
A Dual-Adaptive Approach Based on Discrete Cosine Transform for Removal of ECG Baseline Wander


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Theoretical Backgrounds of Discrete Cosine Transform
2.2. The Proposed Dual-Adaptive Scheme
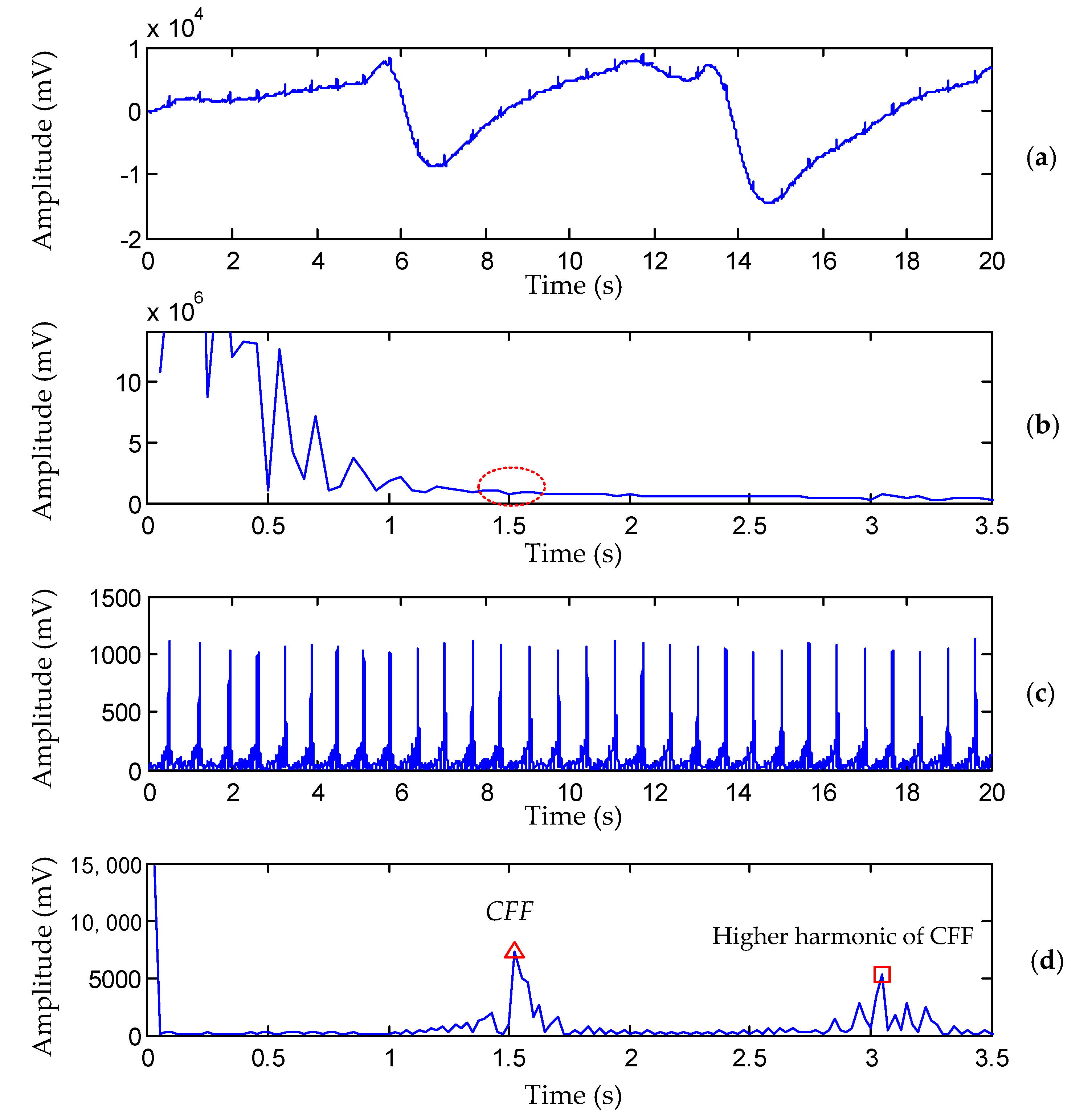
2.2.1. Calculating the Cardiac Fundamental Frequency (CFF)
- Extract the QRS-complexes from the ECG signal by a DCT-based band-pass filter whose passband is [5~40] Hz.
