
Recent Trends in the Diagnostic and Surgical Management of Benign Prostatic Hyperplasia in the U.S. from 2004 to 2017: Annual Changes in the Selection of Treatment Options and Medical Costs

 ,
,  , , ,
, , ,  , ,
, ,  , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shimizu, S.; Tsounapi, P.; Shimizu, T.; Honda, M.; Inoue, K.; Dimitriadis, F.; Saito, M. Lower urinary tract symptoms, benign prostatic hyperplasia/benign prostatic enlargement and erectile dysfunction: Are these conditions related to vascular dysfunction? Int. J. Urol. 2014, 21, 856–864. [Google Scholar] [PubMed]
- Das, A.K. Techniques and innovative technologies for the treatment of BPH. Can. J. Urol. 2019, 26, 1. [Google Scholar]
- Huang, S.W.; Tsai, C.Y.; Tseng, C.S.; Shih, M.C.; Yeh, Y.C.; Chien, K.L.; Pu, Y.S.; Tu, Y.K. Comparative efficacy and safety of new surgical treatments for benign prostatic hyperplasia: Systematic review and network meta-analysis. BMJ 2019, 367, l5919. [Google Scholar] [PubMed]
- Busetto, G.M.; Del Giudice, F.; D’Agostino, D.; Romagnoli, D.; Minervini, A.; Rocco, B.; Antonelli, A.; Celia, A.; Schiavina, R.; Cindolo, L.; et al. Efficacy and safety of Finasteride (5 alpha-reductase inhibitor) monotherapy in patients with benign prostatic hyperplasia: A critical review of the literature. Arch. Ital. Urol. Androl. 2020, 91, 205–210. [Google Scholar] [CrossRef]
- Kim, J.H.; Shim, S.R.; Khandwala, Y.; Del Giudice, F.; Sorensen, S.; Chung, B.I. Risk of Depression after 5 Alpha Reductase Inhibitor Medication: Meta-Analysis. World J. Men’s Health 2020, 38, 535–544. [Google Scholar] [CrossRef]
- Busetto, G.M.; Del Giudice, F.; Maggi, M.; Antonini, G.; D’Agostino, D.; Romagnoli, D.; Del Rosso, A.; Giampaoli, M.; Corsi, P.; Palmer, K.; et al. Surgical blood loss during holmium laser enucleation of the prostate (HoLEP) is not affected by short-term pretreatment with dutasteride: A double-blind placebo-controlled trial on prostate vascularity. Aging 2020, 12, 4337–4347. [Google Scholar] [CrossRef]
- 7. EAU Guidelines. Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Ob-struction (BPO) E. Available online: https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts (accessed on 1 August 2022).
