
The Speed of Pathogen Eradication May Prevent the Early Development of Cartilage Destruction: Case Series of Long-Term Follow-Up of Septic Arthritis (SA) after Anterior Cruciate Ligament Reconstruction (ACL-R) and Literature Review

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
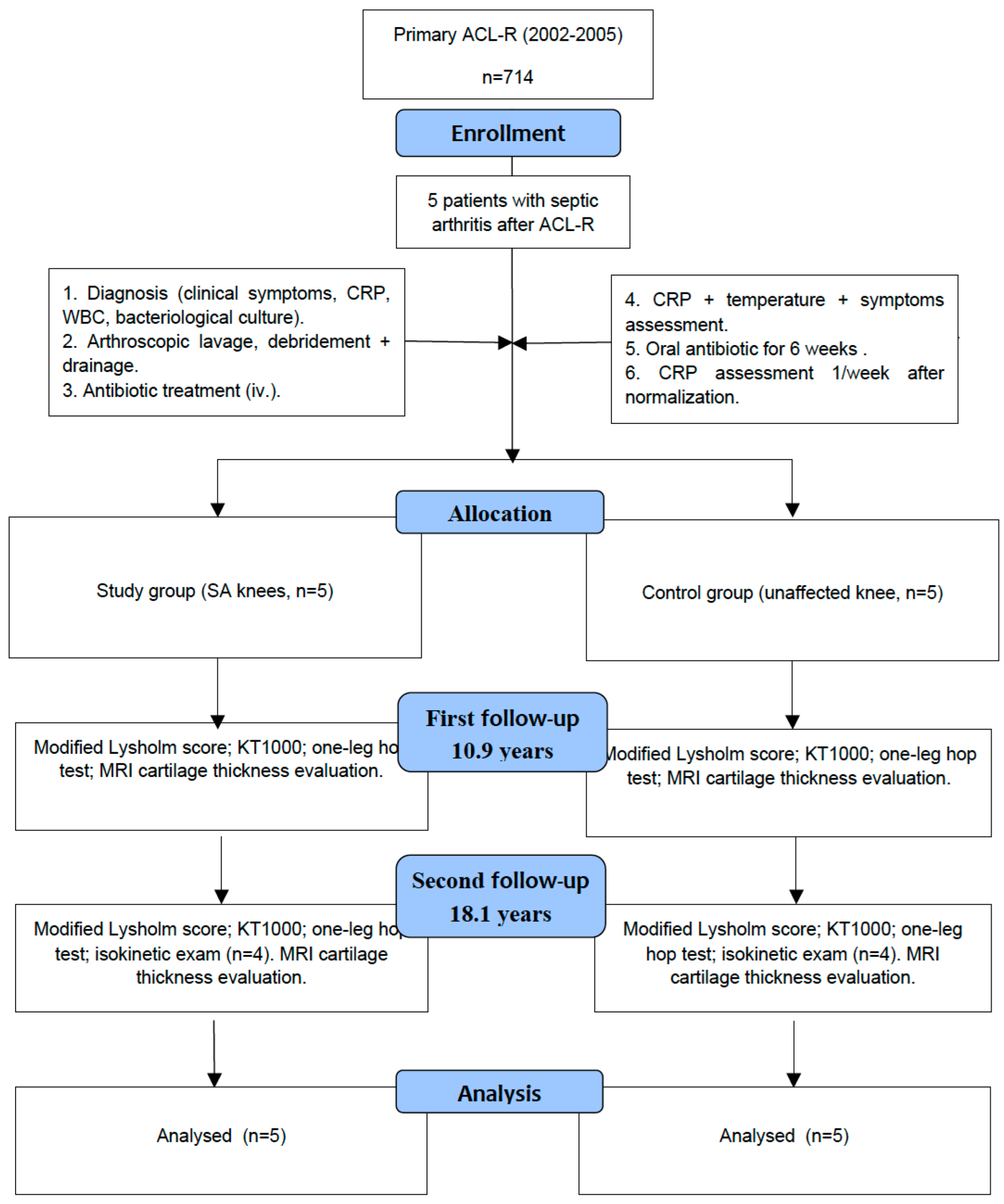
2.1. Study Design
2.2. ACL-R and Acute Knee Arthritis Diagnosis
2.3. Management and Treatment Protocol of Acute Knee Arthritis after ACL-R
2.4. Clinical Examination
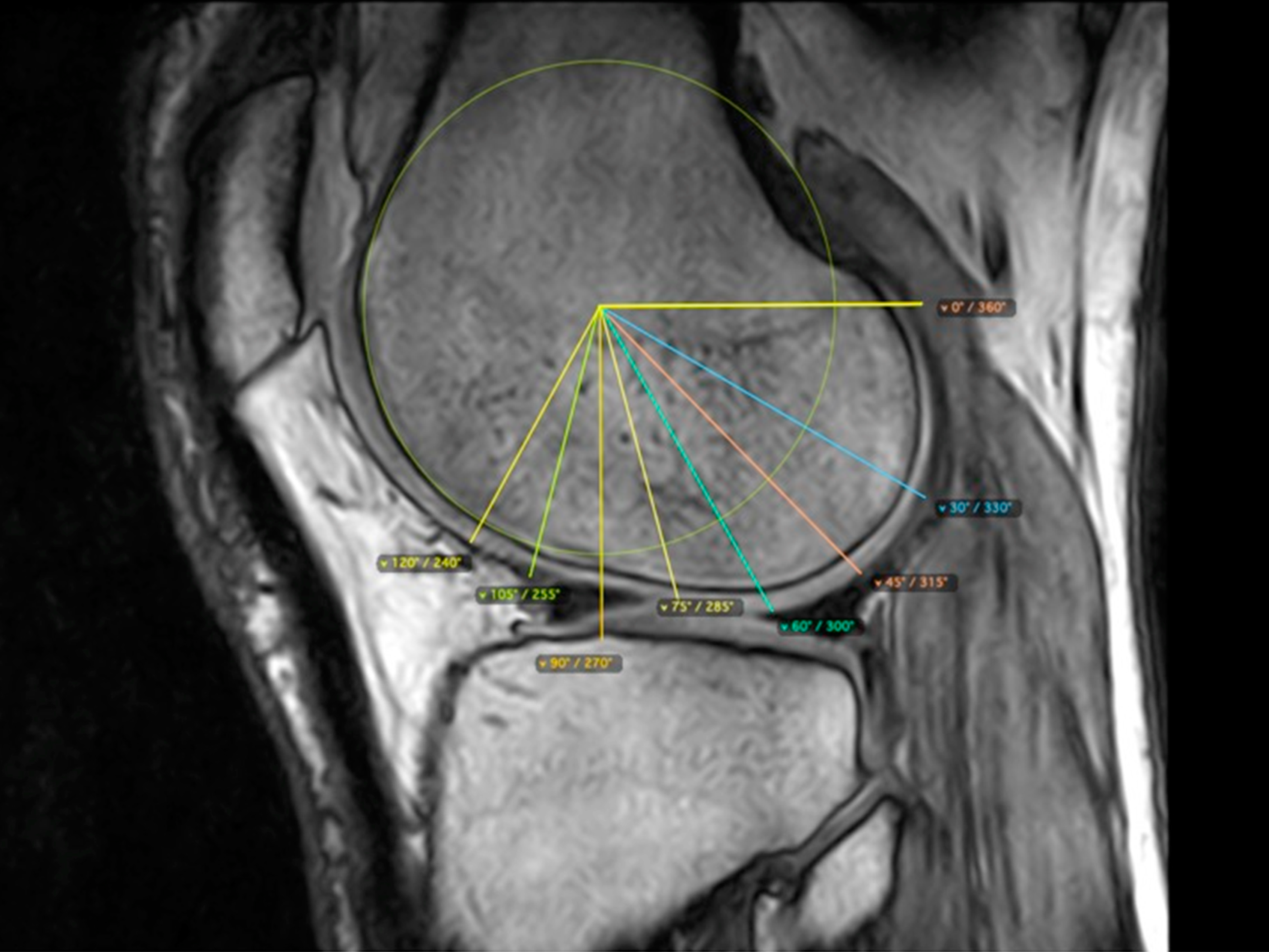
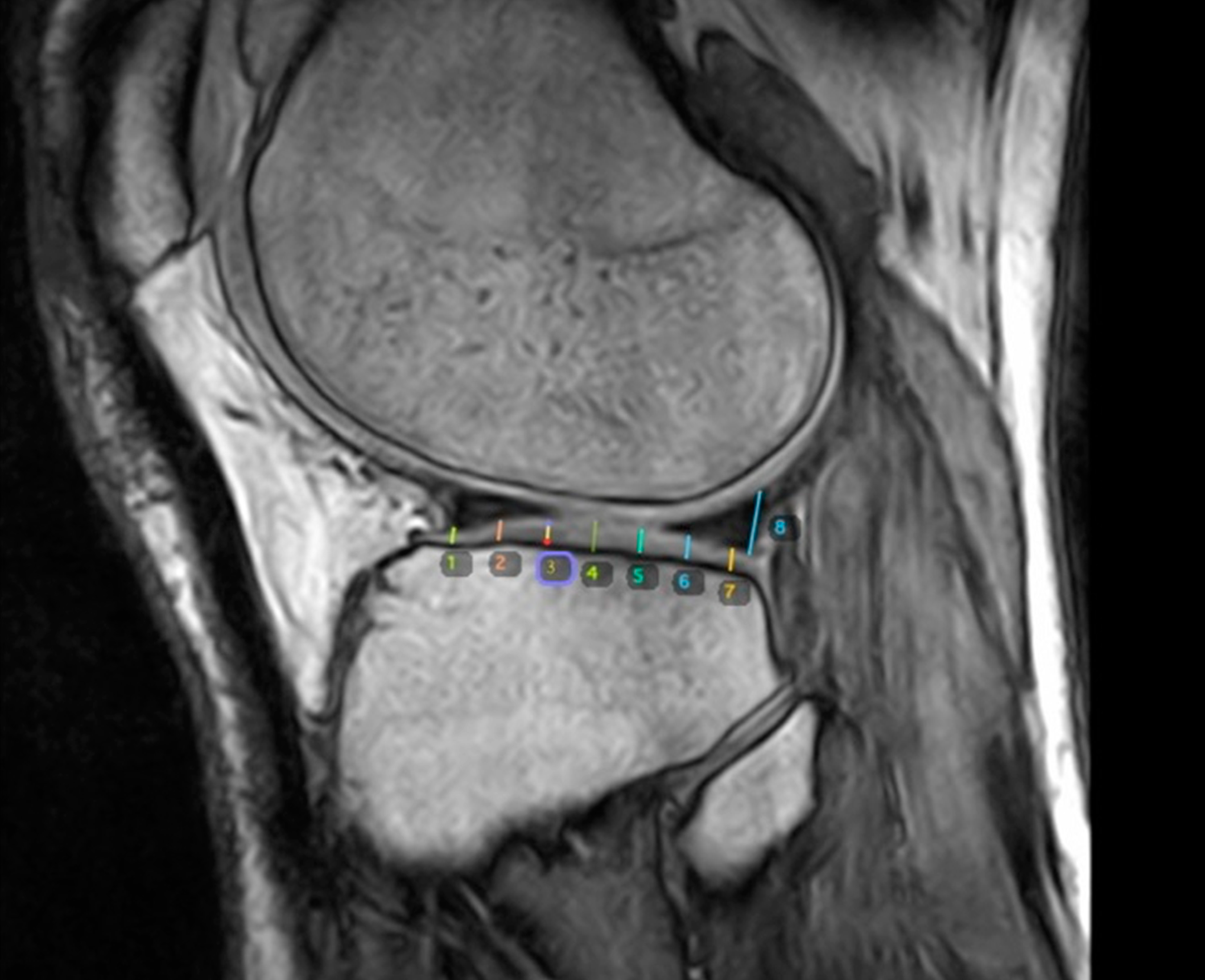
2.5. Evaluation of Knee Cartilage Thickness Using MRI
2.6. Medial and Lateral Femoral Condyle
2.7. Medial and Lateral Tibial Condyle
2.8. Treatment Costs
2.9. Statistical Analysis
3. Results
3.1. Clinical and Functional Results
3.2. Isokinetic Results
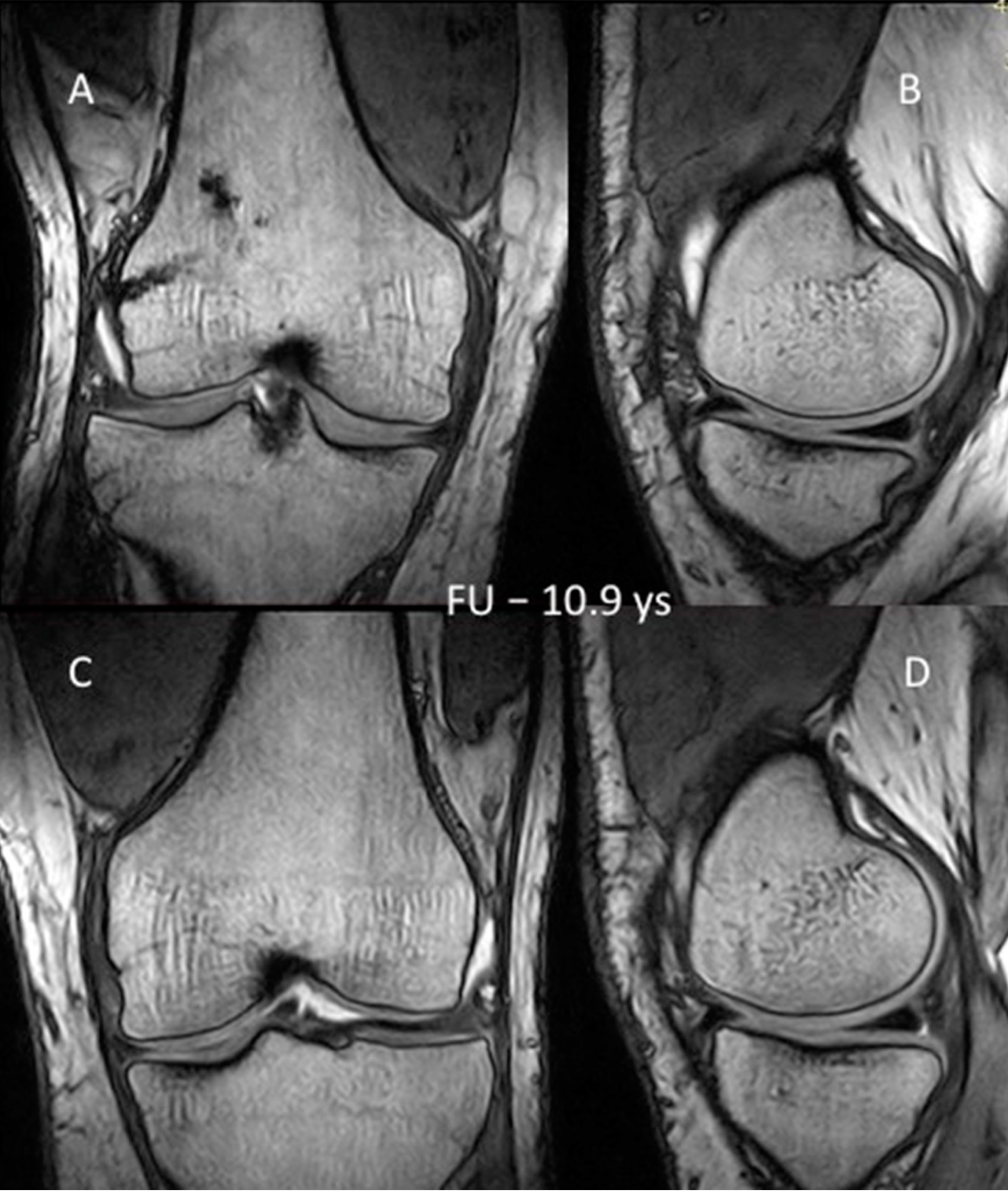
3.3. MRI Evaluation of the Cartilage
4. Discussion
5. Conclusions
- Arthroscopic lavage and debridement combined with flow drainage led to more rapid normalization of CRP values, objectively reflecting the process of infection eradication after ACL-R compared to arthroscopic debridement and lavage alone.
- By faster eradication of infection, the patient can be protected against the early development of degenerative changes, and the treatment costs can be reduced.
- The quantitative evaluation of knee cartilage after SA following ACL-R, proposed for the first time in the present study, may be more accurate for assessing the early symptoms of OA and predicting its development.
- The isokinetic evaluation revealed that despite normalization of hamstring peak torque, deficit of the quadriceps may still persist after a mean of 18.1 years follow-up.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Demirag, B.; Unal, O.K.; Ozakin, C. Graft retaining debridement in patients with septic arthritis after anterior cruciate ligament reconstruction. Acta Orthop. Traumatol. Turc. 2011, 45, 342–347. [Google Scholar] [PubMed]
- Judd, D.; Bottoni, C.; Kim, D.; Burke, M.; Hooker, S. Infections following arthroscopic anterior cruciate ligament reconstruction. Arthroscopy 2006, 22, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Mouzopoulos, G.; Fotopoulos, V.C.; Tzurbakis, M. Septic knee arthritis following ACL reconstruction: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Matava, M.J.; Evans, T.A.; Wright, R.W.; Shively, R.A. Septic arthritis of the knee following anterior cruciate ligament reconstruction: Results of a survey of sports medicine fellowship directors. Arthroscopy 1998, 14, 717–725. [Google Scholar] [CrossRef]
