
Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review

 ,
, 
 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria for the Studies Included in This Review
2.3. Data Collection Process
2.4. Types of Outcomes
2.5. Quality Assessment
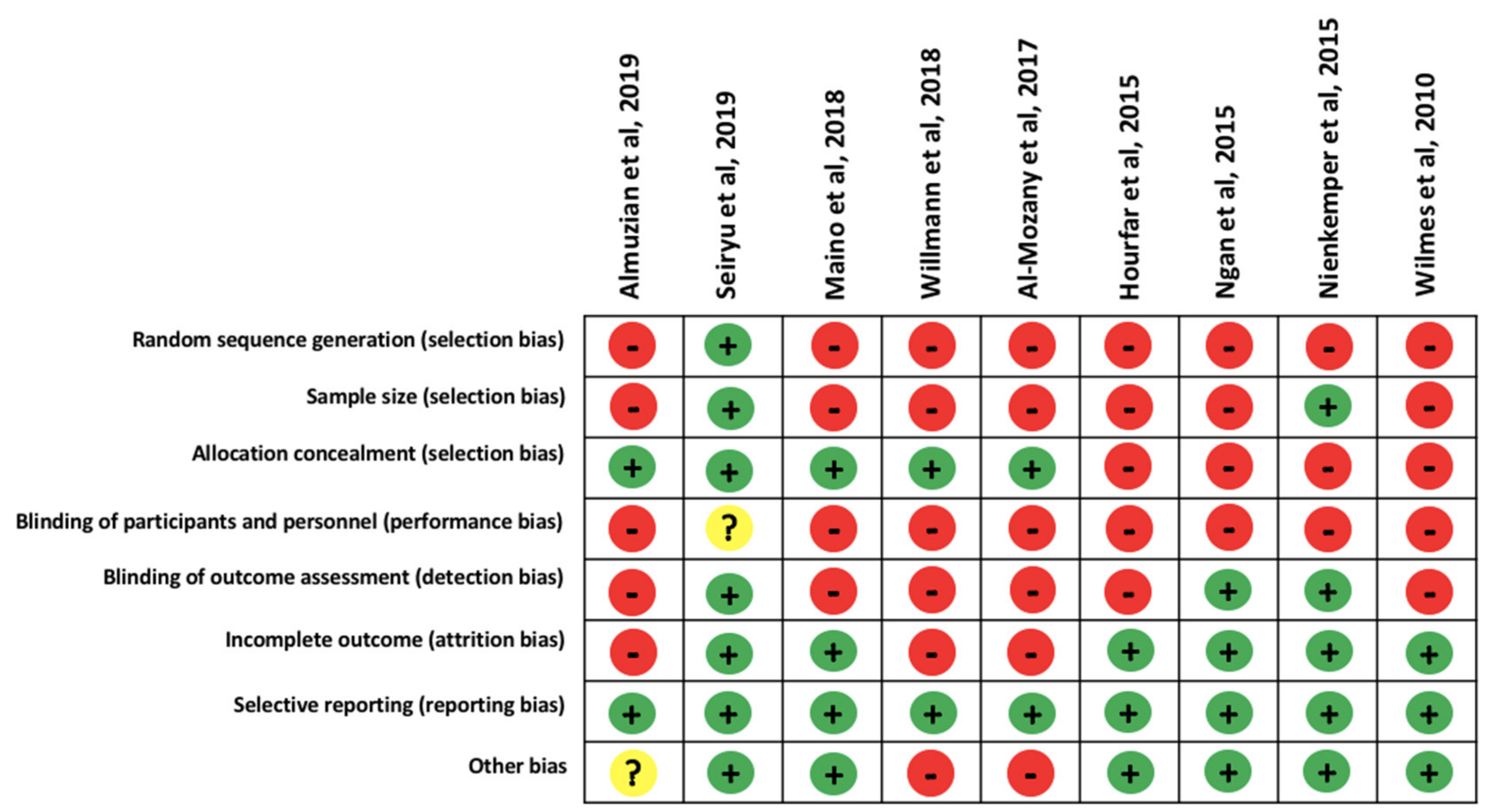
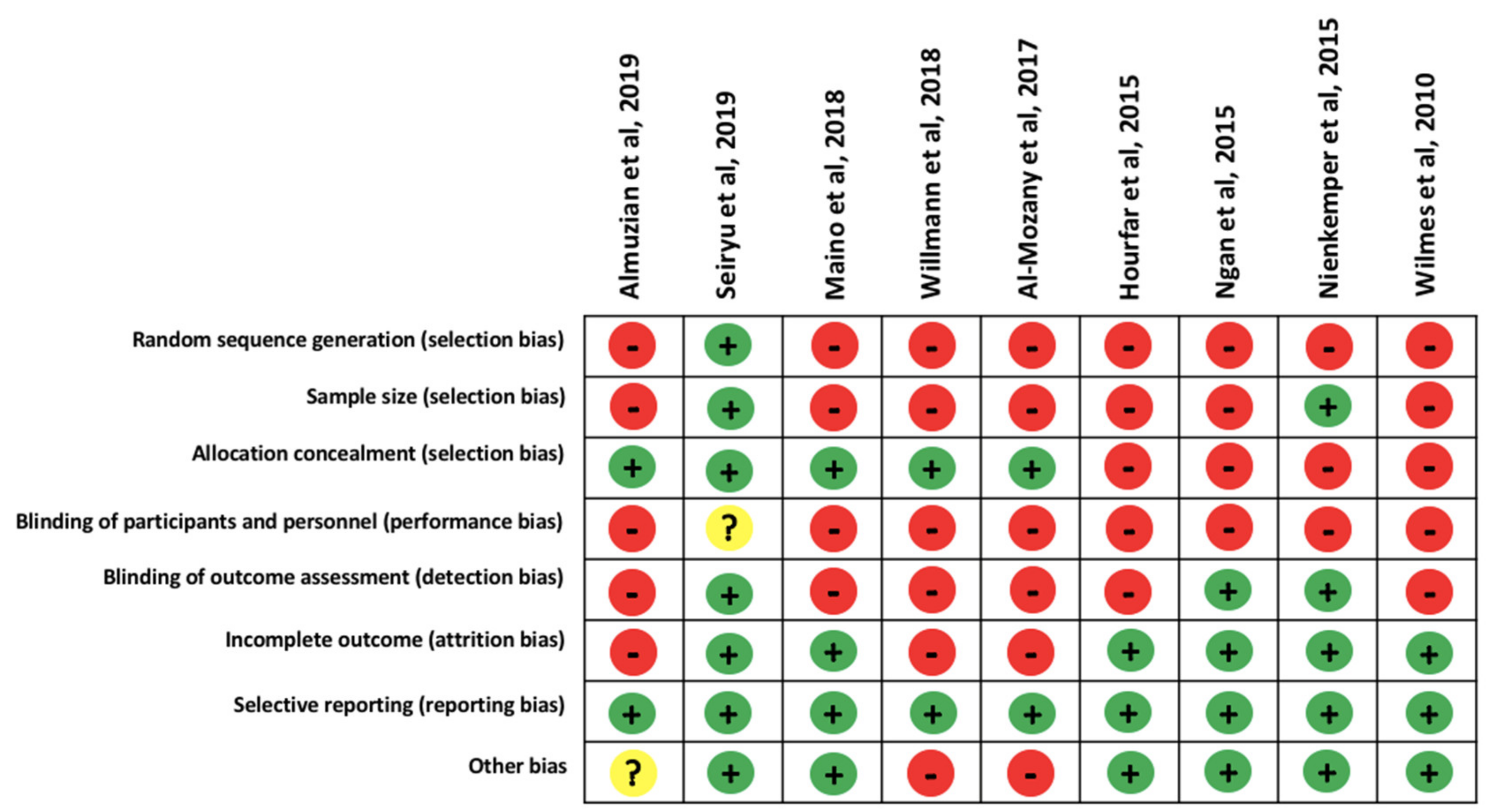
2.6. Risk of Bias Assessment
3. Results
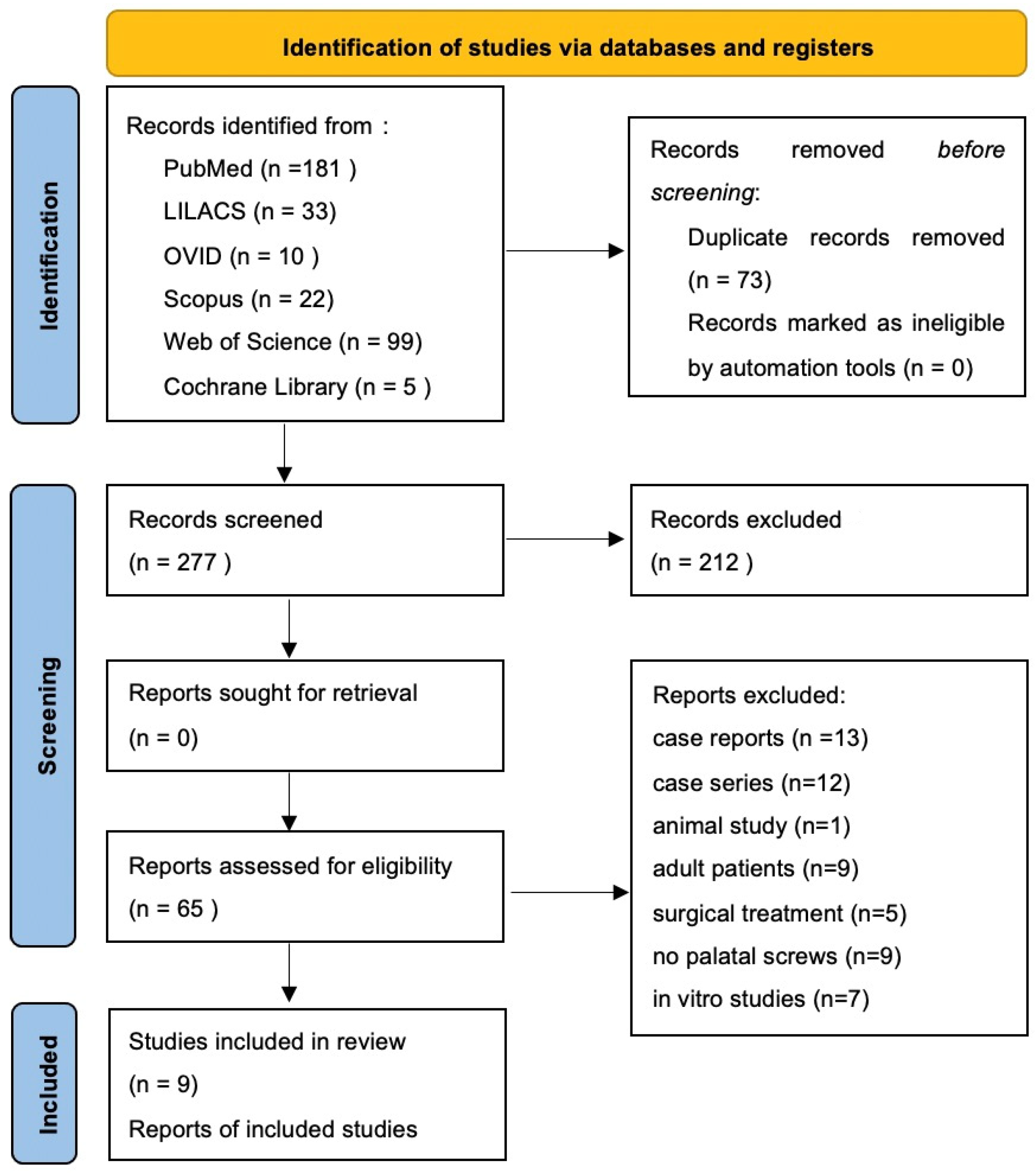
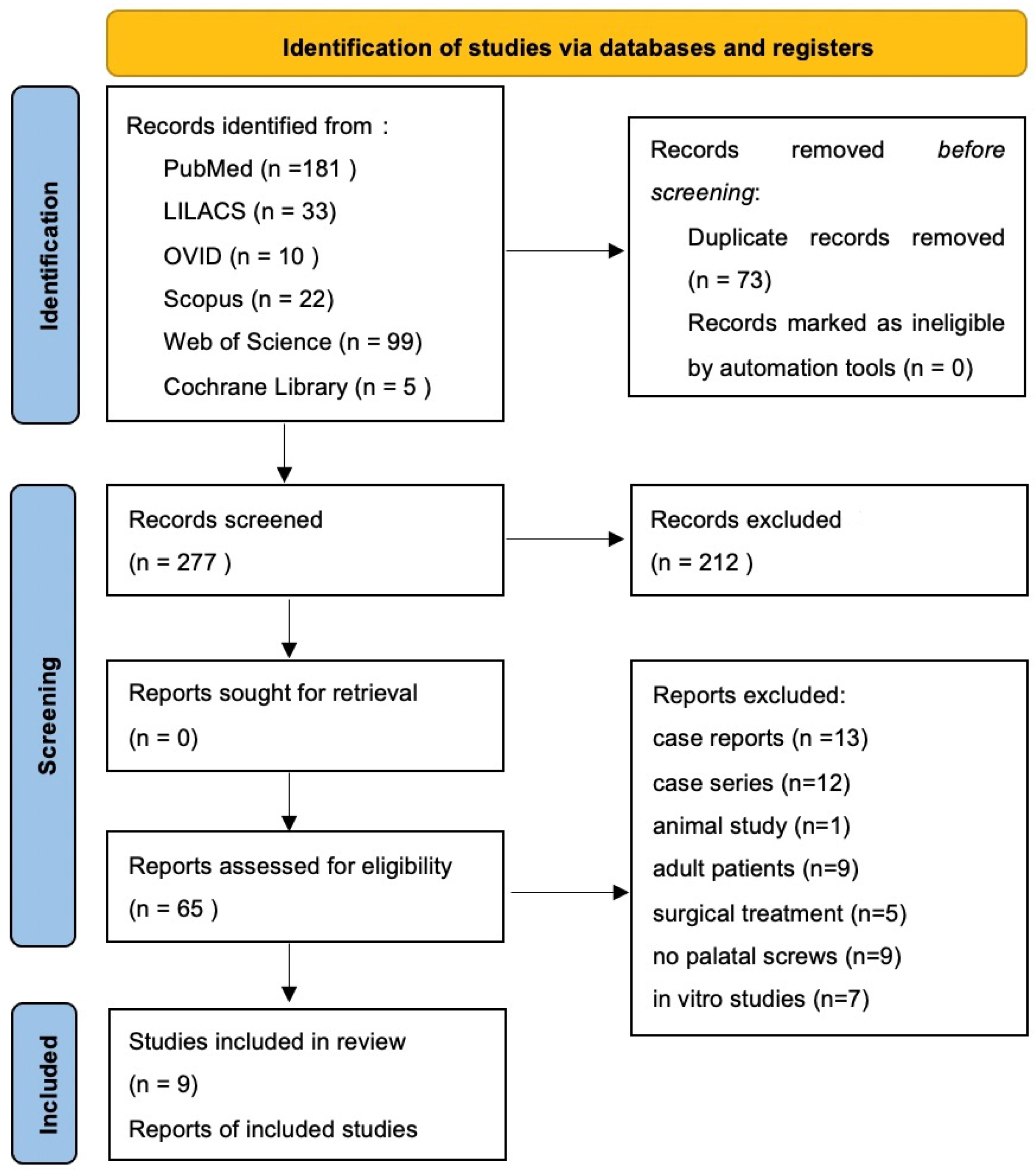
3.1. Study Selection and Flow Diagram
3.2. Study Characteristics
3.3. Qualitative Synthesis of the Studies Included
3.4. Skeletal Anchorage
3.5. Expansion Activation Protocol
3.6. Class III Biomechanics
3.7. Dentoalveolar Effects
3.8. Skeletal Effects
3.9. Soft Tissue Analysis
3.10. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ngan, P.; Moon, W. Evolution of Class III Treatment in Orthodontics. Am. J. Orthod. Dentofacial Orthop. 2015, 148, 22–36. [Google Scholar] [CrossRef] [Green Version]
- Duggal, R.; Mathur, V.; Parkash, H.; Jena, A. Class—III Malocclusion: Genetics or Environment? A Twins Study. J. Indian Soc. Pedod. Prev. Dent. 2005, 23, 27. [Google Scholar] [CrossRef] [PubMed]
- Adina, S.; Dipalma, G.; Bordea, I.R.; Lucaciu, O.; Feurdean, C.; Inchingolo, A.D.; Septimiu, R.; Malcangi, G.; Cantore, S.; Martin, D.; et al. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef]
- Al-Mozany, S.A.; Dalci, O.; Almuzian, M.; Gonzalez, C.; Tarraf, N.E.; Ali Darendeliler, M. A Novel Method for Treatment of Class III Malocclusion in Growing Patients. Prog. Orthod. 2017, 18, 40. [Google Scholar] [CrossRef] [Green Version]
- Di Venere, D.; Nardi, G.M.; Lacarbonara, V.; Laforgia, A.; Stefanachi, G.; Corsalini, M.; Grassi, F.R.; Rapone, B.; Pettini, F. Early mandibular canine-lateral incisor transposition: Case Report. Oral Implantol. 2017, 10, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Di Venere, D.; Corsalini, M.; Nardi, G.M.; Laforgia, A.; Grassi, F.R.; Rapone, B.; Pettini, F. Obstructive site localization in patients with Obstructive Sleep Apnea Syndrome: A comparison between otolaryngologic data and cephalometric values. Oral Implantol. 2017, 10, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Di Venere, D.; Pettini, F.; Nardi, G.M.; Laforgia, A.; Stefanachi, G.; Notaro, V.; Rapone, B.; Grassi, F.R.; Corsalini, M. Correlation between parodontal indexes and orthodontic retainers: Prospective study in a group of 16 patients. Oral Implantol. 