A, Martinez L, Sacco R, Amouyel T, Held E, Beldame J, Billuart F, Lalevée M. Stretching and Eccentric Exercises Normalize Gait Parameters in Gastrocnemius Tightness Subjects. Applied Sciences. 2023; 13(22):12494. https://doi.org/10.3390/app132212494
Chicago/Turabian StyleHamza, Amine, Lucas Martinez, Riccardo Sacco, Thomas Amouyel, Eric Held, Julien Beldame, Fabien Billuart, and Matthieu Lalevée. 2023. "Stretching and Eccentric Exercises Normalize Gait Parameters in Gastrocnemius Tightness Subjects" Applied Sciences 13, no. 22: 12494. https://doi.org/10.3390/app132212494
APA StyleHamza, A., Martinez, L., Sacco, R., Amouyel, T., Held, E., Beldame, J., Billuart, F., & Lalevée, M. (2023). Stretching and Eccentric Exercises Normalize Gait Parameters in Gastrocnemius Tightness Subjects. Applied Sciences, 13(22), 12494. https://doi.org/10.3390/app132212494