- Wang, C.; Ao, Y.; Wang, J.; Hu, Y.; Cui, G.; Yu, J. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: A retrospective analysis of incidence, presentation, treatment, and cause. Arthroscopy 2009, 25, 243–249. [Google Scholar] [CrossRef]
- Schollin-Borg, M.; Michaëlsson, K.; Rahme, H. Presentation, outcome, and cause of septic arthritis after anterior cruciate ligament reconstruction: A case control study. Arthroscopy 2003, 19, 941–947. [Google Scholar] [CrossRef]
- Vallianatos, P.G.; Tilentzoglou, A.C.; Koutsoukou, A.D. Septic arthritis caused by Erysipelothrix rhusiopathiae infection after arthroscopically assisted anterior cruciate ligament reconstruction. Arthroscopy 2003, 19, E26. [Google Scholar]
- Monaco, E.; Maestri, B.; Labianca, L. Clinical and radiological outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. J. Orthop. Sci. 2010, 15, 198–203. [Google Scholar] [CrossRef]
- Fong, S.Y.; Tan, J.L. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction. Ann. Acad. Med. 2004, 33, 228–234. [Google Scholar]
- Katz, L.M.; Battaglia, T.C.; Patino, P.; Reichmann, W.; Hunter, D.J.; Richmond, J.C. A retrospective comparison of the incidence of bacterial infection following anterior cruciate ligament reconstruction with autograft versus allograft. Arthroscopy 2008, 24, 1330–1335. [Google Scholar] [CrossRef]
- Van Tongel, A.; Stuyck, J.; Bellemans, J. Septic arthritis after arthroscopic anterior cruciate ligament reconstruction: A retrospective analysis of incidence, management and outcome. Am. J. Sports Med. 2007, 35, 1059–1063. [Google Scholar] [CrossRef] [PubMed]
- Indelli, P.F.; Dillingham, M.; Fanton, G. Septic arthritis in postoperative anterior cruciate ligament reconstruction. Clin. Orthop. Relat. Res. 2002, 398, 182–188. [Google Scholar] [CrossRef]
- Cadet, E.R.; Makhni, E.C.; Mehran, N.; Schulz, B.M. Management of septic arthritis following anterior cruciate ligament reconstruction: A review of current practices and recommendations. J. Am. Acad. Orthop. Surg. 2013, 21, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Karnatzikos, G.; Chaurasia, S.; Abhishek, M.; Bulgherhoni, E.; Lane, J. Postoperative infection after anterior cruciate ligament reconstruction. Sports Health 2016, 8, 187–189. [Google Scholar] [CrossRef]