- Gravas, S. Hot Topics in the Clinical Practice Guidelines for Treatment of Male Lower Urinary Tract Symptoms due to Benign Prostatic Obstruction. Eur. Urol. Focus 2022, 8, 396–398. [Google Scholar] [CrossRef]
- Salciccia, S.; Del Giudice, F.; Maggi, M.; Eisenberg, M.L.; Chung, B.I.; Conti, S.L.; Kasman, A.M.; Vilson, F.L.; Ferro, M.; Lucarelli, G.; et al. Safety and Feasibility of Outpatient Surgery in Benign Prostatic Hyperplasia: A Systematic Review and Meta-Analysis. J. Endourol. 2021, 35, 395–408. [Google Scholar] [CrossRef]
- DeWitt-Foy, M.E.; Gill, B.C.; Ulchaker, J.C. Cost Comparison of Benign Prostatic Hyperplasia Treatment Options. Curr. Urol. Rep. 2019, 20, 45. [Google Scholar] [CrossRef]
- Chung, K.J.; Kim, J.H.; Min, G.E.; Park, H.K.; Li, S.; Del Giudice, F.; Han, D.H.; Chung, B.I. Changing Trends in the Treatment of Nephrolithiasis in the Real World. J. Endourol. 2019, 33, 248–253. [Google Scholar] [CrossRef]
- Cheung, H.; Wang, Y.; Chang, S.L.; Khandwala, Y.S.; Del Giudice, F.; Chung, B.I. Adoption of Robot-Assisted Partial Nephrectomies: A Population-Based Analysis of U.S. Surgeons from 2004 to 2013. J. Endourol. 2017, 31, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, F.; van Uem, S.; Li, S.; Vilson, F.L.; Sciarra, A.; Salciccia, S.; Busetto, G.M.; Maggi, M.; Tiberia, L.; Viscuso, P.; et al. Contemporary Trends of Systemic Neoadjuvant and Adjuvant Intravesical Chemotherapy in Patients With Upper Tract Urothelial Carcinomas Undergoing Minimally Invasive or Open Radical Nephroureterectomy: Analysis of US Claims on Perioperative Outcomes and Health Care Costs. Clin. Genitourin. Cancer 2021, 20, 198.e1–198.e9. [Google Scholar] [CrossRef]
- Chung, B.I.; Leow, J.J.; Gelpi-Hammerschmidt, F.; Wang, Y.; Del Giudice, F.; De, S.; Chou, E.P.; Song, K.H.; Almario, L.; Chang, S.L. Racial Disparities in Postoperative Complications After Radical Nephrectomy: A Population-based Analysis. Urology 2015, 85, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.A.; Members of the Florey Adelaide Male Ageing Study; Haren, M.T.; Marshall, V.R.; Lange, K.; Wittert, G.A. Prevalence and factors associated with uncomplicated storage and voiding lower urinary tract symptoms in community-dwelling Australian men. World J. Urol. 2010, 29, 179–184. [Google Scholar] [CrossRef]
