

Neurophysiological Evaluation of the Functional State of Muscular and Nervous Systems in High-Maneuvering Jet Fighters



Abstract
1. Introduction
2. Materials and Methods
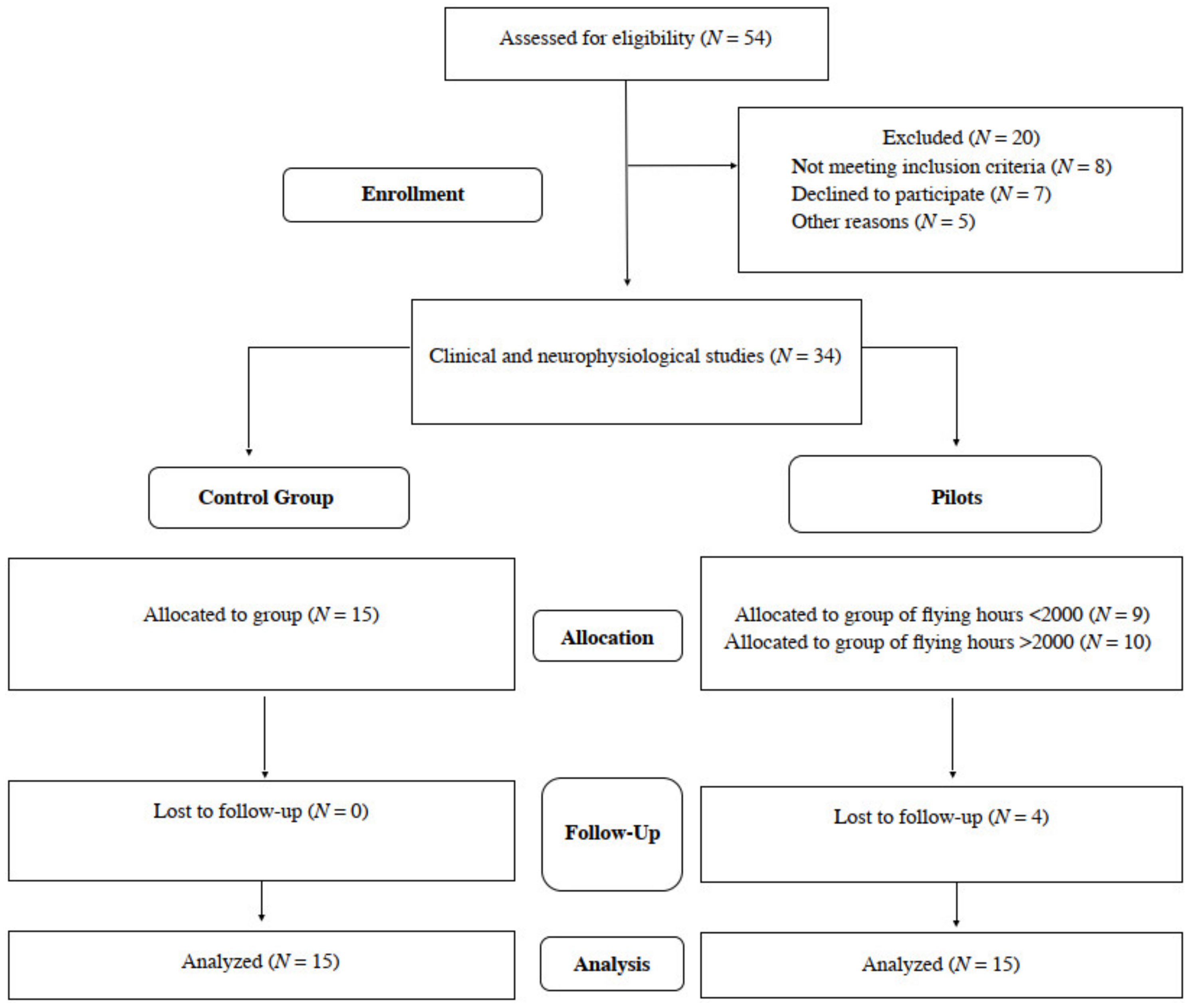
2.1. Participants
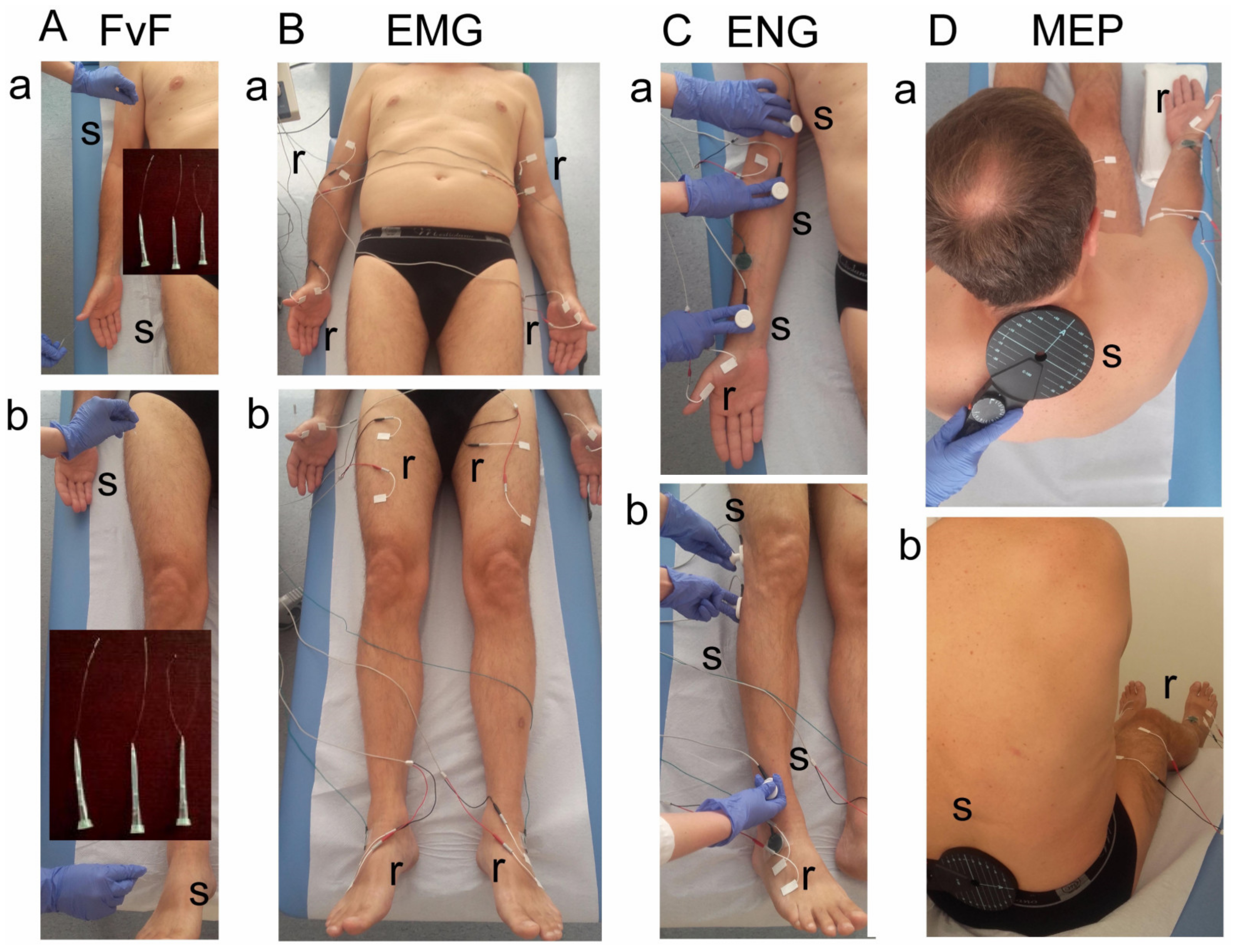
2.2. Clinical Neurophysiology Tests
2.3. Data Analysis and Statistics
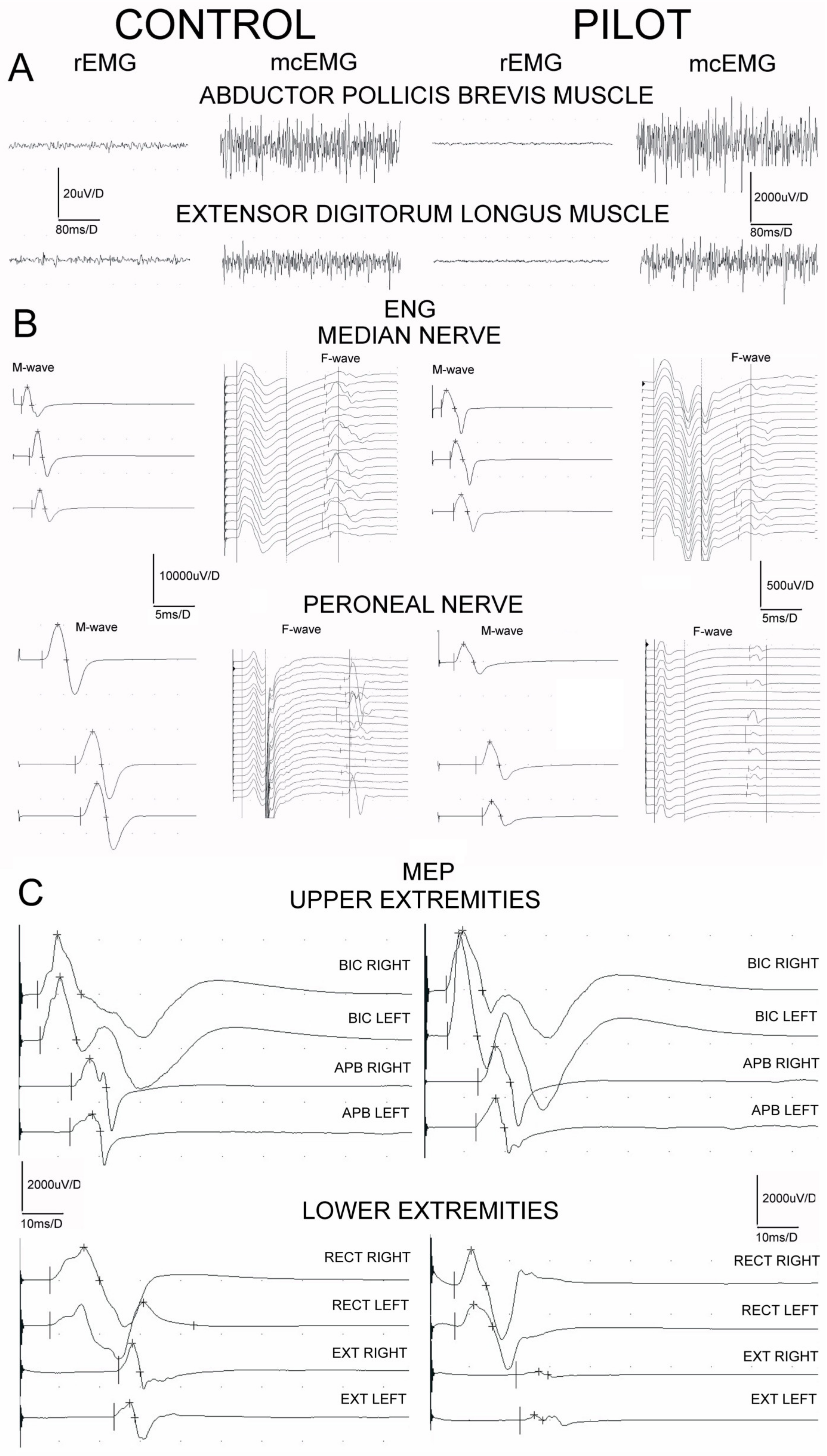
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Green, B.N.; Dunn, A.S.; Pearce, S.M.; Johnson, C.D. Conservative management of uncomplicated mechanical neck pain in a military aviator. J. Can. Chiropr. Assoc. 2010, 54, 92–99. [Google Scholar] [PubMed]
- Kang, S.; Hwang, S.; Lee, E.T.; Yang, S.; Park, J. Measuring the cumulative effect of G force on aviator neck pain. Aviat. Space Environ. Med. 2011, 82, 1042–1048. [Google Scholar] [CrossRef]
- Rintala, H.; Häkkinen, A.; Siitonen, S.; Kyröläinen, H. Relationships Between Physical Fitness, Demands of Flight Duty, and Musculoskeletal Symptoms Among Military Pilots. Mil. Med. 2015, 180, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.S.; Jahr, K.I.; Rodskier, S. +Gz-induced spinal symptoms in fighter pilots: Operational and individual associated factors. Aviat. Space Environ. Med. 2012, 83, 1092–1096. [Google Scholar] [CrossRef] [PubMed]
- Thoolen, S.J.J.; van den Oord, M.H.A.H. Modern air combat developments and their influence on neck and back pain in F-16 pilots. Aerosp. Med. Hum. Perform. 2015, 86, 936–941. [Google Scholar] [CrossRef]
- Drew, W.E.S. Spinal symptoms in aviators and their relationship to G-exposure and aircraft seating angle. Aviat. Space Environ. Med. 2000, 71, 22–30. [Google Scholar] [PubMed]