- Lo Presti, M.; Costa, G.G.; Grassi, A.; Cialdella, S.; Agrò, G.; Busacca, M.; Pia Neri, M.; Filardo, G.; Zaffagnini, S. Graft-preserving arthroscopic debridement with hardware removal is effective for septic arthritis after anterior cruciate ligament reconstruction: A clinical, arthrometric, and magnetic resonance imaging evaluation. Am. J. Sports Med. 2020, 48, 1907–1915. [Google Scholar] [CrossRef]
- Meglic, U.; Salapura, V.; Zupanc, O. MRI Findings of Early Osteoarthritis in Patients Who Sustained Septic Arthritis of the Knee After ACL Reconstruction. Orthop. J. Sports Med. 2021, 9, 23259671211052519. [Google Scholar] [CrossRef] [PubMed]
- Calvo, R.; Figueroa, D.; Anastasiadis, Z.; Vaisman, A.; Olid, G.; Gili, F.; Valderrama, J.J.; De La Fuente, P. Septic arthritis in ACL reconstruction surgery with hamstring autografts. Eleven years of experience. Knee 2014, 21, 717–720. [Google Scholar] [CrossRef]
- Louboutin, H.; Debarge, R.; Richou, J.; Selmi, T.A.; Donell, S.T.; Neyret, P.; Dubrana, F. Osteoarthritis in patients with anterior cruciate ligament rupture: A review of risk factors. Knee 2009, 16, 239–244. [Google Scholar] [CrossRef]
- Schulz, A.P.; Götze, S.; Schmidt, H.G.; Jürgens, C.; Faschingbauer, M. Septic arthritis of the knee after anterior cruciate ligament surgery: A stage-adapted treatment regimen. Am. J. Sports Med. 2007, 35, 1064–1069. [Google Scholar] [CrossRef]
- Schuster, P.; Schulz, M.; Immendoerfer, M.; Mayer, P.; Schlumberger, M.; Richter, J. Septic Arthritis After Arthroscopic Anterior Cruciate Ligament Reconstruction: Evaluation of an Arthroscopic Graft-Retaining Treatment Protocol. Am. J. Sports Med. 2015, 43, 3005–3012. [Google Scholar] [CrossRef]
- Abdel-Aziz, A.; Radwan, Y.A.; Rizk, A. Multiple arthroscopic debridement and graft retention in septic knee arthritis after ACL reconstruction: A prospective case-control study. Int. Orthop. 2014, 38, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Waszczykowski, M.; Fabiś-Strobin, A.; Bednarski, I.; Lesiak, A.; Narbutt, J.; Fabiś, J. Serum Biomarkers of Inflammation and Turnover of Joint Cartilage Can Help Differentiate Psoriatic Arthritis (PsA) Patients from Osteoarthritis (OA) Patients. Diagnostics 2020, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Waszczykowski, M.; Fabiś-Strobin, A.; Bednarski, I.; Narbutt, J.; Fabiś, J. Serum and