- Ng, M.; Baradhi, K.M. Benign Prostatic Hyperplasia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar] [PubMed]
- Stroup, S.P.; Palazzi-Churas, K.; Kopp, R.; Parsons, J.K. Trends in adverse events of benign prostatic hyperplasia (BPH) in the USA, 1998 to 2008. Br. J. Urol. 2011, 109, 84–87. [Google Scholar] [CrossRef]
- Capogrosso, P.; Capitanio, U.; Vertosick, E.A.; Ventimiglia, E.; Chierigo, F.; Oreggia, D.; Moretti, D.; Briganti, A.; Vickers, A.J.; Montorsi, F.; et al. Temporal Trend in Incidental Prostate Cancer Detection at Surgery for Benign Prostatic Hyperplasia. Urology 2018, 122, 152–157. [Google Scholar] [CrossRef]
- Busetto, G.M.; Giovannone, R.; Antonini, G.; Rossi, A.; Del Giudice, F.; Tricarico, S.; Ragonesi, G.; Gentile, V.; De Berardinis, E. Short-term pretreatment with a dual 5α-reductase inhibitor before bipolar transurethral resection of the prostate (B-TURP): Evaluation of prostate vascularity and decreased surgical blood loss in large prostates. Br. J. Urol. 2014, 116, 117–123. [Google Scholar] [CrossRef]
- Lokeshwar, S.D.; Harper, B.T.; Webb, E.; Jordan, A.; Dykes, T.A.; Neal, D.E., Jr.; Terris, M.K.; Klaassen, Z. Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Transl. Androl. Urol. 2019, 8, 529–539. [Google Scholar] [PubMed]
- Sønksen, J.; Barber, N.J.; Speakman, M.J.; Berges, R.; Wetterauer, U.; Greene, D.; Sievert, K.-D.; Chapple, C.R.; Montorsi, F.; Patterson, J.M.; et al. Prospective, Randomized, Multinational Study of Prostatic Urethral Lift Versus Transurethral Resection of the Prostate: 12-month Results from the BPH6 Study. Eur. Urol. 2015, 68, 643–652. [Google Scholar] [CrossRef]
- Ene, C.; Geavlete, P.; Geavlete, B. What’s new in bipolar TURP for surgical management of BPH? Chirurgia 2020, 115, 307–313. [Google Scholar]
- Michalak, J.; Tzou, D.; Funk, J. HoLEP: The gold standard for the surgical management of BPH in the 21(st) Century. Am. J. Clin. Exp. Urol. 2015, 3, 36–42. [Google Scholar] [PubMed]
- Horiuchi, A.; Muto, S.; Horie, S. Holmium laser enucleation of the prostate followed by high-intensity focused ultrasound treat-ment for patients with huge prostate adenoma and localized prostate cancer: 5-year follow-up. Prostate Int. 2016, 4, 49–53. [Google Scholar] [PubMed]
