Abstract
Total ankle replacement (TAR) is the replacement of a damaged arthritic ankle joint with a prosthetic implant to eliminate the source of resultant pain and swelling. Historically, however, the ankle joint has been one of the most difficult joints to analyze and replicate for successful replacement due to its complex anatomy and multiplanar motion. Ankle fusion, the standard of care for end stage ankle arthritis, has excellent functional outcomes but results in loss of motion at the joint. TAR was first attempted in the 1970s and by the early 1990s, prosthesis designs more closely mirrored the natural anatomy of the ankle and TAR was no longer considered an experimental procedure. Although the outcomes of TAR have significantly improved over this short period of time, there are still many areas that warrant further investigation including (1) optimal patient selection, (2) number of prosthesis components, (3) bearing type, (4) revision rates and causes and (5) comprehensive finite element models (FEM) of the ankle. The main goal of this paper is to present a literature review on the background and evolution of TAR, the current state of practice and prosthesis types and challenges and directions for future improvement.
1. Introduction
1.1. Background
The ankle or tibiotalar joint has distinctive anatomic and biomechanical characteristics that allow it to withstand high mechanical stress and strain over a lifetime. The joint is comprised of the distal aspect of the fibula and tibia which articulate with the talus. Its unique geometry involving an oblique axis of rotation contributes to its multiple planes of motion including dorsiflexion, plantarflexion, inversion and eversion [1]. Studies have shown that each 1 mm of talar shift results in roughly 40% decrease in the contact surface area at the tibiotalar joint [2]. Such a change can precipitate the development of arthritis, a degenerative disease that is painful and debilitating. For many years, ankle arthrodesis, or ankle fusion, was the only definitive surgical treatment of primary osteoarthritis (OA), inflammatory arthritis, or post-traumatic arthritis of the ankle joint. This is still an effective treatment which results in consistent pain relief and high functional outcomes. However, it inherently results in loss of motion at the tibiotalar joint by fusing the talus to the tibia which leads to altered gait mechanics. Ankle fusion also increases stress seen at adjacent joints, leading to arthritic changes in other joints of the foot over time [3,4].
The goal of total ankle replacement (TAR) was to address these issues. By the early 1990s, the techniques and prostheses used in TAR had sufficiently developed to start to rival the outcomes of arthrodesis, making TAR a viable alternative to fusion [5,6,7].
A diagram of the basic components of the ankle joint is shown in Figure 1 below. The ankle joint involves the fibula, tibia and talus. Based on the outcomes for both ankle arthrodesis and total ankle replacement, it is evident that there is still not a complete understanding of the physiological mechanics of the ankle complex. Geometrical studies of human joints aim to show how ligaments and shapes of the articular surfaces can guide the movements of the bones upon each other. Mechanical studies show how ligaments can act together with the muscles and articular surfaces to transmit load from one bone to the other. Understanding the role of all structures in the ankle joint is important for a successful design of joint replacement prostheses. In end stage ankle arthritis, total ankle replacement is considered as a means to reduce pain and restore joint stability and mobility. Compared to the population without ankle arthritis, patients have prolonged stance time, shortened stride length, increased cadence and a slower walking speed. Ankle arthrodesis has been shown to improve these metrics from preoperatively to post operatively [8]. However, after TAR, there is less change to the natural motion at the ankle joint complex when compared to arthrodesis [9]. This makes TAR an attractive option when compared to ankle arthrodesis.
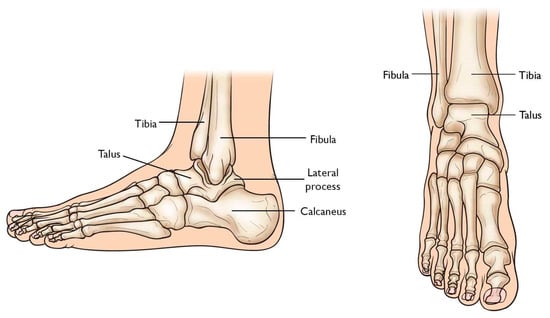
Figure 1.
Simple schematic of the ankle joint.
From the first total ankle replacement in the 1970s TAR has had a steep evolutionary progress with improved reproducible results. The first generation of the implant had two-main component cemented designs that were either unconstrained or constrained. Both types of design eventually fell out of favor because of poor survivorship due to significant bone loss required for component placement, implant incongruency leading to stress deformation and component loosening leading to failure [10].
As technology progressed, second and third-generation prostheses used ultra-high molecular weight polyethylene (UHMWPE) as the spacer. The most current designs can be considered fourth generation. These subsequent generations of prostheses can be categorized by component number (two or three) and device type (fixed bearing or mobile bearing). Figure 2 below shows the difference between fixed-bearing prosthesis and mobile-bearing prosthesis.
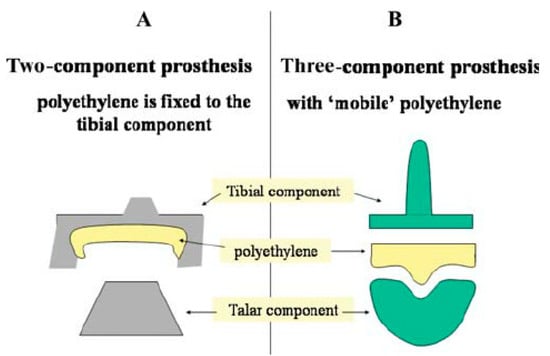
Figure 2.
Difference between fixed-bearing prosthesis and a mobile-bearing prosthesis, where the polyethylene component is either fixed to the tibial component or free to move [11].
While each generation of ankle prostheses has advanced outcomes, a difficulty of this procedure is that the ankle joint is extremely difficult to model due to its unique articular characteristics. Compared to total hip and knee replacements, TAR is still a procedure that lacks the same long-term success rates, though part of this is due to its more recent advent leading to inherent limitations in longer term outcome data. When loaded, the ankle joint has a smaller area of contact between the articulating surfaces when compared to the hip and knee. At the same load of 500 N, the contact area for the ankle is 350 mm2, compared to 1120 mm2 for the knee and 1100 mm2 for the hip. Thus, the smaller contact area signifies a higher normal peak stress in the ankle [12]. Further, the articular cartilage in the ankle has different tensile and thickness properties than that of the knee and hip. These complexities in the ankle joint make it a more challenging joint to model and to improve upon.
