
Influence of Heart Rate on Left and Right Ventricular Longitudinal Strain in Patients with Chronic Heart Failure




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Reproducibility of the Measures of RV and LV Strain
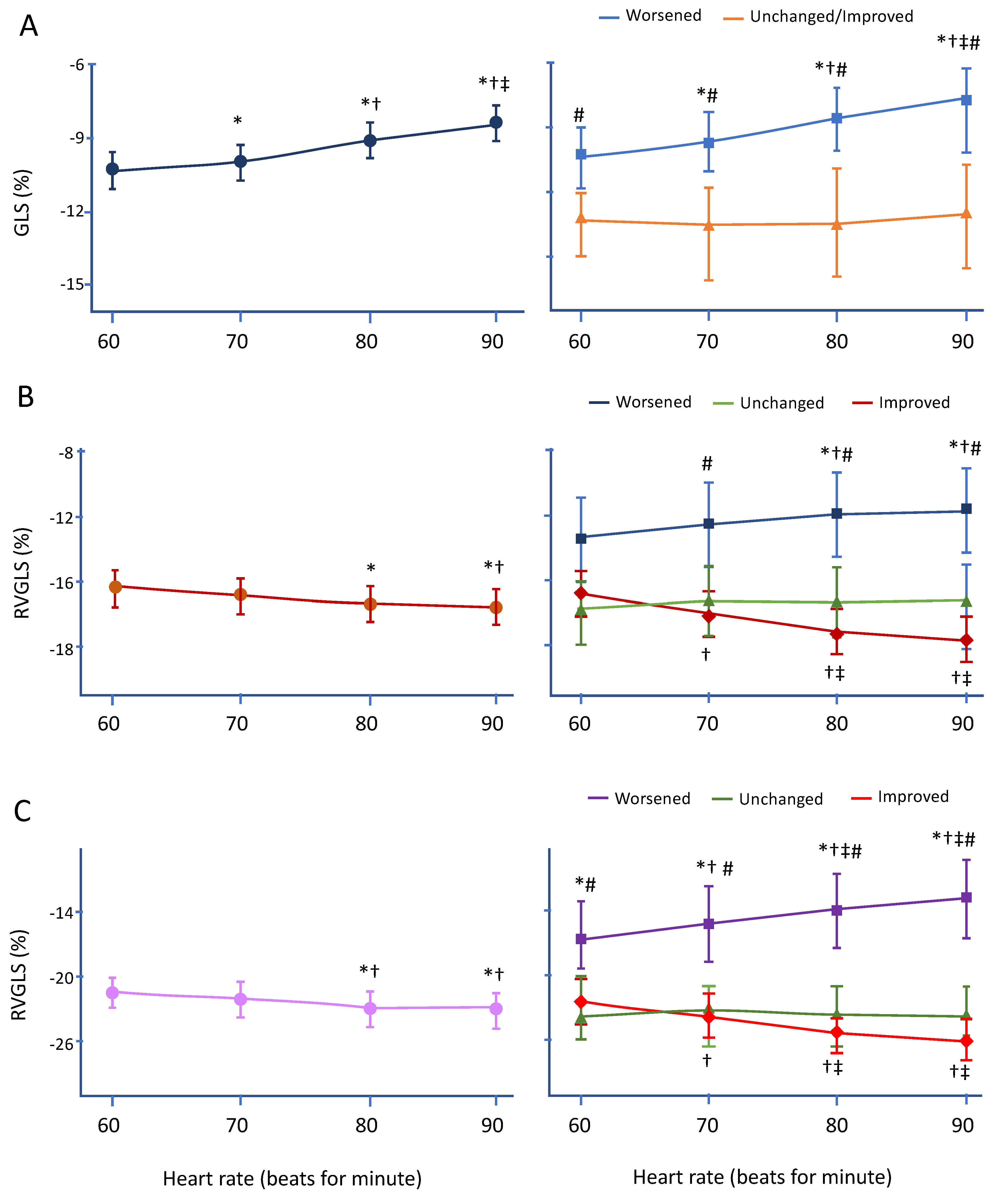
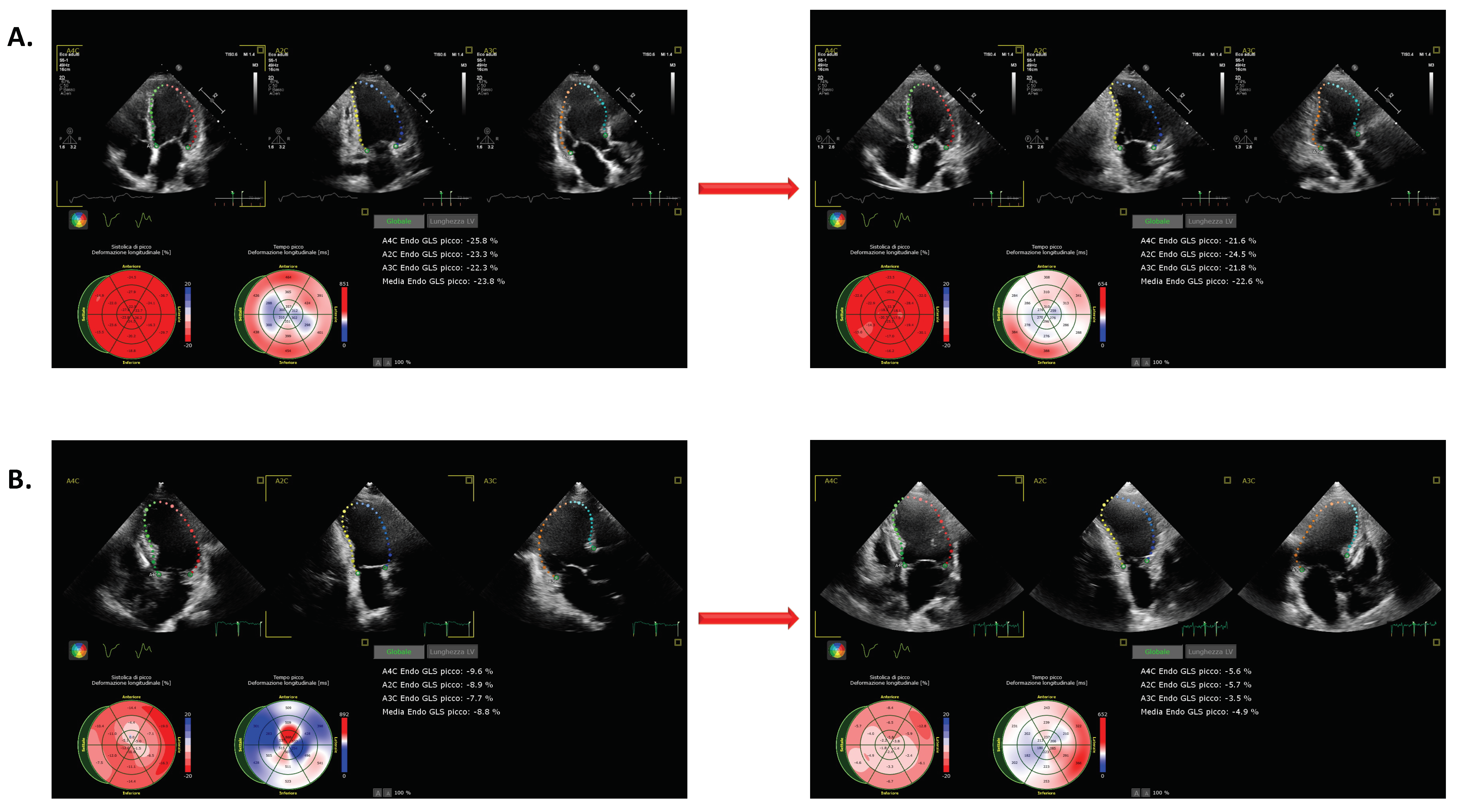
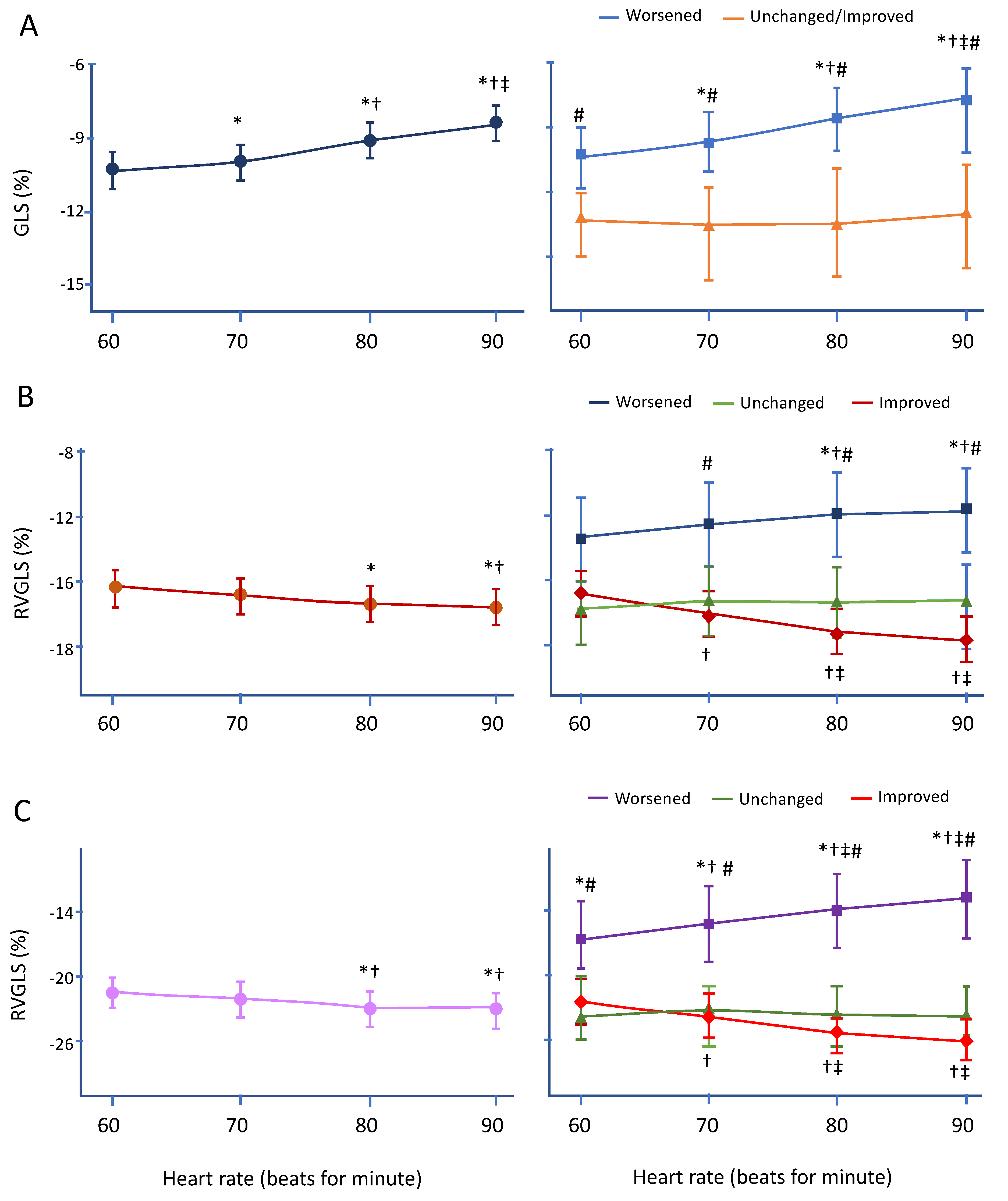
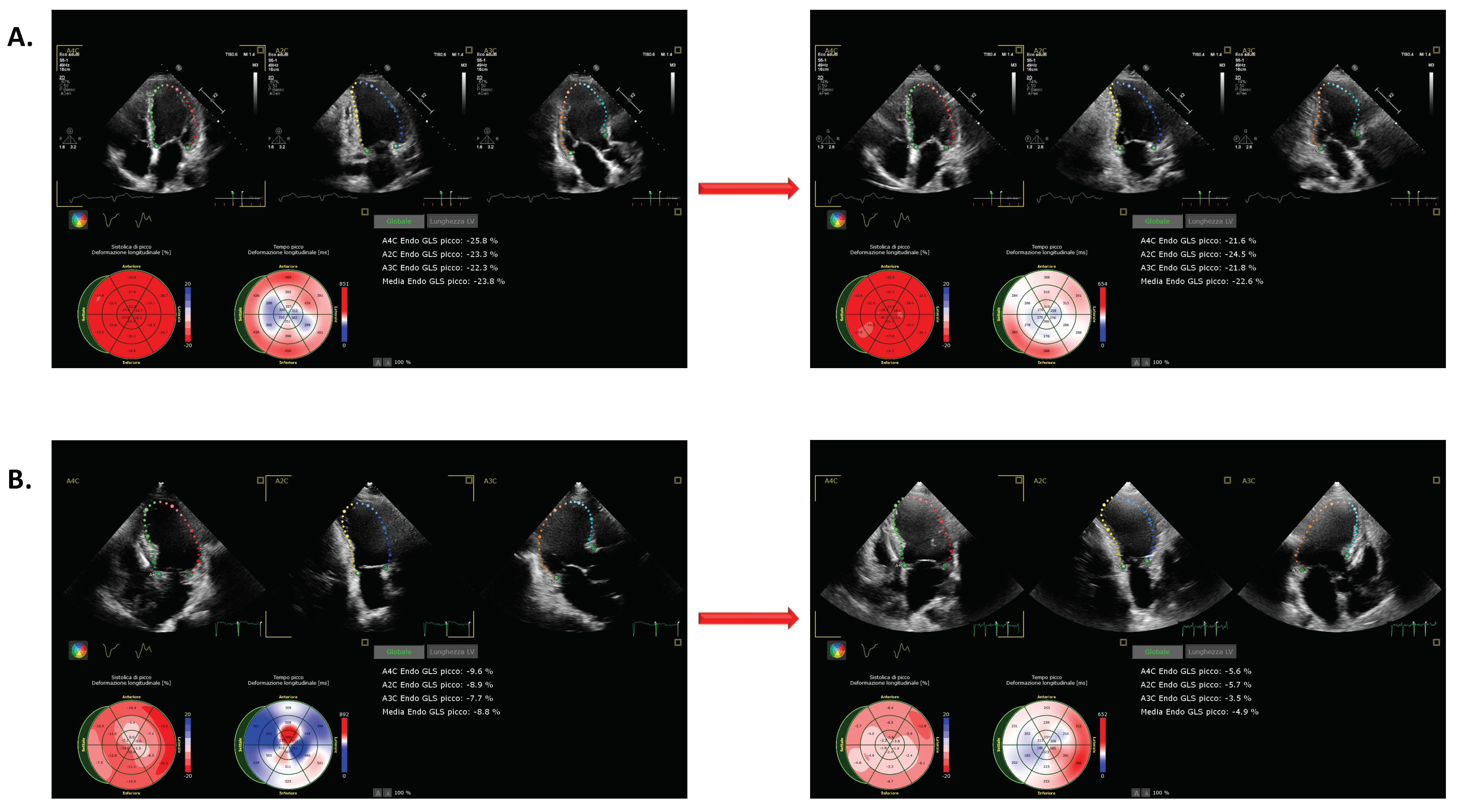
3.3. Changes in LVGLS during Pacing
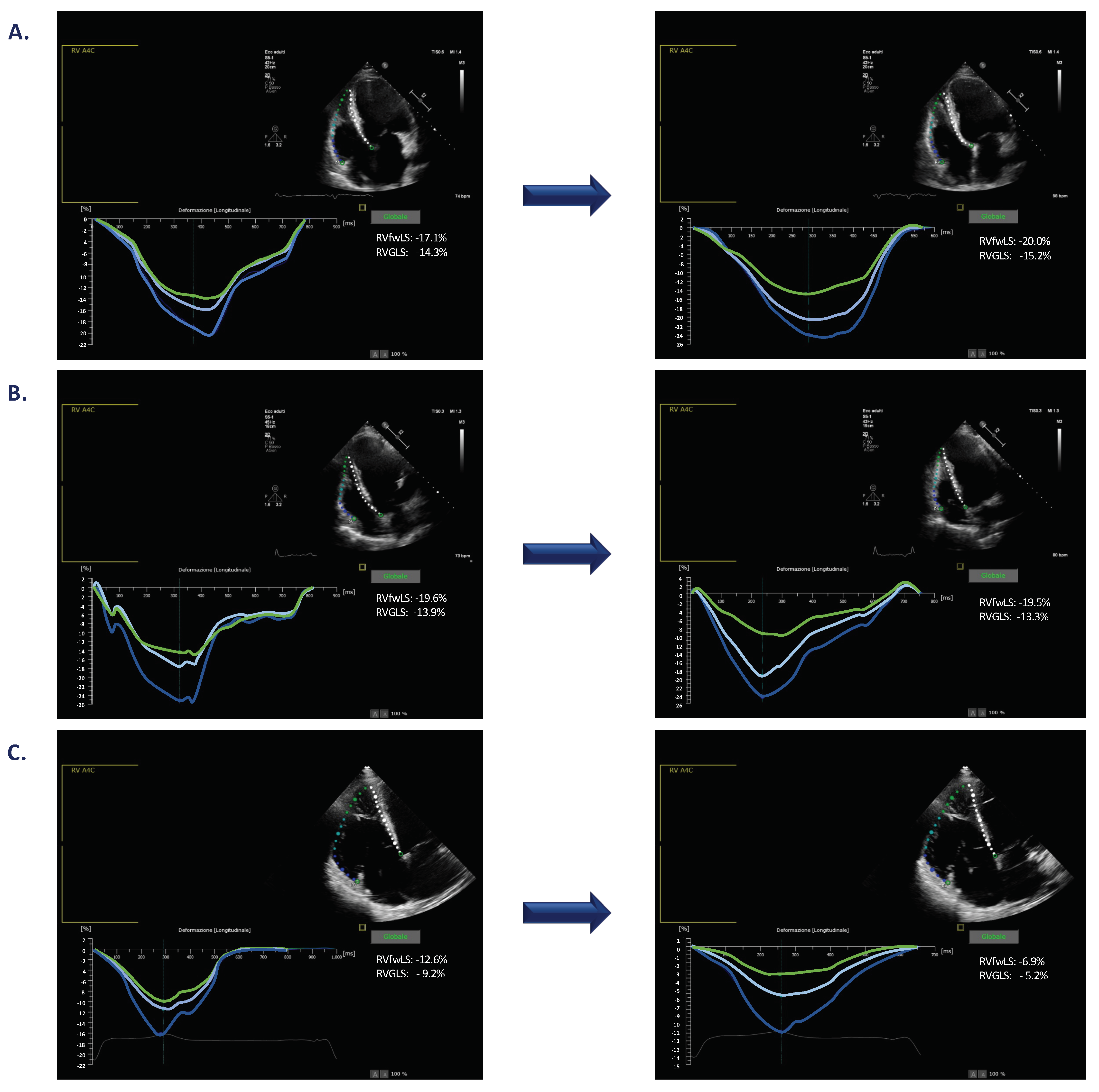
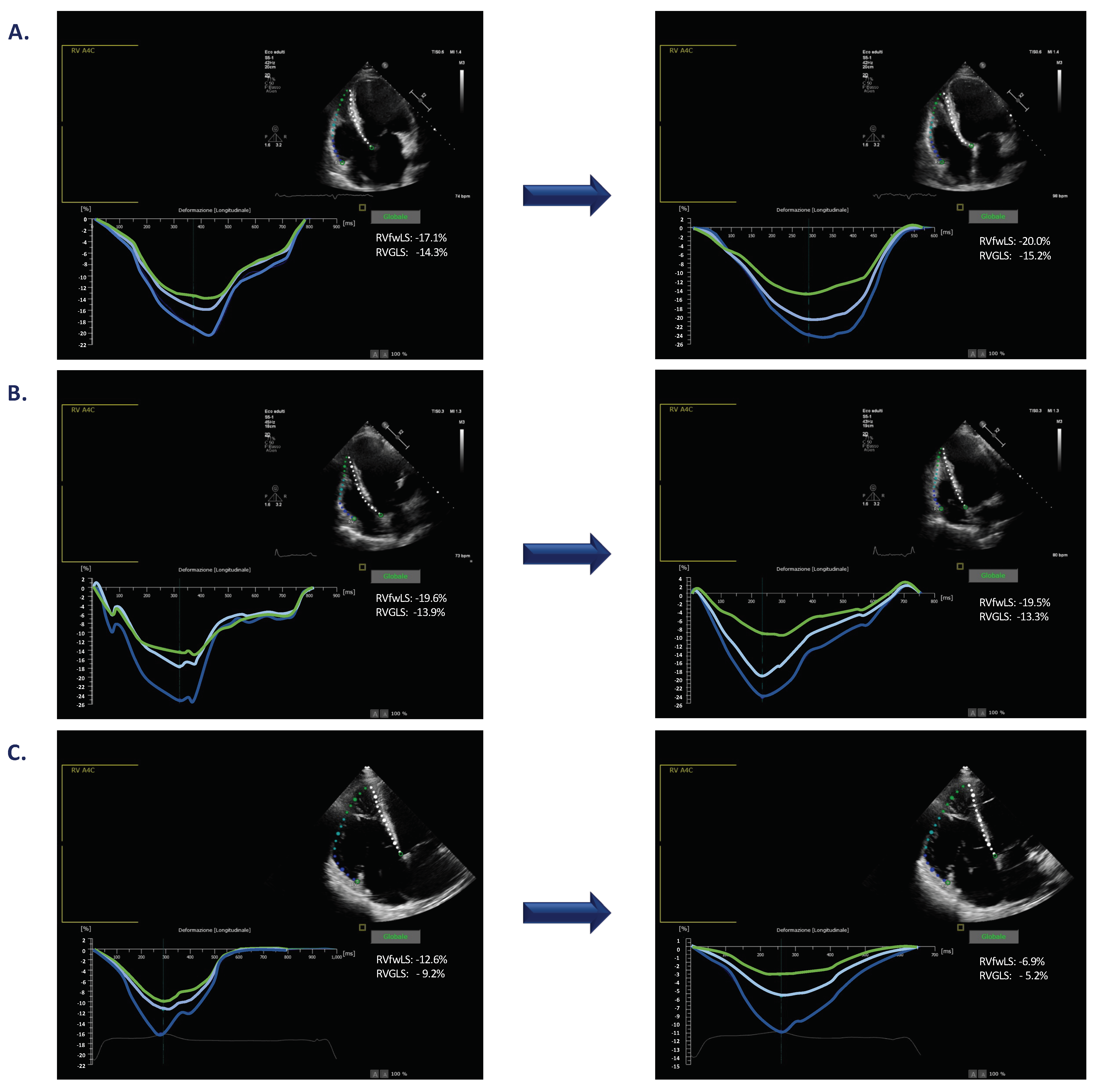
3.4. Changes in RVGLS during Pacing
3.5. Changes in RVfwLS during Pacing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dandel, M.; Lehmkuhl, H.; Knosalla, C.; Suramelashvili, N.; Hetzer, R. Strain and strain rate imaging by echocardiography—Basic concepts and clinical applicability. Curr. Cardiol. Rev. 2009, 5, 133–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iacoviello, M.; Puzzovivo, A.; Guida, P.; Forleo, C.; Monitillo, F.; Catanzaro, R.; Lattarulo, M.S.; Antoncecchi, V.; Favale, S. Independent role of left ventricular global longitudinal strain in predicting prognosis of chronic heart failure patients. Echocardiography 2013, 30, 803–811. [Google Scholar] [CrossRef]
- Iacoviello, M.; Citarelli, G.; Antoncecchi, V.; Romito, R.; Monitillo, F.; Leone, M.; Puzzovivo, A.; Lattarulo, M.S.; Rizzo, C.; Caldarola, P.; et al. Right ventricular longitudinal strain measures independently predict chronic heart failure mortality. Echocardiography 2016, 33, 992–1000. [Google Scholar] [CrossRef]
- Monitillo, F.; Di Terlizzi, V.; Gioia, M.I.; Barone, R.; Grande, D.; Parisi, G.; Brunetti, N.D.; Iacoviello, M. Right Ventricular Function in Chronic Heart Failure: From the Diagnosis to the Therapeutic Approach. J. Cardiovasc. Dev. Dis. 2020, 7, 12. [Google Scholar] [CrossRef]