- Detect the peak’s index related to CFF in . Detecting is based on a threshold decision as shown in Figure 1d. The maximum value of in the range of 0.2 Hz to 2.5 Hz is detected at first. The index of may be related to CFF but also could be related to the higher harmonics of CFF. In this study, a threshold value of 0.65 was chosen empirically to determine which is the first point whose value exceeds .
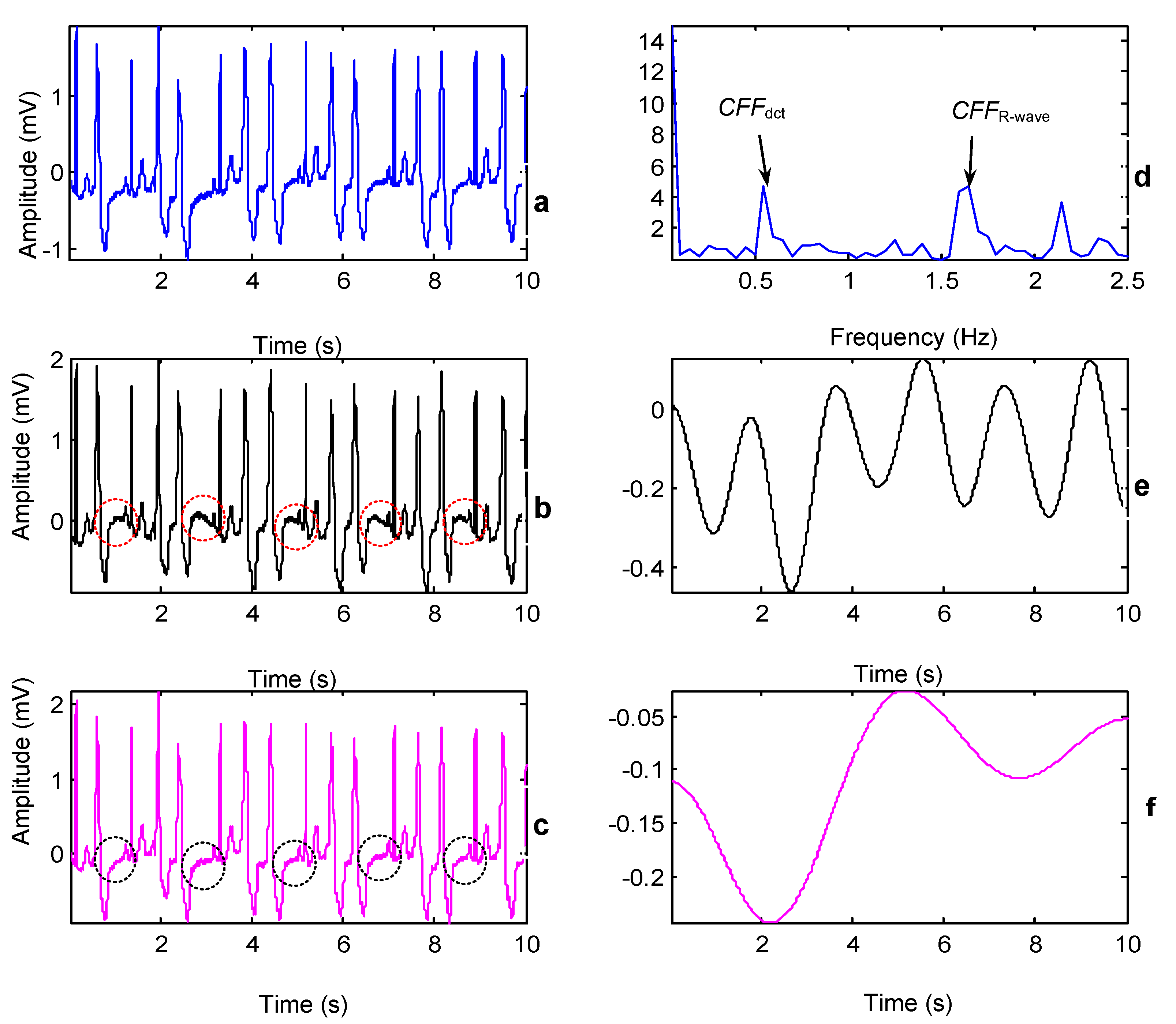
2.2.2. Searching for the Optimal Cut-Point before CFF