2017, 10, 78–86. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an oral appliance in patients with mild to moderate obstructive sleep apnea syndrome intolerant to continuous positive airway pressure use: Preliminary results. Int. J. Immunopathol. Pharmacol. 2016, 29, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Dimonte, M.; Inchingolo, F.; Minonne, A.; Arditi, G.; Dipalma, G. Bone SPECT in management of mandibular condyle hyperplasia. Report of a case and review of literature. Minerva Stomatol. 2004, 53, 281–285. [Google Scholar]
- Sirbu, A.A.; Bordea, R.; Lucaciu, O.; Braitoru, C.; Szuhanek, C.; Campian, R. 3D Printed Splints an Innovative Method to Treat Temporomandibular Joint Pathology. Rev. Chim. 2018, 69, 3087–3089. [Google Scholar] [CrossRef]
- Laudadio, C.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Montenegro, V.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef] [PubMed]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public. Health 2021, 18, 6056. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during Covid-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [CrossRef]
- Almuzian, M.; Almukhtar, A.; Ulhaq, A.; Alharbi, F.; Darendeliler, M.A. 3D Effects of a Bone-Anchored Intra-Oral Protraction in Treating Class III Growing Patient: A Pilot Study. Prog. Orthod. 2019, 20, 37. [Google Scholar] [CrossRef]
- Grassia, V.; d’Apuzzo, F.; DiStasio, D.; Jamilian, A.; Lucchese, A.; Perillo, L. Upper and Lower Arch Changes after Mixed Palatal Expansion Protocol. Eur. J. Paediatr. Dent. 2014, 15, 375–380. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 71, 372. [Google Scholar] [CrossRef]
- Alzabibi, B.A.; Burhan, A.S.; Hajeer, M.Y.; Nawaya, F.R. Short-term effects of the orthodontic removable traction appliance in the treatment of skeletal Class III malocclusion: A randomized controlled trial. Dent. Med. Probl. 2021, 58, 163–172. [Google Scholar] [CrossRef]
- Fatima, F.; Jeelani, W.; Ahmed, M. Current trends in craniofacial distraction: A literature review. Dent. Med. Probl. 2020, 57, 441–448. [Google Scholar] [CrossRef]