1.2. Contribution
This paper provides a comprehensive review of the history, evolution and the current state of TAR. The five main categories and specifications that describe the various types of implants and the methodologies used for further improvement of TAR prostheses are discussed in detail. These categories and areas where work is still in progress includes (1) optimal patient selection, (2) number of prosthesis components, (3) bearing type, (4) revision rates and causes and (5) comprehensive finite element models (FEM) of the ankle. These five areas have been the focus of research on improvement of TAR operative techniques, post-operative recovery and prosthesis longevity. While TAR has certainly progressed from its early implementation, there are still essential areas of research that will improve the function and long term outcomes.
Proper patient selection is essential for the success and survival of any type of joint arthroplasty, including TAR. Indications for TAR, however, are still being defined. Traditional indications have been patients that are >50 years old with end-stage ankle arthritis, minimal deformity at the ankle joint, non-obese, with lower mobility demands. However, these indications are continuing to evolve, as younger patients with inflammatory or post-traumatic arthritis may also be good candidates for this procedure [13,14,15,16].
First generation TAR implants were composed only of two-component constrained or unconstrained designs with a polyethylene component without a separate bearing. Second and third generation designs progressed to include three-component systems allowing mobile-bearing with independent mobility of the spacer as it articulates with the tibial and talar components.
Fixed bearing systems utilize highly congruent components with one articulation between the tibial and talar components where the polyethylene insert is attached to one of the components. This requires greater constraint in order to provide stability.
Mobile bearings involve two articulating surfaces, where a moving polyethylene bearing acts as a meniscus between the tibial and talar components. The goal of this construct is to allow for greater stress distribution and theoretically decrease the risk of having points of high concentrated stress between components. Currently, Stryker’s Scandinavian Total Ankle Replacement (STAR) implant is the first and only three component mobile bearing ankle implant with FDA approval in the United States. The remaining TAR implants in use in the United States are fixed bearing.
Bearing type–either fixed or mobile–has not been shown to affect clinical outcome [17]. Figure 3 below shows one design of a TAR.
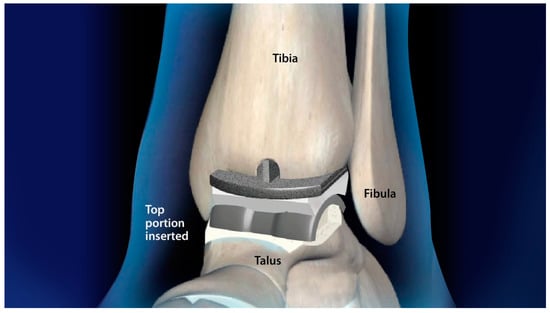
Figure 3.
Rendering of the Salto Talaris total ankle replacement system, which is a fixed bearing design.
Wear in the polyethylene component is one of the main causes of revision in TAR. Debris from polyethylene wear can cause osteolysis at the interface between the bone and the implant, leading to aseptic loosening. Further, high contact pressures and subsurface stresses also contribute to polyethylene liner wear over time. Currently, TAR has almost double the number of revisions when compared to hip and knee replacements. This is partly due to the relatively high stresses experienced in the ankle, 64% higher than that of the knee and 45% more than that of the hip. Thus, TAR prostheses must be designed to withstand much higher stresses than other joints [18].
Understanding the stress-strain distribution, plantar pressures and wear on the polyethylene liner are important parameters for improving TAR prostheses. Comprehensive analysis of the biomechanical nature of the ankle is needed before prostheses can be improved, which is when FEM becomes essential. This will help create ankle replacement prostheses that will better mimic the motion of normal ankle function and ideally prolong implant longevity. Axial loading is the main contributor to prosthesis wear, but shear and torsional loading also contribute. FEM is one of the most important aspects of ankle replacement research, as it allows for better understanding of ankle biomechanics, which will help to improve TAR prostheses.
2. TAR System Study
2.1. Indications
Patient selection is critical for successful TAR outcomes. Most literature suggests that the ideal TAR candidate is older, has low mobility demand, non-obese and without significant deformities or malalignment in order to minimize demands on the implant and prolong longevity [5,14,19,20].
While there are no randomized controlled studies showing a correlation between patient age and revision rates, the concern with TAR in younger patients is the increased demand on the implant requiring inherently greater survivorship. A comparison of functional outcomes in patients > 70 years old, compared to those 50–60 years old has shown equivalent improved outcomes in both cohorts at mean 2 year follow up [15]. Outcomes comparing patients < 55 years old, 55–70 years old and >70 years old also have shown positive, comparable results at mean 3.5 years follow up [16]. Therefore as prostheses have evolved, these indications are continuing to change as well. Additionally, lower demand younger patients such as those suffering from juvenile rheumatoid arthritis present a unique patient population in which TAR may be con
sidered in order to prevent increased stress on adjacent joints over time that would occur with ankle arthrodesis [21].
Preoperative ankle range of motion is another important consideration. TAR will not significantly improve range of motion, but rather, preserves the motion that a patient already has [22]. However, this alone does not predict functional outcomes, as TAR in patients with stiff ankles can still produce positive clinical results [23,24].
Patient BMI must be considered, as increased BMI can negatively affect the prosthesis longevity. Increased BMI has previously been established in total knee arthroplasty and total hip arthroplasty literature as a modifiable risk factor for perioperative complications and long term outcomes [25,26].
However, there is no consensus on optimal BMI cutoffs. A comparison of TAR in obese and non-obese patients has shown similar functional improvement in both cohorts without significant increased complication rate in obese patients [27,28].
Therefore a careful preoperative discussion should be had with these patients rather than eliminating TAR as a viable option in these patients.
Coronal and sagittal plane deformity and alignment must be assessed in order to evaluate viability of TAR. Prior coronal plane deformity correction was limited to >20 degrees or valgus or >15 degrees of varus [29].
However these limitations also continue to be evaluated as prosthesis designs improve [30,31,32]. Therefore all of these factors must be taken into consideration together in order to assess for the role of TAR as a surgical treatment for a patient’s end stage ankle arthritis.
2.2. Component Number
Currently, there are both two and three component systems on the market for TAR, both of which have advantages and disadvantages. Neither has been shown to be definitively superior.