- Moonen, M.; Lancellotti, P.; Zacharakis, D.; Pierard, L. The value of 2D strain imaging during stress testing. Echocardiography 2009, 26, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasselberg, N.E.; Haugaa, K.H.; Sarvari, S.I.; Gullestad, G.; Andreassen, A.K.; Smiseth, O.A.; Edvardsen, T. Left ventricular global longitudinal strain is associated with exercise capacity in failing hearts with preserved and reduced ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Mulieri, L.A.; Hasenfuss, G.; Leavitt, B.; Allen, P.D.; Alpert, N.R. Altered Myocardial Force-Frequency Relation in Human Heart Failure. Circulation 1992, 85, 1743–1750. [Google Scholar] [CrossRef] [Green Version]
- Phillips, P.J.; Gwathmey, J.K.; Feldman, M.D.; Schoen, F.; Grossman, W.; Morgan, J.P. Post-extrasystolic potentiation and the force-frequency relationship: Differential augmentation of myocardial contractility in working myocardium from patients with end-stage heart failure. J. Mol. Cell Cardiol. 1990, 22, 99–110. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar]
- Alessandrini, M.; Chakraborty, B.; Heyde, B.; Bernard, O.; De Craene, M.; Sermesant, M.; D’Hooge, J. Realistic vendor-specific synthetic ultrasound data for quality assurance of 2-D speckle tracking echocardiography: Simulation pipeline and open access database. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2018, 65, 411–422. [Google Scholar] [CrossRef]
- Zhou, Y.; Giffard-Roisin, S.; De Craene, M.; Camarasu-Pop, S.; D’Hooge, J.; Alessandrini, M.; Friboulet, D.; Sermesant, M.; Bernard, O. A framework for the generation of realistic synthetic cardiac ultrasound and magnetic resonance imaging sequences from the same virtual patients. IEEE Trans. Med. Imaging 2018, 37, 741–754. [Google Scholar] [CrossRef] [Green Version]