- Fabozzi, F.F.; Nucci, L.; Correra, A.; d’Apuzzo, F.; Franchi, L.; Perillo, L. Comparison of Two Protocols for Early Treatment of Dentoskeletal Class III Malocclusion: Modified SEC III versus RME/FM. Orthod. Craniofac. Res. 2021, 24, 344–350. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; d’Apuzzo, F.; Majorana, A.; Campus, G.; Nucci, F.; Flores-Mir, C.; Perillo, L. Influence of occlusal characteristics, food intake and oral hygiene habits on dental caries in adolescents: A cross-sectional study. Eur. J. Paediatr. Dent. 2018, 19, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Franchi, L.; Baccetti, T.; McNamara, J.A. Postpubertal Assessment of Treatment Timing for Maxillary Expansion and Protraction Therapy Followed by Fixed Appliances. Am. J. Orthod. Dentofacial Orthop. 2004, 126, 555–568. [Google Scholar] [CrossRef] [PubMed]
- Patianna, A.G.; Ballini, A.; Meneghello, M.; Cantore, S.; Inchingolo, A.M.; Dipalma, G.; Inchingolo, A.D.; Inchingolo, F.; Malcangi, G.; Lucchese, A.; et al. Comparison of conventional orthognathic surgery and “surgery-first” protocol: A new weapon against time. J. Biol. Regul. Homeost. Agents 2019, 33, 59–67. [Google Scholar] [PubMed]
- Quaglia, E.; Moscufo, L.; Corsalini, M.; Coscia, D.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Rapone, B.; Carossa, M.; Carossa, S. Polyamide vs silk sutures in the healing of postextraction sockets: A split mouth study. Oral Implantol. 2018, 11, 115–120. [Google Scholar]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Converti, I.; Grassi, F.R.; Santacroce, L.; Topi, S.; Gnoni, A.; Scacco, S.; Scarano, A.; et al. The Effect of Gaseous Ozone Therapy in Conjunction with Periodontal Treatment on Glycated Hemoglobin Level in Subjects with Type 2 Diabetes Mellitus: An Unmasked Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 54675. [Google Scholar] [CrossRef]
- Farronato, M.; Farronato, D.; Inchingolo, F.; Grassi, L.; Lanteri, V.; Maspero, C. Evaluation of Dental Surface after De-Bonding Orthodontic Bracket Bonded with a Novel Fluorescent Composite: In Vitro Comparative Study. Appl. Sci. 2021, 11, 6354. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Marrelli, M.; Inchingolo, A.M.; Tarullo, A.; Inchingolo, A.D.; Dipalma, G.; Brunetti, S.P.; Tarullo, A.; Cagiano, R. Combined Occlusal and Pharmacological Therapy in the Treatment of Temporo-Mandibular Disorders. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 1296–1300. [Google Scholar]
- Wilmes, B.; Nienkemper, M.; Drescher, D. Application and Effectiveness of a Mini-Implant- and Tooth-Borne Rapid Palatal Expansion Device: The Hybrid Hyrax. World J. Orthod. 2010, 11, 323–330. [Google Scholar]