synovial fluid concentrations of interleukin-18 and interleukin-20 in patients with osteoarthritis of the knee and their correlation with other markers of inflammation and turnover of joint cartilage. Arch. Med. Sci. 2022, 18, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.L.; Kajiyama, G.; Schurman, D.J. Staphylococcal septic arthritis: Antibiotic and nonsteroidal anti-inflammatory drug treatment in a rabbit model. J. Orthop. Res. 1997, 15, 919–926. [Google Scholar] [CrossRef]
- Zwierzchowski, T.J.; Janus, J.; Konecki, W.; Kubiak, G.; Fabiś, J. The quantitative evaluation of the impact of viable medial meniscus graft type on the biochemical and biomechanical properties of the rabbit tibial cartilage. J. Orthop. Surg. Res. 2015, 10, 170. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Zeng, N.; Yan, Z.P.; Li, J.T.; Ni, G.X. Post-traumatic osteoarthritis following ACL injury. Arthritis Res. Ther. 2020, 22, 57. [Google Scholar] [CrossRef]
- Tsoukas, D.; Fotopoulos, V.; Basdekis, G.; Makridis, K.G. No difference in osteoarthritis after surgical and non-surgical treatment of ACL-injured knees after 10 years. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2953–2959. [Google Scholar] [CrossRef]
- Kessler, M.A.; Behrend, H.; Henz, S.; Stutz, G.; Rukavina, A.; Kuster, M.S. Function, osteoarthritis and activity after ACL-rupture: 11 years follow-up results of conservative versus reconstructive treatment. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 442–448. [Google Scholar] [CrossRef]
- Delincé, P.; Ghafil, D. Anterior cruciate ligament tears: Conservative or surgical treatment? A critical review of the literature. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 48–61. [Google Scholar] [CrossRef]
- Van Yperen, D.T.; Reijman, M.; van Es, E.M.; Bierma-Zeinstra, S.M.A.; Meuffels, D.E. Twenty-Year Follow-up Study Comparing Operative Versus Nonoperative Treatment of Anterior Cruciate Ligament Ruptures in High-Level Athletes. Am. J. Sports Med. 2018, 46, 1129–1136. [Google Scholar] [CrossRef]
- Schub, D.L.; Schmitz, L.M.; Sakamoto, F.A.; Winalski, C.S.; Parker, R.D. Long-term outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. Am. J. Sports Med. 2012, 40, 2764–2770. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lee, Y.H.; Siebold, R. Recommendations for the management of septic arthritis after ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2136–2144. [Google Scholar] [CrossRef] [PubMed]