- Christidis, D.; McGrath, S.; Perera, M.; Manning, T.; Bolton, D.; Lawrentschuk, N. Minimally invasive surgical therapies for benign prostatic hypertrophy: The rise in minimally invasive surgical therapies. Prostate Int. 2017, 5, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Pettaway, C.A.; Lamerato, L.E.; Eaddy, M.T.; Edwards, J.K.; Hogue, S.L.; Crane, M.M. Benign prostatic hyperplasia: Racial differences in treatment patterns and prostate cancer prevalence. Br. J. Urol. 2011, 108, 1302–1308. [Google Scholar] [CrossRef]
- Braeckman, J.; Denis, L. Management of BPH then 2000 and now 2016–From BPH to BPO. Asian. J. Urol. 2017, 4, 138–147. [Google Scholar] [PubMed]
- Otto, B.; Barbieri, C.; Lee, R.; Te, A.E.; Kaplan, S.A.; Robinson, B.; Chughtai, B. Incidental Prostate Cancer in Transurethral Resection of the Prostate Specimens in the Modern Era. Adv. Urol. 2014, 2014, 627290. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number (n) | 770 | 1306 | 1762 | 2212 | 2942 | 3741 | 3920 | 4057 | 4305 | 4818 | 4344 | 4873 | 5827 | 6571 |
| Age (years), mean (std) | 67.6 (8.4) | 68.4 (8.2) | 69.3 (8.4) | 69.7 (8.5) | 70.4 (8.8) | 71 (8.7) | 71.3 (8.7) | 71.7 (8.6) | 71.9 (8.7) | 72 (8.6) | 72.6 (8.5) | 72.7 (8.6) | 72.9 (8.6) | 73.4 (8.4) |
| Race, n (%) | ||||||||||||||
| Asian | 18 (2.34) | 25 (1.91) | 27 (1.53) | 34 (1.54) | 63 (2.14) | 79 (2.11) | 80 (2.04) | 101 (2.49) | 115 (2.67) | 139 (2.89) | 132 (3.04) | 146 (3) | 170 (2.92) | 190 (2.89) |
| Black, non-Hispanic | 76 (9.87) | 97 (7.43) | 162 (9.19) | 149 (6.74) | 242 (8.23) | 305 (8.15) | 353 (9.01) | 332 (8.18) | 344 (7.99) | 357 (7.41) | 279 (6.42) | 342 (7.02) | 487 (8.36) | 579 (8.81) |
| Hispanic | 46 (5.97) | 86 (6.68) | 124 (7.04) | 144 (6.51) | 254 (8.63) | 391 (10.45) | 365 (9.31) | 373 (9.19) | 432 (10.03) | 470 (9.76) | 471 (10.84) | 500 (10.26) | 637 (10.93) | 704 (10.71) |
| White | 630 (81.82) | 1098 (84.07) | 1449 (82.24) | 1885 (85.22) | 2383 (81.00) | 2966 (79.28) | 3122 (79.64) | 3251 (80.13) | 3414 (79.3) | 3852 (79.95) | 3462 (79.7) | 3885 (79.73) | 4533 (77.79) | 5098 (77.58) |
| Household Incomes, n (%) | ||||||||||||||
| <USD 40K | 212 (27.53) | 342 (26.19) | 483 (27.41) | 616 (27.85) | 795 (27.02) | 1054 (28.18) | 1083 (27.63) | 1023 (25.22) | 1054 (24.48) | 1096 (22.75) | 963 (22.17) | 995 (20.42) | 1235 (21.19) | 1298 (19.75) |