The only three-component system that is currently approved by the Food and Drug Administration (FDA) is the STAR implant from Stryker. The mobile polyethylene component allows for rotation and translation to theoretically reduce the stress at the junction of the implant and the bone interface [33]. Initial outcomes with STAR showed promising functional results, but with concern for peri-implant osteolysis [34]. Later studies confirmed positive functional outcomes and consistent pain relief, but noted a high rate of revision surgery at 10 years post operatively [35] is another mobile bearing implant, but is currently used in Europe and Canada and not approved for use in the US.
Two-component systems have a conforming saddle geometry and large surface area to distribute stress, theoretically leading to decreased wear [36].
A study that followed 20 patients with a two-component system and 20 patients with a three-component system found that both types of systems significantly improved quality of life for patients. However, when compared to a control group that did not undergo TAR, all 40 patients scored lower on spatial-temporal and functional parameters and did not achieve the normal locomotion patterns of the control group. A clinical difference in outcomes between two or three component systems has not been shown [37,38].
2.3. Bearing Type
Both fixed and mobile-bearing systems exist for TAR implants. The main difference between these two designs is rotation, where the fixed-bearing systems have rotation dictated by the tibial component, while mobile-bearing systems allows translation and rotational movement [39].
Research on implant migration in fixed-bearing systems with a modular stem has shown that the implant continues to migrate for up to 2 years, with an average migration of up to 2 mm. This has shown to be greater in males than females, possibly due to having greater compressive forces in their ankle. This is consistent with previous studies in the knee showing that the prosthesis often needs to “settle”, which can take up to 2 years after the initial operation [40].
A prospective study carried out between 2017 and 2020 compared preoperative and postoperative gait patterns in patients undergoing TAR with fixed bearing implants. Ankle range of motion was maintained from midstance to pre-swing during gait postoperatively. Further, TAR was shown to improve kinematic motion of the hindfoot joints. However, post TAR kinematics were not restored to that of controls without ankle arthritis.
The authors therefore recommend that multi-segment foot modeling is relevant when assessing the outcome of TAR [41].
Another study evaluated polyethylene wear in fixed bearing systems where the polyethylene insert is fixed to the tibial component. Fourteen polyethylene liners were removed from uncemented, fixed bearing total ankle replacements for analysis of wear patterns. The liners were analyzed for burnishing, scratching, mechanical damage, pitting and embedded particles and showed increased wear posteriorly compared to anteriorly. It was theorized that the constraints for anterior to posterior translation of the talus may contribute to this pattern. The heterogeneity in damage supports a non-uniform stress distribution, which could lead to edge loading and eventual failure [42].
Mobile-bearing systems have three unconstrained tibial, talar and polyethylene components, with the theoretical advantage of better stress distribution. However, it can be challenging to determine the ankle axis of rotation and the rotation between tibial and talar components has been shown to have wide variation after mobile-bearing TAR. A study carried out on mobile-bearing TAR showed measurable motion between the mobile-bearing polyethylene insert and the tibial component, emphasizing the importance of axial rotation [43]. A study in the United Kingdom on patient outcomes after uncemented, mobile bearing TAR found equivalent functional and radiographic outcomes in patients receiving TAR for osteoarthritis, post traumatic arthritis and rheumatoid arthritis. Moreover, there was no statistically significant correlation between preoperative deformity and postoperative function. Any preoperative anterior translation was corrected in all groups postoperatively with good patient-reported outcomes. A mobile-bearing design may therefore be more forgiving when compared to a fixed-bearing design if there is incomplete component alignment [44].
A concern specific to mobile bearing implants is the reported high rates of polyethylene failure and periprosthetic osteolysis. A study on 99 HINTEGRA mobile bearing TAR, a prosthesis used commonly in Europe and Canada, found radiographic osteolysis in 37.4% at mean 40 month follow up. Sixty seven percent of these had progression of their radiographic osteolysis, but not all of these were clinically symptomatic. Similarly, mean 159 month follow up of STAR outcomes showed osteolytic lesions in 50% of patients despite 93.9% implant survival rate at 10 years [45]. Therefore the relationship between these radiographic findings and clinical outcomes remains to be elucidated.
Current data shows favorable patient-reported and clinical outcomes for both mobile and fixed bearing TAR designs, without significant clinical difference. A prospective randomized trial compared mobile bearing STAR and fixed bearing Salto-Talaris TAR in 100 patients found no significant functional, radiographic or clinical difference in outcomes at mean 4.5 year follow up. All patients demonstrated statistically significant improvement in all clinical measures. However, there was a significantly higher rate of radiographic peri-talar implant lucency and tibial and talar implant subsidence in the mobile bearing group. There was a significantly higher rate of reoperation in the mobile bearing group performed to decompress mechanical impingement or cyst treatment, but not for component revision [46,47].
3. Revision TAR
Revision TAR is performed for a variety of reasons: implant failure due to septic or aseptic loosening, component subsidence, or mechanical impingement.
The rate of major revision in TAR is low, at <5% at 5 years [48]. A systemic review of clinical studies on TAR revision rates over the last decades showed a 12.6% revision rate within 7 years after surgery [49].
However, revision rates continue to be nearly double those seen in total hip and knee replacements. This is partly due to the different biomechanical factors that affect the ankle joint. The small contact area between the talus and tibia experiences forces four to seven times body weight with normal walking, resulting in extremely high contact stresses in TAR. In conjunction with the relatively low yield point and wear resistance of ultra-high molecular weight polyethylene (UHMWPE), these high stresses contribute greatly to failures in the TAR liners. One cause of aseptic loosening is wear debris created during joint articulation. A study found that up to 54% of TAR revision surgeries may be directly or indirectly caused by the wear of UHMWPE liners. Because UHMWPE wear not only contributes to instability in the joint as the surface decays but also produces UHMWPE debris, these liners are one of the main causes of revision [43].
Despite increases in TAR prevalence and surgical volume over the last two decades, TAR is still a significantly less commonly performed surgery compared to total knee and total hip replacements. Reoperation rates have been shown to be higher in surgical centers or by surgeons that perform < 20 TAR a year, demonstrating that there is a learning curve and technical skill plays a role in successful outcomes [50].
Moreover, as with other joint replacements, appropriate patient selection is critical, as patient factors play a role in TAR failure. Diabetes, peripheral vascular disease, chronic pulmonary disease and alcohol abuse have been shown to significantly increase risk for early failure within 5 years post operatively [51]. Despite traditional recommendations to reserve TAR for older patients, analysis of 10-year implant survivorship showed no significant difference in revision rates between patients older than 50 and those younger than 50 years old [52].