- Oksa, J.; Hämäläinen, O.; Rissanen, S.; Salminen, M.; Kuronen, P. Muscle fatigue caused by repeated aerial combat maneuvering exercises. Aviat. Space Environ. Med. 1999, 70, 556–560. [Google Scholar] [PubMed]
- Coakwell, M.R.; Bloswick, D.S.; Moser, R., Jr. High-risk head and neck movements at high G and interventions to reduce associated neck injury. Aviat. Space Environ. Med. 2004, 75, 68–80. [Google Scholar]
- Truszczyńska, A.; Lewkowicz, R.; Truszczyński, O.; Wojtkowiak, M. Back pain and its consequences among Polish Air Force pilots flying high performance aircraft. Int. J. Occup. Med. Environ. Health 2014, 27, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Verde, P.; Trivelloni, P.; Angelino, G.; Morgagni, F.; Tomao, E. Neck Pain in F-16 vs. Typhoon Fighter Pilots. Aerosp. Med. Hum. Perform. 2015, 86, 402–406. [Google Scholar] [CrossRef]
- Kelley, A.M.; Macdonnell, J.; Grigley, D.; Campbell, J.; Gaydos, S.J. Reported back pain in army aircrew in relation to airframe, gender, age, and experience. Aerosp. Med. Hum. Perform. 2017, 88, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Hewson, D.J.; McNair, P.J.; Marshall, R.N. Aircraft control forces and EMG activity: Comparison of novice and experienced pilots during simulated take-off and landing. Aviat. Space Environ. Med. 1999, 70, 745–751. [Google Scholar] [PubMed]
- Sovelius, R.; Salonen, O.; Lamminen, A.; Huhtala, H.; Hämäläinen, O. Spinal MRI in fighter pilots and controls: A 13-year longitudinal study. Aviat. Space Environ. Med. 2008, 79, 685–688. [Google Scholar] [CrossRef] [PubMed]
