
A Comparison of the Validity of Three Exercise Tests for Estimating Maximal Oxygen Uptake in Korean Adults Aged 19–64 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Procedures
2.3. Measurement of VO2max and Maximal GXT
2.4. Treadmill Test
2.5. YMCA Step Test
2.6. PACER Test
2.7. Statistical Analysis
3. Results
3.1. Results of Measured Values in Three Submaximal Exercise Tests
3.2. Results of Multiple Regression Model to Estimate VO2max in Three Submaximal Exercise Tests
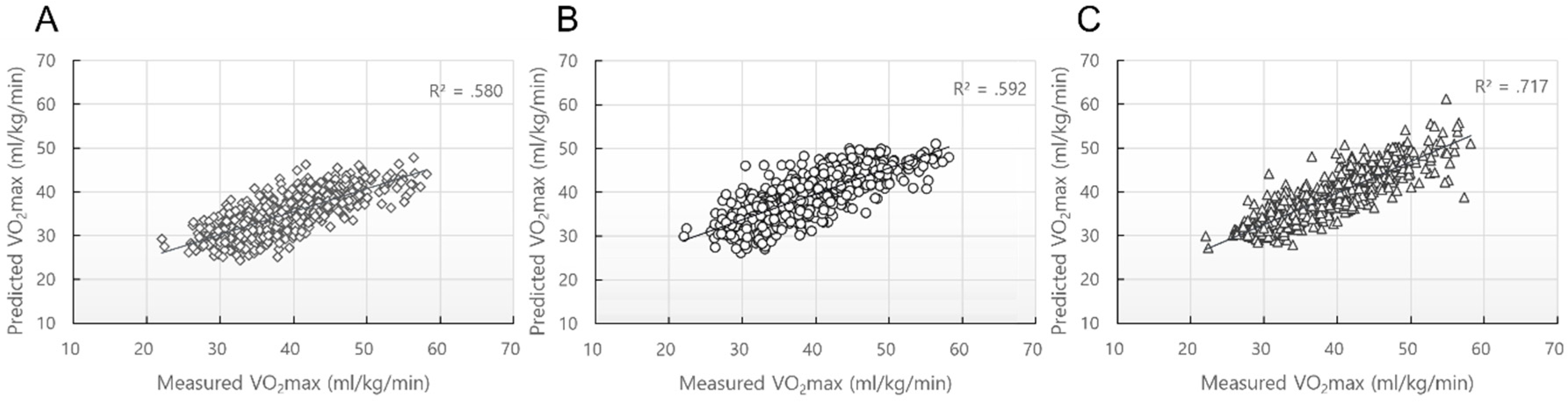
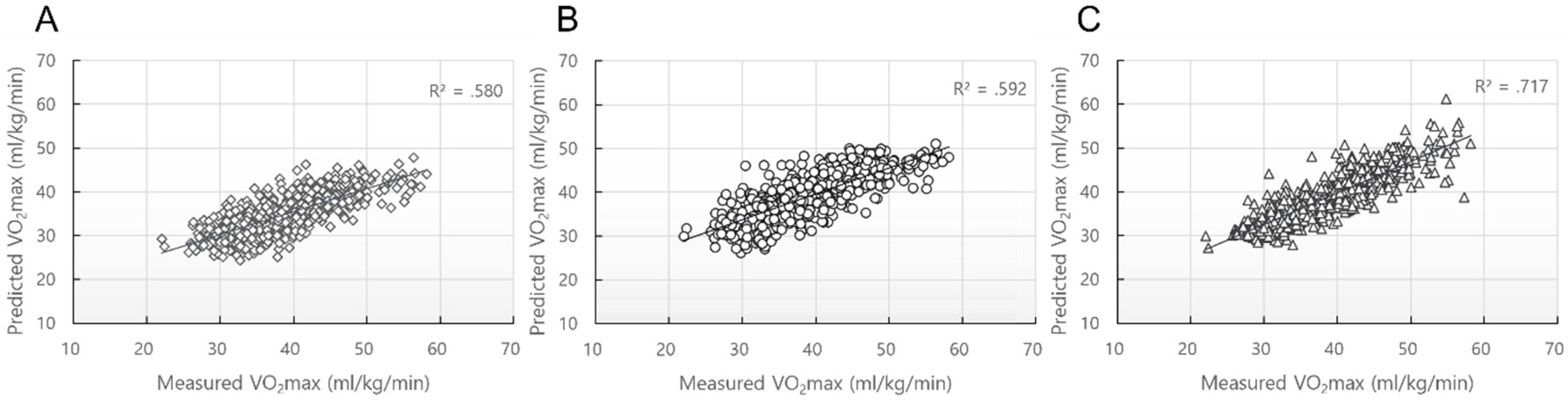
3.3. Comparison of the Validity of the Three Submaximal Exercise Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myers, J.; Kaykha, A.; George, S.; Abella, J.; Zaheer, N.; Lear, S.; Yamazaki, T.; Froelicher, V. Fitness versus physical activity patterns in predicting mortality in men. Am. J. Med. 2004, 117, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Jurca, R.; Jackson, A.S.; LaMonte, M.J.; Morrow, J.R., Jr.; Blair, S.N.; Wareham, N.J.; Haskell, H.L.; van Mechelen, W.; Church, T.S.; Jakicic, J.M.; et al. Assessing cardiorespiratory fitness without performing exercise testing. Am. J. Prev. Med. 2005, 29, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Weltman, A.; Snead, D.; Stein, P.; Seip, R.; Schurrer, R.; Rutt, R.; Weltman, J. Reliability and validity of a continuous incremental treadmill protocol for the determination of lactate threshold, fixed blood lactate concentrations, and VO2max. Int. J. Sports Med. 1990, 11, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, P.A.; Yoder, J.E.; Deuster, P.A. Comparison and cross-validation of cycle ergometry estimates of VO2max. Med. Sci. Sports Exerc. 1997, 29, 1513–1520. [Google Scholar] [CrossRef] [PubMed]
- Pollock, M.L.; Foster, C.; Schmidt, D.; Hellman, C.; Linnerud, A.C.; Ward, A. Comparative analysis of physiologic responses to three different maximal graded exercise test protocols in healthy women. Am. Heart J. 1982, 103, 363–373. [Google Scholar] [CrossRef]
- Andreacci, J.L.; Lemura, L.M.; Cohen, S.L.; Urbansky, E.A.; Chelland, S.A.; Duvillard, S.P.V. The effects of frequency of encouragement on performance during maximal exercise testing. J. Sports Sci. 2002, 20, 345–352. [Google Scholar] [CrossRef]
- Abut, F.; Akay, M.F. Machine learning and statistical methods for the prediction of maximal oxygen uptake: Recent advances. Med. Devices 2015, 8, 369. [Google Scholar]
- Huggett, D.L.; Connelly, D.M.; Overend, T.J. Maximal aerobic capacity testing of older adults: A critical review. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 57–66. [Google Scholar] [CrossRef]
- Vehrs, P.R.; George, J.D.; Fellingham, G.W.; Plowman, S.A.; Dustman-Allen, K. Submaximal treadmill exercise test to predict VO2max in fit adults. Meas. Phys. Educ. Exerc. Sci. 2007, 11, 61–72. [Google Scholar] [CrossRef]
