

A Retrospective Cohort Study of Traumatic Root Fractures in Primary Dentition: Can Splinting Type Improve Therapeutic Outcomes?

 ,
, 
Abstract
1. Introduction
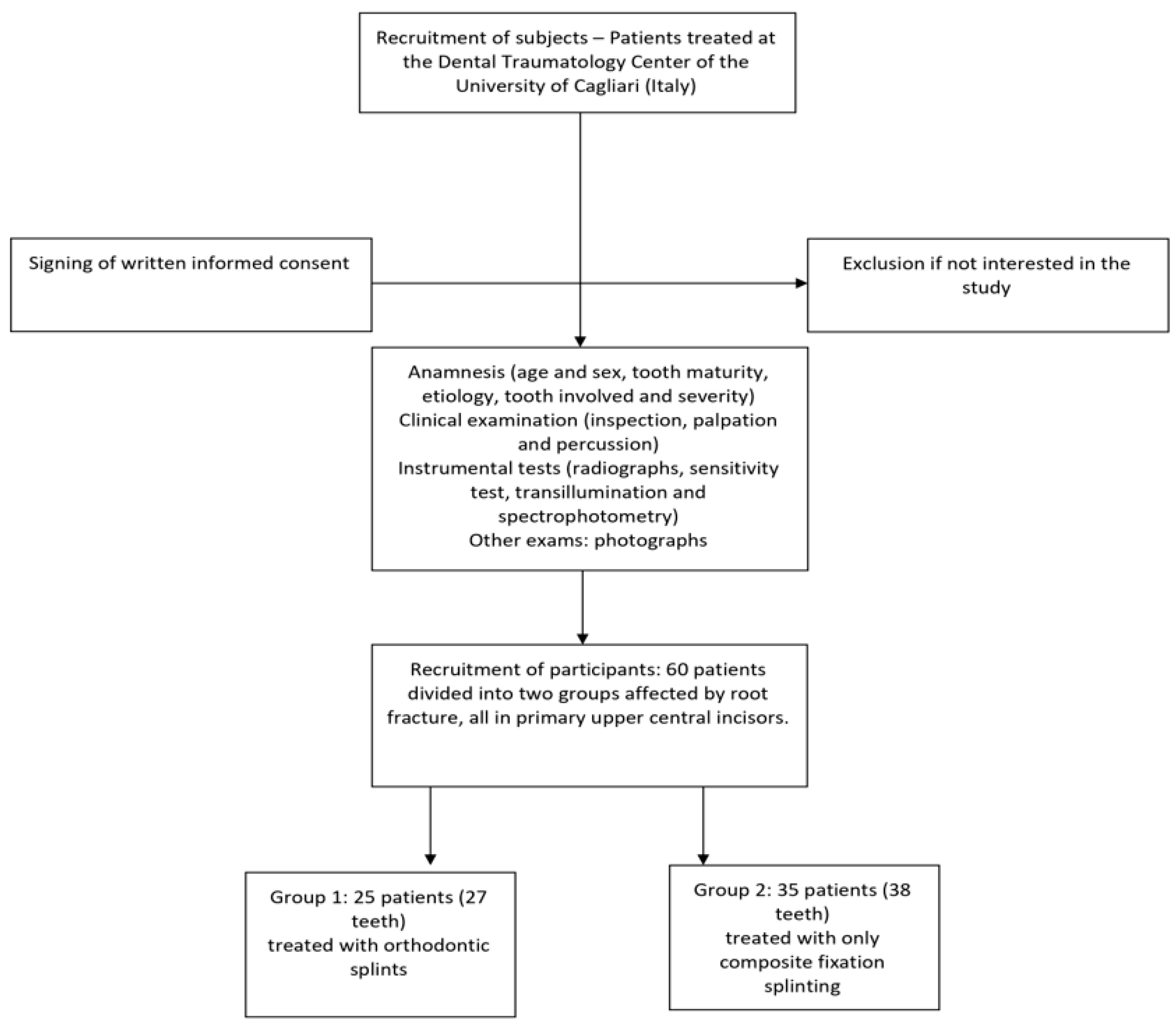
2. Materials and Methods
- -
- Patients with at least one primary incisor presenting with root fracture, with or without compound vestibular cortex fracture;
- -
- Patients examined within 48 h of the dental trauma and whose data had been collected in accordance with the IADT guidelines of 2012, updated in 2020.