- Grassi, F.R.; Grassi, R.; Rapone, B.; Gianfranco, A.; Balena, A.; Kalemaj, Z. Dimensional changes of buccal bone plate in immediate implants inserted through open flap, open flap and bone grafting, and flapless technique. A CBCT randomized controlled clinical trial. Clin Oral Implants Res. 2019, 30, 1155–1164. [Google Scholar] [CrossRef]
- Rapone, B.; Corsalini, M.; Converti, I.; Loverro, M.T.; Gnoni, A.; Trerotoli, P.; Ferrara, E. Does Periodontal Inflammation Affect Type 1 Diabetes in Childhood and Adolescence? A Meta-Analysis. Front. Endocrinol. 2020, 11, 278. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Scacco, S.; Perillo, L.; Scarano, A.; Aityan, S.K.; Contaldo, M.; Nguyen, K.C.; Santacroce, L.; Syed, J.; et al. A comparative study on different stemness gene expression between dental pulp stem cells vs. dental bud stem cells. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1626–1633. [Google Scholar] [PubMed]
- Grassi, F.R.; Rapone, B.; Scarano Catanzaro, F.; Corsalini, M.; Kalemaj, Z. Effectiveness of computer-assisted anesthetic delivery system (STA™) in dental implant surgery: A prospective study. Oral Implantol. 2017, 10, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Corsalini, M.; Di Venere, D.; Carossa, M.; Ripa, M.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Di Santantonio, G.; Lenoci, G.; Barile, G.; et al. Comparative clinical study between zirconium-ceramic and metal-ceramic fixed rehabilitations. Oral Implantol. 2018, 11, 150–160. [Google Scholar]
- Ballini, A.; Cantore, S.; Fotopoulou, E.A.; Georgakopoulos, I.P.; Athanasiou, E.; Bellos, D.; Paduanelli, G.; Saini, R.; Dipalma, G.; Inchingolo, F. Combined sea salt-based oral rinse with xylitol in orthodontic patients: Clinical and microbiological study. J. Biol. Regul. Homeost. Agents 2019, 33, 263–268. [Google Scholar]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Cesarano, F.; Arazzi, M.; Di Liberato, L.; Scacco, S.; Grassi, R.; Grassi, F.R.; Gnoni, A.; et al. Periodontal Microbiological Status Influences the Occurrence of Cyclosporine-A and Tacrolimus- Induced Gingival Overgrowth. Antibiotics 2019, 8, 124. [Google Scholar] [CrossRef] [Green Version]
- Corsalini, M.; Di Venere, D.; Sportelli, P.; Magazzino, D.; Ripa, M.; Cantatore, F.; Cagnetta, C.; De Rinaldis, C.; Montemurro, N.; De Giacomo, A.; et al. Evaluation of prosthetic quality and masticatory efficiency in patients with total removable prosthesis: Study of 12 cases. Oral Implantol. 2018, 11, 230–240. [Google Scholar]