- Bennett, H.; Parfitt, G.; Davison, K.; Eston, R. Validity of submaximal step tests to estimate maximal oxygen uptake in healthy adults. Sports Med. 2016, 46, 737–750. [Google Scholar] [CrossRef]
- Marsh, C.E. Evaluation of the American College of Sports Medicine submaximal treadmill running test for predicting VO2max. J. Strength Cond. Res. 2012, 26, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Lambert, J. A maximal multistage 20-m shuttle run test to predict VO2max. Eur. J. Appl. Physiol. 1982, 49, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Santo, A.S.; Golding, L.A. Predicting maximum oxygen uptake from a modified 3-minute step test. Res. Q. Exerc. Sport 2003, 74, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Shahnawaz, H. Influence of limb length on a stepping exercise. J. Appl. Physiol. 1978, 44, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Ponthieux, N.A.; Barker, D.G. Relationships between race and physical fitness. Res. Q. 1965, 36, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Johnson, W.D.; Blair, S.N.; Church, T.S.; Newton, R.L., Jr. Racial differences in the response of cardiorespiratory fitness to aerobic exercise training in Caucasian and African American postmenopausal women. J. Appl. Physiol. 2013, 114, 1375–1382. [Google Scholar] [CrossRef] [Green Version]
- Town, G.P.; Golding, L.A. Treadmill test to predict maximum aerobic capacity. J. Phys. Educ. 1977, 74, 6–8. [Google Scholar]
- Foster, C.; Crowe, A.J.; Daines, E.; Dumit, M.; Green, M.A.; Lettau, S.; Thompson, N.N.; Weymier, J. Predicting functional capacity during treadmill testing independent of exercise protocol. Med. Sci. Sports Exerc. 1996, 28, 752–756. [Google Scholar] [CrossRef]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Mahar, M.T.; Welk, G.J.; Rowe, D.A.; Crotts, D.J.; McIver, K.L. Development and validation of a regression model to estimate VO2peak from PACER 20-m shuttle run performance. J. Phys. Act. Health 2006, 3, S34–S46. [Google Scholar] [CrossRef] [Green Version]
- Lee, O.; Chung, J.W. Study on validation of 20 m progressive aerobic cardiovascular endurance run and estimation of maximal oxygen uptake in adolescents. Exerc. Sci. 2019, 28, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Noonan, V.; Dean, E. Submaximal exercise testing: Clinical application and interpretation. Phys. Ther. 2000, 80, 782–807. [Google Scholar] [CrossRef] [PubMed]
- Howley, E.T.; Bassett, D.R.; Welch, H.G. Criteria for maximal oxygen uptake: Review and commentary. Med. Sci. Sports Exerc. 1995, 27, 1292. [Google Scholar] [CrossRef] [PubMed]
- Loudon, J.K.; Cagle, P.E.; Figoni, S.F.; Nau, K.L.; Klein, R.M. A submaximal all-extremity exercise test to predict maximal oxygen consumption. Med. Sci. Sports Exerc. 1998, 30, 1299–1303. [Google Scholar] [CrossRef] [PubMed]