Dynamic ultrasonography has been successfully used in cadaveric models to evaluate motion at the bone–prosthesis interface in TAR. Dynamic ultrasonography can directly visualize motion at the bone-prosthesis interface, in contrast to plain radiograph and CT scanning, where static images are evaluated for lucencies that suggest loosening. This could possibly allow for early identification of component aseptic loosening, prior to loss of significant bony architecture [53,54,55].
3.1. Finite Element Modeling
Comprehensive finite element modeling (FEM) is essential to improve future designs of TAR. It is necessary to understand the biomechanics of the ankle and adjacent joints before the analysis of an implanted ankle prosthesis can begin. FEM allows for realistic implant modeling, as in vivo experiments are invasive, costly, time consuming and clinically impractical [56,57].
There have been many iterations of models of the ankle joint used to analyze the midterm and long-term outcomes of primary and revision TAR. These models have been used to validate biomechanical bases of prosthesis components. In one such study, researchers instrumented uncemented mobile-bearing tibial component of a TAR in eight cadaveric tibias in three different positions to validate a FEM of TAR. An axial force was applied to the implants in each of the positions. CT scans were used to evaluate the anatomy of the tibias, to assess implant position and to gauge the environment at the bone-implant interface. The combination of this data was used to calculate bone strains. The finite element model was implemented in Abaqus and analyzed with an implicit solver. Both the predicted and measured strains were highly correlated with a coefficient of determination of 0.91. This model showed great potential for understanding local biomechanics and could assist in optimizing implant design, fixation and positioning [58].
FEM can also be used to understand the stress and wear in TAR. One of the most common reasons for revision is due to polyethylene liner wear [59,60,61,62]. A model of the axial loading profile was coupled with Hertzian contact mechanics to develop a new model to evaluate the maximum contact pressure in TARs. Then, optimization models were developed to consider the geometric characteristics of the TAR systems that could be altered to minimize stress. FEM and mathematical analysis determined that contact area between the talar and polyethylene components was a significant contributor to total stresses in TAR. This information can be utilized to design new generations of TARs that reduce fretting wear and delamination in the UHMWPE liners. One way to decrease contact and subsurface stresses is through optimization of the implant geometry to decrease wear rate. Optimization models are powerful tools to help design new low-stress implants [43].
Similarly, another FEM was used to assess the kinematics and contact pressures in a three-component TAR when subjected to forces of a typical gait cycle. The FEM incorporated a previously validated model of the ankle joint. During the simulated stance phase, the models reported reaction forces that remained within physiologic values. The maximum experienced force was below the load at failure. This model was able to allow the necessary range of motion with maintained constrained motion of the prosthetic components. The congruency of the design led to small peak contact pressures that were almost evenly distributed [63].
The number of segments used in foot modeling has also been shown to affect the calculated gait kinetics. The older one segment foot models overestimate ankle joint range of motion and power generated. A multi-segment foot model is more accurate when assessing the outcome of total ankle replacement [64].
The use of FEM is therefore essential to understanding ankle biomechanics, which will provide the foundation for improving upon current TAR prostheses. Analyzing specific TAR implants can better elucidate what works well and what needs improvement. The limitations of FEM lie in what assumptions can be made when modeling in terms of material properties, loading directions and articulating surfaces. Further research, such as the utilizing specific patient’s information such as a CT based information, to be utilized in finite element modeling, can improve the understanding of how TAR prostheses interact in vivo.
3.2. Current Prostheses
There are a number of prostheses that are currently used and available in the United States. The available implant systems include the STAR device, INBONE II TAR, INVISION TAR, INFINITY TAR, Salto Talaris TAR, Salta Talar XT Revision prosthesis, Zimmer Trabecular Metal TAR, Vantage TAR and Cadence TAR [12]. The most commonly implemented TAR systems in the US are the INBONE, INFINITY, STAR and Vantage [65,66,67].
STAR is an original second-generation implant that has undergone several revisions. This implant was originally developed by Stryker and is now owned by DJO Global. This is an unconstrained mobile bearing implant, but was originally a two-component cemented system. Currently, it is the only mobile bearing, cementless system approved for use in the United States [33,68]. Though studies have shown high patient satisfaction, there is concern for high rates of polyethylene failure and periprosthetic osteolysis with this prosthesis [45,69,70]. Figure 4 below shows the STAR ankle prosthesis.

Figure 4.
STAR ankle prosthesis rendering in the foot.
The INBONE II and INVISION total ankle replacement systems were both made by Wright Medical Technologies. Wright Medical was bought by Stryker, thus these implants are now owned by Stryker.. These are both two-component, fixed-bearing systems used for both primary and revision TAR. The INBONE II system evolved from the INBONE I system, which was a third-generation design cleared by the FDA in 2005. The INBONE II includes a change in talar design from flat to including a sulcus, in order to improve the stability between the polyethylene liner and talar component [71].
The INFINITY system is a fourth-generation design that is also a two-component, fixed bearing device. INFINITY design components can be used with the Prophecy, which is Infinity total ankle replacement with patient specific instrumentation. This implant uses preoperative ankle CT to develop patient specific cut guides. Patient specific instrumentation has been shown to decrease operative time with reproducible and accurate results [72,73,74].
Prophecy’s prosthesis can also be used with the INBONE II, INFINITY and INVISION TAR [33,75,76,77]. Figure 5 below shows the INBONE prostheses.
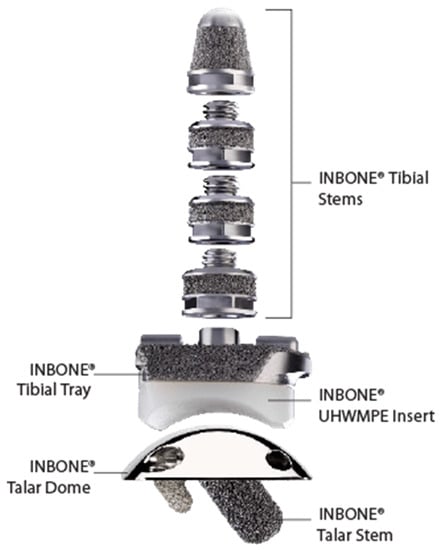
Figure 5.
INBONE prostheses and the labeled components.