- -
- Patients with a history of previous traumatic dental injuries and/or carious lesions;
- -
- Patients who experienced additional traumatic dental injuries during the follow-up period;
- -
- Patients with ongoing interceptive and/or orthodontic therapy.
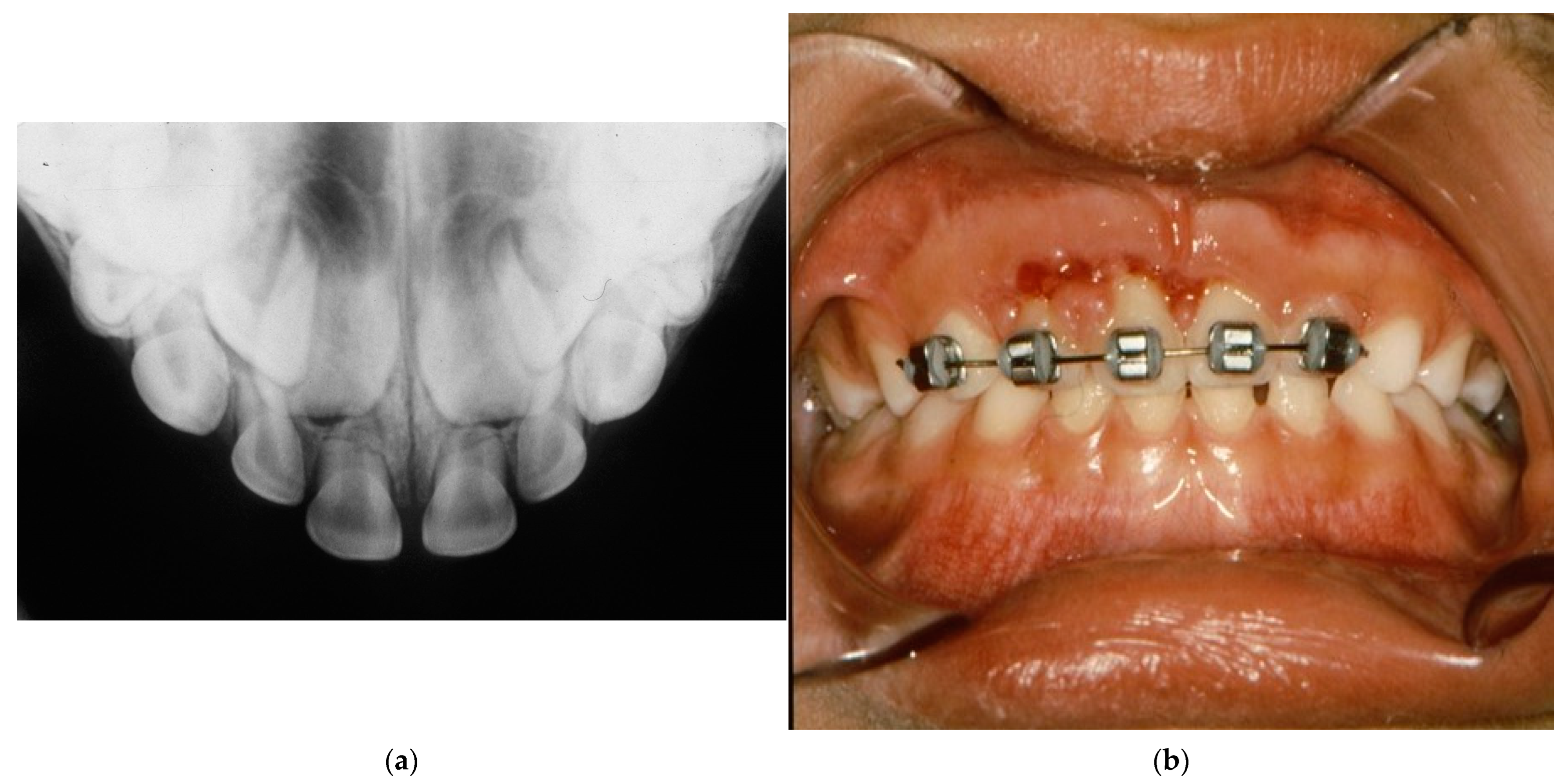
2.1. Management of the Fractures
- Rigid splinting: does not allow any physiological mobility of the tooth and may create conditions for complications of an ankylotic nature.
