
The Effect of Under-Drilling and Osseodensification Drilling on Low-Density Bone: A Comparative Ex Vivo Study




Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
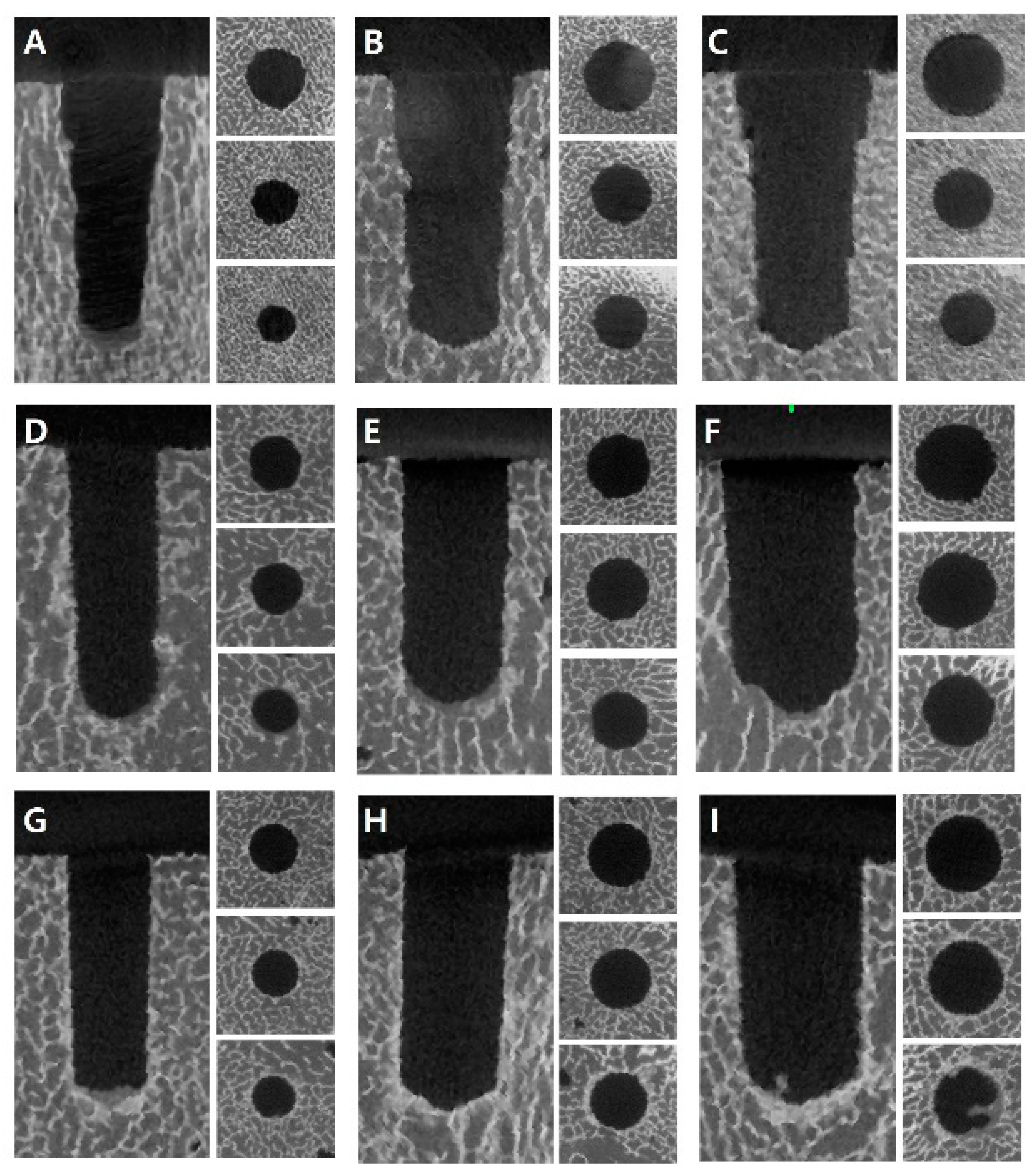
2.1. Bone Sample and Experimental Groups
2.2. Implant Bed Preparation and Implant Installation
2.3. Evaluation of Implant Primary Stability
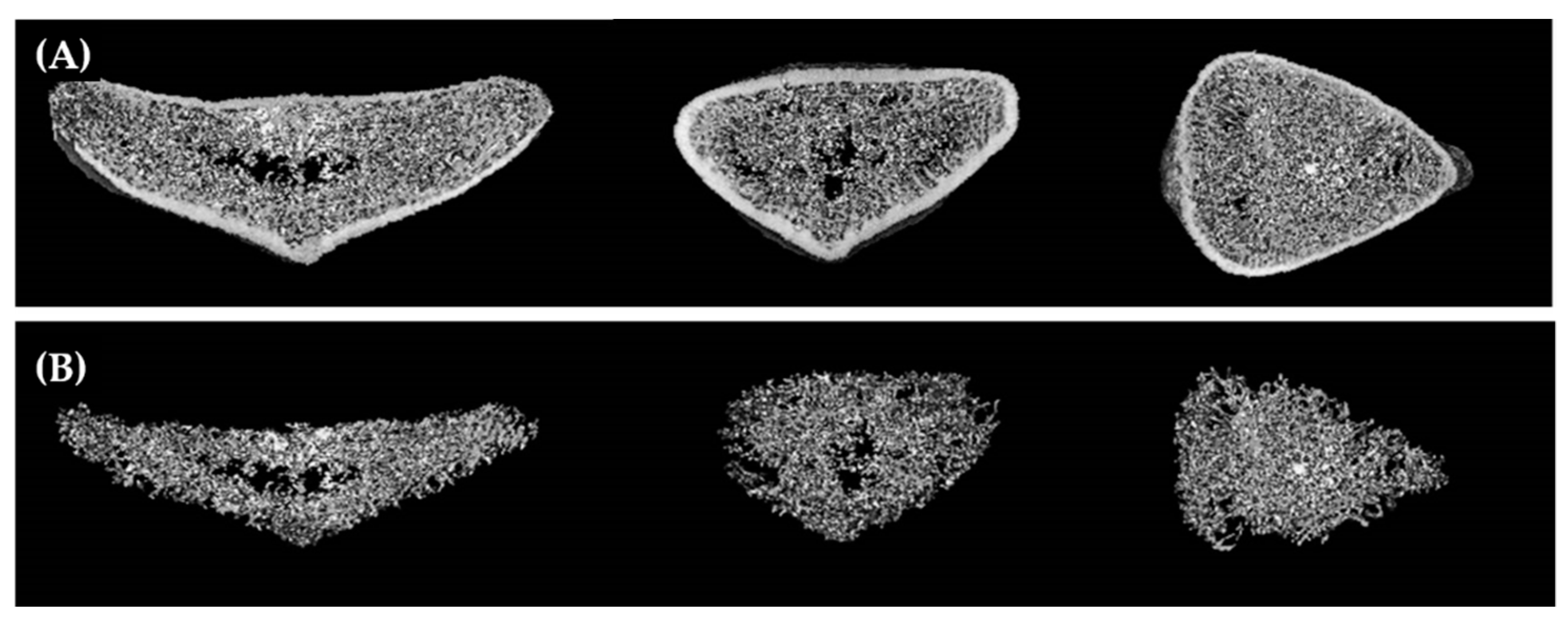
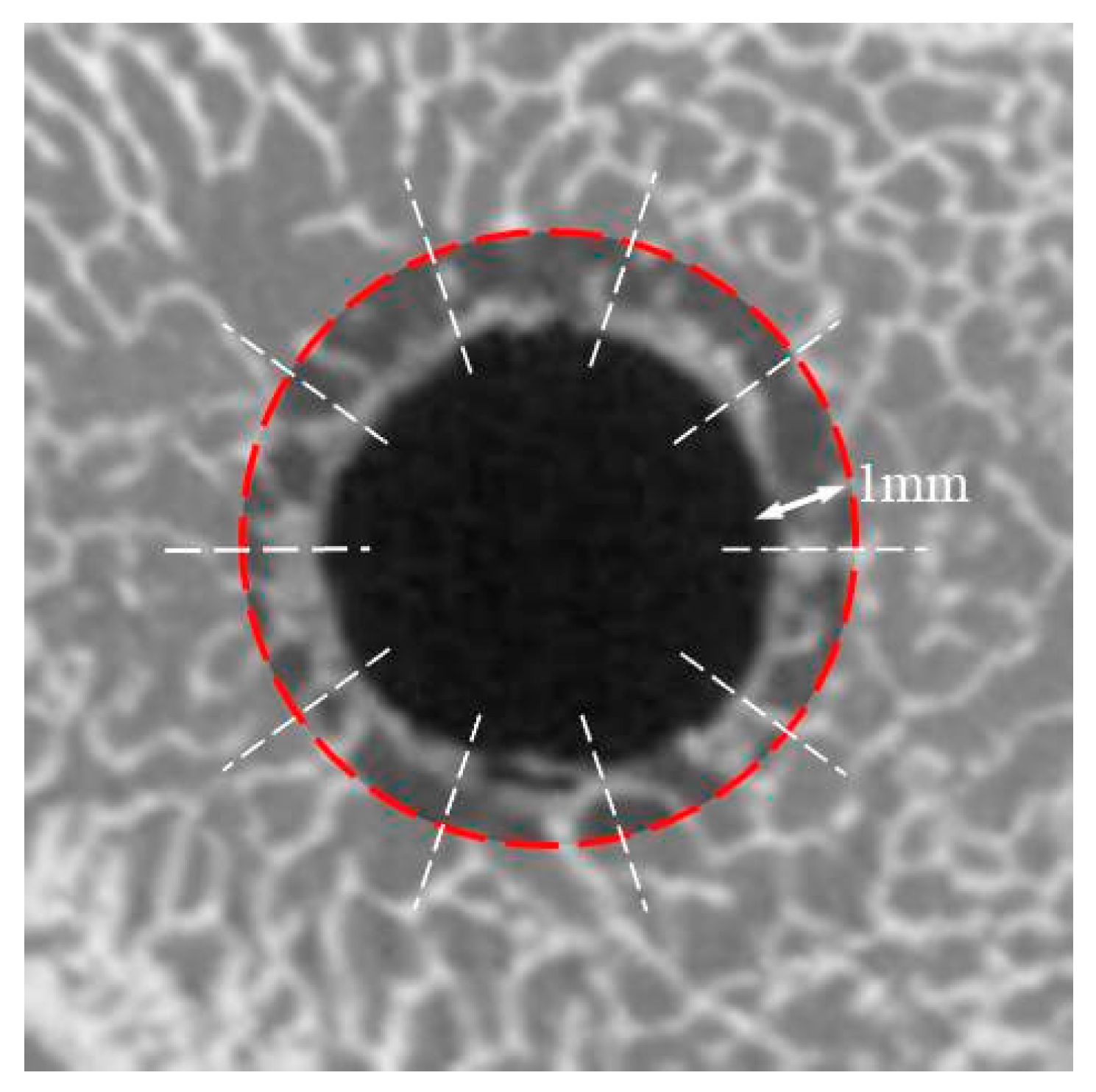
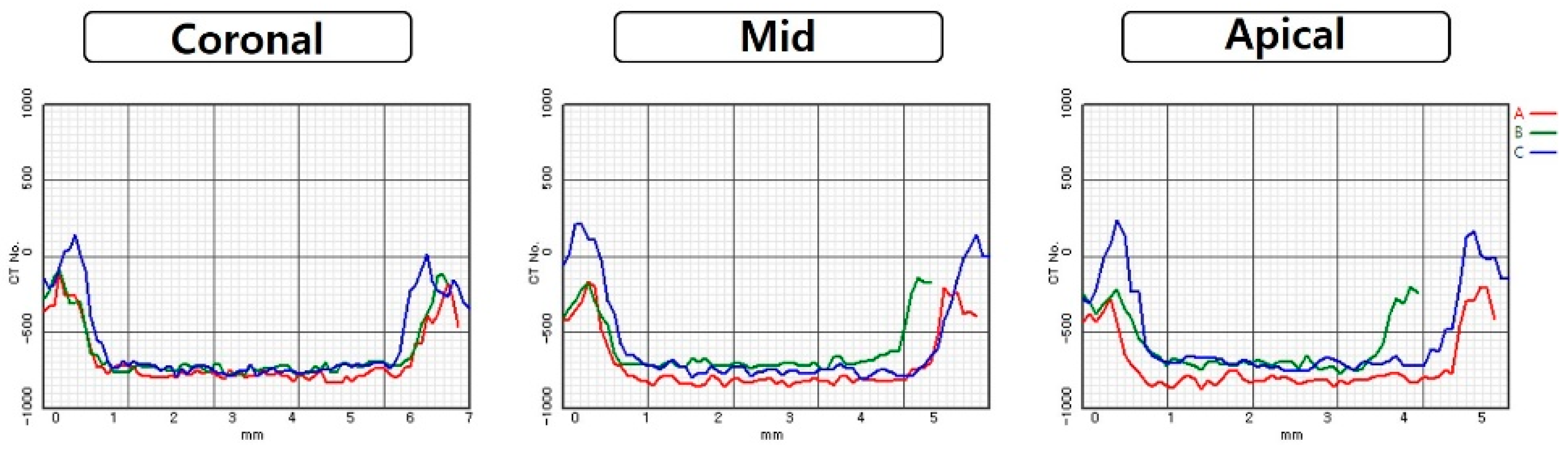
2.4. Evaluation of Bone Density
2.5. Statistical Analysis
3. Results
3.1. Implant Primary Stability
3.2. Bone Density
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brånemark, P.I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated titanium implants: Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trisi, P.; Perfetti, G.; Baldoni, E.; Berardi, D.; Colagiovanni, M.; Scogna, G. Implant micromotion is related to peak insertion torque and bone density. Clin. Oral Implants Res. 2009, 20, 467–471. [Google Scholar] [CrossRef]
- Brunski, J.B. In vivo bone response to biomechanical loading at the bone/dental-implant interface. Adv. Dent. Res. 1999, 13, 99–119. [Google Scholar] [CrossRef] [PubMed]
