The most important finding of this study was that wedging of bike tires in tram tracks is a frequent injury mechanism, mainly causing fractures of the upper extremity. The risk of falls and the associated risk of injury to cyclists must be taken into account by urban traffic planners. To the best of our knowledge, this report on tram-related bicycle injuries has the largest patient sample size and longest study period so far studied.
4.2. Risk Factors and Circumstances of Injury
The lowest number of injuries was found in the months of January and February, while most injuries happened between July and October. This might be best explained with a higher total number of cyclists during the summer months, despite possibly worse road conditions in the winter months. Similarly, Juhra et al. [
3] reported a high count of overall cycling accidents in the summertime with a steady decrease towards the winter months but a further peak in December. Similar to the present data in this study, this peak value might also be explained with the weather and consequent road conditions, but possibly also with the frequent celebrations during this month, which may be related to higher alcohol consumption as reported by Juhra et al. [
3].
Alcohol consumption has been previously described as a risk factor for overall cycling, and specifically tram-system-related cycling injuries [
1,
3]. In our department, alcohol consumption is not routinely tested in bicycle accidents and was therefore not included in the analysis.
4.3. Cost of Injury
The estimated direct treatment costs in this study were EUR 361.000 in total, and, respectively, EUR 955.03 per injured patient.
Similarly, Aertsens et al. [
7] analyzed the economic costs of 118 minor bicycle accidents, excluding accidents resulting in death or hospital visits lasting more than 24 h, and calculated an average total cost of EUR 841 per accident or EUR 0.125 per kilometer traveled. Considering that the observed cohort in this study includes hospitalized patients with potentially more severe injuries, the total cost of injuries potentially could be substantially higher.
4.4. Preventing Injury
Given the overall high incidence rates, some of which continue to increase, several authors have discussed ways to prevent injury and prevent this mechanism of injury in particular. Teschke et al. [
5] compared bicycle crashes directly involving tram tracks to crashes in other circumstances and found track crashes to be more common on highly frequented streets with parked cars and no bike infrastructure. In addition, Teschke et al. [