- Non-rigid/semi-rigid/flexible splinting: allows for physiological functional mobility of the traumatized tooth, promoting healing of the periodontal ligament with a consequent reduction of the risk of ankylosis.
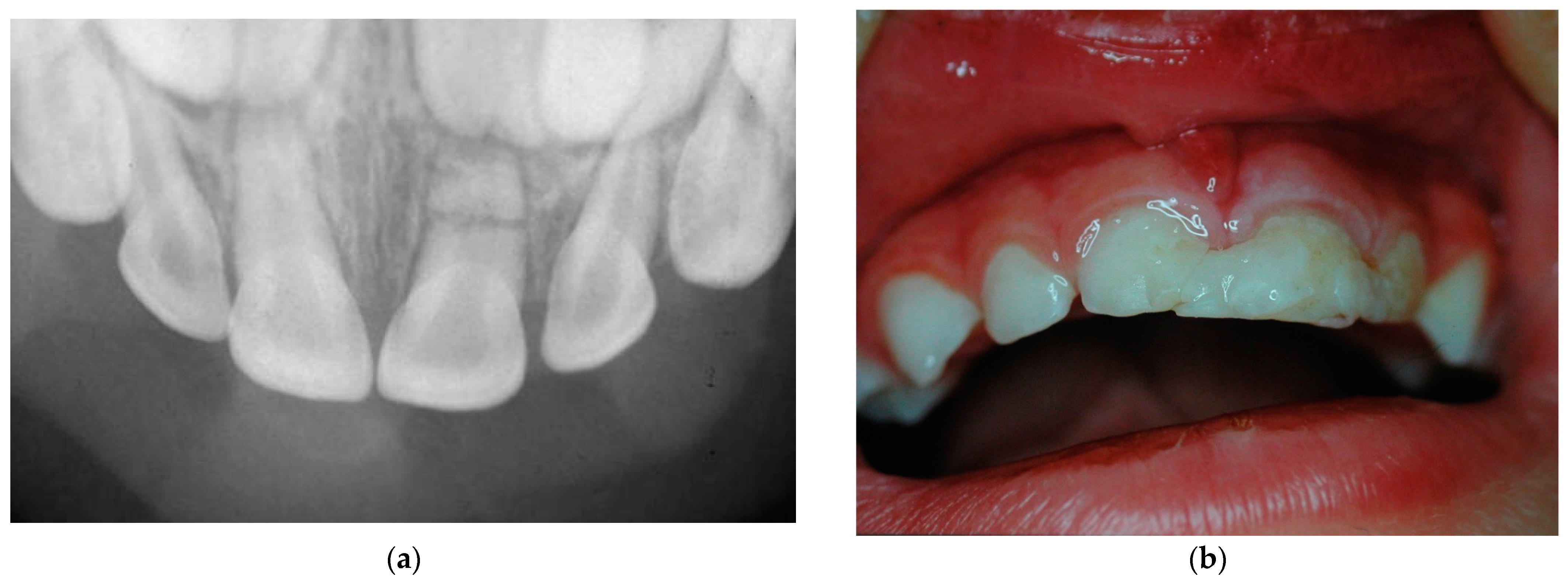
- Conditioning of the enamel of damaged and nearby teeth;
- Application of adhesive and composite material to the affected tooth and adjacent teeth;
- Light curing to harden the composite material.