The Salto Talaris TAR is a third-generation implant that was originally designed as a mobile-bearing device. In 2006, the FDA approved a fixed-bearing, two-component version of the implant that is available in the US. The Salto Talaris XT Revision Ankle Prosthesis is a fixed-bearing, semi-constrained system that can be used for both primary and revision surgery. The implant is somewhat unique in that the tibial trial component is mobile, which uses the talar component to guide it to settle and self-align in the optimal position on the resected distal tibia surface [78].
The talar component uses the same general design as the primary implant [32]. Mid- and long term results of this implant have shown consistent positive results with significant increase in patient reported clinical outcomes [47,79].
The Zimmer Trabecular Metal TAR is a third-generation, two-component, fixed-bearing system that uses a trans-fibular approach for implantation. This makes it the only laterally based TAR in the US, which avoids the anterior-based incision over the ankle joint to minimize wound healing issues. This approach also provides the ability to perform curved bone cuts which are more anatomic and biomechanically provide greater bony support [80].
The polyethylene spacer is made of highly cross-lined polyethylene (HXLPE) that has decreased wear and less debris when compared to standard spacers [33]. Figure 6 below shows the Zimmer TAR.
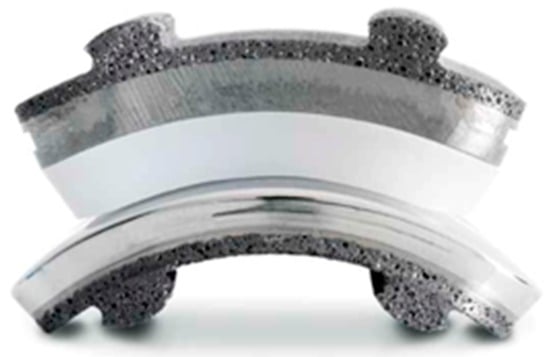
Figure 6.
Zimmer TAR prosthesis.
Finally, the Cadence and Vantage TARs are the newest systems. The Cadence is a fourth-generation, two-component, fixed-bearing implant that gained FDA clearance in 2016. The liner is made of HXLPE and the system reduces contact and frictional forces against the fibula with a recess in the tibia component. The Vantage TAR was also cleared by the FDA in 2016 and has both two- and three-component designs. However, in the United States, it is available only as a fixed-bearing device that has a spacer “clipped” into the tibial component [33,81]. In Vantage, which is a fixed bearing and not a mobile bearing, polyethene is attached to tibial component. Both of these implants have shown positive short term radiographic and clinical results [82,83]. Figure 7 below shows both the Vantage TAR and the Cadence TAR.

Figure 7.
The Vantage TAR is shown on the left and the Cadence TAR is shown on the right.
4. Conclusions
There are many areas of TAR that are still being researched and developed to improve outcomes. The impact of younger age and higher body mass impact on the outcomes of TAR need to be further explored. Clearly-defined patient selection will help optimize outcomes. Both two- and three-component systems, as well as fixed and mobile bearing implants have shown positive clinical outcomes, but more research is needed to determine which is best long term.
Further research is needed to decrease revision rates by optimizing the geometrical shape of the components, improve surface articulation and to better distribute and reduce contact stresses. FEM can allow for analysis of all these variables to further improve designs of TAR and improve implant longevity and patient outcomes.
Author Contributions
Conceptualization, J.Y.O.; methodology, M.N., N.B.N. and W.A.A.; software, J.Y.O. and N.B.N.; formal analysis, M.N. and W.A.A.; investigation, J.Y.O.; resources, M.N., N.B.N. and W.A.A.; writing—original draft preparation, J.Y.O.; writing—review and editing, M.N., N.B.N. and W.A.A.; visualization, N.B.N., W.A.A.; supervision, M.N.; project administration, J.Y.O., M.N., N.B.N. and W.A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blockett, C.L.; Graham, J.C. Biomechanics of the ankle. Orthop. Trauma 2016, 30, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, P.L.; Hamilton, W. Changes in tibiotalar area of contact caused by lateral talar shift. J. Bone Jt. Surg. Am. 1976, 58, 356–357. [Google Scholar] [CrossRef]
- Muir, D.C.; Amendola, A.; Saltzman, C.L. Long-term outcome of ankle arthrodesis. Foot Ankle Clin. 2002, 7, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Coester, L.M.; Saltzman, C.L.; Leupold, J.; Pontarelli, W. Long-term results following ankle arthrodesis for post-traumatic arthritis. J. Bone Jt. Surg. Am. 2001, 83, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Heuvel, A.; van bouwel, S.; Dereymaeker, G. Total ankle replacement Design evolution and results. Acta Orthop. Belg. 2010, 76, 150–161. [Google Scholar]
- Nathan, C.H.; Sang-Hyun, P.; Patricia, C.; Douglas, W.V.C.; Edward, E.; Sophia, S. Damage patterns in polyethylene fixed bearings of retrieved total ankle replacements. Foot Ankle Surg. 2021, 27, 316–320. [Google Scholar] [CrossRef]
- Hordyk, P.J.; Fuerbringer, B.A.; Roukis, T.S. Sagittal Ankle and Midfoot Range of Motion Before and After Revision Total Ankle Replacement: A Retrospective Comparative Analysis. Foot Ankle Surg. 2018, 57, 521–526. [Google Scholar] [CrossRef]
- Brodsky, J.W.; Kane, J.M.; Coleman, S.; Bariteau, J.; Tenenbaum, S. Abnormalities of gait caused by ankle arthritis are improved by ankle arthrodesis. Bone Jt. J. 2016, 98, 1369–1375. [Google Scholar] [CrossRef]