| USD 40K–USD 49K | 66 (8.57) | 124 (9.49) | 150 (8.51) | 223 (10.08) | 263 (8.94) | 326 (8.72) | 343 (8.75) | 372 (9.17) | 397 (9.22) | 420 (8.72) | 336 (7.73) | 365 (7.49) | 476 (8.17) | 488 (7.43) |
| USD 50K–USD 59K | 61 (7.92) | 117 (8.96) | 162 (9.19) | 211 (9.54) | 289 (9.82) | 318 (8.5) | 364 (9.29) | 418 (10.3) | 397 (9.22) | 456 (9.46) | 379 (8.72) | 442 (9.07) | 518 (8.89) | 611 (9.3) |
| USD 60K–USD 74K | 93 (12.08) | 149 (11.41) | 213 (12.09) | 261 (11.8) | 341 (11.59) | 481 (12.86) | 508 (12.96) | 524 (12.92) | 520 (12.08) | 590 (12.25) | 573 (13.19) | 622 (12.76) | 783 (13.44) | 864 (13.15) |
| USD 75K–USD 99K | 128 (16.62) | 222 (17) | 284 (16.12) | 361 (16.32) | 479 (16.28) | 622 (16.63) | 632 (16.12) | 679 (16.74) | 757 (17.58) | 877 (18.2) | 802 (18.46) | 957 (19.64) | 1103 (18.93) | 1317 (20.04) |
| USD 100K+ | 210 (27.27) | 352 (26.95) | 470 (26.67) | 540 (24.41) | 775 (26.34) | 939 (25.11) | 990 (25.26) | 1041 (25.66) | 1180 (27.41) | 1379 (28.62) | 1291 (29.72) | 1492 (30.62) | 1712 (29.38) | 1993 (30.33) |
| Education | ||||||||||||||
| Less than 12th grade | <11 | <11 | <11 | <11 | 26 (0.88) | 29 (0.78) | 35 (0.89) | 18 (0.44) | 24 (0.56) | 26 (0.54) | 35 (0.81) | 32 (0.66) | 60 (1.03) | 35 (0.53) |
| High school diploma | 195 (25.32) | 293 (22.43) | 433 (24.57) | 578 (26.13) | 824 (28.01) | 1063 (28.42) | 1109 (28.29) | 1164 (28.69) | 1258 (29.45) | 1318 (27.36) | 1125 (25.9) | 1210 (24.83) | 1569 (26.93) | 1794 (27.3) |
| Less than bachelor’s degree | 444 (57.66) | 779 (59.65) | 1019 (57.83) | 1291 (58.36) | 1598 (54.32) | 2093 (55.96) | 2201 (56.15) | 2261 (55.73) | 2357 (54.75) | 2720 (56.45) | 2464 (56.72) | 2771 (56.86) | 3230 (55.43) | 3716 (56.55) |
| Bachelor’s degree plus | 100+ | 200+ | 200+ | 300+ | 494 (16.79) | 555 (14.84) | 575 (14.67) | 614 (15.13) | 656 (15.24) | 754 (15.65) | 720 (16.57) | 860 (17.65) | 968 (16.61) | 1026 (15.61) |
| Co-morbidity, n (%) | ||||||||||||||
| Hypertension | 667 (86.62) | 1153 (88.28) | 1554 (88.2) | 1943 (87.84) | 2570 (87.36) | 3286 (87.84) | 3398 (86.68) | 3544 (87.36) | 3776 (87.71) | 4180 (86.76) | 3753 (86.4) | 4171 (85.59) | 4960 (85.12) | 5506 (83.79) |
| Heart disease | 480 (62.34) | 844 (64.62) | 1144 (64.93) | 1442 (65.19) | 1842 (62.61) | 2364 (63.19) | 2444 (62.35) | 2549 (62.83) | 2647 (61.49) | 2857 (59.3) | 2584 (59.48) | 2857 (58.63) | 3381 (58.02) | 3604 (54.85) |