2.2. Statistical Analysis
3. Results
3.1. General Data of the Selected Patients
3.2. Localization of the Trauma
3.3. Etiology
3.4. Location of the Root Fracture
3.5. Presence of Dislocation with Extrusion
3.6. Other Type of Trauma
3.7. Treatment Time after Trauma
3.8. Follow-Up
3.9. Reabsorption of the Apical Root Fragment
4. Complications
4.1. Premature Loss of Deciduous Teeth
4.2. PCO
4.3. Changes in Permanent Teeth
4.4. Splinting Time
5. Discussion
6. Conclusions
- -
- Early resorption of the distal fragment of the fractured root is a common and non-pathological healing phenomenon in primary teeth, typically occurring within one year of the trauma;
- -
- PCO in primary teeth does not require endodontic treatment unless accompanied by acute symptoms as suppurative manifestations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holan, G.; Needleman, H.L. Premature loss of primary anterior teeth due to trauma—Potential short- and long-term sequelae. Dent. Traumatol. 2013, 30, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.; De Carvalho Rocha, M.J. Traumatized Primary Teeth in Children Assisted at the Federal University of Santa Catarina, Brazil. Dent. Traumatol. 2002, 18, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Day, P.F.; Flores, M.T.; O’Connell, A.C.; Abbott, P.V.; Tsilingaridis, G.; Fouad, A.F.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent. Traumatol. 2020, 36, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Bonanato, K.; Sardenberg, F.; Santos, E.R.; Ramos-Jorge, M.L.; Zarzar, P.M. Horizontal root fracture with displacement in the primary dentition. Gen. Dent. 2011, 57, e31-4. [Google Scholar]
- Bhayya, D.P.; Shyagali, T.R. Traumatic injuries in the primary teeth of 4- to 6-year-old school children in gulbarga city, India. A prevalence study. Oral Health Dent. Manag. 2014, 12, 17–23. [Google Scholar]
- Qassem, A.; Goettems, M.; Torriani, D.D.; Pappen, F.G. Radicular maturity level of primary teeth and its association with trauma sequelae. Dent. Traumatol. 2013, 30, 227–231. [Google Scholar] [CrossRef]
- Feldens, C.A.; Borges, T.S.; Vargas-Ferreira, F.; Kramer, P.F. Risk factors for traumatic dental injuries in the primary dentition: Concepts, interpretation, and evidence. Dent. Traumatol. 2016, 32, 429–437. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Andreasen, F.M.; Andersson, L. Textbook and Color Atlas of Traumatic Injuries to the Teeth. Stomatol. EDU J. 2019, 6, 279. [Google Scholar] [CrossRef]
- Borum, M.K.; Andreasen, J.O. Therapeutic and economic implications of traumatic dental injuries in Denmark: An estimate based on 7549 patients treated at a major trauma centre. Int. J. Paediatr. Dent. 2001, 11, 249–258. [Google Scholar] [CrossRef]
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef]
- Liu, X.; Huang, J.; Bai, Y.; Wang, X.; Baker, A.; Chen, F.; Wu, L.-A. Conservation of root-fractured primary teeth-report of a case. Dent. Traumatol. 2013, 29, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Spinas, E.; Di Giorgio, G.; Murgia, M.S.; Garau, V.; Pinna, M.; Zerman, N. Root Fractures in the Primary Teeth and Their Management: A Scoping Review. Dent. J. 2022, 10, 74. [Google Scholar] [CrossRef] [PubMed]
- dos Santos Fernandez, M.; Schuch, H.S.; Araújo, A.B.G.; Goettems, M.L. Splinting in the management of dental trauma in the primary dentition: A systematic review. Eur. Arch. Paediatr. Dent. 2023, 24, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.C.; Nam, O.H.; Kim, M.S.; Lee, H.-S.; Choi, S.C. A retrospective study of traumatic dental injuries in primary dentition: Treatment outcomes of splinting. Acta Odontol. Scand. 2018, 76, 253–256. [Google Scholar] [CrossRef]