- Kubiak, G.; Fabiś, J. Evaluation of treatment strategy of acute knee infection after ACL reconstruction with hamstring. Pol. Orthop. Traumatol. 2013, 78, 235–238. [Google Scholar] [PubMed]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 1982, 10, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Guermazi, A.; Roemer, F.W.; Haugen, I.K.; Crema, M.D.; Hayashi, D. MRI-based semiquantitative scoring of joint pathology in osteoarthritis. Nat. Rev. Rheumatol. 2013, 9, 236–251. [Google Scholar] [CrossRef]
- Li, G.; Park, S.E.; De Frate, L.E.; Schutzer, M.E.; Ji, L.; Gill, T.J.; Rubash, H.E. The cartilage thickness distribution in the tibiofemoral joint and its correlation with cartilage-to-cartilage contact. Clin. Biomech. 2005, 20, 736–744. [Google Scholar] [CrossRef]
- Mittal, S.; Pradhan, G.; Singh, S.; Batra, R. T1 and T2 mapping of articular cartilage and menisci in early osteoarthritis of the knee using 3-Tesla magnetic resonance imaging. Pol. J. Radiol. 2019, 8, 549–564. [Google Scholar] [CrossRef]
- Peterfy, C.G.; Guermazi, A.; Zaim, S.; Tirman, P.F.; Miaux, Y.; White, D.; Kothari, M.; Lu, Y.; Fye, K.; Zhao, S.; et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthr. Cartil. 2004, 12, 177–190. [Google Scholar] [CrossRef]
- Mühlbauer, R.; Lukasz, T.S.; Faber, T.S.; Stammberger, T.; Eckstein, F. Comparison of knee joint cartilage thickness in triathletes and physically inactive volunteers based on magnetic resonance imaging and three-dimensional analysis. Am. J. Sports Med. 2000, 28, 541–546. [Google Scholar] [CrossRef]
- Leiter, J.R.; Gourlay, R.; McRae, S.; de Korompay, N.; MacDonald, P.B. Long-term follow-up of ACL reconstruction with hamstring autograft. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1061–1069. [Google Scholar] [CrossRef]
- Boström Windhamre, H.; Mikkelsen, C.; Forssblad, M.; Willberg, L. Postoperative septic arthritis after anterior cruciate ligament reconstruction: Does it affect the outcome? A retrospective controlled study. Arthroscopy 2014, 30, 1100–1109. [Google Scholar] [CrossRef]