- Korinek, J.; Wang, J.; Sengupta, P.P.; Miyazaki, C.; Kjaergaard, J.; McMahon, E.; Abraham, T.P.; Belohlavek, M. Two-dimensional strain—A Doppler-independent ultrasound method for quantitation of regional deformation: Validation in vitro and in vivo. J. Am. Soc. Echocardiogr. 2005, 18, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Amzulescu, M.S.; Langet, H.; Saloux, E.; Manrique, A.; Boileau, L.; Slimani, A.; Allain, P.; Roy, C.; de Meester, C.; Pasquet, A.; et al. Head-to-head comparison of global and regional two-dimensional speckle tracking strain versus cardiac magnetic resonance tagging in a multicenter validation study. Circ. Cardiovasc. Imaging 2017, 10, e006530. [Google Scholar] [CrossRef] [Green Version]
- Bansal, M.; Cho, G.Y.; Chan, J.; Leano, R.; Haluska, B.A.; Marwick, T.H. Feasibility and accuracy of different techniques of two-dimensional speckle-based strain and validation with harmonic phase magnetic resonance imaging. J. Am. Soc. Echocardiogr. 2008, 21, 1318–1325. [Google Scholar] [CrossRef]
- Mirea, O.; Pagourelias, E.D.; Duchenne, J.; Bogaert, J.; Thomas, J.D.; Badano, L.P.; Voigt, J.U. Variability and Reproducibility of Segmental Longitudinal Strain Measurement. A Report from the EACVI-ASE Strain Standardization Task Force. JACC Cardiovasc. Imaging 2018, 11, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Iacoviello, M.; Forleo, C.; Puzzovivo, A.; Nalin, I.; Guida, P.; Anaclerio, M.; Marangelli, V.; Sorrentino, S.; Monitillo, F.; Ciccone, M.M.; et al. Altered two-dimensional strain measures of the right ventricle in patients with Brugada syndrome and arrhythmogenic right ventricular dysplasia/cardiomyopathy. Eur. J. Echocardiogr. 2011, 12, 773–781. [Google Scholar] [CrossRef] [Green Version]