- Stanford, C.M.; Brand, R.A. Toward an understanding of implant occlusion and strain adaptive bone modeling and remodeling. J. Prosthet. Dent. 1999, 81, 553–561. [Google Scholar] [CrossRef]
- Fugazzotto, P.A.; Wheeler, S.L.; Lindsay, J.A. Success and failure rates of cylinder implants in type IV bone. J. Periodontol. 1993, 64, 1085–1087. [Google Scholar] [CrossRef] [PubMed]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implants Res. 2006, 17, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Duyck, J.; Vandamme, K.; Geris, L.; van Oosterwyck, H.; De Cooman, M.; Vandersloten, J.; Puers, R.; Naert, I. The influence of micro-motion on the tissue differentiation around immediately loaded cylindrical turned titanium implants. Arch. Oral Biol. 2006, 51, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Soballe, K.; Brockstedt-Rasmussen, H.; Hansen, E.S.; Bunger, C. Hydroxyapatite coating modifies implant membrane formation. Controlled micromotion studied in dogs. Acta Orthop. Scand. 1992, 63, 128–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podaropoulos, L. Increasing the stability of dental implants: The concept of osseodensification. Balk. J. Dent. Med. 2017, 21, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early wound healing around endosseous implants: A review of the literature. Int. J. Oral Maxillofac. Implants 2005, 20, 425–431. [Google Scholar] [PubMed]