- Zwiren, L.D.; Freedson, P.S.; Ward, A.; Wilke, S.; Rippe, J.M. Estimation of VO2max: A comparative analysis of five exercise tests. Res. Q. Exerc. Sport 1991, 62, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.A.; Joseph, A.N.; Campagna, P.D. The prediction of VO2max: A comparison of 7 indirect tests of aerobic power. J. Strength Cond. Res. 1999, 13, 346–352. [Google Scholar] [CrossRef]
- Sun, M.; Gower, B.A.; Nagy, T.R.; Trowbridge, C.A.; Dezenberg, C.; Goran, M.I. Total, resting, and activity-related energy expenditures are similar in Caucasian and African-American children. Am. J. Physiol. 1998, 274, E232–E237. [Google Scholar] [CrossRef]
- Bruce, R.A.; Blackmon, J.R.; Jones, J.W.; Strait, G. Exercising testing in adult normal subjects and cardiac patients. Pediatrics 1963, 32, 742–756. [Google Scholar] [CrossRef]
- Hamlin, M.; Draper, N.; Blackwell, G.; Shearman, J.; Kimber, N. Determination of maximal oxygen uptake using the bruce or a novel athlete-led protocol in a mixed population. J. Hum. Kinet. 2011, 31, 97–104. [Google Scholar] [CrossRef] [Green Version]
- George, J.D.; Bradshaw, D.I.; Hyde, A.; Vehrs, P.R.; Hager, R.L.; Yanowitz, F.G. A maximal graded exercise test to accurately predict VO2max in 18–65-year-old adults. Meas. Phys. Educ. Exerc. Sci. 2007, 11, 149–160. [Google Scholar] [CrossRef]
- Lawrence, A.; Coldin, G. YMCA Fitness Testing and Assessment Manual; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Lee, O.; Lee, S.; Kang, M.; Mun, J.; Chung, J. Prediction of maximal oxygen consumption using the Young Men’s Christian Association-step test in Korean adults. Eur. J. Appl. Physiol. 2019, 119, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Lambrick, D.M.; Faulkner, J.A.; Rowlands, A.V.; Eston, R.G. Prediction of maximal oxygen uptake from submaximal ratings of perceived exertion and heart rate during a continuous exercise test: The efficacy of RPE 13. Eur. J. Appl. Physiol. 2009, 107, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Beutner, F.; Ubrich, R.; Zachariae, S.; Engel, C.; Sandri, M.; Teren, A.; Gielen, S. Validation of a brief step-test protocol for estimation of peak oxygen uptake. Eur. J. Prev. Cardiol. 2015, 22, 503–512. [Google Scholar] [CrossRef]
- McMurray, R.G.; Harrell, J.S.; Bradley, C.B.; Deng, S.H.I.B.I.N.G.; Bangdiwala, S.I. Predicted maximal aerobic power in youth is related to age, gender, and ethnicity. Med. Sci. Sports Exerc. 2002, 34, 145–151. [Google Scholar] [CrossRef]
- Van Kieu, N.T.; Jung, S.J.; Shin, S.W.; Jung, H.W.; Jung, E.S.; Won, Y.H.; Kim, Y.G.; Chae, S.W. The validity of the YMCA 3-minute step test for estimating maximal oxygen uptake in healthy Korean and Vietnamese adults. J. Lifestyle Med. 2020, 10, 21–29. [Google Scholar] [CrossRef]