- McAllister, D.R.; Parker, R.D.; Cooper, A.E.; Recht, M.P.; Abate, J. Outcomes of postoperative septic arthritis after anterior cruciate ligament reconstruction. Am. J. Sports Med. 1999, 27, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Wipfler, B.; Donner, S.; Zechmann, C.M.; Springer, J.; Siebold, R.; Paessler, H.H. Anterior cruciate ligament reconstruction using patellar tendon versus hamstring tendon: A prospective comparative study with 9-year follow-up. Arthroscopy 2011, 27, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Saper, M.; Stephenson, K.; Heisey, M. Arthroscopic irrigation and debridement in the treatment of septic arthritis after anterior cruciate ligament reconstruction. Arthroscopy 2014, 30, 747–754. [Google Scholar] [CrossRef]
- Banios, K.; Komnos, G.A.; Raoulis, V.; Bareka, M.; Chalatsis, G.; Hantes, M.E. Soaking of autografts with vancomycin is highly effective on preventing postoperative septic arthritis in patients undergoing ACL reconstruction with hamstrings autografts. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Zwierzchowski, T.J.; Stasikowska-Kanicka, O.; Janus, J.; Konecki, W.; Danilewicz, M.; Fabiś, J. Evidence for apoptosis, MMP-1, MMP-3 and TIMP-2 expression and their effect on the mechanical and biochemical properties of fresh viable knee medial meniscal allografts and autografts in the rabbit. Arch. Med. Sci. 2012, 8, 724–732. [Google Scholar] [CrossRef]
- Zwierzchowski, T.J.; Stasikowska-Kanicka, O.; Danilewicz, M.; Fabiś, J. Assessment of apoptosis and MMP-1, MMP-3 and TIMP-2 expression in tibial hyaline cartilage after viable medial meniscus transplantation in the rabbit. Arch. Med. Sci. 2012, 8, 1108–1114. [Google Scholar] [CrossRef]
- Torres-Claramunt, R.; Gelber, P.; Pelfort, X.; Hinarejos, P.; Leal-Blanquet, J.; Pérez-Prieto, D.; Monllau, J.C. Managing septic arthritis after knee ligament reconstruction. Int. Orthop. 2016, 40, 607–614. [Google Scholar] [CrossRef]
- Fabiś, J. The impact of a isokinetic training program on the peak torque of the quadriceps and knee flexors after anterior cruciate ligament reconstruction with hamstrings. Ortop. Traumatol. Rehabil. 2007, 9, 527–531. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | All | |
|---|---|---|---|---|---|---|
| Sex (M/F) | M | M | M | M | M | 5/0 |
| Hamstring tendon graft | Y | Y | Y | Y | Y | 5/5 |
| Concomitant meniscal injury | N | Y | N | N | Y | 2/5 |
| Meniscal repair | N | N | N | N | Y | 1/5 |
| First follow-up period (years) | 11.7 | 12.3 | 9.8 | 10.4 | 10.2 | 10.9 ± 0.94 |
| Second follow-up period (years) | 18.6 | 19.1 | 16.6 | 17.3 | 17.4 | 18.1 ± 0.94 |
| Time from initial operation to knee infection symptoms (days) | 7 | 9 | 12 | 6 | 6 | 8 ± 2.27 |