- Lisiński, P.; Huber, J. Evolution of muscles dysfunction from myofascial pain syndrome through cervical disc-root conflict to degenerative spine disease. Spine 2017, 42, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Huber, J.; Lisiński, P. Early results of supervised versus unsupervised rehabilitation of patients with cervical pain. Int. J. Artif. Organs 2019, 42, 695–703. [Google Scholar] [CrossRef]
- Bryndal, A.; Wojtysiak, M.; Moskal, J.; Lipiec-Kowalska, J.; Borowczyk, M.; Tańska, M.; Grochulska, A.; Huber, J.; Majchrzycki, M. Motor evoked potentials after supraspinal stimulation in pre- and postoperative evaluations of patients with cervical radiculopathy. Biomed Res. Int. 2019, 2019, 4576493. [Google Scholar] [CrossRef] [PubMed]
- Wojtysiak, M.; Huber, J.; Wiertel-Krawczuk, A.; Szymankiewicz-Szukała, A.; Moskal, J.; Janicki, J. Pre- and postoperative evaluation of patients with lumbosacral disc herniation by neurophysiological and clinical assessment. Spine 2014, 39, 1792–1800. [Google Scholar] [CrossRef] [PubMed]
- Huber, J.; Lisinski, P.; Samborski, W.; Wytrazek, M. The effect of early isometric exercises on clinical and neurophysiological parameters in patients with sciatica: An interventional randomized single-blinded study. Isokinet. Exerc. Sci. 2011, 19, 207–214. [Google Scholar] [CrossRef]
- Huber, J.; Lisiński, P.; Polowczyk, A. Reinvestigation of the dysfunction in neck and shoulder girdle muscles as the reason of cervicognic headache among office workers. Disabil. Rehabil. 2013, 35, 793–802. [Google Scholar] [CrossRef]
- Leszczyńska, K.; Wincek, A.; Fortuna, W.; Huber, J.; Łukaszek, J.; Okurowski, S.; Chmielak, K.; Tabakow, P. Treatment of patients with cervical and upper thoracic incomplete spinal cord injury using repetitive transcranial magnetic stimulation. Int. J. Artif. Organs 2019, 43, 323–331. [Google Scholar] [CrossRef]
