1. Introduction
The general concept of remote rehabilitation using motion capture (MoCap) systems has undergone a turbulent change in recent years, as there are several tools for three-dimensional assessments, including sophisticated automation technologies and algorithms, often costing time, expensive equipment and inapplicable inconvenience to the daily practice [
1]. Telerehabilitation, or remote physical therapy, is one of the most common types of complex distance medicine that is applied in practice [
2]. During recent years, a large number of MoCap systems detecting the pose of a human using a “markerless” approach have emerged [
3], these systems work without the necessity of placement of any markers on the human body [
4].
This approach reduces the technical and financial requirements and complexity of arrangement [
5] and therefore it can be found in the context of distance medicine, not only in specialized clinics but also in the home environment [
6].
Considering the application of distance medicine in the home environment, the most promising systems seem to be systems for the evaluation of body movements from commonly used standard video (RGB) records [
7].
In this case, we only need a regular camera, which is currently integrated into most common electronic devices, such as smartphones or laptops, or smart TVs.
These systems have great potential for use mainly due to the reduced financial costs of purchasing these systems. These systems have reached such technical levels that they could be used in specific cases as alternatives to costly systems in clinics. However, these systems must also use special camera data processing software [
8].
The most commonly used software tools for pose detection are OpenPose [
9], Mask R-CNN [
10], Google’s Media Pipe [
11], Alpha-Pose [
12] all available as open source.
The time to the advent of markerless-based systems using neural networks is described in detail in Coyer’s review [
13]. All the systems mentioned above were operated only under laboratory conditions or used special HW.
All these software tools use artificial intelligence methods, namely neural networks (NN) trained on annotated images [
14]. The datasets contain general static images of people in undefined positions, according to which NN learns to recognize anatomical points on the body. Existing benchmarks compare the speed and accuracy of detection using the above algorithms based on NN [
14]. A shortcoming that limits wider use of low-cost MoCap systems and the mentioned software is the absence of evaluation of the validity of the data provided by these systems. This raises doubts about the use of telemedicine where it is necessary to know relatively accurately the information about the movement of specific anatomical points that physiotherapists need to monitor and modulate the rehabilitation intervention [
15]. Thus, the main aim of our study is to determine whether the systems are sufficient to be used for home rehabilitation and under what specific conditions. We focus on the evaluation of the motion capture of different exercise positions and by different camera views, i.e., camera position relative to the subject. To achieve this aim, it is not possible to rely on existing benchmarks, but it is necessary to evaluate the efficiency of software use on video recordings of people moving while exercising. Thus, our study aims to validate the application of markerless systems using only one, generally positioned camera and thus applicable to home telerehabilitation.
2. Methods
2.1. Design
The advantage of the camera-based approach is the ability to detect motion from any regular RGB video. This allows to use existing recordings and perform a large-scale evaluation. In this study, we choose to use the database created by PhysioTools. PhysioTools is one of the world’s most comprehensive exercise libraries [
21]. In our study, we consider only the ability of the system to estimate the human pose. We do not analyze the exercise itself. Therefore, we only extract the OpenPose reported confidence of the selected keypoints to infer the quality of detection. The design of our study is shown in
Figure 1.
For research purposes, we use a database based on an agreed template of commonly prescribed physical exercises printed from commonly used PhysioTools computer software (PhysioTools©, Product ID RG-PT1ENG, General Exercises Second Edition (English), Tampere, 339 Finland) [
22]. PhysioTools is a database of professional trainers and serves as a video aid for exercises in the home environment. The average length of a video is 20 s. Videos have frame rates ranging from 25 fps to 50 fps, resolutions ranging from 0.1–0.6 Mpixel, and bit rate greater than 200 kbs. Our aim is to evaluate practical usability of recordings made in an uncontrolled home environment so we use no additional constraints on video quality.
Unlike typical studies [
23] studying only one type of movement, the database we used is composed of hundreds of unique physical exercises, see
Table 1 for quantity and
Table 2 for categories.An exercise can be included in the database if it is performed by a single person and shows their whole body. Each video was manually checked to confirm that the entire trainee’s body was in view throughout the recording. At the same time, manual categorization into specific groups was done by a single rater. Border cases were excluded from the analysis.
2.2. Video Analysis
Since the practical use assumes only one camera, we were interested in the influence of the orientation of the person towards the camera.
By analyzing the database, we determined the following three basic views to be the most common: the frontal view (frontal plane), the side view (sagittal plane), and the ¾ view, which is in between these planes, please see
Figure 2. Although the ¾ plane is not biomechanically defined, it was most frequently used in instructional videos, because it provides an overview of the entire body and a better spatial understanding of records.
2.3. Keypoint Confidence Extraction
The videos were analyzed using the OpenPose [
25] algorithm. OpenPose uses a model with 25 keypoints. In the context of performing rehabilitation exercises, the body segments that are part of the appendicular skeleton are very often measured [
26]. These segments allow for translational movement of the body through cyclic movements such as walking [
27]. Thus, we used 12 points that allow us to determine the positions and orientations of segments of the appendicular skeleton for further analysis. These 12 points are described in
Table 3.
The outputs of OpenPose for each frame are the x,y coordinate values and the detection confidence for each of the 25 model points, please see
Figure 3. From this information, we use only the confidence for the twelve points for each frame. This gives us 12 temporal signals for each unique video.