- Flavin, R.; Coleman, S.C.; Tenenbaum, S.; Brodsky, J.W. Comparison of gait after total ankle arthroplasty and ankle arthrodesis. Foot Ankle Int. 2013, 34, 1340–1348. [Google Scholar] [CrossRef]
- Henne, T.D.; Anderson, J.G. Total ankle arthroplasty: A historical perspective. Foot Ankle Clin. 2002, 7, 695–702. [Google Scholar] [CrossRef]
- Gougoulias, N.; Khanna, A.; Maffulli, N. History and evolution in total ankle arthroplasty. Br. Med. Bull. 2008, 89, 111–151. [Google Scholar] [CrossRef] [PubMed]
- Bonasia, D.E.; Dettoni, F.; Femino, J.E.; Phisitkul, P.; Germano, M.; Amendola, A. Total ankle replacement: Why, when and how? Iowa Orthop. J. 2010, 30, 119–130. [Google Scholar] [PubMed]
- Usuelli, F.G.; Maccario, C.; D’Ambrosi, R.; Surace, M.F.; Vulcano, E. Age-related outcome of mobile- bearing total ankle replacement. Orthopedics 2017, 40, e567–e573. [Google Scholar] [CrossRef] [PubMed]
- Easley, M.E.; Vertullo, C.J.; Urban, W.C.; Nunley, J.A. Total ankle arthroplasty. J. Am. Acad. Orthop. Surg. 2002, 10, 157–167. [Google Scholar] [CrossRef]
- Tenenbaum, S.; Bariteau, J.; Coleman, S.; Brodsky, J. Functional and clinical outcomes of total ankle arthroplasty in elderly compared to younger patients. Foot Ankle Surg. 2017, 23, 102–107. [Google Scholar] [CrossRef]
- Demetracopoulos, C.A.; Adams, S.B., Jr.; Queen, R.M.; DeOrio, J.K.; Nunley, J.M.; Easley, M.E. Effect of age on outcomes in total ankle arthroplasty. Foot Ankle Int. 2015, 36, 871–880. [Google Scholar] [CrossRef]
- Queen, R.M.; Franck, C.T.; Schmitt, D.; Adams, S.B. Are there differences in gait mechanics in patients with a fixed versus mobile bearing total ankle arthroplasty? A randomized trial. Clin. Orthop. Relat. Res. 2017, 475, 2599–2606. [Google Scholar] [CrossRef]
- Martinelli, N.; Baretta, S.; Pagano, J.; Bianchi, A.; Villa, T.; Casaroli, G.; Galbusera, F. Contact stresses, pressure and area in a fixed-bearing total ankle replacement: A finite element analysis. BMC Musculoskelet Disord. 2017, 18, 493. [Google Scholar] [CrossRef]
- Protheroe, D.; Mulroy, M. An update on Total Ankle Replacement survivorship rates and future directions for patient selection. Sport. Orthop. Traumatol. 2020, 36, 60–69. [Google Scholar] [CrossRef]
- Rodrigues-Pinto, R.; Muras, J.; Oliva, X.M.; Amado, P. Total ankle replacement in patients under the age of 50. Should the indications be revised? Foot Ankle Surg. 2013, 19, 229–233. [Google Scholar] [CrossRef]
- Wansbrough, G.; Sharp, R.; Cooke, P. Total ankle replacement in juvenile chronic arthritis. Orthop. Proc. 2012, 94, 32. [Google Scholar]
- Roxa, R.; Nicola, K.; Roman, S.; Tamara, H.; Alexej, B.; Beat, H. Ankle range of motion following 3-component total ankle arthroplasty. Foot Ankle Int. 2021, 42, 31–37. [Google Scholar]
- James, W.B.; Justin, M.K.; Akira, T.; Scott, C.; Yahya, D. Role of total ankle arthroplasty in stiff ankles. Foot Ankle Int. 2017, 38, 1070–1077. [Google Scholar]
- James, W.B.; Justin, M.K.; Andrew, W.P.; David, D.V.; Scott, C.; Yahya, D. Role of Total Ankle Arthroplasty in Stiff Ankles–Long Term Follow-Up. Foot Ankle Int. 2019, 4, 2473011419S00013. [Google Scholar]
- David, E.D.; Scott, A.M.; Christopher, N.C.; Natalie, A.G.; Timothy, S.B.; Nicholas, A.B. What is the Impact of Body Mass Index Cutoffs on Total Knee Arthroplasty Complications? Arthroplasty 2022, 37, 683–687. [Google Scholar]
- Jaiben, G.; Nicolas, S.P.; Mitchell, N.; Nipun, S.; Anton, A.K.; Michael, A.M. Association between body mass index and thirty-day complications after total knee arthroplasty. Arthroplasty 2018, 33, 865–871. [Google Scholar]
- Oliver, N.S.; Sahitya, K.D.; Ying, Z.; Steven, L.H. The impact of obesity on the outcome of total ankle replacement. Foot Ankle Int. 2015, 97, 904–910. [Google Scholar]
- Alexej, B.; Markus, K.; Andrew, E.A.; Beat, H. Total ankle replacement in obese patients: Component stability, weight change, and functional outcome in 118 consecutive patients. Foot Ankle Int. 2011, 32, 925–932. [Google Scholar]
- Haskell, A.; Mann, R.A. Ankle arthroplasty with preoperative coronal plane deformity: Short-term results. Clin. Orthop. Relat. Res.® 2004, 424, 98–103. [Google Scholar]
- Hanselman, A.E.; Powell, B.D.; Santrock, R.D. Total ankle arthroplasty with severe preoperative varus deformity. Orthopedics 2015, 38, e343–e346. [Google Scholar] [CrossRef]
- Sung, K.S.; Ahn, J.; Lee, K.H.; Chun, T.H. Short-term results of total ankle arthroplasty for end-stage ankle arthritis with severe varus deformity. Foot Ankle Int. 2014, 35, 225–231. [Google Scholar] [CrossRef]
- Queen, R.M.; Adams, S.B., Jr.; Viens, N.A.; Friend, J.K.; Easley, M.E.; Deorio, J.K.; Nunley, J.A. Differences in outcomes following total ankle replacement in patients with neutral alignment compared with tibiotalar joint malalignment. Bone Jt. Surg Am. 2013, 95, 1927–1934. [Google Scholar] [CrossRef] [PubMed]
- Roberto, A.B.; Mark, A.P.; Christopher, F.H. Current and Emerging Insights on Total Ankle Replacement. Podiatry Today. HMP Glob. Learn. Netw. 2018. Available online: https://www.hmpgloballearningnetwork.com/site/podiatry/current-and-emerging-insights-total-ankle-replacement. (accessed on 29 November 2022).