| Time from knee infection symptoms to treatment (days) | 1 | 1 | 2 | 1 | 1 | 1.2 ± 0.4 |
| ACL graft retention | Y | Y | Y | Y | Y | 5/5 |
| C-reactive protein level in time of admission to hospital (mg/L) | 68.5 | 51.4 | 53.8 | 126.3 | 62.5 | 72.5 ± 27.59 |
| Time of C-reactive protein level normalization (days) < 5 mg/L | 9 | 8 | 7 | 12 | 9 | 9 ± 1.66 |
| Time of intravenous antibiotic treatment (days) | 16 | 15 | 14 | 21 | 15 | 16.2 ± 2.47 |
| FU | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | All (n = 5) * | |
|---|---|---|---|---|---|---|---|
| Lysholm score | I | 90 | 91 | 90 | 95 | 85 | 90.2 ± 3.19 |
| II | 92 | 91 | 91 | 94 | 89 | 91.4 ± 1.61 | |
| Single-leg hop test | I | 92 | 82 | 101 | 89 | 105 | 93.8 ± 8.27 |
| II | 87.5 | 82.5 | 99.5 | 86.5 | 101.5 | 91.5 ± 7.55 | |
| KT-1000 (side-to-side difference) | I | 1.8 | 1.7 | 3.7 | 0 | 4.6 | 2.36 ± 1.61 |
| II | 3.0 | 0.5 | 4.0 | 0 | 4.7 | 2.44 ± 1.86 |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | ||
|---|---|---|---|---|---|---|
| Gait distribution [%] | S | 49 | 50 | 50 | 50 | 51 |
| C | 51 | 50 | 50 | 50 | 49 | |
| Standing [%] | S | 0 | 100 | 82.7 | 53 | 0 |
| C | 100 | 0 | 17.2 | 47 | 100 | |
| PT-60 [Nm] | Q | 42.4 | 19.4 | 8.1 | 23.1 | 17.8 |
| H | 1.3 | −29.7 | −10.8 | 11.2 | 6.5 | |
| PT-180 [Nm] | Q | 29.8 | 8.2 | −1.3 | 19.4 | 14,3 |
| H | 6.4 | −8.3 | 2 | 10.5 | −3.2 | |
| PT/BW [Nm/kg] | 60° | 118.0 | 113.1 | 146.2 | 136.7 | 126.4 |
| H/Q [Nm] | 60° | 48.8 | 55.1 | 67.5 | 53.1 | 57.3 |
| 180° | 47.8 | 51.1 | 60.7 | 49.5 | 52.6 | |
| Time to PT-60 [ms] | S | 440 | 670 | 410 | 520 | 720 |
| C | 540 | 800 | 670 | 660 | 850 | |
| Time to PT-180 [ms] | S | 230 | 220 | 280 | 240 | 290 |
| C | 270 | 200 | 250 | 190 | 310 | |
| Angle to PT-60 [deg.] | S | 74 | 76 | 83 | 79 | 81 |
| C | 68 | 59 | 68 | 64 | 63 | |
| Angle to PT-180 [deg.] | S | 70 | 83 | 66 | 65 | 72 |
| C | 63 | 61 | 69 | 71 | 65 | |
| Work fatigue-60 | S | 12.6 | 5.6 | −1.0 | −10.3 | 14.5 |
| C | 12 | −15.6 | 2.8 | −6.4 | 9.3 | |
| Work fatigue-180 | S | 26.6 | 40.2 | 15.5 | 27.1 | 32.4 |
| C | 32 | 23.5 | 24.2 | 19.4 | 20.3 | |
| Knee Cartilage Thickness [mm] | |||||||
|---|---|---|---|---|---|---|---|
| Condyle | FU | Group | Av | Min | Max | SD | p-Value |
| LFC | 10.8-years | SG | 2.165 | 0.92 | 3.71 | 0.77 | 0.1 * |
| CG | 2.332 | 0.87 | 4.71 | 0.805 | |||
| 18.1-years | SG | 2.217 | 0.63 | 3.99 | 0.725 | 0.043 ** | |