- Kaczmarek, A.M.; Huber, J.; Leszczyńska, K.; Wietrzak, P.; Kaczmarek, K. Relationships between the Clinical Test Results and Neurophysiological Findings in Patients with Thoracic Outlet Syndrome. Bioengineering 2022, 9, 598. [Google Scholar] [CrossRef] [PubMed]
- Alricsson, M.; Harms-Ringdahl, K.; Larsson, B.; Linder, J.; Werner, S. Neck muscle strength and endurance in fighter pilots: Effects of a supervised training program. Aviat. Space Environ. Med. 2004, 75, 23–28. [Google Scholar] [PubMed]
- Clark, J.B. Cervical dystonia following exposure to high-G forces. Aviat. Space Environ. Med. 1990, 61, 935–937. [Google Scholar]
- Chumbley, E.M.; O’Hai, N.; Stolfi, A.; Lienesch, C.; McEachen, J.C.; Wright, B.A. Home Cervical Traction to Reduce Neck Pain in Fighter Pilots. Aerosp. Med. Hum. Perform. 2016, 87, 1010–1015. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Pilots (N = 15) | Healthy Subjects (N = 15) Control | p |
|---|---|---|---|
| Age (years) | (25–48) 38.2 ± 7.6 | (22–47) 35.6 ± 6.9 | NS |
| Height (cm) | (171–189) 178.0 ± 4.8 | (161–182) 173.3 ± 5.9 | NS |
| Weight (kg) | (52–95) 76.4 ± 9.5 | (50–95) 76.9 ± 10.3 | NS |
| BMI | (20.2–36.2) 28.1 ± 5.3 | (19.2–28.7) 25.1 ± 2.6 | NS |
| Number of flying hours (all years) | (410–3100) 1711.7 ± 861.9 | NA | |
| Average number of training catapultings | 4 | NA | |
| Traumas | 1/15 | 0 | |
| Conservative treatment | 1/15 | 0 | |
| Activity (days in a week) | (1–4) 1.9 ± 0.4 | (1–4) 2.3 ± 0.5 | NS |
| Spine pain VAS (0–10) | (0–3) 1.4 ± 0.6 | (0–0) 0 | NS |
| Spine pain (since when, years) | (1–3) 1.7 ± 0.8 | 0 | |