- Cantore, S.; Ballini, A.; De Vito, D.; Martelli, F.S.; Georgakopoulos, I.; Almasri, M.; Dibello, V.; Altini, V.; Farronato, G.; Dipalma, G.; et al. Characterization of human apical papilla-derived stem cells. J. Biol. Regul. Homeost. Agents 2017, 31, 901–910. [Google Scholar]
- Marinelli, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Limongelli, L.; Montenegro, V.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; et al. White spot lesions in orthodontics: Prevention and treatment. A descriptive review. J. Biol. Regul. Homeost. Agents 2021, 35, 227–240. [Google Scholar]
- Cirulli, N.; Ballini, A.; Cantore, S.; Farronato, D.; Inchingolo, F.; Dipalma, G.; Gatto, M.R.; Alessandri Bonetti, G. Mixed dentition space analysis of a southern italian population: New regression equations for unerupted teeth. J. Biol. Regul. Homeost. Agents 2015, 29, 515–520. [Google Scholar]
- Cevidanes, L.; Baccetti, T.; Franchi, L.; McNamara, J.A.; De Clerck, H. Comparison of Two Protocols for Maxillary Protraction: Bone Anchors versus Face Mask with Rapid Maxillary Expansion. Angle Orthod. 2010, 80, 799–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heymann, G.C.; Cevidanes, L.; Cornelis, M.; De Clerck, H.J.; Tulloch, J.F.C. Three-Dimensional Analysis of Maxillary Protraction with Intermaxillary Elastics to Miniplates. Am. J. Orthod. Dentofacial Orthop. 2010, 137, 274–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Inchingolo, F.; Rapone, B.; Festa, F.; Tari, S.R.; Lorusso, F. Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery. Int. J. Environ. Res. Public Health 2021, 18, 2363. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, F.; Noumbissi, S.; Inchingolo, F.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific Trends in Clinical Research on Zirconia Dental Implants: A Bibliometric Review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef] [PubMed]
- Bordea, I.; Sîrbu, A.; Lucaciu, O.; Ilea, A.; Câmpian, R.; Todea, D.; Alexescu, T.; Aluaș, M.; Budin, C.; Pop, A. Microleakage—The Main Culprit in Bracket Bond Failure? J. Mind Med. Sci. 2019, 6, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Moon, W.; Wu, K.W.; MacGinnis, M.; Sung, J.; Chu, H.; Youssef, G.; Machado, A. The Efficacy of Maxillary Protraction Protocols with the Micro-Implant-Assisted Rapid Palatal Expander (MARPE) and the Novel N2 Mini-Implant—a Finite Element Study. Prog. Orthod. 2015, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 26 January 2022).