| CG | 2.43 | 0.58 | 4.9 | 0.87 | |||
| LTC | 10.8-years | SG | 3.18 | 0.99 | 6.05 | 0.92 | 0.414 * |
| CG | 3.126 | 1.26 | 6.1 | 1.03 | |||
| 18.1-years | SG | 3.076 | 1.32 | 4.76 | 0.831 | 0.131 * | |
| CG | 2.94 | 1.37 | 5.15 | 0.887 | |||
| MFC | 10.8-years | SG | 2.077 | 0.94 | 3.55 | 0.59 | 0.021 * |
| CG | 2.237 | 0.87 | 3.37 | 0.61 | |||
| 18.1-years | SG | 2.158 | 0.93 | 3.38 | 0.561 | 0.185 * | |
| CG | 2.073 | 0.82 | 3.25 | 0.564 | |||
| MTC | 10.8-years | SG | 2.478 | 1.42 | 4.98 | 0.77 | 0.008 * |
| CG | 2.24 | 1.06 | 4.15 | 0.703 | |||
| 18.1-years | SG | 2.38 | 1,29 | 4.5 | 0.68 | 0.434 * | |
| CG | 2.32 | 1.22 | 3.94 | 0.696 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waszczykowski, M.; Fabiś-Strobin, A.; Korczyc-Stępnicka, A.; Małecki, K.; Białecki, J.; Bartosz, P.; Fabiś, J. The Speed of Pathogen Eradication May Prevent the Early Development of Cartilage Destruction: Case Series of Long-Term Follow-Up of Septic Arthritis (SA) after Anterior Cruciate Ligament Reconstruction (ACL-R) and Literature Review. Appl. Sci. 2022, 12, 11679. https://doi.org/10.3390/app122211679
Waszczykowski M, Fabiś-Strobin A, Korczyc-Stępnicka A, Małecki K, Białecki J, Bartosz P, Fabiś J. The Speed of Pathogen Eradication May Prevent the Early Development of Cartilage Destruction: Case Series of Long-Term Follow-Up of Septic Arthritis (SA) after Anterior Cruciate Ligament Reconstruction (ACL-R) and Literature Review. Applied Sciences. 2022; 12(22):11679. https://doi.org/10.3390/app122211679
Chicago/Turabian StyleWaszczykowski, Michał, Anna Fabiś-Strobin, Agnieszka Korczyc-Stępnicka, Krzysztof Małecki, Jerzy Białecki, Paweł Bartosz, and Jarosław Fabiś. 2022. "The Speed of Pathogen Eradication May Prevent the Early Development of Cartilage Destruction: Case Series of Long-Term Follow-Up of Septic Arthritis (SA) after Anterior Cruciate Ligament Reconstruction (ACL-R) and Literature Review" Applied Sciences 12, no. 22: 11679. https://doi.org/10.3390/app122211679
APA StyleWaszczykowski, M., Fabiś-Strobin, A., Korczyc-Stępnicka, A., Małecki, K., Białecki, J., Bartosz, P., & Fabiś, J. (2022). The Speed of Pathogen Eradication May Prevent the Early Development of Cartilage Destruction: Case Series of Long-Term Follow-Up of Septic Arthritis (SA) after Anterior Cruciate Ligament Reconstruction (ACL-R) and Literature Review. Applied Sciences, 12(22), 11679. https://doi.org/10.3390/app122211679