| Pain—upper extremity | 0/15 | 0/15 | |
| Pain—lower extremity | 0/15 | 0/15 | |
| Numbness in hands | 0/15 | 0/15 | |
| Numbness in legs | 0/15 | 0/15 | |
| Superficial sensory perception (FvF) | 1 | 1 |
| Number of Flying Hours | Activity | Spine Pain VAS |
|---|---|---|
| <2000 | 1.89 | 0.88 |
| >2000 | 2.0 | 1.67 |
| Type of Test Recording Site Stimulation Site | Measured Parameter | Controls (Healthy Subjects) | Pilots | P | ||||
|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | |||
| sEMG | BIC | rEMG (µV) | 13.6 ± 3.5 | 15.7 ± 3.2 | 15.0 ± 1.9 | 14.3 ± 2.6 | 0.06 | 0.07 |
| mcEMG (µV) | 1500.0 ± 379.8 | 1435.7 ± 359.8 | 2842.9 ± 1233.9 | 2392.9 ± 1167.7 | 0.02 ↑ | 0.03 ↑ | ||
| FI | 2.8 ± 0.4 | 2.8 ± 0.4 | 2.7 ± 0.5 | 2.7 ± 0.5 | 0.06 | 0.06 | ||
| APB | rEMG (µV) | 16.4 ± 2.9 | 13.6 ± 2.9 | 13.6 ± 4.4 | 13.2 ± 4.4 | 0.02 ↓ | 0.07 | |
| mcEMG (µV) | 1557.1 ± 394.1 | 1664.3 ± 345.6 | 3057.1 ± 1080.8 | 2785.7 ± 1249.5 | 0.01 ↑ | 0.02 ↑ | ||
| FI | 2.9 ± 0.3 | 2.9 ± 0.3 | 2.8 ± 0.6 | 2.9 ± 0.3 | 0.1 | 0.12 | ||
| RECT | rEMG (µV) | 15.0 ± 3.3 | 13.9 ± 4.3 | 15.4 ± 1.2 | 15.4 ± 1.3 | 0.07 | 0.06 | |
| mcEMG (µV) | 1442.9 ± 145.0 | 1535.7 ± 183.6 | 2671.4 ± 1412.9 | 2292.9 ± 1310.1 | 0.02 ↑ | 0.04 ↑ | ||
| FI | 2.7 ± 0.5 | 2.9 ± 0.3 | 2.8 ± 0.4 | 2.9 ± 0.3 | 0.12 | 0.11 | ||
| EXT | rEMG (µV) | 16.1 ± 2.8 | 13.2 ± 2.4 | 17.1 ± 2.5 | 14.2 ± 4.5 | 0.06 | 0.07 | |
| mcEMG (µV) | 1492.9 ± 373.1 | 1707.1 ± 308.1 | 2907.1 ± 1602.4 | 2664.3 ± 1256.8 | 0.02 ↑ | 0.03 ↑ | ||
| FI | 2.8 ± 0.4 | 2.9 ± 0.3 | 2.9 ± 0.3 | 2.9 ± 0.3 | 0.07 | 0.06 | ||
| ENG—median nerve | M- wave Wrist | Amplitude (µV) | 6214.3 ± 2086.3 | 5778.6 ± 1467.3 | 7150.0 ± 2629.7 | 4907.1 ± 2080.3 | 0.06 | 0.07 |