OpenPose processes each frame independently without using the time context. Repeated image analysis returns the same results. OpenPose has almost perfect test–retest reliability within device [
8].
In our study, we are not dealing with the absolute position of the detected points. To evaluate the quality of detection, we use directly the confidence returned by OpenPose. Thus, we are not evaluating the accuracy of detection, but the detection capability itself.
Detection accuracy using annotated images is a classical metric for comparing machine learning algorithms; accuracy calculations are performed on large image datasets COCO [
28], MPII [
29]. In contrast, the evaluation of dynamic events has been studied only for single exercises and sub-joints [
23]. Existing annotated 2D datasets deal with either images [
30] or deal with a small variety of activities [
31,
32].
In contrast to the above-mentioned studies, we deal with many unique rehabilitation exercises.
OpenPose returns the confidence values of the keypoints in the interval of <0, 1>. Points that are not detected have a confidence value of zero. The confidence value is rarely used in single-camera setups because the position of the detected joints is accurate even with an average confidence value. On the other hand, in multi camera setup and 3D reconstruction tasks, which are very sensitive to misclassification, the confidence is used to weight joint positions [
33] or to discard joints with a low confidence value, as the misclassification of points appears with values below 0.2 [
34].
The result of the processed video is a matrix of 12 keypoint confidences in time.
2.4. Statistical Analysis
To compare the records, we calculated the medians of each time signal. This gave us 12 scalar keypoint confidence values defining each video. All records were assigned to exactly one of the subgroups, see
Table 1. For each subcategory, we calculated the median confidence of the individual keypoints.
To visualize the results we chose box plots where outliers are not shown for clarity. We define outliers as elements more than 1.5 interquartile ranges above the upper quartile (75 percent) or below the lower quartile (25 percent).
The Kruskal–Wallis test was used to determine the statistical significance of group differences. Due to a large amount of data and the significant difference of one of the groups, all results were significant. Therefore, we decided to compare all groups, individually, with each other. To verify the normality of the data we used the Shapiro–Wilks test. The test has shown that values in the groups are not normally distributed. The groups also varied in size, see
Table 1, therefore we used the Wilcoxon test to determine the statistical significance of the difference between the categories. All statistical calculations were performed using the Matlab (MATLAB and Statistics Toolbox Release 2019b, The MathWorks, Inc., Natick, MA, USA).
3. Results
In our study, we analyzed a total of 2133 videos. Each video shows only one trainee performing a unique exercise. Each video belonged to one of the “Camera View” and one of the “Starting position” groups. We present the results of our findings using OpenPose reported confidence values. We can use the confidence returned by the OpenPose algorithm as a measure of detection quality because it correlates with the percentage of correct keypoints metric [
35].
The resulting median confidences for each joint and each category are shown in
Table 4. Keypoints with a confidence value above 0.5 can be considered correctly detected [
35]. These confidence values are associated with with clearly visible body parts [
9].
Due to the large amount of data in the groups, the differences in confidence between groups are largely significant, although small in absolute terms. Therefore, for clarity, only differences that were not statistically significant (n.s.) are highlighted in the following boxplots. All the other differences were statistically significant, see
Table A1 and
Table A2 in the
Appendix A. Box-and-whisker plots of detection confidence for all the categories are show in
Figure 4,
Figure 5,
Figure 6,
Figure 7,
Figure 8 and
Figure 9.
When interpreting the plots, it is important to note that the confidence correlates nonlinearly with the detection accuracy. If all keypoints in the image are clearly visible and accurately detected, confidence values in the range of 0.7–0.9 are commonly obtained. From a practical perspective of a single camera-based recording, the differences in accuracy associated with this range of confidences are not relevant. Even points with a confidence value above 0.5 can be considered correctly detected [
9]. Lower confidence values are also associated with high-frequency keypoint jitter [
36], but this effect can be easily filtered out because the body movements during rehabilitation exercises are slow relative to the sampling rate of the camera. False-positive detections or swapped keypoints can only be expected for low confidence values around 0.2 [
34]. Small confidence values (0.1) are associated with guessed and occluded keypoints; the smaller the value, the more false positives detections are likely [
9].
To summarize, as long as the value of the lower quartile is above 0.5, we can say that the combination of body position and camera view is practically usable.
Interestingly we can see the differences between upper body points and lower body points. Upper body detection performs better for all camera views.
Non-significant differences in confidence are often found with standing and sitting positions, which is due to the fact that detection works very well.
If the value of the lower quartile of confidence is less than 0.5, it is likely that the detection will not work in all cases.
In all boxplots, we can observe an increasing tendency of confidence values between the groups of starting positions. The worst confidences are achieved by lying down (red), followed by on the knees (brown), and the best results are achieved by exercises performed in sitting (green) and standing (blue).
In the boxplots, the black line represents the groups that have no significant differences between them. These are mostly groups of exercises in sitting and standing positions. Thus, we can say that the detection is very reliable in both these groups and there are no significant differences between these groups. The achieved results clearly show that there are significant differences with respect to starting position.
4. Discussion
The main objective of our research was to determine the usability of a camera-based system in a home environment. Since human position detection is captured by only one RGB camera, we were mainly interested in the influence of camera view and the position of the trainee, where we expected the greatest impact on the detection of keypoints. The quality of detection was determined by the confidence of detection of each keypoint.