- Montinaro, F.; Nucci, L.; Carfora, M.; d’Apuzzo, F.; Franchi, L.; Perillo, L. Modified SEC III Protocol: Vertical Control Related to Patients’ Compliance with the Chincup. Eur. J. Orthod. 2021, 43, 80–85. [Google Scholar] [CrossRef]
- Maino, G.; Turci, Y.; Arreghini, A.; Paoletto, E.; Siciliani, G.; Lombardo, L. Skeletal and Dentoalveolar Effects of Hybrid Rapid Palatal Expansion and Facemask Treatment in Growing Skeletal Class III Patients. Am. J. Orthod. Dentofacial Orthop. 2018, 153, 262–268. [Google Scholar] [CrossRef]
- Hourfar, J.; Kinzinger, G.S.M.; Ludwig, B.; Spindler, J.; Lisson, J.A. Differential Treatment Effects of Two Anchorage Systems for Rapid Maxillary Expansion: A Retrospective Cephalometric Study. J. Orofac. Orthop. Fortschr. Kieferorthopädie 2016, 77, 314–324. [Google Scholar] [CrossRef]
- Nienkemper, M.; Wilmes, B.; Franchi, L.; Drescher, D. Effectiveness of Maxillary Protraction Using a Hybrid Hyrax-Facemask Combination: A Controlled Clinical Study. Angle Orthod. 2015, 85, 764–770. [Google Scholar] [CrossRef] [Green Version]
- Marra, P.M.; Nucci, L.; Abdolreza, J.; Perillo, L.; Itro, A.; Grassia, V. Odontoma in a young and anxious patient associated with unerupted permanent mandibular cuspid: A case report. J. Int. Oral Health 2020, 12, 182–186. [Google Scholar] [CrossRef]
- Willmann, J.H.; Nienkemper, M.; Tarraf, N.E.; Wilmes, B.; Drescher, D. Early Class III Treatment with Hybrid-Hyrax -Facemask in Comparison to Hybrid-Hyrax-Mentoplate—Skeletal and Dental Outcomes. Prog. Orthod. 2018, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Ngan, P.; Wilmes, B.; Drescher, D.; Martin, C.; Weaver, B.; Gunel, E. Comparison of Two Maxillary Protraction Protocols: Tooth-Borne versus Bone-Anchored Protraction Facemask Treatment. Prog. Orthod. 2015, 16, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seiryu, M.; Ida, H.; Mayama, A.; Sasaki, S.; Sasaki, S.; Deguchi, T.; Takano-Yamamoto, T. A Comparative Assessment of Orthodontic Treatment Outcomes of Mild Skeletal Class III Malocclusion Between Facemask and Facemask in Combination with a Miniscrew For Anchorage in Growing Patients: A Single-Center, Prospective Randomized Controlled Trial. Angle Orthod. 2020, 90, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Dekel, E.; Nucci, L.; Weill, T.; Flores-Mir, C.; Becker, A.; Perillo, L.; Chaushu, S. Impaction of Maxillary Canines and Its Effect on the Position of Adjacent Teeth and Canine Development: A Cone-Beam Computed Tomography Study. Am. J. Orthod. Dentofacial Orthop. 2021, 159, e135–e147. [Google Scholar] [CrossRef]
- Eslami, S.; Faber, J.; Fateh, A.; Sheikholaemmeh, F.; Grassia, V.; Jamilian, A. Treatment Decision in Adult Patients with Class III Malocclusion: Surgery versus Orthodontics. Prog. Orthod. 2018, 19, 28. [Google Scholar] [CrossRef] [Green Version]
- Clemente, R.; Contardo, L.; Greco, C.; Di Lenarda, R.; Perinetti, G. Class III Treatment with Skeletal and Dental Anchorage: A Review of Comparative Effects. BioMed Res. Int. 2018, 2018. [Google Scholar] [CrossRef]
- Luchian, I.; Moscalu, M.; Goriuc, A.; Nucci, L.; Tatarciuc, M.; Martu, I.; Covasa, M. Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment. J. Clin. Med. 2021, 10, 379. [Google Scholar] [CrossRef]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Di Pede, C.; Garibaldi, M.; Ciocia, A.M.; et al. Treatment of Class III Malocclusion and Anterior Crossbite with Aligners: A Case Report. Medicina 2022, 58, 603. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Author/Year [Reference] | Selection | Comparability | Exposure | |||||
|---|---|---|---|---|---|---|---|---|
| Case Definition Adequate | Representativeness of Cases | Selection of Controls | Definition of Controls | Comparability of Cases & Controls | Ascertainment of Exposure | Same Method of Ascertainment | Non-Response Rate | |
| Al-Mozany et al. Almuzian et al. | * | * | * | |||||
| Wilmes et al. | * | * | ||||||
| Maino et al. | * | * | * | |||||
| Nienkemper et al. | * | * | * | * | * | * | * | |
| Hourfar et al. | * | * | * | * | * | |||
| Seiryu et al. | * | * | * | * | * | * | ||
| Ngan et al. | * | * | * | * | * | * | ||
| Willmann et al. | * | * | * | * | * | * | ||
| Authors | Aim | C (Cases) Co (Controls)Mean Age (MA) | Randomized | Control (Yes or Not) | Number and Position of Screw (Appliance Design) | Inclusion Criteria | Methods | Results |
|---|---|---|---|---|---|---|---|---|
| Al-Mozany et al./ Almuzian et al. | To evaluate the skeletal and soft tissue effects of the alternate RME and constriction (Alt-Ramec) protocol in conjunction with a miniscrew forgrowing participants with retrognathic maxilla, evaluated by cephalometric analysis (2017) and 3D cone-beam (2019). | Ca (14) MA (12.5 ± 1.9 years) | No | No | MARME with two paramedial palatal TADs and two mandibular TADs, inserted between the canine and the lateral incisor | -Patients at CVM Stage 2 or 3 -Patients with clinically diagnosed retrognathic or hypoplastic maxilla -Anterior crossbite and dental Class III molars and canines | All participants had a MARME appliance that was activated by the Alt-Ramec protocol. Full time Class III elastics, delivering 400 g/side, were then used for maxillary protraction. | -Maxilla protraction (SNA 1.87 ± 1.06°; Vert.T-A 3.29 ± 1.54 mm p < 0.001) -Mandibular retropositioning (SNB-2.03 ± 0.85°; Vert.T-B-3.43 ± 4.47 mm, p < 0.001 and p < 0.05 respectively) -A significant improvement in the skeletal relationship (ANB 3.95 ± 0.57°, p < 0.001; Wits 5.15 ±1.51 mm, p < 0.001) -Increase of Y-axis angle (1.95 ± 1.11°, p < 0.001) -The upper incisors proclination (+ 2.98 ± 2.71°, p < 0.01), coupled with a significant retroclination of the lower incisors (−3.2 ± 3.4°, p < 0.05) -A significant improvement in the OVJ (5.62 ± 1.36 mm, p < 0.001) and in the Harmony angle (2.76 ± 1.8°, p < 0.001) |