2.2.3. Reconstructing BW and Subtracting It from the Original ECG
3. Results
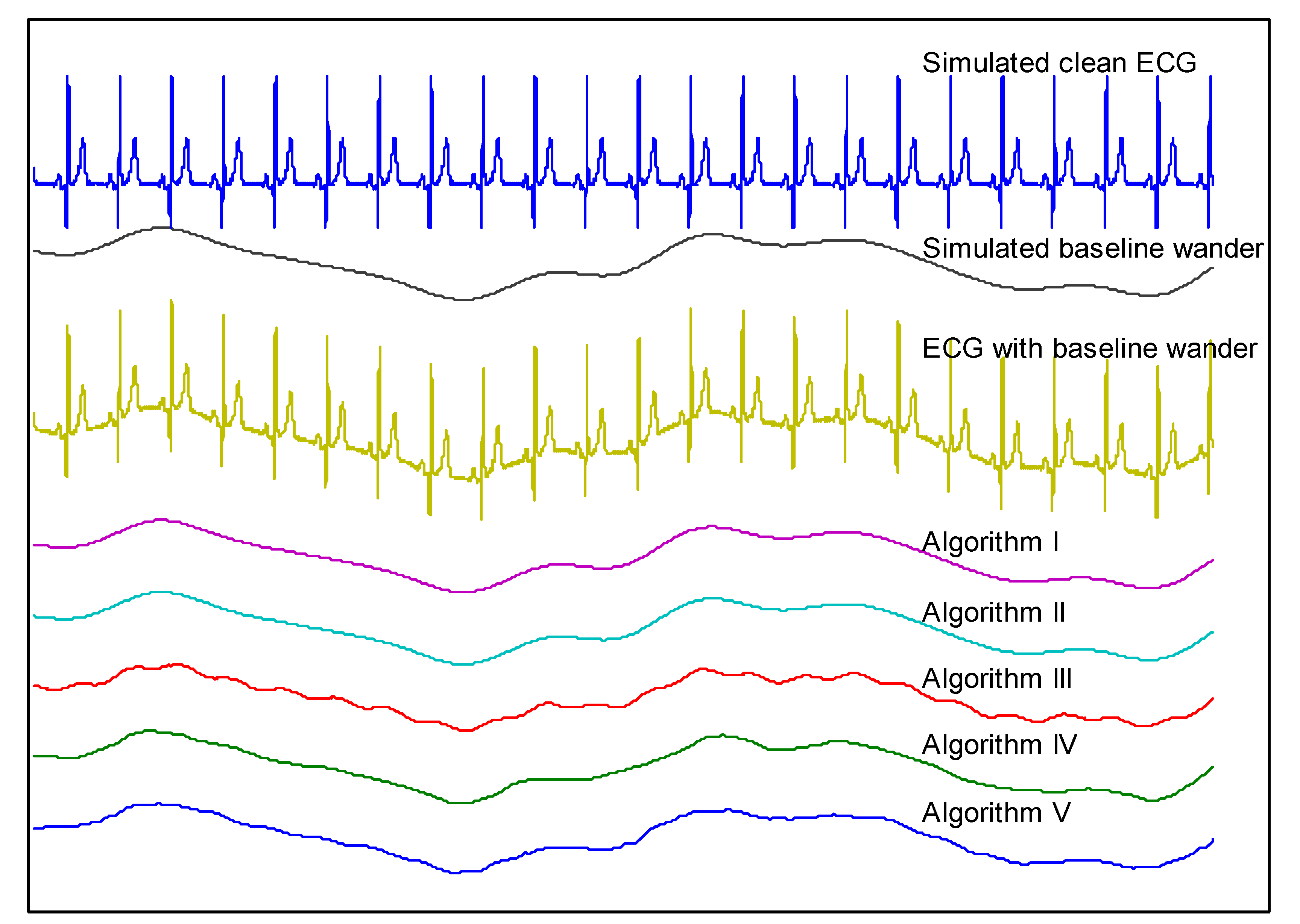
- A DCT-based filter [27] with the proposed dual-adaptive scheme to search for the optimal cut-point between BW and the true ECG. .
- A DCT-based filter [27] which let the cutoff frequency be 0.9 × CFF.
- A linear phase, sharp cut-off FIR filter [28] with a cutoff frequency of 0.9 × CFF.
- A WT-based algorithm using Daub-4 mother wavelet [29].
- A weighted median filter [30] with parameters (.