Our main findings are the following: regardless of the camera view, the lying position comes out as the least detectable, followed by the position on the knees. The standing position is the most efficient, but the absolute differences against the sitting position are small. In the case of the camera view, the results were not so convincing. For the lying position and the position on the knees, the differences are not statistically significant in most cases, but no conclusions can be drawn because of the large variances.
For standing and sitting positions, the camera view from the side is a bit worse. From the data we have available, it is not possible to give a clear answer to the question of whether the confidences for the different camera views differ.
We also found out the difference in confidence between upper-body and lower-body keypoints. Confidence of lower-body keypoints is generally lower. This can be explained by the fact that the positions of the upper limbs are more variable than the position of the lower limbs. Generally speaking, joint positions are easier to establish if they are at an angle other than 180 degrees, which is typically the angle of the knee. The hips are not as visible as the shoulders and the ankles are often covered by shoes and trousers, while the position of the wrist can be very easily derived from the palm of the hand.
We can justify generalizing the results about views and postures given the high number of unique exercises, as opposed to works focusing on specific exercises, where only a few different types of exercises are involved.
Before applying the research results in practice, it is important to define several assumptions and limitations. They are closely linked to the application area of telerehabilitation in home settings. The first assumption and limitation at the same time is the use of a single simple camera (smart phone, tablet). The second assumption is the application use by nontechnical users that results in the requirement of simple control and setup of the application. These considerations led us to experiments analyzing the influence of the body position in relation to the camera and evaluation of many different exercises recorded by a single camera.
In the light of these facts, we are well aware of the limitations of the proposed approach, in particular the precise identification of certain motions in the front or side view. For example, abduction of the right arm cannot be well recognized in the side view from the left side, the range of straddling backward or angle of the knee cannot be precisely identified in frontal view.
For practical usability, it is important that there are not too many dropouts, i.e., that the joints are detected, and that they are not mistaken with another part of the body, e.g., the left and right limbs are swapped when viewed from the side, and so on. Another important aspect of the evaluation is that each individual exercise engages different parts of the body, thus only certain points are important for the analysis of the given exercise. The camera view is chosen so that the parts of the body being exercised are clearly visible while at the same time some parts of the body can be obscured. With the side camera view, the other side is often not visible.
Therefore, it can be assumed that points with a lower confidence value do not play a large role in the exercise. Just the fact that low confidences are found for individual joints does not necessarily mean that the exercise cannot be successfully evaluated. This is also the reason why we decided to present the results of individual joints and not evaluate the confidence of the whole exercise.
5. Conclusions
Despite the fact that there have been many recent publications describing the possibility of using a camera-based system for home rehabilitation, there has been no work to date that has validated the detection capability on a large dataset consisting specifically of videos of people performing rehabilitation exercises in front of a camera.
We validated the ability of the OpenPose algorithm to detect the keypoints of the human skeleton on more than two thousand videos of people performing rehabilitation exercises.
Based on our findings, we can say that OpenPose, for detection, is a sufficiently robust algorithm that is capable of detecting people during commonly performed exercises in a home environment. Only exercises performed in the lying and on-the-knees positions may not always be correctly detected. In this study, we also analyzed closely the basic landmarks of the human skeleton, see
Table 3 and gave a summary of which keypoints are more reliably detectable. In that way, we provided an identification of the important points on the skeleton for each exercise, and, thus, offered a practical overview for designers of future camera-based telerehabilitation systems.
Author Contributions
Conceptualization, J.D. and J.A.; methodology, P.K.; software, J.A.; validation, J.A., L.L. and J.H.; formal analysis, P.K., J.H.; investigation, J.H.; resources, J.A.; data curation, J.A., J.H.; writing—original draft preparation, J.A., J.D.; writing—review and editing, L.L.; visualization, J.A.; supervision, L.L.; project administration, P.K.; funding acquisition, P.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a grant from the Ministry of Science & Technology, Israel and The Ministry of Education, Youth and Sports of the Czech Republic. The described research was supported by the project No. LTAIZ19008 Enhancing Robotic Physiotherapeutic Treatment using Machine Learning awarded in frame of the Czech–Israeli cooperative scientific research program (Inter-Excellence MEYS CR and MOST Israel).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
For research purposes, we only used body keypoints extraction, but did not store the videos themselves for future use. The videos are available on the Physiotools website [
21]. Our statistical data are available along with our research.
Conflicts of Interest
The author declares no conflict of interest.
Appendix A
Table A1.
Camera view, p-values of comparison of starting positions. Ly—Lying; Kn—on the knees; St—standing; Si—sitting. The bold values show non-significant values.
Table A1.