| Diabetes | 299 (38.83) | 504 (38.59) | 697 (39.56) | 898 (40.6) | 1176 (39.97) | 1567 (41.89) | 1689 (43.09) | 1708 (42.1) | 1791 (41.6) | 2052 (42.59) | 1794 (41.3) | 2018 (41.41) | 2363 (40.55) | 2578 (39.23) |
| Circulatory system diseases | 411 (53.38) | 712 (54.52) | 939 (53.29) | 1179 (53.3) | 1474 (50.1) | 1898 (50.74) | 1933 (49.31) | 2007 (49.47) | 2105 (48.9) | 2263 (46.97) | 2030 (46.73) | 2128 (43.67) | 2536 (43.52) | 2674 (40.69) |
| Prostate cancer | 153 (19.87) | 227 (17.38) | 344 (19.52) | 357 (16.14) | 464 (15.77) | 499 (13.34) | 480 (12.24) | 475 (11.71) | 443 (10.29) | 498 (10.34) | 458 (10.54) | 453 (9.3) | 468 (8.03) | 380 (5.78) |
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
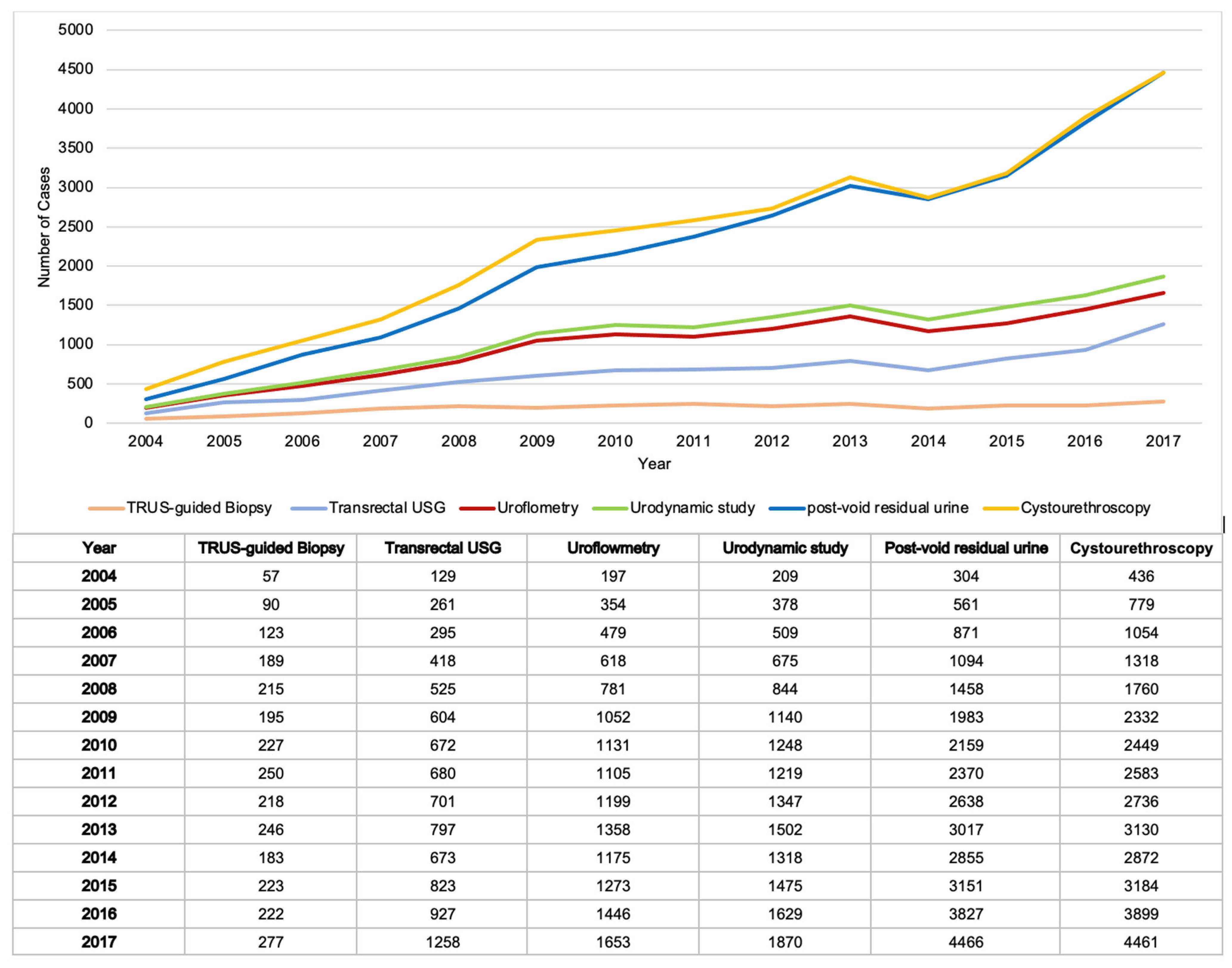
| Urodynamic study | ||||||||||||||
| number | 209 | 378 | 509 | 675 | 844 | 1140 | 1248 | 1219 | 1347 | 1502 | 1318 | 1475 | 1629 | 1870 |
| Cost (USD), median (IQR) | 24 (12–147) | 24 (13–147) | 24 (24–275) | 27 (24–318) | 26 (24–331) | 49 (24–331) | 65 (24–839) | 61 (24–856) | 79 (24–962) | 107 (24–1146) | 99 (14–1121) | 299 (19–1242) | 180 (14–1261) | 132 (14–1233) |
| Cystourethroscopy | ||||||||||||||
| number | 436 | 779 | 1054 | 1318 | 1760 | 2332 | 2449 | 2583 | 2736 | 3130 | 2872 | 3184 | 3899 | 4461 |
| Cost (USD), median (IQR) | 287 (287–305) | 287 (287–364) | 287 (287–364) | 287 (287–365) | 287 (287–364) | 287 (287–388) | 287 (287–384) | 287 (287–388) | 287 (287–384) | 324 (287–417) | 324 (324–409) | 324 (324–437) | 324 (324–437) | 324 (324–403) |
| Transrectal USG | ||||||||||||||
| number | 129 | 261 | 295 | 418 | 525 | 604 | 672 | 680 | 701 | 797 | 673 | 823 | 927 | 1258 |
| Cost (USD), median (IQR) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 152 (120–272) | 160 (152–263) | 160 (149–227) | 160 (148–193) | 160 (153–191) | 160 (160–171) |
| TRUS-guided biopsy | ||||||||||||||
| number | 57 | 90 | 123 | 189 | 215 | 195 | 227 | 250 | 218 | 246 | 183 | 223 | 222 | 277 |
| Cost (USD), median (IQR) | 338 (223–338) | 338 (338–338) | 338 (338–338) | 338 (338–338) | 338 (338–338) | 338 (338–338) | 338 (338–338) | 338 (278–338) | 338 (338–338) | 343 (338–343) | 343 (205–343) | 343 (343–343) | 343 (298–343) | 343 (177–343) |