3.1. Performance Comparison on Real ECG Record
3.2. Experiments with Simulated ECG and BW
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shin, S.; Kang, M.; Zhang, G.; Jung, J.; Kim, Y.T. Lightweight Ensemble Network for Detecting Heart Disease Using ECG Signals. Appl. Sci. 2022, 12, 3291. [Google Scholar] [CrossRef]
- Liu, R.; Shu, M.; Chen, C. ECG Signal Denoising and Reconstruction Based on Basis Pursuit. Appl. Sci. 2021, 11, 1591. [Google Scholar] [CrossRef]
- Hagiwara, Y.; Fujita, H.; Oh, S.L.; Tan, J.H.; San Tan, R.; Ciaccio, E.J.; Acharya, U.R. Computer-aided diagnosis of atrial fibrillation based on ECG Signals: A review. Inf. Sci. 2018, 467, 99–114. [Google Scholar] [CrossRef]
- Vogel, B.; Claessen, B.E.; Arnold, S.V.; Chan, D.; Cohen, D.J.; Giannitsis, E.; Gibson, C.M.; Goto, S.; Katus, H.A.; Kerneis, M.; et al. ST-segment elevation myocardial infarction. Nat. Rev. Dis. Primers 2019, 5, 39. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.C.; Lin, J.J.; Hsieh, J.C.; Weng, J. Myocardial infarction classification with multi-lead ECG using hidden Markov models and Gaussian mixture models. Appl. Soft Comput. 2012, 12, 3165–3175. [Google Scholar] [CrossRef]
- Almeida, B.C.S.; Carmo, A.A.L.D.; Barbosa, M.P.T.; Silva, J.L.P.D.; Ribeiro, A.L.P. Association between microvolt T-wave alternans and malignant ventricular arrhythmias in Chagas disease. Arq. Bras. De Cardiol. 2018, 110, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, K.H.; Lee, J.W.; Kim, K.S. Semi-real-time removal of baseline fluctuations in electrocardiogram (ECG) signals by an infinite impulse response low-pass filter (IIR-LPF). J. Supercomput. 2018, 74, 6785–6793. [Google Scholar] [CrossRef]
- Boudet, S.; de l’Aulnoit, A.H.; Demailly, R.; Peyrodie, L.; Beuscart, R.; de l’Aulnoit, D.H. Fetal heart rate baseline computation with a weighted median filter. Comput. Biol. Med. 2019, 114, 103468. [Google Scholar] [CrossRef]
- Khosravy, M.; Gupta, N.; Patel, N.; Senjyu, T.; Duque, C.A. Particle swarm optimization of morphological filters for electrocardiogram baseline drift estimation. In Applied Nature-Inspired Computing: Algorithms and Case Studies; Springer: Singapore, 2020; pp. 1–21. [Google Scholar]
- Sun, P.; Wu, Q.H.; Weindling, A.M.; Finkelstein, A.; Ibrahim, K. An improved morphological approach to background normalization of ECG signals. IEEE Trans. Biomed. Eng. 2003, 50, 117–121. [Google Scholar] [CrossRef]
- Romero, F.P.; Romaguera, L.V.; Vázquez-Seisdedos, C.R.; Costa, M.G.F.; Neto, J.E. Baseline wander removal methods for ECG signals: A comparative study. arXiv 2018, arXiv:1807.11359. [Google Scholar]
- Ojo, J.A.; Adetoyi, T.B.; Adeniran, S.A. Removal of Baseline Wander Noise from Electrocardiogram (ECG) using Fifth-order Spline Interpolation. J. Appl. Comput. Sci. Math. 2016, 10, 9–14. [Google Scholar] [CrossRef]
- Shusterman, V.; Shah, S.I.; Beigel, A.; Anderson, K.P. Enhancing the precision of ECG baseline correction: Selective filtering and removal of residual error. Comput. Biomed. Res. 2000, 33, 144–160. [Google Scholar] [CrossRef] [PubMed]
- Barhatte, A.S.; Ghongade, R.; Tekale, S.V. Noise analysis of ECG signal using fast ICA. In Proceedings of the 2016 Conference on Advances in Signal Processing (CASP), Pune, India, 9–11 June 2016; pp. 118–122. [Google Scholar]
- Kora, P.; Kumari, C.U.; Swaraja, K.; Meenakshi, K. Atrial fibrillation detection using discrete wavelet transform. In Proceedings of the 2019 IEEE International Conference on Electrical, Computer and Communication Technologies (ICECCT), Coimbatore, India, 20–22 February 2019; pp. 1–3. [Google Scholar]
- Lin, C.C.; Chang, H.Y.; Huang, Y.H.; Yeh, C.Y. A novel wavelet-based algorithm for detection of QRS complex. Appl. Sci. 2019, 9, 2142. [Google Scholar] [CrossRef]