- Boorum, M.K.; Andreasen, J.O. Sequelae of trauma to primary maxillary incisors. I. Complications in the primary dentition. Dent. Traumatol. 1998, 14, 31–44. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, B.Z.; Cardoso, M.; Almeida, I.C.S. Pulp canal obliteration following trauma to primary incisors: A 9-year clinical study. Pediatr. Dent. 2011, 33, 399–402. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Flores, M.T. Traumatic injuries in the primary dentition. Dent. Traumatol. 2002, 18, 287–298. [Google Scholar] [CrossRef]
- Faria, L.V.; Chaves, H.G.D.S.; Silva, E.A.B.; Antunes, L.D.S.; Antunes, L.A.A. Minimally invasive treatment of an extruded deciduous tooth—Case report. Dent. Traumatol. 2020, 36, 303–306. [Google Scholar] [CrossRef]
- Abreu, M.G.L.; Milani, A.J.; Fernandes, T.D.O.; Gomes, C.C.; Antunes, L.S.; Antunes, L.A.A. Dental trauma in primary dentition, its effect on permanent successors and on Oral Health-Related Quality of Life: A 4-year follow-up case report. Int. J. Burns Trauma 2020, 10, 201–209. [Google Scholar]
- Berger, T.D.; Kenny, D.J.; Casas, M.J.; Barrett, E.J.; Lawrence, H.P. Effects of severe dentoalveolar trauma on the quality-of-life of children and parents. Dent. Traumatol. 2009, 25, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Karataş, M.S.; Sönmez, I. Developmental Disturbances of a Maxillary Central Incisor due to Trauma to Its Predecessor: A Case Report. Med. Princ. Pr. 2013, 22, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Mello-Moura, A.C.; Bonini, G.A.; Suga, S.S.; Navarro, R.S.; Wanderley, M.T. Multidisciplinary approach on rehabilitation of primary teeth traumatism repercussion on the permanent successor: 6-year follow-up case report. J. Indian Soc. Pedod. Prev. Dent. 2009, 27, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Arenas, M.; Barberia, E.; Lucavechi, T.; Maroto, M. Severe trauma in the primary dentition—Diagnosis and treatment of sequelae in permanent dentition. Dent. Traumatol. 2006, 22, 226–230. [Google Scholar] [CrossRef]
- Huang, B.; Marcenes, W.; Croucher, R.; Hector, M. Activities related to the occurrence of traumatic dental injuries in 15- to 18-year-olds. Dent. Traumatol. 2009, 25, 64–68. [Google Scholar] [CrossRef]
- Fidalgo, T.K.; Maia, L.C. Minimally invasive intervention of acute trauma in the primary dentition: Successful five-year follow-up. Gen. Dent. 2012, 60, e158-61. [Google Scholar]
- Ruviére, D.B.; Costa, M.M.; Cunha, R.F. Conservative management of severe intru-sion in a primary tooth: A 4-year follow-up. J. Dent. Child. 2009, 76, 87–91. [Google Scholar]
- Charone, S.; Kuchler, E.; Costa, M.D.C.; Maia, L. A successful outcome using a minimal invasive approach to manage a severe trauma to the primary maxillary incisor in a toddler. Dent. Traumatol. 2010, 26, 294–297. [Google Scholar] [CrossRef]
- de Amorim, L.F.G.; da Costa, L.R.R.S.; Estrela, C. Retrospective study of traumatic dental injuries in primary teeth in a Brazilian specialized pediatric practice. Dent. Traumatol. 2011, 27, 368–373. [Google Scholar] [CrossRef]
- Lin, S.; Pilosof, N.; Karawani, M.; Wigler, R.; Kaufman, A.Y.; Teich, S.T. Occurrence and timing of complications following traumatic dental injuries: A retrospective study in a dental trauma department. J. Clin. Exp. Dent. 2016, 8, e429–e436. [Google Scholar] [CrossRef]