- Iacoviello, M.; Monitillo, F.; Citarelli, G.; Leone, M.; Grande, D.; Antoncecchi, V.; Rizzo, C.; Terlizzese, P.; Romito, R.; Caldarola, P.; et al. Right ventriculo-arterial coupling assessed by two-dimensional strain: A new parameter of right ventricular function independently associated with prognosis in chronic heart failure patients. Int. J. Cardiol. 2017, 15, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Tsougos, E.; Angelidis, G.; Gialafos, E.; Tzavara, C.; Tzifos, C.; Tsougos, I.; Georgoulias, P. Myocardial strain may predict exercise tolerance in patients with reduced and mid-range ejection fraction. Hell. J. Cardiol. 2018, 59, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Von Scheidt, F.; Kiesler, V.; Kaestner, M.; Bride, P.; Krämer, J.; Apitz, C. Left ventricular strain and strain rate during submaximal semisupine bicycle exercise stress echocardiography in healthy adolescents and young adults: Systematic protocol and reference values. J. Am. Soc. Echocardiogr. 2020, 33, 848–857. [Google Scholar] [CrossRef]
- Mak, S.; Van Spall, H.G.C.; Wainstein, R.V.; Sasson, Z. Strain, strain rate, and the force frequency relationship in patients with and without heart failure. J. Am. Soc. Echocardiogr. 2012, 25, 341–348. [Google Scholar] [CrossRef]
- Fredholm, M.; Jörgensen, K.; Houltz, E.; Ricksten, S.E. Load-dependence of myocardial deformation variables—A clinical strain-echocardiographic study. Acta Anaesthesiol. Scand. 2017, 61, 1155–1165. [Google Scholar] [CrossRef] [PubMed]
- Esfandiari, S.; Fuchs, F.; Wainstein, R.V.; Chelvanathan, A.; Mitoff, P.; Sasson, Z.; Mak, S. Heart rate-dependent left ventricular diastolic function in patients with and without heart failure. J. Card. Fail. 2015, 21, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Bohm, M.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Heart rate as a risk factor in chronic heart failure (SHIFT): The association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet 2010, 376, 886–894. [Google Scholar] [CrossRef]