5] discussed modifying standard tire width in order to prevent tire wedging and suggested separate lanes for public transportation and cyclists. The width of the tram tracks is around 37 mm in our city. Thicker tires might prevent wedging because they would not fit into the tracks while thinner tires could easily get into the tracks and lead to a fall. Moreover, thinner tires show less grip to the surface than thicker ones, which may potentially also be a reason for easier slippage inside the tracks.
Bike helmets have repeatedly been mentioned as an effective measure to reduce incidence and severity of traumatic brain injuries [
6,
7,
8,
9]. Although all cyclists are advised to wear a helmet to reduce the risk of brain injury, this is far from being widely implemented, and cyclists without helmets are still frequently seen. It should be noted that in Austria, there is no legal obligation to wear a bicycle helmet for persons over the age of twelve. In our cohort, helmet usage was reported only for one of the nine patients with a diagnosed traumatic brain injury. This might have been the real count, or the consequence of incomplete documentation of patient history or more difficult data collection in patients with traumatic brain injury and possibly impaired vigilance.
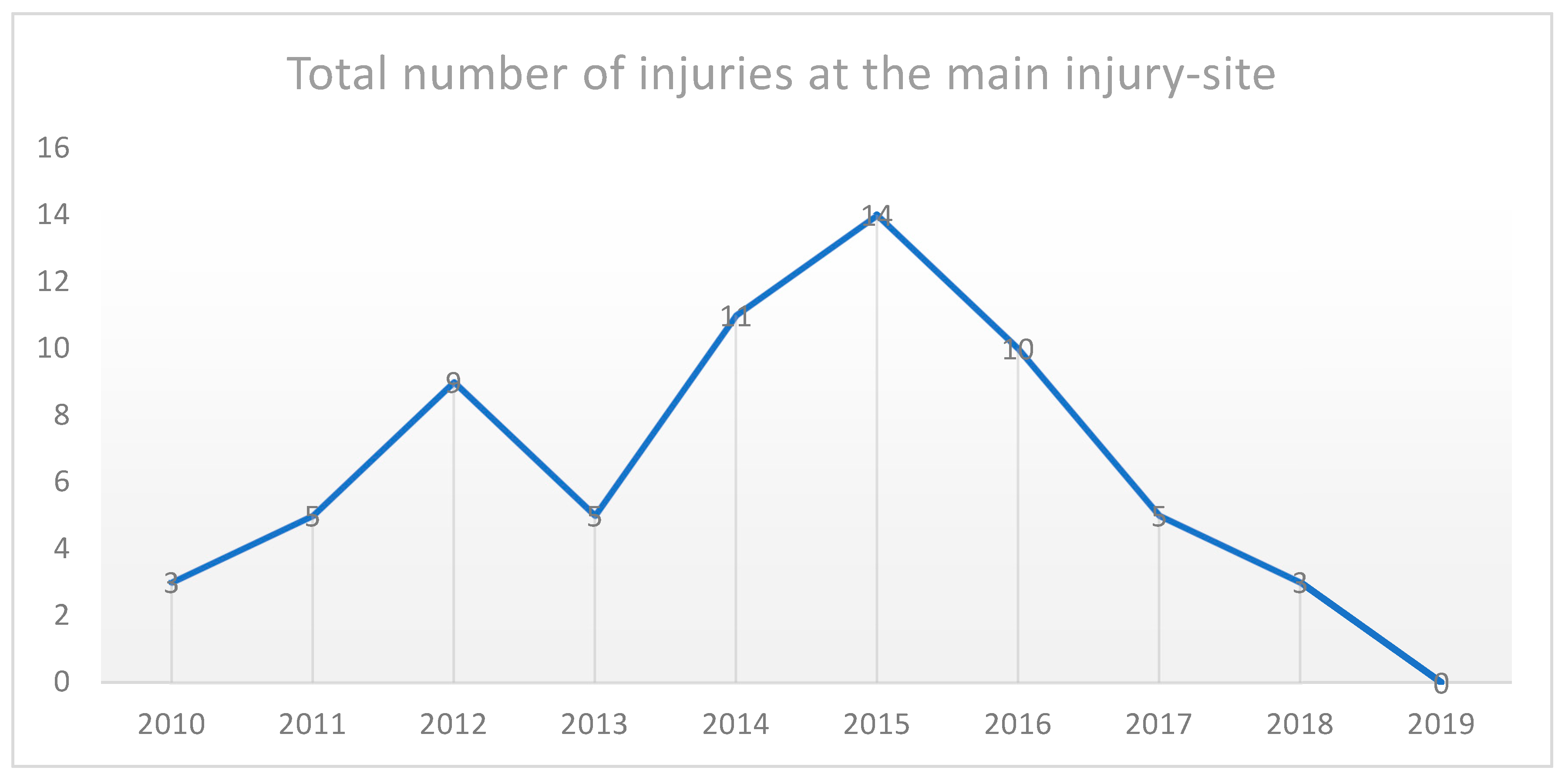
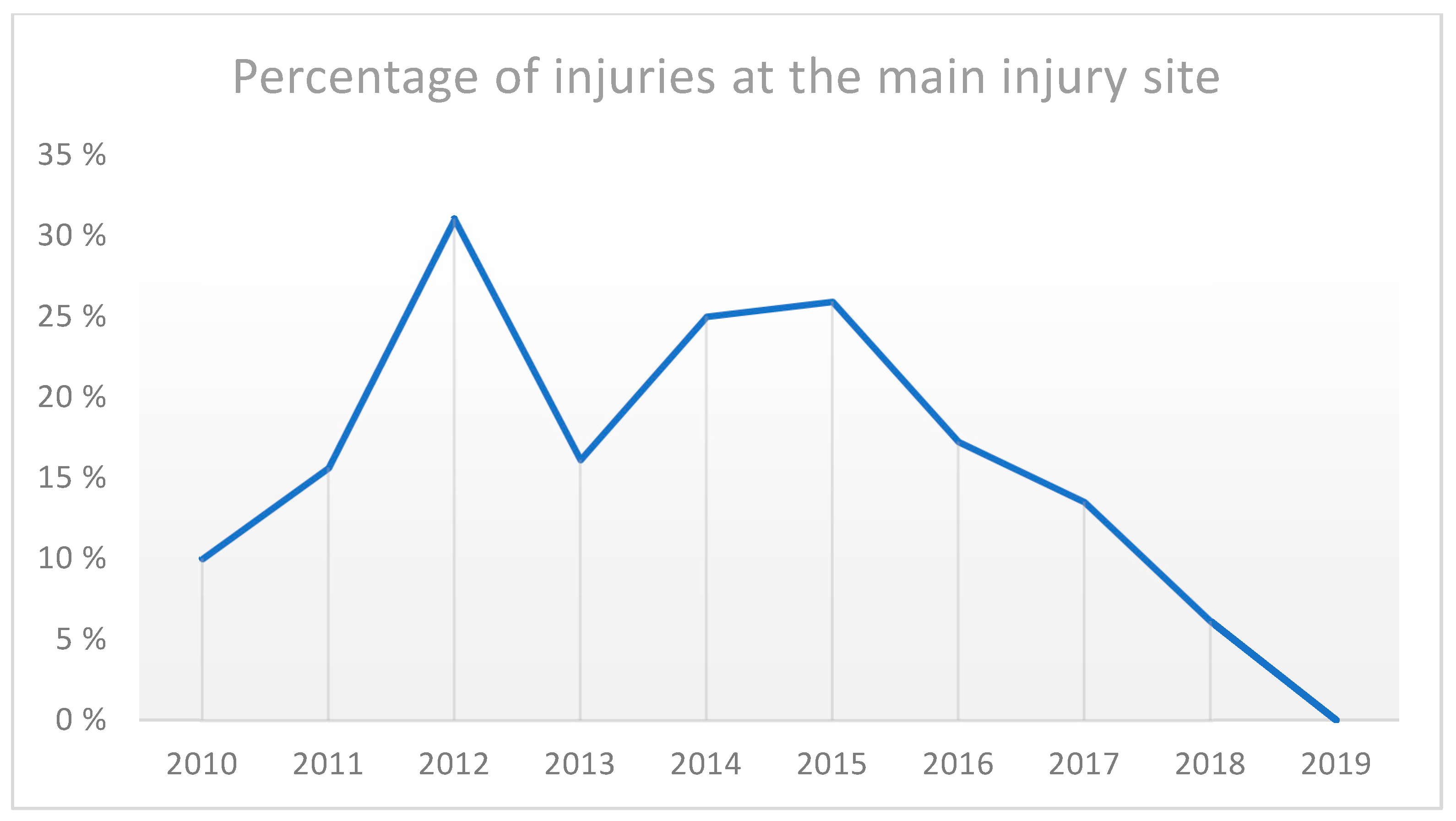
Across the entire 10-year period, about one sixth (17%), even a quarter of the cases in some years, were related to the most common injury site in the inner city. Throughout this 10-year study period, the city government implemented several measurements to the most frequented traffic hubs to increase cyclists’ safety. A taxi waiting area along a highly frequented road was removed at the most common injury site and replaced with a non-road bike lane in November 2018. Furthermore, so-called “sharrows” were introduced to indicate to cyclists the preferred bike lane in order to decrease the risk of accidents with suddenly opened car doors or entrapments between parked cars or pedestrian walkways.
Figure 3 shows the separation of bike and tram routes at one main injury site.
Besides physical protective equipment and separation of traffic with ideally dedicated bicycle lanes, public awareness of common injury mechanisms and hazards related to trams was reported to decrease the injury incidence [
1,
10,
11,
12,
13,
14]. Cameron et al. [
1] reported a sharp decrease in tram-system-related cycling injuries after a period of local media attention. Furthermore, the results of a literature review by Schepers et al. [