- Mann, J.A.; Mann, R.A.; Horton, E. STAR™ ankle: Long-term results. Foot Ankle Int. 2011, 32, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Jastifer, J.R.; Coughlin, M.J. Long-term follow-up of mobile bearing total ankle arthroplasty in the United States. Foot Ankle Int. 2015, 36, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.; DeOrio, J. The INBONE Total Ankle Replacement. Oper. Tech. Orthop. 2010, 20, 201–210. [Google Scholar] [CrossRef]
- Giada, L.; Paolo, C.; Alberto, L.; Maurizio, O.; Antonio, M.; Sandro, G.; Lisa, B. Retrospective comparison between a two- and three-component ankle arthroplasty: Clinical and functional evaluation via gait analysis. Clin. Biomech. 2020, 80, 105180. [Google Scholar] [CrossRef]
- Leardini, A.; O’Connor, J.J.; Giannini, S. Biomechanics of the natural, arthritic, and replaced human ankle joint. Foot Ankle Res. 2014, 7, 8. [Google Scholar] [CrossRef]
- Helka, K.; Sami, K.; Ia, K.; Hannu, T. The motion between components in a mobile-bearing total ankle replacement measured by cone-beam CT scanning. Foot Ankle Surg. 2022, 28, 324–330. [Google Scholar] [CrossRef]
- Stephen, A.B.; Garrett, M.W.; Melissa, M.G.; Scott, T.B.; Nicole, M.P. Evaluating Component Migration After Modular Stem Fixed-Bearing Total Ankle Replacement. Foot Ankle Surg. 2015, 54, 326–331. [Google Scholar] [CrossRef]
- Paul-André, D.; Alexandre, N.; Laurence, C.; Raphaël, D.; Bernhard, D.B.; Ivan, B.; Jean-Luc, B.; Thibaut, L. Changes in ankle and foot kinematic after fixed-bearing total ankle replacement. Biomechanics 2022, 136, 111060. [Google Scholar] [CrossRef]
- Anders, H.; Stanislav, P.; Urban, R. Six-year results of the Rebalance mobile bearing total ankle replacement. Foot Ankle Surg. 2021, 27, 66–69. [Google Scholar] [CrossRef]
- Bradley, J.E.; Dinesh, G.; Tarun, G. Finite element analysis of stress and wear characterization in total ankle replacements. Mech. Behav. Biomed. Mater. 2014, 34, 134–145. [Google Scholar] [CrossRef]
- Johnson-Lynn, S.; Siddique, M. The Effect of Sagittal and Coronal Balance on Patient-Reported Outcomes Following Mobile-Bearing Total Ankle Replacement. Foot Ankle Surg. 2019, 58, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.S.; Lee, J.; Choi, W.J.; Lee, J.W. Periprosthetic osteolysis after total ankle arthroplasty. Foot Ankle Int. 2014, 35, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Nunley, J.A.; Adams, S.B.; Easley, M.E.; DeOrio, J.K. Prospective Randomized Trial Comparing Mobile-Bearing and Fixed-Bearing Total Ankle Replacement. Foot Ankle Int. 2019, 40, 1239–1248. [Google Scholar] [CrossRef]
- Matthew, G.S.; Cindy, L.G.; Samuel, B.A.; James, K.D.; Mark, E.E.; James, A.N. Midterm results of the Salto Talaris total ankle arthroplasty. Foot Ankle Int. 2017, 38, 1215–1221. [Google Scholar] [CrossRef]
- Pagenstert, G.; Wimmer, M.D.; Jacxsens, M.; Saltzman, C.L.; Barg, A. Aseptic loosening of total ankle replacement: One-stage revision ankle arthroplasty. Oper. Orthop. Traumatol. 2017, 29, 220–235. [Google Scholar] [CrossRef]
- Georg, H.; Reinhard, H.; Markus, K.; Jan, L.; Lukas, L.; Roman, R.; Andreas, L.; Patrick, S. Revision Rates After Total Ankle Replacement: A Comparison of Clinical Studies and Arthroplasty Registers. Foot Ankle Int. 2022, 43, 176–185. [Google Scholar]
- Zaidi, R.; Macgregor, A.J.; Goldberg, A. Quality measures for total ankle replacement, 30-day readmission and reoperation rates within 1 year of surgery: A data linkage study using the NJR data set. BMJ Open 2016, 6, e011332. [Google Scholar] [CrossRef]
- Jung, W.L.; Woo-Young, I.; Si, Y.; Jae-Young, C.; Sung, J.K. Analysis of early failure rate and its risk factor with 2157 total ankle replacements. Sci. Rep. 2022, 11, 1901. [Google Scholar]
- Christian, S.; Matthias, L.; Stella, S.; Manuel, G.; Lorenz, P.; Tobias, G.; Antonio, K.; Matthias, C.K. Revision rate of total ankle replacement in patients younger than 50 years. Foot Ankle Surg. 2017, 23, 28. [Google Scholar] [CrossRef]
- Paul, M.R.; Michael, W.D.; David, F.; John, K. Dynamic Ultrasonography: A Cadaveric Model for Evaluating Aseptic Loosening of Total Ankle Arthroplasty. Foot Ankle Surg. 2013, 52, 311–314. [Google Scholar] [CrossRef]
- Rohit, D.; Jake, T.; Vikas, S.; Ramesh, K.N. Tri-Component, Mobile Bearing, Total Ankle Replacement: Mid-term Functional Outcome and Survival. Foot Ankle Surg. 2012, 51, 566–569. [Google Scholar] [CrossRef]
- Roukis, T.; Prissel, M. Management of Extensive Talar Osteolysis with Agility™ Total Ankle Replacement Systems Using Geometric Metal-reinforced Polymethylmethacrylate Cement Augmentation. Foot Ankle Surg. 2014, 53, 108–113. [Google Scholar] [CrossRef]
- Dharia, M.A.; Snyder, S.; Bischoff, J.E. Computational Model Validation of Contact Mechanics in Total Ankle Arthroplasty. Orthop Res. 2020, 38, 1063–1069. [Google Scholar] [CrossRef]
- Mondal, S.; Ghosh, R. Experimental and finite element investigation of total ankle replacement: A review of literature and recommendations. Orthopaedics 2020, 18, 41–49. [Google Scholar] [CrossRef]
- Alexandre, T.; Xabier, L.; Jonas, G.; Xavier, C. Development and experimental validation of a finite element model of total ankle replacement. Biomechanics 2014, 47, 742–745. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Z.; Wong, D.W.; Cheng, C.K.; Zhang, M. Finite element analysis of biomechanical effects of total ankle arthroplasty on the foot. Orthop Translat. 2017, 12, 55–65. [Google Scholar] [CrossRef]
- Federico, G.U.; Luigi, M.; Francesco, G.; Camilla, M.; Christian, I.; Alexander, M.C.; Christopher, E.G. Previous Surgery and the Temporal Evolution of Functional Outcomes and Complication Rates in Total Ankle Replacement. Foot Ankle Surg. 2022, 61, 572–576. [Google Scholar] [CrossRef]
- Wood, P.; Clough, T.; Smith, R. The present state of ankle arthroplasty. Foot Ankle Surg. 2008, 14, 115–119. [Google Scholar] [CrossRef]
- Yu, J.; Zhang, C.; Chen, W.M.; Zhao, D.; Chu, P.; Wang, S.; Huang, J.; Wang, X.; Ma, X. Finite-element analysis of the influence of tibial implant fixation design of total ankle replacement on bone-implant interfacial biomechanical performance. Orthop. Surg. 2020, 28, 2309499020966125. [Google Scholar] [CrossRef] [PubMed]
- Reggiani, B.; Leardini, A.; Corazza, F.; Taylor, M. Finite element analysis of a total ankle replacement during the stance phase of gait. Biomechanics 2006, 39, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Paul-André, D.; Alexandre NThibaut, L.; Raphaël, D.; Bernhard, D.B.; Jean-Luc, B.; Xavier, C.; Laurence, C. Impact of foot modeling on the quantification of the effect of total ankle replacement: A pilot study. Gait Posture 2021, 84, 308–314. [Google Scholar] [CrossRef]
- Collet, A. Top Ankle Replacement Implants in the United States. IData Res. 2021. Available online: https://idataresearch.com/top-ankle-replacement-implants/ (accessed on 29 November 2022).