- Norton, M.R.; Gamble, C. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implants Res. 2001, 12, 79–84. [Google Scholar] [CrossRef]
- Jaffin, R.A.; Berman, C.L. The excessive loss of Branemark fixtures in type IV bone: A 5-year analysis. J. Periodontol. 1991, 62, 2–4. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, R.C.G.; Leles, C.R.; Normanha, L.M.; Lindh, C.; Ribeiro-Rotta, R.F. Assessments of trabecular bone density at implant sites on CT images. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Lindh, C.; Obrant, K.; Petersson, A. Maxillary bone mineral density and its relationship to the bone mineral density of the lumbar spine and hip. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 98, 102–109. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; Tözüm, T.; Tumer, C. Bone density assessments of oral implant sites using computerized tomography. J. Oral Rehabil. 2007, 34, 267–272. [Google Scholar] [CrossRef]
- Isoda, K.; Ayukawa, Y.; Tsukiyama, Y.; Sogo, M.; Matsushita, Y.; Koyano, K. Relationship between the bone density estimated by cone-beam computed tomography and the primary stability of dental implants. Clin. Oral Implants Res. 2012, 23, 832–836. [Google Scholar] [CrossRef]
- Jackson, C.; Ghosh, S.; Johnson, W. On the evolution of drill-bit shapes. J. Mech. Work. Technol. 1989, 18, 231–267. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A. Influence of underpreparation on primary stability of implants inserted in poor quality bone sites: An in vitro study. J. Oral Maxillofac. Surg. 2015, 73, 1084–1088. [Google Scholar] [CrossRef]
- Alghamdi, H.; Anand, P.S.; Anil, S. Undersized implant site preparation to enhance primary implant stability in poor bone density: A prospective clinical study. J. Oral Maxillofac. Surg. 2011, 69, e506–e512. [Google Scholar] [CrossRef]
- Boustany, C.M.; Reed, H.; Cunningham, G.; Richards, M.; Kanawati, A. Effect of a modified stepped osteotomy on the primary stability of dental implants in low-density bone: A cadaver study. Int. J. Oral Maxillofac. Implants 2015, 30, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Summers, R.B. A new concept in maxillary implant surgery: The osteotome technique. Compendium 1994, 15, 154–156. Available online: https://pubmed.ncbi.nlm.nih.gov/8055503 (accessed on 19 July 2021).