| Latency (ms) | 3.3 ± 0.2 | 3.4 ± 0.3 | 3.5 ± 0.5 | 3.5 ± 0.7 | 0.16 | 0.13 | ||
| M- wave Cubital fossa | Amplitude (µV) | 5450.0 ± 1947.1 | 4885.7 ± 1923.9 | 6685.7 ± 2251.3 | 4500.0 ± 2571.5 | 0.06 | 0.07 | |
| Latency (ms) | 7.0 ± 0.8 | 7.0 ± 1.0 | 7.3 ± 0.9 | 7.0 ± 0.9 | 0.07 | 0.07 | ||
| M- wave Arm | Amplitude (µV) | 6914.3 ± 1879.5 | 5728.6 ± 2546.3 | 7671.4 ± 2127.5 | 5985.7 ± 3224.9 | 0.05 ↑ | 0.06 | |
| Latency (ms) | 8.1 ± 0.7 | 7.9 ± 1.1 | 8.6 ± 0.8 | 8.2 ± 1.2 | 0.07 | 0.06 | ||
| F wave frequency [x/20] | 16.7 ± 1.7 | 16.9 ± 1.9 | 17.4 ± 1.6 | 17.0 ± 2.3 | 0.16 | 0.12 | ||
| M-F Latency [ms] | 24.5 ± 1.8 | 24.5 ± 1.6 | 24.6 ± 1.5 | 24.7 ± 1.6 | 0.07 | 0.06 | ||
| ENG—peroneal nerve | M-wave Ankle | Amplitude (µV) | 5164.3 ± 1578.2 | 5464.3 ± 1982.6 | 4485.7 ± 1285.0 | 5292.9 ± 2389.1 | 0.05 ↓ | 0.06 |
| Latency (ms) | 4.7 ± 0.7 | 4.9 ± 0.6 | 4.8 ± 1.1 | 5.2 ± 0.8 | 0.06 | 0.05 ↑ | ||
| M- wave Below knee | Amplitude (µV) | 5628.6 ± 1278.6 | 5321.4 ± 1734.2 | 4992.9 ± 1548.5 | 5550.0 ± 2118.9 | 0.05 ↓ | 0.06 | |
| Latency (ms) | 11.5 ± 1.0 | 11.4 ± 0.8 | 13.6 ± 11.8 | 14.6 ± 11.8 | 0.05 ↑ | 0.04 ↑ | ||
| M- wave Above knee | Amplitude (µV) | 4864.3 ± 1290.4 | 5421.4 ± 1641.5 | 4450.0 ± 1148.8 | 5085.7 ± 1993.9 | 0.12 | 0.06 | |
| Latency (ms) | 13.0 ± 0.9 | 13.0 ± 0.9 | 14.7 ± 13.1 | 14.7 ± 13.1 | 0.05 ↑ | 0.05 ↑ | ||
| F wave frequency [x/20] | 17.6 ± 1.6 | 17.3 ± 1.5 | 13.0 ± 4.1 | 13.7 ± 3.7 | 0.05 ↓ | 0.05 ↓ | ||
| M-F Latency [ms] | 43.2 ± 2.1 | 43.7 ± 2.4 | 45.2 ± 4.1 | 44.8 ± 3.0 | 0.06 | 0.06 | ||
| MEP | BIC | Amplitude (µV) | 1510.7 ± 601.2 | 1657.1 ± 793.5 | 1530.7 ± 1211.5 | 1753.6 ± 960.0 | 0.06 | 0.07 |