Camera view, p-values of comparison of starting positions. Ly—Lying; Kn—on the knees; St—standing; Si—sitting. The bold values show non-significant values.
| No. | Ly X Kn | Ly X Si | Ly X St | Si X Kn | St X Kn | St X Si |
|---|
| Camera View FRONT |
| Upper Body |
| 2 | 0.68 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 3 | 0.07 | <0.01 | <0.01 | <0.01 | <0.01 | 0.05 |
| 4 | 0.07 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 5 | 0.29 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 6 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 7 | <0.01 | <0.01 | <0.01 | 0.58 | <0.01 | <0.01 |
| Lower Body |
| 9 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.44 |
| 10 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.95 |
| 11 | 0.05 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 12 | 0.18 | <0.01 | <0.01 | <0.01 | <0.01 | 0.33 |
| 13 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.97 |
| 14 | 0.42 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| Camera View ¾ |
| Upper Body |
| 2 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 3 | <0.01 | <0.01 | <0.01 | 0.18 | <0.01 | <0.01 |
| 4 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.13 |
| 5 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.56 |
| 6 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 7 | <0.01 | <0.01 | <0.01 | 0.45 | 0.21 | <0.01 |
| Lower Body |
| 9 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.22 |
| 10 | <0.01 | <0.01 | <0.01 | <0.01 | 0.18 | <0.01 |
| 11 | <0.01 | <0.01 | <0.01 | 0.32 | <0.01 | <0.01 |
| 12 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.15 |
| 13 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 14 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| Camera View SIDE |
| Upper Body |
| 2 | 0.96 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 3 | <0.01 | <0.01 | <0.01 | 0.38 | 0.13 | <0.01 |
| 4 | <0.01 | <0.01 | <0.01 | 1.00 | <0.01 | 0.07 |
| 5 | 0.16 | <0.01 | <0.01 | <0.01 | <0.01 | 0.37 |
| 6 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.51 |
| 7 | <0.01 | <0.01 | <0.01 | 0.29 | 0.07 | 0.36 |
| Lower Body |
| 9 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 10 | <0.01 | <0.01 | <0.01 | 0.46 | 0.23 | 0.85 |
| 11 | <0.01 | <0.01 | <0.01 | 0.22 | <0.01 | <0.01 |
| 12 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| 13 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | 0.54 |
| 14 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
Table A2.
Starting position, p-values of comparison of starting positions. Fr—front view; Sid—side view; ¾—¾ view.
Table A2.
Starting position, p-values of comparison of starting positions. Fr—front view; Sid—side view; ¾—¾ view.
| | Lying | On the Knees |
|---|
| | Fr X ¾ | Fr X Sid | ¾ X Sid | Fr X ¾ | Fr X Sid | ¾ X Sid |
| Upper Body |
| 2 | 0.18 | 0.34 | <0.01 | 0.65 | 0.47 | 0.84 |
| 3 | 0.92 | 0.43 | 0.31 | 0.36 | 0.16 | 0.46 |
| 4 | 0.78 | <0.01 | <0.01 | 0.11 | <0.01 | 0.55 |
| 5 | 0.34 | 0.40 | 0.82 | 0.59 | 0.45 | <0.01 |
| 6 | 0.72 | 0.48 | 0.12 | 0.77 | 0.13 | <0.01 |
| 7 | 0.85 | 0.67 | 0.31 | 0.33 | 0.65 | 0.05 |
| Lower Body |
| 9 | 0.14 | 0.83 | 0.08 | 0.31 | 0.80 | 0.29 |
| 10 | 0.72 | 0.50 | 0.16 | 0.08 | 0.15 | 0.56 |
| 11 | 0.78 | 0.27 | 0.23 | <0.01 | 0.19 | 0.12 |
| 12 | 0.21 | 0.29 | 0.81 | 0.54 | 0.52 | <0.01 |
| 13 | 0.66 | 0.54 | 0.15 | 0.58 | 0.49 | 0.08 |
| 14 | 0.96 | 0.85 | 0.57 | <0.01 | 0.63 | <0.01 |
| | Sitting | Standing |
| | Fr X ¾ | Fr X Sid | ¾ X Sid | Fr X ¾ | Fr X Sid | ¾ X Sid |
| | Fr X ¾ | Fr X Sid | ¾ X Sid | Fr X ¾ | Fr X Sid | ¾ X Sid |
| Upper Body |
| 2 | 0.57 | <0.01 | <0.01 | <0.01 | <0.01 | 0.07 |
| 3 | 0.69 | 0.16 | 0.15 | 0.81 | 0.16 | 0.14 |
| 4 | 0.74 | 0.23 | <0.01 | 0.12 | <0.01 | 0.14 |
| 5 | 0.09 | 0.18 | <0.01 | 0.35 | <0.01 | <0.01 |
| 6 | 0.29 | <0.01 | 0.18 | <0.01 | <0.01 | <0.01 |
| 7 | 0.93 | 0.49 | 0.38 | <0.01 | <0.01 | <0.01 |
| Lower Body |
| 9 | 0.50 | <0.01 | <0.01 | 0.42 | <0.01 | 0.09 |
| 10 | <0.01 | 0.19 | <0.01 | 0.11 | <0.01 | 0.17 |
| 11 | 0.28 | <0.01 | <0.01 | <0.01 | <0.01 | 0.12 |
| 12 | 0.51 | <0.01 | <0.01 | 0.08 | <0.01 | <0.01 |
| 13 | 0.12 | 0.40 | <0.01 | 0.11 | <0.01 | <0.01 |
| 14 | 0.92 | <0.01 | <0.01 | 0.29 | <0.01 | 0.08 |
References
- Demeco, A.; Marotta, N.; Moggio, L.; Pino, I.; Marinaro, C.; Barletta, M.; Petraroli, A.; Palumbo, A.; Ammendolia, A. Quantitative analysis of movements in facial nerve palsy with surface electromyography and kinematic analysis. J. Electromyogr. Kinesiol. 2021, 56, 102485. [Google Scholar] [CrossRef]
- Suso-Martí, L.; Touche, R.L.; Herranz-Gómez, A.; Angulo-Díaz-Parreño, S.; Paris-Alemany, A.; Cuenca-Martínez, F. Effectiveness of Telerehabilitation in Physical Therapist Practice: An Umbrella and Mapping Review With Meta–Meta-Analysis. Phys. Ther. 2021, 101, pzab053. [Google Scholar] [CrossRef]