- Friedberg, M.K.; Redington, A.N. Right versus left ventricular failure: Differences, similarities, and interactions. Circulation 2014, 129, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Bellenger, N.G.; Burgess, M.I.; Ray, S.G.; Lahiri, A.; Coats, A.J.S.; Cleland, J.G.F.; Pennell, D.J. Comparison of left ventricular ejection fraction and volumes in heart failure by echocardiography, radionuclide ventriculography and cardiovascular magnetic resonance. Are they interchangeable? Eur. Heart J. 2000, 21, 1387–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Echocardiographic Characteristics | ||
|---|---|---|---|
| Age (years) | 66 ± 13 | LVEDV (mL) | 176 ± 87 |
| Male, n (%) | 36 (80%) | LVESV (mL) | 121 ± 76 |
| BMI (kg/m2) | 24 ± 4 | LVEF (%) | 36 ± 13 |
| Ischemic cardiomyopathy, n (%) | 19 (42%) | LVGLS (%) | −10.2 ± 4.0 |
| Arterial hypertension, n (%) | 29 (64%) | LV Tei index | 0.64 ± 0.23 |
| Diabetes mellitus, n (%) | 13 (29%) | SV (mL) | 65 ± 16 |
| Dyslipidemia, n (%) | 32 (71%) | CO (L/min) | 4.2 ± 1.1 |
| CHF, n (%) | 39 (87%) | CI (L/min/m2) | 2.2 ± 0.6 |
| SAP (mmHg) | 116 ± 21 | LVMI (g/m2) | 156 ± 40 |
| Heart rate (bpm) | 66 ± 7 | LAVi (mL) | 40 ± 19 |
| LVEF ≤ 40%, n (%) | 31 (69%) | e’ s (cm/s) | 5.0 ± 1.4 |
| NYHA class, n (%) I | 7 (16%) | e’ l (cm/s) | 6.9 ± 2.8 |
| NYHA class, n (%) II | 21 (46%) | e’ m (cm/s) | 5.9 ± 1.9 |
| NYHA class, n (%) III | 17 (38%) | E/e’ ratio | 13.1 ± 5.9 |
| GFR-EPI (mL/min/1.73 m2) | 80 ± 17 | MR (a.u.) | 2.0 ± 0.9 |
| NT-proBNP (pg/mL) | 2879 ± 2841 | TAPSE (mm) | 18.9 ± 3.5 |
| ACEi/ARBs, n (%) | 22 (49%) | RVGLS (%) | −15.5 ± 3.8 |
| ARNI, n (%) | 12 (27%) | RVfwLS | −20.9 ± 5.2 |
| Beta-blockers, n (%) | 42 (93%) | CVP (mmHg) | 6.2 ± 3.2 |
| MRA, n (%) | 22 (49%) | PASP (mmHg) | 36 ± 13 |
| Loop diuretics, n (%) | 32 (71%) | TR (a.u.) | 1.8 ± 1.1 |
| Changes in LVGLS in Response to Increasing HR | |||
|---|---|---|---|