| Latency (ms) | 5.1 ± 0.5 | 5.0 ± 0.5 | 5.0 ± 0.9 | 5.2 ± 1.0 | 0.09 | 0.07 | ||
| APB | Amplitude (µV) | 1939.3 ± 816.0 | 1914.3 ± 976.8 | 2057.1 ± 2282.5 | 1820.0 ± 1527.8 | 0.12 | 0.14 | |
| Latency (ms) | 12.9 ± 1.0 | 12.8 ± 1.0 | 13.4 ± 1.3 | 14.5 ± 3.0 | 0.01 | 0.01 | ||
| RECT | Amplitude (µV) | 2257.1 ± 1360.5 | 2514.3 ± 1161.2 | 1146.4 ± 2247.7 | 671.4 ± 1240.1 | 0.03 ↓ | 0.02 ↓ | |
| Latency (ms) | 5.2 ± 0.6 | 5.2 ± 0.6 | 7.1 ± 1.1 | 7.2 ± 1.3 | 0.05 ↑ | 0.04 ↑ | ||
| EXT | Amplitude (µV) | 1714.3 ± 715.0 | 1435.7 ± 735.4 | 1485.7 ± 2179.2 | 1482.1 ± 2223.2 | 0.03 ↓ | 0.06 | |
| Latency (ms) | 23.0 ± 0.9 | 22.9 ± 0.8 | 22.5 ± 4.1 | 21.7 ± 2.8 | 0.13 | 0.14 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wesołek, A.; Daroszewski, P.; Huber, J. Neurophysiological Evaluation of the Functional State of Muscular and Nervous Systems in High-Maneuvering Jet Fighters. Appl. Sci. 2023, 13, 1120. https://doi.org/10.3390/app13021120
Wesołek A, Daroszewski P, Huber J. Neurophysiological Evaluation of the Functional State of Muscular and Nervous Systems in High-Maneuvering Jet Fighters. Applied Sciences. 2023; 13(2):1120. https://doi.org/10.3390/app13021120
Chicago/Turabian StyleWesołek, Angelika, Przemysław Daroszewski, and Juliusz Huber. 2023. "Neurophysiological Evaluation of the Functional State of Muscular and Nervous Systems in High-Maneuvering Jet Fighters" Applied Sciences 13, no. 2: 1120. https://doi.org/10.3390/app13021120
APA StyleWesołek, A., Daroszewski, P., & Huber, J. (2023). Neurophysiological Evaluation of the Functional State of Muscular and Nervous Systems in High-Maneuvering Jet Fighters. Applied Sciences, 13(2), 1120. https://doi.org/10.3390/app13021120