- B’charri, E.; Latif, R.; Elmansouri, K.; Abenaou, A.; Jenkal, W. ECG signal performance de-noising assessment based on threshold tuning of dual-tree wavelet transform. Biomed. Eng. Online 2017, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.H.; Lee, S.G. ECG identification based on non-fiducial feature extraction using window removal method. Appl. Sci. 2017, 7, 1205. [Google Scholar] [CrossRef]
- Haider, S.I.; Alhussein, M. Detection and classification of baseline-wander noise in ECG signals using discrete wavelet transform and decision tree classifier. Elektron. Ir Elektrotech. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Belkacem, S.; Messaoudi, N.; Dibi, Z. Artifact removal from electrocardiogram signal: A comparative study. In Proceedings of the 2018 International Conference on Signal, Image, Vision and their Applications (SIVA), Guelma, Algeria, 26–27 November 2018; pp. 1–5. [Google Scholar]
- Ahmed, N.; Natarajan, T.; Rao, K.R. Discrete cosine transform. IEEE Trans. Comput. 1974, 100, 90–93. [Google Scholar] [CrossRef]
- Sufyanu, Z.; Mohamad, F.S.; Yusuf, A.A.; Mamat, M.B. Enhanced Face Recognition Using Discrete Cosine Transform. Eng. Lett. 2016, 24, 52–61. [Google Scholar]
- Nikolaev, N.; Gotchev, A.; Egiazarian, K.; Nikolov, Z. Suppression of electromyogram interference on the electrocardiogram by transform domain denoising. Med. Biol. Eng. Comput. 2001, 39, 649–655. [Google Scholar] [CrossRef]
- Raj, S.; Ray, K.C. ECG signal analysis using DCT-based DOST and PSO optimized SVM. IEEE Trans. Instrum. Meas. 2017, 66, 470–478. [Google Scholar] [CrossRef]
- Bousseljot, R.; Kreiseler, D.; Schnabel, A. Nutzung der EKG-Signaldatenbank CARDIODAT der PTB über das Internet. Biomed. Tech. 1995, 40, 317–318. [Google Scholar] [CrossRef]
- Van Alste, J.A.; Schilder, T.S. Removal of base-line wander and power-line interference from the ECG by an efficient FIR filter with a reduced number of taps. IEEE Trans. Biomed. Eng. 1985, BME-32, 1052–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, H.S.; Lee, C.; Lee, M. Ideal filtering approach on DCT domain for biomedical signals: Index blocked DCT filtering method (IB-DCTFM). J. Med. Syst. 2010, 34, 741–753. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Chandra, A. A new method for denoising ECG signal using sharp cut-off FIR filter. In Proceedings of the 2018 International Symposium on Devices, Circuits and Systems, Howrah, India, 29–31 March 2018. [Google Scholar]
- Goel, S.; Tomar, P.; Kaur, G. An optimal wavelet approach for ECG noise cancellation. Int. J. Bio-Sci. Bio-Technol. 2016, 8, 39–52. [Google Scholar] [CrossRef]
- Subbiah, S.; Patro, R.; Rajendran, K. Reduction of noises in ECG signal by various filters. Int. J. Eng. Res. Technol. 2014, 3, 656–660. [Google Scholar]
- Kichloo, A.; Haji, A.Q.; Kanjwal, K. Cardiac memory presenting as ST elevations following premature ventricular complex ablation. HeartRhythm Case Rep. 2021, 7, 52–55. [Google Scholar] [CrossRef]
- Farzam, K.; Richards, J.R. Premature Ventricular Contraction. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK532991/ (accessed on 18 May 2022).






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-C.; Chang, P.-C.; Tsai, P.-H. A Dual-Adaptive Approach Based on Discrete Cosine Transform for Removal of ECG Baseline Wander. Appl. Sci. 2022, 12, 8839. https://doi.org/10.3390/app12178839
Lin C-C, Chang P-C, Tsai P-H. A Dual-Adaptive Approach Based on Discrete Cosine Transform for Removal of ECG Baseline Wander. Applied Sciences. 2022; 12(17):8839. https://doi.org/10.3390/app12178839
Chicago/Turabian StyleLin, Chun-Chieh, Pei-Chann Chang, and Ping-Heng Tsai. 2022. "A Dual-Adaptive Approach Based on Discrete Cosine Transform for Removal of ECG Baseline Wander" Applied Sciences 12, no. 17: 8839. https://doi.org/10.3390/app12178839
APA StyleLin, C.-C., Chang, P.-C., & Tsai, P.-H. (2022). A Dual-Adaptive Approach Based on Discrete Cosine Transform for Removal of ECG Baseline Wander. Applied Sciences, 12(17), 8839. https://doi.org/10.3390/app12178839