2] suggest a rather paradox finding that a higher proportion of all journeys made by bicycle reduces the proportion of cyclist injuries caused by single-bicycle crashes. It might therefore also be concluded from these findings that traffic that is based a lot on bicycle routes, is frequently used, and adapted accordingly in terms of urban planning represents a more safe environment for cyclists. However, due to the chosen retrospective study design, no statement can be made about the absolute numbers of bicycle trips made in this study; these findings also indicate that regulatory measures taken by urban planners have relevant effects on the risk of injury to cyclists. The results of this study should furthermore be of high relevance to clinicians, traumatologists, orthopedic surgeons, and rescue workers who need to provide medical care to injured cyclists with appropriate injury mechanisms and corresponding injuries that warrant rapid treatment.
Preventing this injury mechanism requires a multifaceted approach that includes infrastructure improvements, bicyclist awareness and education, and evaluation of safety measures to reduce the frequency and severity of bicycle crashes on tram tracks. Future studies should prospectively investigate which measures have an injury prevention effect, quantify their magnitude, and thus enable urban planners to use evidence-based measures to make urban cycling as safe as possible. Several limitations apply to this study. First, because patients with only minor injuries might not have attended the emergency department of our hospital, the true injury incidence is presumably higher. Furthermore, country hospitals were not included in the evaluation and therefore it cannot be ruled out that a patient attended another hospital. Nonetheless, our emergency department is the primary care reference unit located directly in the city center, and it can be assumed that most of the patients, especially with severe injuries, were treated at our department. Second, due to the retrospective design of this study, it remains unclear if the noticeable reduction in injuries at the most common injury site represents the positive outcome of a successful city government intervention or if further unknown factors came into play. Third, due to missing data on the overall usage of the studied cycle tracks, the true incidence rate of bicycle-related tram injuries cannot be calculated.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