- Desmarais, Y.; Mottet, D.; Slangen, P.; Montesinos, P. A review of 3D human pose estimation algorithms for markerless motion capture. arXiv 2020, arXiv:2010.06449. [Google Scholar] [CrossRef]
- Cotton, R.J. Kinematic Tracking of Rehabilitation Patients With Markerless Pose Estimation Fused with Wearable Inertial Sensors. In Proceedings of the 2020 15th IEEE International Conference on Automatic Face and Gesture Recognition (FG 2020), Buenos Aires, Argentina, 16–20 November 2020; pp. 508–514. [Google Scholar] [CrossRef]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef]
- Adolf, J.; Jaromir, D.; Kutilek, P.; Hourova, M.; Hejda, J.; Milerska, I.; Lhotska, L. Automatic Telerehabilitation System in a Home Environment Using Computer Vision. Stud. Health Technol. Inform. 2020, 273, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Farulla, G.A.; Pianu, D.; Cempini, M.; Cortese, M.; Russo, L.; Indaco, M.; Nerino, R.; Chimienti, A.; Oddo, C.; Vitiello, N. Vision-Based Pose Estimation for Robot-Mediated Hand Telerehabilitation. Sensors 2016, 16, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ota, M.; Tateuchi, H.; Hashiguchi, T.; Kato, T.; Ogino, Y.; Yamagata, M.; Ichihashi, N. Verification of reliability and validity of motion analysis systems during bilateral squat using human pose tracking algorithm. Gait Posture 2020, 80, 62–67. [Google Scholar] [CrossRef]
- Hidalgo, G.; Cao, Z.; Simon, T.; Wei, S.E.; Raaj, Y.; Joo, H.; Sheikh, Y. OpenPose Library, CMU-Perceptual-Computing-Lab. 2021. Available online: https://github.com/CMU-Perceptual-Computing-Lab/openpose (accessed on 10 October 2021).
- He, K.; Gkioxari, G.; Dollar, P.; Girshick, R. Mask R-CNN. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar] [CrossRef]
- Ahmadyan, A.; Hou, T.; Wei, J.; Zhang, L.; Ablavatski, A.; Grundmann, M. Instant 3D Object Tracking with Applications in Augmented Reality. arXiv 2020, arXiv:2006.13194. [Google Scholar]
- Fang, H.S.; Xie, S.; Tai, Y.W.; Lu, C. RMPE: Regional Multi-person Pose Estimation. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar] [CrossRef] [Green Version]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods Towards Developing a Markerless System. Sport. Med.-Open 2018, 4, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidziński, Ł.; Yang, B.; Hicks, J.L.; Rajagopal, A.; Delp, S.L.; Schwartz, M.H. Deep neural networks enable quantitative movement analysis using single-camera videos. Nat. Commun. 2020, 11, 4054. [Google Scholar] [CrossRef]
- Marotta, N.; Demeco, A.; Moggio, L.; Ammendolia, A. Why is telerehabilitation necessary? A pre-post COVID-19 comparative study of ICF activity and participation. J. Enabling Technol. 2021, 15, 117–121. [Google Scholar] [CrossRef]
- Chua, J.; Ong, L.Y.; Leow, M.C. Telehealth Using PoseNet-Based System for In-Home Rehabilitation. Future Internet 2021, 13, 173. [Google Scholar] [CrossRef]
- Hernández, Ó.G.; Morell, V.; Ramon, J.L.; Jara, C.A. Human Pose Detection for Robotic-Assisted and Rehabilitation Environments. Appl. Sci. 2021, 11, 4183. [Google Scholar] [CrossRef]
- Takeda, I.; Yamada, A.; Onodera, H. Artificial Intelligence-Assisted motion capture for medical applications: A comparative study between markerless and passive marker motion capture. Comput. Methods Biomech. Biomed. Eng. 2020, 24, 864–873. [Google Scholar] [CrossRef]
- Stenum, J.; Rossi, C.; Roemmich, R.T. Two-dimensional video-based analysis of human gait using pose estimation. PLoS Comput. Biol. 2021, 17, e1008935. [Google Scholar] [CrossRef] [PubMed]
- Nakano, N.; Sakura, T.; Ueda, K.; Omura, L.; Kimura, A.; Iino, Y.; Fukashiro, S.; Yoshioka, S. Evaluation of 3D Markerless Motion Capture Accuracy Using OpenPose With Multiple Video Cameras. Front. Sport. Act. Living 2020, 2, 50. [Google Scholar] [CrossRef] [PubMed]
- PhysioTools©. Product ID RG-PT1ENG. In General Exercises, 2nd ed.; PhysioTools©: Tampere, Finland. (In English)
- Hay, E.; Dziedzic, K.; Foster, N.; Peat, G.; van der Windt, D.; Bartlam, B.; Blagojevic-Bucknall, M.; Edwards, J.; Healey, E.; Holden, M.; et al. Optimal primary care management of clinical osteoarthritis and joint pain in older people: A mixed-methods programme of systematic reviews, observational and qualitative studies, and randomised controlled trials. Programme Grants Appl. Res. 2018, 6, 1–260. [Google Scholar] [CrossRef]
- Badiola-Bengoa, A.; Mendez-Zorrilla, A. A Systematic Review of the Application of Camera-Based Human Pose Estimation in the Field of Sport and Physical Exercise. Sensors 2021, 21, 5996. [Google Scholar] [CrossRef]
- Anatomical Planes. Available online: https://teachmeanatomy.info/the-basics/anatomical-terminology/planes/ (accessed on 3 November 2021).