| Wilmes et al. | To assess the clinical applicability and 3D effects of RPE using the hybrid hyrax. | Ca (13) MA (11.2 years) | No | No | Two miniscrews were inserted in the anterior palate next to the midpalatal suture and near the second and third palatal rugae. The miniscrews and two molar bands were used to connect the Hybrid Hyrax device. | -Patients with Class III malocclusion | RPE was performed in 13 patients. In 10 patients with a skeletal Class III occlusion, a facemask was used for maxillary protraction. | -The mean expansion in the first premolar/first primary molar region was 6.3 ± 2.9 mm and 5.0 ± 1.5 mm in the first molar region. -The Wits appraisal changed from −5.2 ± 1.3 mm to −2.5 ± 1.5 mm (mean improvement 2.7 ± 1.3 mm). -The right first molar migrated 0.4 ± 0.6 mm mesially and the left one 0.3 ± 0.2 mm. |
| Maino et al. | To describe the skeletal and dentoalveolar changes in a group of growing skeletal Class III patients treated with hybrid palatal expander and facemask. | Ca (28) MA (11.4 ± 2.5 years) | No | No | Hybrid palatal expander was connected to two paramedial palatal miniscrews | -Growing patient with Class III malocclusion. | 28 patients were treated using a rapid maxillary expander with hybrid anchorage according to the ALT-Ramec protocol, followed by 4 months of facemask therapy. Palatal miniscrew placement was accomplished via digital planning and the construction of a high-precision, individualized surgical guide. | -Point A advanced by a mean of 3.4 mm with respect to the reference plane Vert-T. -The mandibular plane rotated clockwise, improving the ANB (+3.41°) and the Wits appraisal (+4.92 mm). -The maxillary first molar had slight extrusion (0.42 mm) and mesialization (0.87 mm). |
| Nienkemper et al. | To value the efficacy of hybrid hyrax and facemask (FM) combination in growing Class III patients. | Ca (16) MA (9.5 ± 1.6 years) Co (16) MA (9.4 ± 1.1 years) | No | Yes | On both sides of the midpalatal suture, two micro implants were placed in the anterior palate. The miniscrews and two molar bands were used to connect the Hybrid hyrax device. To apply the protraction, two rigid sectional wires were welded to the buccal side of the molar bands. | -Class III malocclusion in the mixed dentition characterized by a Wits index of −2 mm or less (mean, −5.6 ± 2.2 mm) -Anterior crossbite or incisor edge-to-edge relationship -Class III molar relationship -CVM (CS1-3) | 16 growing Class III patients were treated with a RPE with a hybrid hyrax. A facemask was used to perform a maxillary protraction. A control group of 16 untreated Class III participants was compared to the treatment group. | -SNA and Point A to nasion perpendicular showed significant increments of 2.4° and 2.4 mm, respectively. -A significant reduction in the length and sagittal position of the mandible (CoGn −2.3 mm and SNB −1.7°) -The Wits index augmented by 4.5 mm and the ANB improved by 4.1° -Co-Go-Me angle decrease significantly (2.0°). No significant increase of FMA (0.5°) -OVJ and molar relationship improved significantly (3.2 mm and −3.1 mm, respectively) -No significant differences could be found in OVB or inclination of the maxillary and mandibular incisors. |
| Hourfar et al. | To compare cephalometric changes after treatment with two types of fast maxillary expansion appliances: a tooth-borne appliance and a tooth-and-bone-borne appliance. | Ca (50); MA (13.04 ± 4.82 years) Co (50); MA (13.04 ± 4.82 years) | No | Yes | Two miniscrews were placed in the anterior palate at paramedian locations. These miniscrews held the anterior side of a hybrid hyrax, while the posterior side was attached to the orthodontic bands on the front molars. | -Patients treated with strictly tooth-borne or patients treated with combined tooth- and bone-borne appliances -Skeletal Class I (0° < ANB ≤ 4°) or Class III (ANB ≤ 0°) -Caucasian descendent -Bilateral posterior crossbite | Cephalometry was used to examine the pre- and post-treatment lateral cephalograms of 100 patients. 50 of the patients were treated with exclusively tooth-borne appliances, whereas the other 50 were treated with a combination of tooth-and-bone-borne appliances. Additional sub-groups were constructed based on pre-treatment cephalometric data for skeletal Class I or Class III to detect any implications for clinical therapy. | -Pronounced anterior shift of the maxilla (SNA increase by 2°) -Caudal shift of the maxilla -Upper jaw inclination remained almost the same. -Increases in the vertical parameters ML/NSL (1.46°) and Björk sum (1.46). |
| Seiryu et al. | To investigate difference in treatment outcomes of milder skeletal class III malocclusion between FM and FM + MS in growing patients | Ca (20) MA (10.05 ± 1.8 years) Co (19) MA (11 ± 1.3 years) | Yes | Yes | In the FM + MS group, one miniscrew was inserted in the anterior region of the palate. A lingual arch with soldered hooks was attached to the miniscrew. | -Skeletal class III (ANB ≤ 2.5°) -OVJ ≥ 0 -CVMS II–IV -No congenital or systemic disease -No skeletal asymmetry -No missing teeth -No temporomandibular joint disorder | A lingual arch with hooks was fixed to the maxillary arch in both groups and a protractive force of 500 g was applied form the FM to the hooks, 12 hours per day. | -No MS mobility or loss during treatment -Cephalometric analysis showed a significant increase In SNA (1.1°), SN-ANS (1.3°), and ANB (0.8°) in the FM + MS group -Proclination of maxillary incisors significantly greater in the FM group (4.6°) |