- Matsuzaka, A.; Takahashi, Y.; Yamazoe, M.; Kumakura, N.; Ikeda, A.; Wilk, B.; Bar-Or, O. Validity of the multistage 20-m shuttle-run test for Japanese children, adolescents, and adults. Pediatr. Exerc. Sci. 2004, 16, 113–125. [Google Scholar] [CrossRef]
- Mahar, M.T.; Welk, G.J.; Rowe, D.A. Estimation of aerobic fitness from PACER performance with and without body mass index. Meas. Phys. Educ. Exerc. Sci. 2018, 22, 239–249. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Subgroup (n) | Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | |
|---|---|---|---|---|---|
| Males (287) | 19~24 (31) | 22.68 ± 1.49 | 176.08 ± 6.60 | 71.66 ± 8.73 | 23.16 ± 2.63 |
| 25~29 (33) | 27.27 ± 1.38 | 176.06 ± 4.58 | 74.44 ± 10.30 | 24.09 ± 3.24 | |
| 30~34 (34) | 32.09 ± 1.29 | 175.55 ± 5.96 | 73.61 ± 10.60 | 23.82 ± 3.14 | |
| 35~39 (33) | 37.15 ± 1.28 | 174.19 ± 6.49 | 77.02 ± 10.90 | 25.24 ± 2.96 | |
| 40~44 (34) | 41.71 ± 1.34 | 172.28 ± 5.46 | 71.08 ± 8.04 | 23.88 ± 2.23 | |
| 45~49 (34) | 46.79 ± 1.32 | 172.32 ± 4.74 | 75.14 ± 10.03 | 25.21 ± 2.99 | |
| 50~54 (23) | 52.70 ± 1.52 | 169.11 ± 5.95 | 71.77 ± 9.31 | 24.96 ± 2.14 | |
| 55~59 (34) | 56.82 ± 1.64 | 169.32 ± 5.42 | 69.76 ± 8.01 | 24.21 ± 2.19 | |
| 60~64 (31) | 62.29 ± 1.42 | 169.96 ± 6.25 | 65.35 ± 12.50 | 24.03 ± 2.48 | |
| Total (287) | 41.83 ± 12.83 | 172.56 ± 6.46 | 72.27 ± 10.30 | 24.28 ± 2.76 | |
| Females (254) | 19~24 (29) | 22.14 ± 1.58 | 162.69 ± 4.81 | 54.65 ± 6.93 | 20.86 ± 2.62 |
| 25~29 (26) | 27.46 ± 1.36 | 163.42 ± 6.02 | 54.41 ± 5.81 | 20.38 ± 1.81 | |
| 30~34 (26) | 31.77 ± 1.28 | 162.34 ± 5.36 | 56.64 ± 10.70 | 21.35 ± 3.15 | |
| 35~39 (36) | 36.81 ± 1.45 | 162.35 ± 6.24 | 57.31 ± 7.39 | 21.81 ± 2.44 | |
| 40~44 (31) | 42.10 ± 1.38 | 161.04 ± 4.51 | 59.97 ± 9.40 | 22.97 ± 3.24 | |
| 45~49 (26) | 47.04 ± 1.46 | 160.79 ± 5.15 | 57.42 ± 6.04 | 22.00 ± 2.23 | |
| 50~54 (32) | 52.66 ± 1.58 | 158.10 ± 4.21 | 55.51 ± 6.30 | 22.19 ± 2.16 | |
| 55~59 (27) | 56.89 ± 1.31 | 157.73 ± 4.85 | 57.57 ± 6.17 | 23.04 ± 2.31 | |
| 60~64 (21) | 61.62 ± 1.32 | 154.43 ± 5.56 | 56.86 ± 8.17 | 23.81 ± 3.11 | |
| Total (254) | 41.54 ± 12.48 | 160.50 ± 5.77 | 56.75 ± 7.64 | 22.01 ± 2.73 | |
| Total (541) | 41.69 ± 12.66 | 166.89 ± 8.60 | 64.98 ± 11.99 | 23.21 ± 2.97 | |
| Male (287) | Female (254) | Total (541) | |
|---|---|---|---|
| Maximal GXT | |||
| VO2max (mL/kg/min) | 42.63 ± 6.29 | 34.90 ± 5.23 | 39.01 ± 6.98 |
| Stable HR (bpm/min) | 73.44 ± 10.10 | 77.22 ± 8.88 | 75.21 ± 9.73 |
| Maximal RER | 1.23 ± 0.08 | 1.24 ± 0.09 | 1.23 ± 0.08 |
| Maximal HR (bpm/min) | 180.96 ± 13.15 | 176.32 ± 13.08 | 178.78 ± 13.31 |
| Treadmill test | |||
| Stage 3 HR (bpm/min) | 157.18 ± 13.55 | 169.91 ± 11.96 | 163.16 ± 14.30 |
| YMCA Step test | |||
| RHR (bpm/min) | 99.64 ± 16.24 | 107.46 ± 15.03 | 103.29 ± 16.14 |
| PACER test | |||
| Counts (# laps) | 50.65 ± 18.42 | 28.78 ± 11.92 | 40.38 ± 19.13 |