- Cao, Z.; Simon, T.; Wei, S.E.; Sheikh, Y. Realtime Multi-Person 2D Pose Estimation using Part Affinity Fields. In Proceedings of the Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–28 July 2017. [Google Scholar]
- Stirling, D.; Hesami, A.; Ritz, C.; Adistambha, K.; Naghdy, F. Symbolic Modelling of Dynamic Human Motions; InTech: Rijeka, Croatia, 2010. [Google Scholar] [CrossRef] [Green Version]
- Karatsidis, A.; Jung, M.; Schepers, H.M.; Bellusci, G.; de Zee, M.; Veltink, P.H.; Andersen, M.S. Musculoskeletal model-based inverse dynamic analysis under ambulatory conditions using inertial motion capture. Med. Eng. Phys. 2019, 65, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.Y.; Maire, M.; Belongie, S.; Bourdev, L.; Girshick, R.; Hays, J.; Perona, P.; Ramanan, D.; Zitnick, C.L.; Dollár, P. Microsoft COCO: Common Objects in Context. arXiv 2014, arXiv:1405.0312. [Google Scholar]
- Andriluka, M.; Pishchulin, L.; Gehler, P.; Schiele, B. 2D Human Pose Estimation: New Benchmark and State of the Art Analysis. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Columbus, OH, USA, 23–28 June 2014. [Google Scholar]
- Johnson, S.; Everingham, M. Learning Effective Human Pose Estimation from Inaccurate Annotation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Colorado Springs, CO, USA, 20–25 June 2011. [Google Scholar]
- Zhang, W.; Zhu, M.; Derpanis, K.G. From Actemes to Action: A Strongly-Supervised Representation for Detailed Action Understanding. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Sydney, Australia, 1–8 December 2013. [Google Scholar] [CrossRef]
- Kazemi, V.; Sullivan, J. Using Richer Models for Articulated Pose Estimation of Footballers. In Proceedings of the BMVC, Surrey, UK, 3–7 September 2012. [Google Scholar]
- Garcia-Salguero, M.; Gonzalez-Jimenez, J.; Moreno, F.A. Human 3D Pose Estimation with a Tilting Camera for Social Mobile Robot Interaction. Sensors 2019, 19, 4943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slembrouck, M.; Luong, H.; Gerlo, J.; Schütte, K.; Cauwelaert, D.V.; Clercq, D.D.; Vanwanseele, B.; Veelaert, P.; Philips, W. Multiview 3D Markerless Human Pose Estimation from OpenPose Skeletons; Springer International Publishing: Cham, Switzerland, 2020; pp. 166–178. [Google Scholar] [CrossRef]
- Ng, K.D.; Mehdizadeh, S.; Iaboni, A.; Mansfield, A.; Flint, A.; Taati, B. Measuring Gait Variables Using Computer Vision to Assess Mobility and Fall Risk in Older Adults With Dementia. IEEE J. Transl. Eng. Health Med. 2020, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Needham, L.; Evans, M.; Cosker, D.P.; Colyer, S.L. Can Markerless Pose Estimation Algorithms Estimate 3D Mass Centre Positions and Velocities during Linear Sprinting Activities? Sensors 2021, 21, 2889. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study design—diagram explaining the sequence of steps.
Figure 1.
Study design—diagram explaining the sequence of steps.
Figure 2.
Orientation of the camera relative to the subject. Camera view options: front, ¾ and side [
24].
Figure 2.
Orientation of the camera relative to the subject. Camera view options: front, ¾ and side [
24].
Figure 3.
OpenPose 25 keypoints model [
9].
Figure 3.
OpenPose 25 keypoints model [
9].
Figure 4.
Confidence of detection of selected KP (keypoints)—front view, upper body. Camera views are shown in colour as follows: lying down (N = 75); on the knees (N = 26); sitting (N = 186); and standing (N = 70). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 4.
Confidence of detection of selected KP (keypoints)—front view, upper body. Camera views are shown in colour as follows: lying down (N = 75); on the knees (N = 26); sitting (N = 186); and standing (N = 70). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 5.
Confidence of detection of selected KP (keypoints)—front view, lower body. Camera views are shown in colour as follows: lying down (N = 75), on the knees (N = 26), sitting (N = 186) and standing (N = 70). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 5.
Confidence of detection of selected KP (keypoints)—front view, lower body. Camera views are shown in colour as follows: lying down (N = 75), on the knees (N = 26), sitting (N = 186) and standing (N = 70). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 6.