- Levin, L.; Day, P.F.; Hicks, L.; O’Connell, A.; Fouad, A.F.; Bourguignon, C.; Abbott, P.V. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction. Dent. Traumatol. 2020, 36, 309–313. [Google Scholar] [CrossRef]
- Spinas, E.; Melis, A.; Savasta, A. Therapeutic approach to intrusive luxation inju-ries in primary dentition. A clinical follow-up study. Eur. J. Paediatr. Dent. 2006, 7, 179–186. [Google Scholar] [PubMed]
- La Monaca, G.; Pranno, N.; Vozza, I.; Annibali, S.; Polimeni, A.; Bossù, M.; Cristalli, M.P. Sequelae in permanent teeth after traumatic injuries to primary dentition. Minerva Dent. Oral Sci. 2019, 68, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Lopes, T.D.S.; Santin, G.C.; Marengoni, L.A.; Crispim, J.B.; Ceron, L.C.; Fracasso, M.D.L.C. Clinical and Radiographic Sequelae in Primary Teeth due to Dental Trauma. Pesqui. Bras. Odontopediatria Clin. Integr. 2019, 19, e4526. [Google Scholar] [CrossRef]
- Spinas, E.; Deias, M.; Mameli, A.; Giannetti, L. Pulp canal obliteration after extrusive and lateral luxation in young permanent teeth: A scoping review. Eur. J. Paediatr. Dent. 2021, 22, 55–60. [Google Scholar] [CrossRef]
- Spinas, E.; Giannetti, L.; Mameli, A.; Re, D. Dental injuries in young athletes, a five-year follow-up study. Eur. J. Paediatr. Dent. 2018, 19, 187–193. [Google Scholar] [CrossRef]
- Santos, L.V.; da Hora, K.C.; Alves, A.C. Successful minimally invasive intervention in a primary central incisor after root fracture: A case report. Dent. Traumatol. 2021, 37, 807–812. [Google Scholar] [CrossRef]
- Nam, O.H.; Kim, M.S.; Kim, G.T.; Choi, S.C. Atypical root resorption following root fractures in primary teeth. Quintessence Int. 2017, 48, 793–797. [Google Scholar] [CrossRef]
- Holan, G.; Yodko, E.; Sheinvald-Shusterman, K. The association between traumatic dental injuries and atypical external root resorption in maxillary primary incisors. Dent. Traumatol. 2015, 31, 35–41. [Google Scholar] [CrossRef]
- Di Giorgio, G.; Zumbo, G.; Saccucci, M.; Luzzi, V.; Ierardo, G.; Biagi, R.; Bossù, M. Root Fracture and Extrusive Luxation in Primary Teeth and Their Management: A Case Report. Dent. J. 2021, 9, 107. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Evaluated Parameters |
|---|
| Gender and age of the patient |
| Localization of the root fracture |
| Presence of extrusion and/or other types of concomitant trauma |
| Time interval since the trauma |
| Type and duration of splinting |
| Onset of PCO |
| Follow-up and X-ray checks; results based on the type of splinting used |
| Gender | Age at Trauma (Months) | Tooth Involved | Root Fracture Position | Extrusion | Other Type of Trauma | Place of Trauma | Time from the Accident | Splint Time | Complications | PCO | Apical Fragment Resorption | Damage of Permanent Tooth |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | 30 | 6.1 | MD | Yes | VCF OI | Asylum | 4 | 60–90 | Not | Yes | Yes | Not |
| F | 32 | 5.1 | MD | Yes | OI | Asylum | 6 | 60–90 | Not | Yes | Yes | Not |
| M | 36 | 5.1 | MD | Yes | Luxation of adjacent teeth, OI | Home | 5 | 60–90 | Not | Yes | Yes | Not |
| F | 46 | 6.1 | MD/AT | Yes | Not | Outside | 18 | 60–90 | Early loss | Not | Yes | Delayed eruption |
| M | 40 | 5.1 | MD | Yes, palatal | OI | Outside | 14 | 60–90 | Not | Not | Yes | Not |
| F | 30 | 6.1 | AT | Not | Not | Home | 24 | 60–90 | Not | Yes | Yes | Not |
| M | 24 | 5.1 | AT | Yes, vestibular | Mobility | Home | 18 | 60–90 | Not | Yes | Yes | Not |