| Treadmill Test | YMCA Step Test | PACER Test | |
|---|---|---|---|
| Intercept | 68.828 | 60.400 | 43.418 |
| Sex | 8.428 | 9.138 | 5.114 |
| Age (years) | −0.249 | −0.229 | −0.094 |
| Height (cm) | 0.071 | 0.045 | −0.022 |
| Weight (kg) | −0.208 | −0.182 | −0.135 |
| Stage 3 HR (beat/min) | −0.137 | - | - |
| RHR (bpm/min) | - | −0.120 | - |
| Count (reps) | - | - | 0.229 |
| R | 0.762 | 0.770 | 0.847 |
| R2 | 0.580 | 0.592 | 0.717 |
| SEE | 4.545 | 4.478 | 3.732 |
| F | 147.801 | 155.466 | 270.900 |
| p | 0.000 | 0.000 | 0.000 |
| Durbin-Watson | 1.903 | 1.900 | 1.819 |
| N (541) | Regression Equation |
|---|---|
| Treadmill test | =68.828 + 8.428 (sex; male 1, female 0) − 0.249 (age) + 0.071 (height) − 0.208 (weight) − 0.137 (stage 3 HR) |
| YMCA step test | =60.400 + 9.138 (sex; male 1, female 0) − 0.229 (age) + 0.045 (height) − 0.182 (weight) − 0.120 (RHR) |
| PACER test | =43.418 + 5.114 (sex; male 1, female 0) − 0.094 (age) − 0.022 (height) − 0.135 (weight) + 0.229 (counts) |
| Predicted VO2max (mL/kg/min) | Measured-Predicted VO2max (mL/kg/min) | ICC (α) | CV (%) | |
|---|---|---|---|---|
| Treadmill test | 38.90 ± 5.32 | 0.108 ± 4.52 | 0.847 | 13.68 |
| YMCA step test | 38.97 ± 5.37 | 0.020 ± 4.45 | 0.853 | 13.78 |
| PACER test | 39.02 ± 5.92 | −0.010 ± 3.71 | 0.910 | 15.17 |
| Tests | B | SE | β | 95% CI | R | R2 | SEE | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Treadmill test | ||||||||
| Intercept | 0.129 | 1.438 | −2.696 | 2.954 | 0.762 | 0.580 | 4.528 | |
| Slope | 0.999 | 0.037 | 0.762 | 0.928 | 1.071 | |||
| YMCA Step test | ||||||||
| Intercept | 0.017 | 1.406 | −2.746 | 2.779 | 0.770 | 0.592 | 4.461 | |
| Slope | 1.000 | 0.036 | 0.770 | 0.930 | 1.070 | |||
| PACER test | ||||||||
| Intercept | 0.047 | 1.067 | −2.052 | 2.139 | ||||
| Slope | 0.999 | 0.027 | 0.847 | 0.946 | 1.052 | 0.847 | 0.717 | 3.718 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, J.; Lee, K. A Comparison of the Validity of Three Exercise Tests for Estimating Maximal Oxygen Uptake in Korean Adults Aged 19–64 Years. Appl. Sci. 2022, 12, 1371. https://doi.org/10.3390/app12031371
Chung J, Lee K. A Comparison of the Validity of Three Exercise Tests for Estimating Maximal Oxygen Uptake in Korean Adults Aged 19–64 Years. Applied Sciences. 2022; 12(3):1371. https://doi.org/10.3390/app12031371
Chicago/Turabian StyleChung, Jinwook, and Kihyuk Lee. 2022. "A Comparison of the Validity of Three Exercise Tests for Estimating Maximal Oxygen Uptake in Korean Adults Aged 19–64 Years" Applied Sciences 12, no. 3: 1371. https://doi.org/10.3390/app12031371
APA StyleChung, J., & Lee, K. (2022). A Comparison of the Validity of Three Exercise Tests for Estimating Maximal Oxygen Uptake in Korean Adults Aged 19–64 Years. Applied Sciences, 12(3), 1371. https://doi.org/10.3390/app12031371