Confidence of detection of selected KP (keypoints)—¾ view, upper body. Camera views are shown in colour as follows: lying down (N = 177); on the knees (N = 95); sitting (N = 165); and standing (N = 490). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 6.
Confidence of detection of selected KP (keypoints)—¾ view, upper body. Camera views are shown in colour as follows: lying down (N = 177); on the knees (N = 95); sitting (N = 165); and standing (N = 490). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
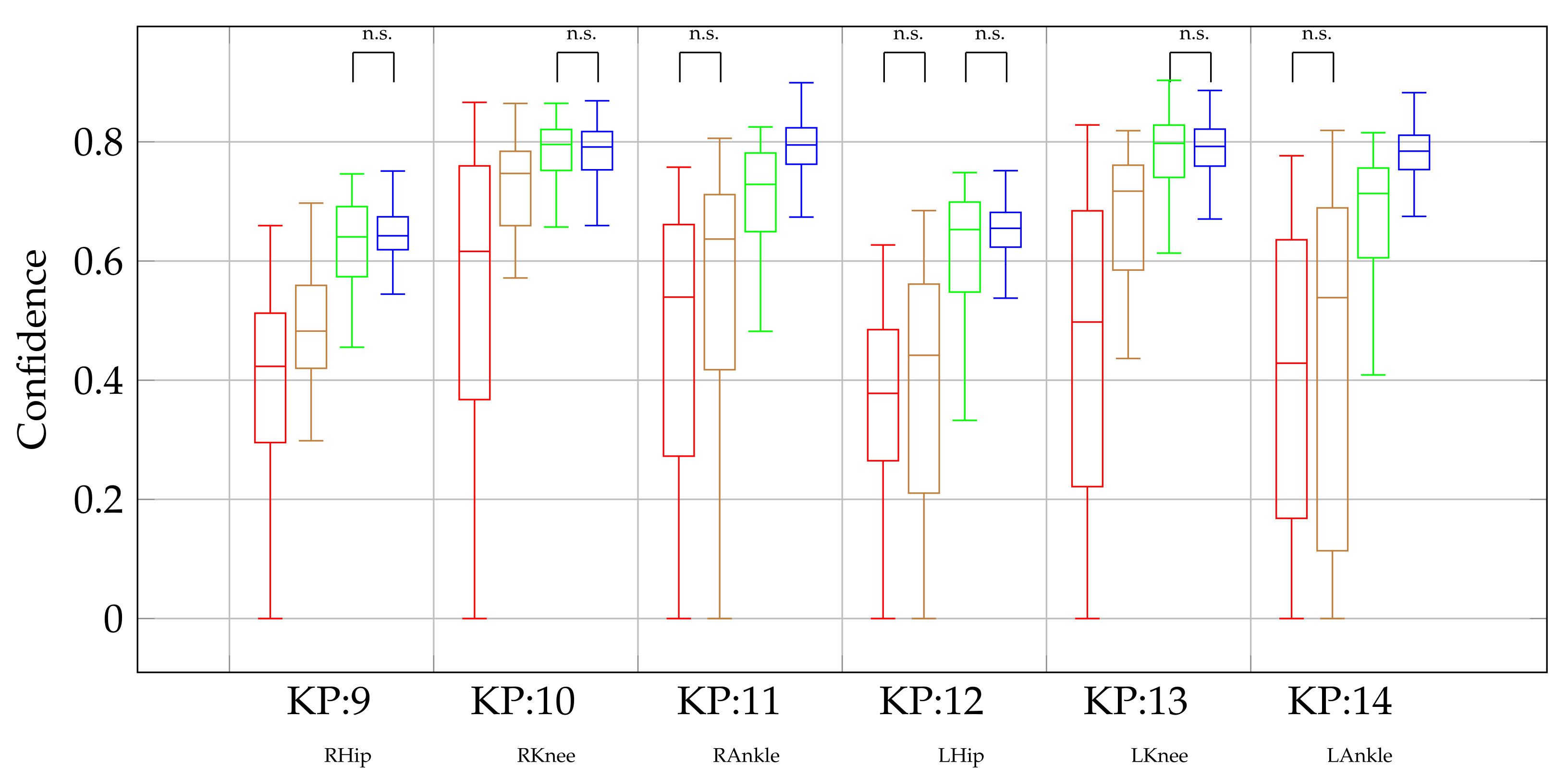
Figure 7.
Confidence of detection of selected KP (keypoints)—¾ view, lower body. Camera views are shown in colour as follows: lying down (N = 177); on the knees (N = 95); sitting (N = 165); and standing (N = 490). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 7.
Confidence of detection of selected KP (keypoints)—¾ view, lower body. Camera views are shown in colour as follows: lying down (N = 177); on the knees (N = 95); sitting (N = 165); and standing (N = 490). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 8.
Confidence of detection of selected KP (keypoints)—side view, upper body. Camera views are shown in colour as follows: lying down (N = 215); on the knees (N = 92); sitting (N = 145); and standing (N = 297). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 8.
Confidence of detection of selected KP (keypoints)—side view, upper body. Camera views are shown in colour as follows: lying down (N = 215); on the knees (N = 92); sitting (N = 145); and standing (N = 297). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 9.
Confidence of detection of selected KP (keypoints)—side view, lower body. Camera views are shown in colour as follows: lying down (N = 215); on the knees (N = 92); sitting (N = 145); and standing (N = 297). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Figure 9.