- Choi, J.H.; Coleman, S.C.; Tenenbaum, S.; Polo, F.E.; Brodsky, J.W. Prospective study of the effect on gait of a two-component total ankle replacement. Foot Ankle Int. 2013, 34, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Cottom, J.; Plemmons, B.; Douthett, S. Relationship Between Body Mass Index and Complications in Total Ankle Arthroplasty: A Single Surgeon’s Experience in Ninety-Seven Replacements. Foot Ankle Surg. 2019, 58, 687–691. [Google Scholar] [CrossRef]
- Seth, A. A review of the STAR prosthetic system and the biomechanical considerations in total ankle replacements. Foot Ankle Surg. 2011, 17, 64–67. [Google Scholar] [CrossRef]
- Daniels, T.R.; Mayich, D.J.; Penner, M.J. Intermediate to long-term outcomes of total ankle replacement with the Scandinavian Total Ankle Replacement (STAR). Bone Jt. Surg Am. 2015, 97, 895–903. [Google Scholar] [CrossRef]
- Koivu, H.; Kohonen, I.; Mattila, K.; Loyttyniemi, E.; Tiusanen, H. Long-term results of Scandinavian total ankle replacement. Foot Ankle Int. 2017, 38, 723–731. [Google Scholar] [CrossRef]
- Scott, R.T.; Witt, B.L.; Hyer, C.F. Design comparison of the INBONE I versus INBONE II total ankle system. Foot Ankle Spec. 2013, 6, 137–140. [Google Scholar] [CrossRef]
- Hsu, A.R.; Davis, W.H.; Cohen, B.E.; Jones, C.P.; Ellington, J.K.; Anderson, R.B. Radiographic outcomes of preoperative CT scan-derived patient-specific total ankle arthroplasty. Foot Ankle Int. 2015, 36, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Daigre, J.; Berlet, G.; Van Dyke, B.; Peterson, K.S.; Santrock, R. Accuracy and reproducibility using patient-specific instrumentation in total ankle arthroplasty. Foot Ankle Int. 2017, 38, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Hamid, K.S.; Matson, A.P.; Nwachukwu, B.U.; Scott, D.J.; Mather, R.C.; DeOrio, J.K. Determining the cost-savings threshold and alignment accuracy of patient-specific instrumentation in total ankle replacements. Foot Ankle Int. 2017, 38, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Basile, P.; Miner, S.; Crafton, J.; McKenna, B. Preliminary Report of a Hybrid Total Ankle Arthroplasty Combining a Stemmed Intramedullary Tibial Component With Chamfer-Cut Talar Dome. Foot Ankle Surg. 2021, 61, E25–E33. [Google Scholar] [CrossRef]
- Assaf, A.; Susan, M.G.; Patrick, P.; Dan, C.; Laura, E.; Ruth, E.C.; Monika, V. Total ankle arthroplasty results using fixed bearing CT-guided patient specific implants in posttraumatic versus nontraumatic arthritis. Foot Ankle Surg. 2022, 28, 222–228. [Google Scholar] [CrossRef]
- Barg, A.; Wiewiorski, M.; Valderrabano, V. Aseptic loosening of total ankle replacement: Two-stage revision with bone augmentation of osseous defects and secondary prosthesis implantation. Oper. Orthop. Traumatol. 2017, 29, 236–252. [Google Scholar] [CrossRef]
- Karl, M.S.; Samuel, B.A.; Mark, E.E.; James, K.D.; James, A.N. Total ankle arthroplasty with a modern fixed-bearing system: The Salto Talaris prosthesis. JBJS Essent. Surg. Tech. 2013, 3, e18. [Google Scholar] [CrossRef]
- Jonathan, D.; Jaeyoung, K.; Martin, J.O.; Constantine, A.D.; Jonathan, G.; Austin, S.; Andrew, R.; Jonathan, T.D.; David, S.L.; Scott, J.E. Radiographic and clinical outcomes of the Salto Talaris total ankle arthroplasty. Foot Ankle Int. 2020, 41, 1519–1528. [Google Scholar]
- Bischoff, J.E.; Schon, L.; Saltzman, C. Influence of geometry and depth of resections on bone support for total ankle replacement. Foot Ankle Int. 2017, 38, 1026–1034. [Google Scholar] [CrossRef]
- King, M.; Vesely, B.; Scott, A. Early outcomes with the vantage total ankle prosthesis. Foot Ankle Surg. Tech. Rep. Cases 2022, 2, 100121. [Google Scholar] [CrossRef]
- Brianna, F.; Daniel, O.C.; Ryan, G.R.; David, I.P.; Justin, T. Short-Term Complications and Outcomes of the Cadence Total Ankle Arthroplasty. Foot Ankle Int. 2022, 43, 371–377. [Google Scholar] [CrossRef]
- DeOrio, J.K.; Nunley, J.A.; Easley, M.; Valerrabano, V. Vantage Total Ankle Replacement. In Primary and Revision Total Ankle Replacement; Springer: Cham, Switzerland, 2021; pp. 151–163. [Google Scholar]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).