| Worsened (n = 34) | Unchanged/Improved (n = 11) | p | |
| Age (years) | 67 ± 14 | 65 ± 13 | 0.714 |
| BMI (kg/m2) | 24 ± 5 | 25 ± 4 | 0.559 |
| SAP (mm Hg) | 114 ± 21 | 123 ± 22 | 0.212 |
| NYHA | 2.4 ± 0.6 | 2.0 ± 0.8 | 0.141 |
| Baseline HR (bpm) | 66 ± 7 | 68 ± 5 | 0.392 |
| ICD/CRTD/PM (%) | 53/35/12 | 27/45/43 | 0.261 |
| LVEDV (mL) | 178 ± 83 | 170 ± 104 | 0.794 |
| LVEF (%) | 33 ± 11 | 44 ± 16 | 0.019 |
| LVEF ≤ 40% (%) | 81 | 19 | 0.237 |
| LVGLS (%) | −9.5 ± 3.4 | −12.0 ± 5.15 | 0.049 |
| LV Tei index | 0.69 ± 0.21 | 0.47 ± 0.19 | 0.003 |
| CI (L/min/m2) | 2.1 ± 0.5 | 2.5 ± 0.6 | 0.057 |
| LVMI (g/m2) | 153 ± 39 | 164 ± 44 | 0.457 |
| LAVi (mL) | 40 ± 20 | 38 ± 17 | 0.712 |
| E/e’ ratio | 13.2 ± 6.1 | 12.9 ± 5.8 | 0.884 |
| MR (a.u.) | 1.9 ± 0.9 | 2.2 ± 0.9 | 0.440 |
| TAPSE (mm) | 18.6 ± 3.5 | 20.2 ± 3.4 | 0.189 |
| PASP (mmHg) | 34 ± 11 | 32 ± 10 | 0.680 |
| TR (a.u.) | 1.7 ± 1.0 | 2.2 ± 1.7 | 0.193 |
| RVGLS (%) | −15.2 ± 3.9 | −16.4 ± 3.7 | 0.355 |
| RVfwLS (%) | −20.8 ± 5.2 | −21.3 ± 5.4 | 0.787 |
| RVGLS/PASP | −0.55 ± 0.19 | −0.50 ± 0.18 | 0.425 |
| RVfwLS/PASP | −0.68 ± 0.26 | −0.70 ± 0.26 | 0.868 |
| HR RVGLS Changes | ||||
|---|---|---|---|---|
| Worsened (n = 8) | Unchanged (n = 11) | Improved (n = 26) | ANOVA p | |
| Age (years) | 64 ± 14 | 63 ± 13 | 67 ± 13 | 0.630 |
| BMI (kg/m2) | 23 ± 3 | 25 ± 5 | 24 ± 5 | 0.518 |
| SAP (mm Hg) | 111 ± 17 | 115 ± 21 | 119 ± 23 | 0.624 |
| NYHA class | 2.4 ± 0.5 | 2.2 ± 0.8 | 2.3 ± 0.7 | 0.839 |
| Baseline HR (bpm) | 66 ± 8 | 67 ± 7 | 66 ± 7 | 0.917 |
| ICD/CRTD/PM (%) | 50/50/0 | 55/27/18 | 42/38/19 | 0.657 |
| LVEDV (mL) | 179 ± 69 | 199 ± 113 | 166 ± 80 | 0.586 |
| LVEF (%) | 29 ± 9 | 37 ± 14 | 38 ± 14 | 0.235 |
| LVEF ≤ 40% (%) | 23 | 26 | 52 | 0.364 |
| LVGLS (%) | −7.6 ± 3.3 | −10.2 ± 4.0 | −10.9 ± 4.0 | 0.122 |
| LV Tei index | 0.73 ± 0.60 | 0.60 ± 0.25 | 0.64 ± 0.23 | 0.551 |