| M | 30 | 5.1 | MD | Yes | Not | Asylum | 4 | 60–90 | Not | Yes | Yes | Not |
| F | 28 | 5.1 | MD | Yes | OI | Home | 3 | 60–90 | Not | Yes | Yes | Not |
| M | 48 | 6.1 | MD | Not | Not | Outside | 19 | 60–90 | Not | Not | Yes | Not |
| M | 32 | 5.1 | AT | Not | Mobility | Home | 12 | 60–90 | Not | Not | Yes | Not |
| F | 40 | 6.1 | MD | Yes, palatal | VCF, OI | Asylum | 3 | 60–90 | Not | Yes | Yes | Not |
| M | 45 | 6.1/6.1 | AT | Not | Not | Asylum | 18 | 60–90 | Not | Not | Yes | Not |
| M | 30 | 5.1 | MD/AT | Yes, vestibular | Mobility | Home | 5 | 60–90 | Early loss | Yes | Yes | Delayed eruption |
| F | 48 | 6.1 | MD | Yes | Not | Outside | 24 | 60–90 | Not | Not | Yes | Not |
| M | 28 | 5.1 | MD/AT | Yes | OI | Home | 12 | 60–90 | Early loss | Yes | Yes | Delayed eruption |
| F | 29 | 5.1 | AT | Not | Not | Home | 20 | 60–90 | Not | Not | Yes | Not |
| M | 30 | 6.1 | MD | Yes, palatal | OI | Asylum | 4 | 60–90 | Not | Yes | Yes | Not |
| F | 44 | 6.1 | MD | Not | Not | Asylum | 6 | 60–90 | Not | Yes | Yes | Not |
| M | 30 | 5.1/6.1 | MD | Yes | Not | Home | 3 | 60–90 | Not | Not | Yes | Not |
| F | 31 | 6.1 | AT | Not | OI | Outside | 18 | 60–90 | Not | Yes | Yes | Not |
| M | 36 | 6.1 | MD | Yes, palatal | Not | Asylum | 4 | 60–90 | Early loss | Yes | Yes | Not |
| M | 38 | 5.1 | MD | Not | Mobility | Asylum | 3 | 60–90 | Not | Yes | Yes | Not |
| F | 40 | 5.1 | MD | Yes, vestibular | Not | Outside | 19 | 60–90 | Not | Yes | Yes | Not |
| M | 42 | 6.1 | MD | Not | Not | Outside | 14 | 60–90 | Not | Yes | Yes | Not |
| Gender | Age at Trauma (Months) | Tooth | Root Fracture Position | Extrusion | Other Type of Trauma | Place of Trauma | Time from the Accident | Splint Time | Complications | PCO | Apical Fragment Resorption | Type of Damage of Permanent Tooth |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | 18 | 5.1 | MT | Yes | OI | Home | <2 | 55 | Early loss | Not | Yes | Enamel dysplasia |
| M | 24 | 5.1 | MT | Not | Mobility | Outside | <2 | 28 | Not | Yes | Yes | Enamel dysplasia |
| F | 28 | 6.1 | MT | Not | Not | Home | >24 | 46 | Not | Yes | Not | Not |
| M | 26 | 5.1/6.1 | MT | Yes, palatal | OI | Asylum | <2 | 60 | Not | Not | Not | Not |
| F | 26 | 6.1 | MT | Not | Not | Outside | <2 | 60 | Early loss | Not | Yes | Enamel dysplasia |
| F | 30 | 5.1 | MT | Yes, vestibular | Mobility | Home | <2 | 25 | Early loos | Not | Yes | Enamel dysplasia |
| M | 30 | 5.1 | MT | Not | Not | Asylum | >24 | 60 | Early loss | Not | Not | Enamel dysplasia |
| M | 30 | 6.1 | MT | Yes | OI | Home | <2 | 50 | Not | Yes | Yes | Enamel dysplasia |
| M | 30 | 6.1 | MT | Yes, palatal | OI | Asylum | <2 | 15 | Early loss | Not | Yes | Enamel dysplasia |
| F | 30 | 5.1 | MT | Not | Not | Home | >24 | 25 | Early loss | Not | Yes | Not |
| M | 30 | 5.1 | AT | Not | Not | Asylum | >24 | 60 | Not | Yes | Not | Not |
| F | 30 | 5.1 | MT | Yes | OI | Asylum | <2 | 60 | Dyschromia | Yes | Yes | Not |
| M | 31 | 6.1 | AT | Yes, vestibular | Mobility | Home | <2 | 65 | Not | Yes | Yes | Not |
| M | 31 | 6.1 | MT | Not | Mobility | Home | >24 | 35 | Early loss | Not | Yes | Enamel dysplasia |
| M | 32 | 5.1 | MT | Not | Not | Asylum | >24 | 60 | Not | Not | Yes | Not |
| F | 32 | 6.1 | MT | Yes | OI | Outside | <2 | 50 | Not | Yes | Yes | Not |
| M | 32 | 5.1 | MT | Yes, palatal | OI | Outside | <2 | 40 | Early loss | Not | Yes | Enamel dysplasia |
| M | 35 | 5.1 | MT | Yes, palatal | OI | Home | <2 | 60 | Dyschromia | Yes | Yes | Not |