- Huwais, S.; Meyer, E.G. A novel osseous densification approach in implant osteotomy preparation to increase biomechanical primary stability, bone mineral density, and bone-to-implant contact. Int. J. Oral Maxillofac. Implants 2017, 32, 27–36. [Google Scholar] [CrossRef]
- Almutairi, A.S.; Walid, M.A.; Alkhodary, M.A. The effect of osseodensification and different thread designs on the dental implant primary stability. F1000Research 2018, 7, 1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cáceres, F.; Troncoso, C.; Silva, R.; Pinto, N. Effects of osseodensification protocol on insertion, removal torques, and resonance frequency analysis of BioHorizons® conical implants. An ex vivo study. J. Oral Biol. Craniofacial Res. 2020, 10, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Boutroy, S.; Bouxsein, M.L.; Munoz, F.; Delmas, P.D. In vivo assessment of trabecular bone microarchitecture by high-resolution peripheral quantitative computed tomography. J. Clin. Endocrinol. Metab. 2005, 90, 6508–6515. [Google Scholar] [CrossRef] [Green Version]
- Link, T.M.; Bauer, J.; Kollstedt, A.; Stumpf, I.; Hudelmaier, M. Trabecular bone structure of the distal radius, the calcaneus, and the spine: Which site predicts fracture status of the spine best? Investig. Radiol. 2004, 39, 487–497. [Google Scholar] [CrossRef]
- Montangero, V.E.; Capiglioni, R.; Roldán, E.J. Mandible and maxilla bone mineral density and threshold analysis studies by pQCT in two edentulous women receiving pamidronate. Cranio 2003, 21, 110–115. [Google Scholar] [CrossRef]
- Norton, M.R. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. Int. J. Oral Maxillofac. Implants 2011, 26, 1333–1343. [Google Scholar] [PubMed]
- Ottoni, J.M.P.; Oliveira, Z.F.L.; Mansini, R.; Cabral, A.M. Correlation between placement torque and survival of single-tooth implants. Int. J. Oral Maxillofac. Implants 2005, 20, 769–776. [Google Scholar]
- Trisi, P.; Berardi, D.; Paolantonio, M.; Spoto, G.; D’Addona, A.; Perfetti, G. Primary stability, insertion torque, and bone density of conical implants with internal hexagon: Is there a relationship? J. Craniofacial Surg. 2013, 24, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Alfonsi, F.; Derchi, G.; Tonelli, P.; Toti, P.; Marchionni, S.; Covani, U. The effect of insertion torque on the clinical outcome of single implants: A randomized clinical trial. Clin. Implants Dent. Relat. Res. 2016, 18, 588–600. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Lang, N.P.; Rangert, B. Validity and clinical significance of biomechanical testing of implant/bone interface. Clin. Oral Implants Res. 2006, 17, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Sennerby, L.; Meredith, N. Resonance frequency analysis: Measuring implant stability and osseointegration. Compend. Contin. Educ. Dent. 1998, 19, 493–498. [Google Scholar] [PubMed]
- Gallardo, S.; Ibanez, M.C.; Ibanez, J.C. Correlation between ISQ and insertion torque values using double acid-etched implants. J. Osseointegr. 2016, 8, 29–36. [Google Scholar] [CrossRef]
- Kold, S.; Bechtold, J.; Ding, M.; Chareancholvanich, K.; Rahbek, O.; Søballe, K. Compacted cancellous bone has a spring-back effect. Acta Orthop. Scand. 2003, 74, 591–595. [Google Scholar] [CrossRef]
- Alifarag, A.M.; Lopez, C.D.; Neiva, R.F.; Tovar, N.; Witek, L.; Coelho, P.G. Atemporal osseointegration: Early biomechanical stability through osseodensification. J. Orthop. Res. 2018, 36, 2516–2523. [Google Scholar] [CrossRef] [Green Version]