| CI (L/min/m2) | 2.3 ± 0.6 | 2.2 ± 0.6 | 2.1 ± 0.6 | 0.764 |
| LVMI (g/m2) | 158 ± 31 | 169 ± 43 | 149 ± 42 | 0.367 |
| LAVi (mL) | 47 ± 25 | 41 ± 23 | 37 ± 15 | 0.404 |
| E/e’ ratio | 17.4 ± 6.3 | 13.2 ± 8.3 | 12.0 ± 4.3 | 0.136 |
| MR (a.u.) | 1.9 ± 1.2 | 1.8 ± 0.8 | 2.1 ± 0.8 | 0.596 |
| TAPSE (mm) | 15.3 ± 4.0 | 20.2 ± 3.1 * | 19.4 ± 2.9 * | 0.006 |
| PASP (mmHg) | 42 ± 14 | 31 ± 11 | 32 ± 8 | 0.029 |
| TR (a.u.) | 2.5 ± 1.1 | 2.0 ± 1.3 | 1.5 ± 0.9 | 0.057 |
| RVGLS (%) | −12.2 ± 1.1 | −16.6 ± 1.1 * | −16.0 ± 3.2 * | 0.020 |
| RVfwLS (%) | −17.0 ± 6.7 | −21.5 ± 4.8 | −21.9 ± 4.4 | 0.058 |
| RVGLS/PASP | −0.35 ± 0.21 | −0.58 ± 0.17 * | −0.54 ± 0.16 * | 0.013 |
| RVfwLS/PASP | −0.48 ± 0.28 | −0.73 ± 0.22 * | −0.74 ± 0.23 * | 0.033 |
| HR RVfwLS Changes | ||||
|---|---|---|---|---|
| Worsened (n = 7) | Unchanged (n = 13) | Improved (n = 25) | ANOVA p | |
| Age (years) | 61 ± 13 | 66 ± 13 | 66 ± 13 | 0.699 |
| BMI (kg/m2) | 23 ± 3 | 26 ± 4 | 24 ± 5 | 0.192 |
| SAP (mm Hg) | 105 ± 12 | 119 ± 24 | 118 ± 21 | 0.315 |
| NYHA class | 2.4 ± 0.5 | 2.2 ± 0.8 | 2.2 ± 0.7 | 0.448 |
| Baseline HR (bpm) | 66 ± 8 | 67 ± 7 | 66 ± 7 | 0.259 |
| ICD/CRTD/PM (%) | 57/43/0 | 38/54/8 | 48/28/24 | 0.321 |
| LVEDV (mL) | 219 ± 131 | 181 ± 76 | 161 ± 77 | 0.291 |
| LVEF (%) | 27 ± 9 | 36 ± 10 | 38 ± 15 | 0.116 |
| LVEF ≤ 40% (%) | 19 | 32 | 48 | 0.326 |
| LVGLS (%) | −7.1 ± 3.5 | −9.9 ± 3.5 | −11.2 ± 4.0 * | 0.048 |
| LV Tei index | 0.70 ± 0.21 | 0.59 ± 0.23 | 0.65 ± 0.23 | 0.603 |
| CI (L/min/m2) | 2.5 ± 0.5 | 2.1 ± 0.5 | 2.5 ± 0.6 | 0.457 |
| LVMI (g/m2) | 170 ± 49 | 166 ± 39 | 146 ± 37 | 0.191 |
| LAVi (mL) | 56 ± 26 | 39 ± 17 | 36 ± 16 | 0.051 |
| E/e’ ratio | 16.7 ± 7.0 | 13.1 ± 6.6 | 12.3 ± 5.3 | 0.395 |
| MR (a.u.) | 2.0 ± 1.3 | 1.8 ± 0.9 | 2.1 ± 0.8 | 0.749 |
| TAPSE (mm) | 16.8 ± 5.1 | 18.9 ± 3.5 | 19.5 ± 3.0 | 0.246 |