| M | 35 | 5.1/6.1 | MT | Yes | OI | Home | <2 | 55 | Not | Not | Yes | Delayed eruption |
| F | 36 | 6.1 | MT | Not | VCF | Outside | >24 | 60 | Not | Not | Yes | Not |
| M | 36 | 6.1 | MT | Not | Mobility | Outside | >24 | 58 | Not | Not | Yes | Delayed eruption |
| M | 37 | 5.1 | MT | Not | Not | Home | < 2 | 60 | Not | Not | Not | Delayed eruption |
| M | 38 | 5.1 | MT | Yes, palatal | OI | Home | <2 | 20 | Early loss | Not | Yes | Delayed eruption |
| F | 38 | 5.1 | AT | Yes | OI | Outside | <2 | 30 | Early loss | Yes | Yes | Delayed eruption |
| F | 38 | 6.1 | MT | Yes | OI | Outside | >24 | 30 | Early loss | Not | Yes | Delayed eruption |
| M | 40 | 6.1 | MT | Not | VCF | Playground | <2 | 28 | Early loss | Not | Yes | Delayed eruption |
| F | 40 | 6.1 | MT | Not | Not | Home | >24 | 60 | Dyschromia | Yes | Yes | Delayed eruption |
| M | 40 | 5.1 | MT | Not | Mobility | Asylum | <2 | 30 | Early loss | Not | Yes | Delayed eruption |
| M | 40 | 5.1 | MT | Yes, vestibular | Mobility | Asylum | <2 | 21 | Early loss | Not | Yes | Enamel dysplasia |
| M | 44 | 6.1 | MT | Yes, palatal | OI | Outside | <2 | 60 | Early loss | Not | Yes | Not |
| M | 44 | 5.1 | MT | Not | Not | Playground | >24 | 70 | Not | Not | Yes | Not |
| F | 45 | 6.1 | MT | Not | Not | Playground | >24 | 90 | Early loss | Not | Yes | Not |
| M | 46 | 5.1/6.1 | MT | Yes | OI | Home | <2 | 58 | Not | Not | Not | Not |
| F | 46 | 5.1 | MT | Not | VCF | Playground | >24 | 30 | Early loss | Not | Yes | Not |
| M | 46 | 5.1 | MT | Not | VCF | Playground | >24 | 45 | Early loss | Not | Yes | Not |
| Apical Fragment Resorption | |||
|---|---|---|---|
| 1 | 2 | Total | |
| 1 | 23 | 4 | 27 |
| 85.19 | 14.81 | 100.00 | |
| 2 | 29 | 9 | 38 |
| 76.32 | 23.68 | 100.00 | |
| Total | 52 | 13 | 65 |
| 80.00 | 20.00 | 100.00 | |
| Fisher’s exact = | 0.532 | ||
| Early Loss | |||
|---|---|---|---|
| 1 | 2 | Total | |
| 1 | 4 | 23 | 27 |
| 14.81 | 85.19 | 100.00 | |
| 2 | 18 | 20 | 38 |
| 47.37 | 52.63 | 100.00 | |
| Total | 22 | 43 | 65 |
| 33.85 | 66.15 | 100.00 | |
| Fisher’s exact = | 0.008 | ||
| 1 | 2 | Total | |
|---|---|---|---|
| 1 | 17 | 10 | 27 |
| 62.96 | 37.04 | 100.00 | |
| 2 | 10 | 28 | 38 |
| 26.32 | 73.68 | 100.00 | |
| Total | 27 | 38 | 65 |
| 41.54 | 58.46 | 100.00 | |
| Fisher’s exact = | 0.005 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murgia, M.S.; Zerman, N.; Cubeddu, S.; Carboni, L.; Spinas, E. A Retrospective Cohort Study of Traumatic Root Fractures in Primary Dentition: Can Splinting Type Improve Therapeutic Outcomes? Appl. Sci. 2023, 13, 6530. https://doi.org/10.3390/app13116530
Murgia MS, Zerman N, Cubeddu S, Carboni L, Spinas E. A Retrospective Cohort Study of Traumatic Root Fractures in Primary Dentition: Can Splinting Type Improve Therapeutic Outcomes? Applied Sciences. 2023; 13(11):6530. https://doi.org/10.3390/app13116530
Chicago/Turabian StyleMurgia, Martina Salvatorina, Nicoletta Zerman, Stefano Cubeddu, Laura Carboni, and Enrico Spinas. 2023. "A Retrospective Cohort Study of Traumatic Root Fractures in Primary Dentition: Can Splinting Type Improve Therapeutic Outcomes?" Applied Sciences 13, no. 11: 6530. https://doi.org/10.3390/app13116530
APA StyleMurgia, M. S., Zerman, N., Cubeddu, S., Carboni, L., & Spinas, E. (2023). A Retrospective Cohort Study of Traumatic Root Fractures in Primary Dentition: Can Splinting Type Improve Therapeutic Outcomes? Applied Sciences, 13(11), 6530. https://doi.org/10.3390/app13116530