- Bergamo, E.T.P.; Zahoui, A.; Barrera, R.B.; Huwais, S.; Coelho, P.G.; Karateew, E.D.; Bonfante, E.A. Osseodensification effect on implants primary and secondary stability: Multicenter controlled clinical trial. Clin. Implants Dent. Relat. Res. 2021, 23, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P. New osseodensification implant site preparation method to increase bone density in low-density bone: In vivo evaluation in sheep. Implants Dent. 2016, 25, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padhye, N.M.; Padhye, A.M.; Bhatavadekar, N.B. Osseodensification––A systematic review and qualitative analysis of published literature. J. Oral Biol. Craniofacial Res. 2020, 10, 375–380. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | ISQ Value | Comparison between Groups * | |
|---|---|---|---|
| A | Standard drilling with CD | 66.35 ± 2.11 | C, D |
| B | Standard drilling with OD-C | 67.85 ± 3.59 | C, E |
| C | Standard drilling with OD-CC | 71.25 ± 2.57 | A, B, D, F |
| D | Under-drilling with CD | 74.25 ± 2.10 | A, C, F |
| E | Under-drilling with OD-C | 78.30 ± 3.83 | B, F |
| F | Under-drilling with OD-CC | 81.25 ± 3.09 | C, D, E |
| Group | ISQ Value | Comparison between Groups * | |
|---|---|---|---|
| A | Standard drilling with CD | −4.38 ± 1.58 | C, D |
| B | Standard drilling with OD-C | −5.49 ± 1.51 | E |
| C | Standard drilling with OD-CC | −6.10 ± 0.87 | A, F |
| D | Under-drilling with CD | −6.23 ± 0.87 | A, F |
| E | Under-drilling with OD-C | −7.02 ± 0.98 | B, F |
| F | Under-drilling with OD-CC | −7.67 ± 0.47 | C, D, E |
| Drilling Diameter | Coronal Area | Middle Area | Apical Area | |
|---|---|---|---|---|
| CD | 3.8 mm | 587.50 ± 65.24 | 572.50 ± 84.17 | 583.33 ± 83.39 |
| 4.8 mm | 604.17 ± 71.94 | 610.83 ± 61.48 | 615.00 ± 87.74 | |
| 5.8 mm | 615.84 ± 61.41 | 595.00 ± 87.94 | 582.50 ± 81.25 | |
| OD-C | 3.5 mm | 602.50 ± 69.28 | 604.17 ± 61.97 | 606.67 ± 63.29 |
| 4.5 mm | 588.33 ± 64.57 | 611.67 ± 72.14 | 611.67 ± 75.64 | |
| 5.5 mm | 605.83 ± 82.44 | 603.33 ± 69.09 | 596.67 ± 86.29 | |
| OD-CC | 3.5 mm | 648.33 ± 76.26 | 647.50 ± 59.94 | 704.17 ± 52.56 |
| 4.5 mm | 672.50 ± 76.38 | 690.00 ± 75.89 | 745.83 ± 74.30 | |
| 5.5 mm | 685.00 ± 59.67 | 714.17 ± 73.01 | 776.67 ± 79.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, D.-J.; Moon, S.-Y.; You, J.-S.; Lee, W.-P.; Oh, J.-S. The Effect of Under-Drilling and Osseodensification Drilling on Low-Density Bone: A Comparative Ex Vivo Study. Appl. Sci. 2022, 12, 1163. https://doi.org/10.3390/app12031163
Seo D-J, Moon S-Y, You J-S, Lee W-P, Oh J-S. The Effect of Under-Drilling and Osseodensification Drilling on Low-Density Bone: A Comparative Ex Vivo Study. Applied Sciences. 2022; 12(3):1163. https://doi.org/10.3390/app12031163
Chicago/Turabian StyleSeo, Dong-Jun, Seong-Yong Moon, Jae-Seek You, Won-Pyo Lee, and Ji-Su Oh. 2022. "The Effect of Under-Drilling and Osseodensification Drilling on Low-Density Bone: A Comparative Ex Vivo Study" Applied Sciences 12, no. 3: 1163. https://doi.org/10.3390/app12031163
APA StyleSeo, D.-J., Moon, S.-Y., You, J.-S., Lee, W.-P., & Oh, J.-S. (2022). The Effect of Under-Drilling and Osseodensification Drilling on Low-Density Bone: A Comparative Ex Vivo Study. Applied Sciences, 12(3), 1163. https://doi.org/10.3390/app12031163