| PASP (mmHg) | 49 ± 13 | 30 ± 9 * | 31 ± 6 * | <0.001 |
| TR (a.u.) | 2.6 ± 1.1 | 1.8 ± 1.2 | 1.6 ± 0.9 | 0.841 |
| RVGLS (%) | −11.3 ± 5.1 | −16.0 ± 2.3 * | −16.4 ± 3.3 * | 0.005 |
| RVfwLS (%) | −15.3 ± 6.4 | −22.7 ± 3.7 * | −21.6 ± 4.6 * | 0.004 |
| RVGLS/PASP | −0.27 ± 0.19 | −0.57 ± 0.18 * | −0.55 ± 0.13 * | <0.001 |
| RVfwLS/PASP | −0.37 ± 0.24 | −0.81 ± 0.26 * | −0.72 ± 0.17 * | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Terlizzi, V.; Barone, R.; Manuppelli, V.; Correale, M.; Casavecchia, G.; Goffredo, G.; Pellegrino, P.; Puteo, A.; Ieva, R.; Di Biase, M.; et al. Influence of Heart Rate on Left and Right Ventricular Longitudinal Strain in Patients with Chronic Heart Failure. Appl. Sci. 2022, 12, 556. https://doi.org/10.3390/app12020556
Di Terlizzi V, Barone R, Manuppelli V, Correale M, Casavecchia G, Goffredo G, Pellegrino P, Puteo A, Ieva R, Di Biase M, et al. Influence of Heart Rate on Left and Right Ventricular Longitudinal Strain in Patients with Chronic Heart Failure. Applied Sciences. 2022; 12(2):556. https://doi.org/10.3390/app12020556
Chicago/Turabian StyleDi Terlizzi, Vito, Roberta Barone, Vincenzo Manuppelli, Michele Correale, Grazia Casavecchia, Giovanni Goffredo, Pierluigi Pellegrino, Alessandra Puteo, Riccardo Ieva, Matteo Di Biase, and et al. 2022. "Influence of Heart Rate on Left and Right Ventricular Longitudinal Strain in Patients with Chronic Heart Failure" Applied Sciences 12, no. 2: 556. https://doi.org/10.3390/app12020556
APA StyleDi Terlizzi, V., Barone, R., Manuppelli, V., Correale, M., Casavecchia, G., Goffredo, G., Pellegrino, P., Puteo, A., Ieva, R., Di Biase, M., Brunetti, N. D., & Iacoviello, M. (2022). Influence of Heart Rate on Left and Right Ventricular Longitudinal Strain in Patients with Chronic Heart Failure. Applied Sciences, 12(2), 556. https://doi.org/10.3390/app12020556