Confidence of detection of selected KP (keypoints)—side view, lower body. Camera views are shown in colour as follows: lying down (N = 215); on the knees (N = 92); sitting (N = 145); and standing (N = 297). All the other differences are statistically significant. Only differences that were not statistically significant (n.s.) are highlighted in the boxplots.
Table 1.
Number of videos in each category. Subcategories are: lying down (LY); on the knees (Kn); sitting (Si); standing (St).
Table 1.
Number of videos in each category. Subcategories are: lying down (LY); on the knees (Kn); sitting (Si); standing (St).
| Total (2133) |
|---|
| Front View (357) | ¾ View (1027) | Side view (749) |
| Ly | Kn | Si | St | Ly | Kn | Si | St | Ly | Kn | Si | St |
| 75 | 26 | 186 | 70 | 177 | 95 | 165 | 490 | 215 | 92 | 145 | 297 |
Table 2.
Categorization of videos.
Table 2.
Categorization of videos.
| Starting Position | Camera View |
|---|
| lying down (Ly) | front view (frontal plane) |
| on the knees (Kn) | ¾ view |
| sitting (Si) | side view (sagittal plane) |
| standing (St) | |
Table 3.
The 12 basic keypoints of the appendicular skeleton.
Table 3.
The 12 basic keypoints of the appendicular skeleton.
| No. | OP Name | The Most Appropriate Name of the Anatomical Point |
|---|
| Upper body |
| 2 | RShoulder | R. acromion, end of the clavicle (collar bone)—top of shoulder |
| 3 | RElbow | R. lateral epicondyle of humerus, lateral epicondyle of the humerus. Outside of elbow. |
| 4 | RWrist | R. styloid process of the radius; wrist on thumb side. |
| 5 | LShoulder | R. acromion, end of the clavicle (collar bone)—top of shoulder |
| 6 | LElbow | R. lateral epicondyle of humerus, lateral epicondyle of the humerus. Outside of elbow. |
| 7 | LWrist | L. styloid process of the radius; wrist on thumb side. |
| Lower body |
| 9 | RHip | R. femur greater trochanter |
| 10 | RKnee | R. femur lateral epicondyle |
| 11 | RAnkle | R. fibula apex of lateral malleolus |
| 12 | LHip | L. femur greater trochante |
| 13 | LKnee | L. femur lateral epicondyle |
| 14 | LAnkle | L. fibula apex of lateral malleolus |
Table 4.
Median confidence value for each specific group.
Table 4.
Median confidence value for each specific group.
| Medians of Confidence for Selected Group and OP Keypoint |
|---|
| Camera View | Front view | ¾ view | Side view |
| Starting possition | Ly | Kn | Si | St | Ly | Kn | Si | St | Ly | Kn | Si | St |
| No. | KP name | |
| Upper body |
| 2 | RShoulder | 0.67 | 0.65 | 0.78 | 0.80 | 0.62 | 0.67 | 0.77 | 0.79 | 0.68 | 0.68 | 0.76 | 0.78 |
| 3 | RElbow | 0.75 | 0.81 | 0.82 | 0.84 | 0.76 | 0.81 | 0.82 | 0.84 | 0.78 | 0.82 | 0.81 | 0.83 |
| 4 | RWrist | 0.75 | 0.79 | 0.82 | 0.84 | 0.75 | 0.80 | 0.82 | 0.83 | 0.79 | 0.81 | 0.81 | 0.83 |
| 5 | LShoulder | 0.54 | 0.60 | 0.79 | 0.80 | 0.53 | 0.63 | 0.80 | 0.80 | 0.52 | 0.54 | 0.77 | 0.78 |
| 6 | Lelbow | 0.39 | 0.78 | 0.81 | 0.83 | 0.66 | 0.78 | 0.79 | 0.81 | 0.41 | 0.72 | 0.79 | 0.79 |
| 7 | LWrist | 0.39 | 0.77 | 0.79 | 0.83 | 0.59 | 0.80 | 0.79 | 0.81 | 0.30 | 0.77 | 0.78 | 0.80 |
| Lower body |
| 9 | RHip | 0.42 | 0.48 | 0.64 | 0.64 | 0.38 | 0.51 | 0.66 | 0.64 | 0.40 | 0.49 | 0.59 | 0.64 |
| 10 | RKnee | 0.62 | 0.75 | 0.80 | 0.79 | 0.61 | 0.78 | 0.81 | 0.78 | 0.65 | 0.78 | 0.78 | 0.78 |
| 11 | RAnkle | 0.54 | 0.64 | 0.73 | 0.79 | 0.53 | 0.68 | 0.71 | 0.79 | 0.56 | 0.67 | 0.69 | 0.78 |
| 12 | LHip | 0.38 | 0.44 | 0.65 | 0.65 | 0.35 | 0.47 | 0.66 | 0.65 | 0.35 | 0.40 | 0.58 | 0.63 |
| 13 | LKnee | 0.50 | 0.72 | 0.80 | 0.79 | 0.41 | 0.71 | 0.81 | 0.79 | 0.51 | 0.66 | 0.79 | 0.78 |
| 14 | LAnkle | 0.43 | 0.54 | 0.71 | 0.78 | 0.40 | 0.65 | 0.71 | 0.78 | 0.47 | 0.55 | 0.68 | 0.78 |
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}