| Ngan et al. | The goal of this study was to examine the skeletal and dentoalveolar alterations in patients treated with tooth-borne Hyrax + FM versus hybrid Hyrax + FM. | Ca (20) MA (9.8 ± 1.6 years) Co (20) MA (9.6 ± 1.2 years) | No | Yes | In the hybrid Hyrax group two Benefit micro-implants were placed in the third palatal rugae. | -Class III malocclusion: -Anterior crossbite or edge-to-edge incisal relationship -Wits ≤ −3/ANB ≤ −2° | A total of 20 patients were treated with tooth-borne Hyrax + FM, while 20 patients were treated with bone-borne Hyrax +FM in a row. The screw was activated twice daily by the patients in both groups for one week, and two weeks when a constricted maxilla was evident. Maxillary protraction was performed with 380 g per side elastics for 12–14 hours per day. | -Sagittal relationship improved in both groups: tooth-borne (Wits 2.19, ANB 2.58°) and bone-borne (Wits 2.31 mm, ANB 2.17°). -Greater downward movement of the maxilla in tooth-borne (OLparallel–A pt. 1.2 mm) compared to bone-borne (−0.4 mm, p < 0.005) -Forward and backward movement of the mandible in both groups (OLp-A pt., 0.7 mm/2.2 mm) -Mandibular plane angle was found to open more in tooth-borne (SNL-ML 2.76°) compared to bone-borne (−0.25°, p < 0.05) -Greater change in OVJ in the tooth-borne group (5.5 mm) compared to the bone-anchored group (3.4 mm, p < 0.001) -Greater forward movement of maxillary incisors in the tooth-borne group (OLp-Is 2.12 vs. 0.87, p < 0.05) and greater differential maxillary/mandibular molars movement |
| Willmann et al. | To compare skeletal and dental effects of hybrid Hyrax + FM and hybrid Hyrax + Mentoplate (MP) | Ca (17) MA (8.74 ± 1.20 years) Co (17) MA (9.43 ± 0.95 years) | No | Yes | Hybrid Hyrax devices were fitted on two paramedian mini-implants in the anterior palate; Mentoplate was inserted subapical to the lower incisors. | -Wits ≤ −2.0 mm -From 7 to 12 years -Anterior crossbite or incisor edge-to-edge relationship -Molar class III relationship | 34 patients were treated with Hybrid Hyrax. In 17, maxillary protraction was performed with FM, while the other 17 were treated in combination with MP. The expander screw was activated 4 times/day; the FM group wore 400 g elastics on each side 14–16 h per day while the MP full-time. | -Significant forward movement of A-point (FM GROUP: SNA + 2.23° ± 1.30°— p 0.000 *; ME: 2.23° ± 1.43°— p 0.000 *); -B-Point showed a larger sagittal change in the FM Group (SNB 1.51 ± 1.1°— p 0.000 *) compared to the ME group (SNB: − 0.30 ± 0.9°— p 0.070); -FM group showed a significant increase in the ML-NL + 1.86 ± 1.65° (p 0.000 *) and NSL-ML + 1.17 ± 1.48 (p 0.006 *); -Upper incisor inclination as well as the distance of the first upper Molar in relation to A-point did not change significantly in both groups. |
| Authors | SNA | SNB | ANB | OVB | OVJ | WITS | SN^GoMe or Equivalents | Upper Incisor Position | Lower Incisor Position |
|---|---|---|---|---|---|---|---|---|---|
| Al-Mozany et al./Almuzian et al. | 1.87 ± 1.06° | 2.02 ± 0.85° | 3.95 ± 0.57° | 1.21 ± 1.89 mm | 5.63 ± 1.36 mm | 5.16 ± 1.5 mm | Y-axis:1.95° ± 1.11° | UI-PP:2.98 ± 2.71° | LI-MP:3.2 ± 3.4° |
| Wilmes et al. | na | na | na | na | na | 2.7 ± 1.3 mm | na | na | na |
| Maino et al. | +2.50° | −0.92° | +3.41° | na | na | +4.92 mm | SN-GoGn: +1.64° | U1-PP: −2.26° Pr-VertT: +3.62 mm | na |
| Nienkemper et al. | 2.4° | −1.7° | 4.1° | −0.2 mm | 3.2 mm | 4.5 mm | Co-Go-Me: −2.0° | U1-PP: −0.5° | L1-MP: −1.7° |
| Hourfar et al. | 2.17° | −0.97° | +2.77° | na | na | na | ML/NSL: 1.46° | na | na |
| Seiryu et al. | +2.2 ± 1.3° | +0.1 ± 1.3 | +2.0 ± 1.3 | na | na | na | MP-SN: −0.1 ± 1.3 | U1-SN: −0.4 ± 4.2 | na |
| Ngan et al. | 1.59° | −0.8° | +2.4° | −0.14 mm | +3.46 mm | +2.58 mm | SNL-ML: +0.24° | Is-SNL: −2.03 | Ii-ML: −1.67 |
| Willmann et al. | FM: 2.23 ± 1.30 MP: 2.23 ± 1.43 | FM:−1.51 ± 1.13 MP: −0.30 ± 0.98 | FM: 3.75 ± 1.45 MP: 2.54 ± 0.99 | na | na | FM: 4.81 ± 1.38 MP: 4.14 ± 1.25 | ML-NSL: FM: 1.17 ± 1.48 MP: − 0.55 ± 1.09 | U1-PP°: FM:−1.15 ± 6.45 MP: 0.57 ± 5.49 | L1-ML°: FM: −3.84 ± 6.13 MP: 0.56 ± 3.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Apuzzo, F.; Nucci, L.; Strangio, B.M.; Inchingolo, A.D.; Dipalma, G.; Minervini, G.; Perillo, L.; Grassia, V. Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review. Appl. Sci. 2022, 12, 4646. https://doi.org/10.3390/app12094646
d’Apuzzo F, Nucci L, Strangio BM, Inchingolo AD, Dipalma G, Minervini G, Perillo L, Grassia V. Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review. Applied Sciences. 2022; 12(9):4646. https://doi.org/10.3390/app12094646
Chicago/Turabian Styled’Apuzzo, Fabrizia, Ludovica Nucci, Bruno M. Strangio, Alessio Danilo Inchingolo, Gianna Dipalma, Giuseppe Minervini, Letizia Perillo, and Vincenzo Grassia. 2022. "Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review" Applied Sciences 12, no. 9: 4646. https://doi.org/10.3390/app12094646
APA Styled’Apuzzo, F., Nucci, L., Strangio, B. M., Inchingolo, A. D., Dipalma, G., Minervini, G., Perillo, L., & Grassia, V. (2022). Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review. Applied Sciences, 12(9), 4646. https://doi.org/10.3390/app12094646