| Uroflowmetry | ||||||||||||||
| number | 197 | 354 | 479 | 618 | 781 | 1052 | 1131 | 1105 | 1199 | 1358 | 1175 | 1273 | 1446 | 1653 |
| Cost (USD), median (IQR) | 35 (24–73) | 37 (24–61) | 46 (24–73) | 37 (24–73) | 48 (24–73) | 49 (24–97) | 49 (24–97) | 49 (24–97) | 49 (24–97) | 54 (28–97) | 55 (28–97) | 44 (28–84) | 47 (28–83) | 55 (28–94) |
| Post-void residual urine | ||||||||||||||
| number | 304 | 561 | 871 | 1094 | 1458 | 1983 | 2159 | 2370 | 2638 | 3017 | 2855 | 3151 | 3827 | 4466 |
| Cost (USD), median (IQR) | 29 (29–58) | 29 (29–58) | 29 (29–58) | 29 (29–58) | 29 (29–58) | 34 (29–58) | 44 (29–58) | 44 (29–66) | 44 (29–73) | 49 (32–81) | 49 (32–81) | 49 (32–81) | 49 (32–81) | 49 (32–81) |
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
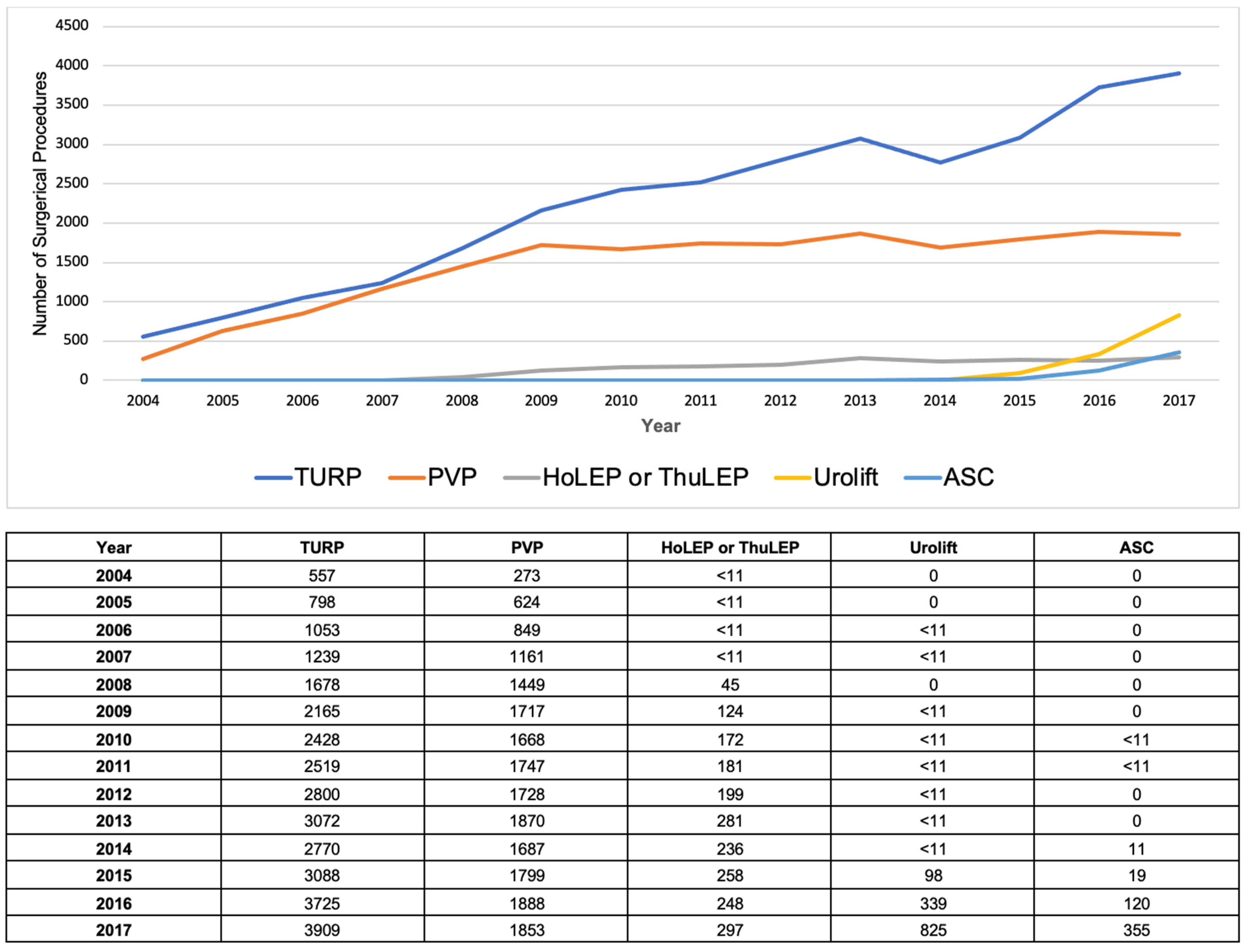
| TURP | ||||||||||||||
| number | 557 | 798 | 1053 | 1239 | 1678 | 2165 | 2428 | 2519 | 2800 | 3072 | 2770 | 3088 | 3725 | 3909 |
| Cost (USD), median (IQR) | 1321 (1321–1321) | 1321 (1321–1321) | 1321 (1321–1321) | 1321 (1321–1321) | 1321 (1321–1321) | 1321 (1321–1321) | 1321 (1321–1638) | 1321 (1321–2403) | 1321 (1321–2710) | 1321 (1321–3332) | 1459 (1321–3332) | 1459 (1252–3783) | 1459 (1459–3708) | 1459 (1459–4260) |
| PVP | ||||||||||||||
| number | 273 | 624 | 849 | 1161 | 1449 | 1717 | 1668 | 1747 | 1728 | 1870 | 1687 | 1799 | 1888 | 1853 |
| Cost (USD), median (IQR) | 1351 (1351–5999) | 1351 (1314–6382) | 1351 (1314–6412) | 1351 (1314–5742) | 1351 (1314–5694) | 1434 (1314–4763) | 1743 (1314–5318) | 2031 (1314–5318) | 2048 (1314–4921) | 2210 (1286–5335) | 2084 (1286–5335) | 2000 (1286–4862) | 2261 (1286–4692) | 2194 (1286–4988) |
| HoLEP or ThuLEP | ||||||||||||||
| number | <11 | <11 | <11 | <11 | 45 | 124 | 172 | 181 | 199 | 281 | 236 | 258 | 248 | 297 |
| Cost (USD), median (IQR) | 1393 (1393–6901) | 1393 (1393–6689) | 1404 (1393–6689) | 1410 (1393–5072) | 1419 (1393–5660) | 1419 (1419–5680) | 1419 (1419–5680) | 1419 (1419–4082) | 1419 (1419–5742) | 1419 (1419–6465) | ||||
| Urolift | ||||||||||||||
| number | 0 | 0 | <11 | <11 | 0 | <11 | <11 | <11 | <11 | <11 | <11 | 98 | 339 | 825 |
| Cost (USD), median (IQR) | 2867 (1642–4569) | 3284 (2193–4959) | 3284 (2517–5313) |
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
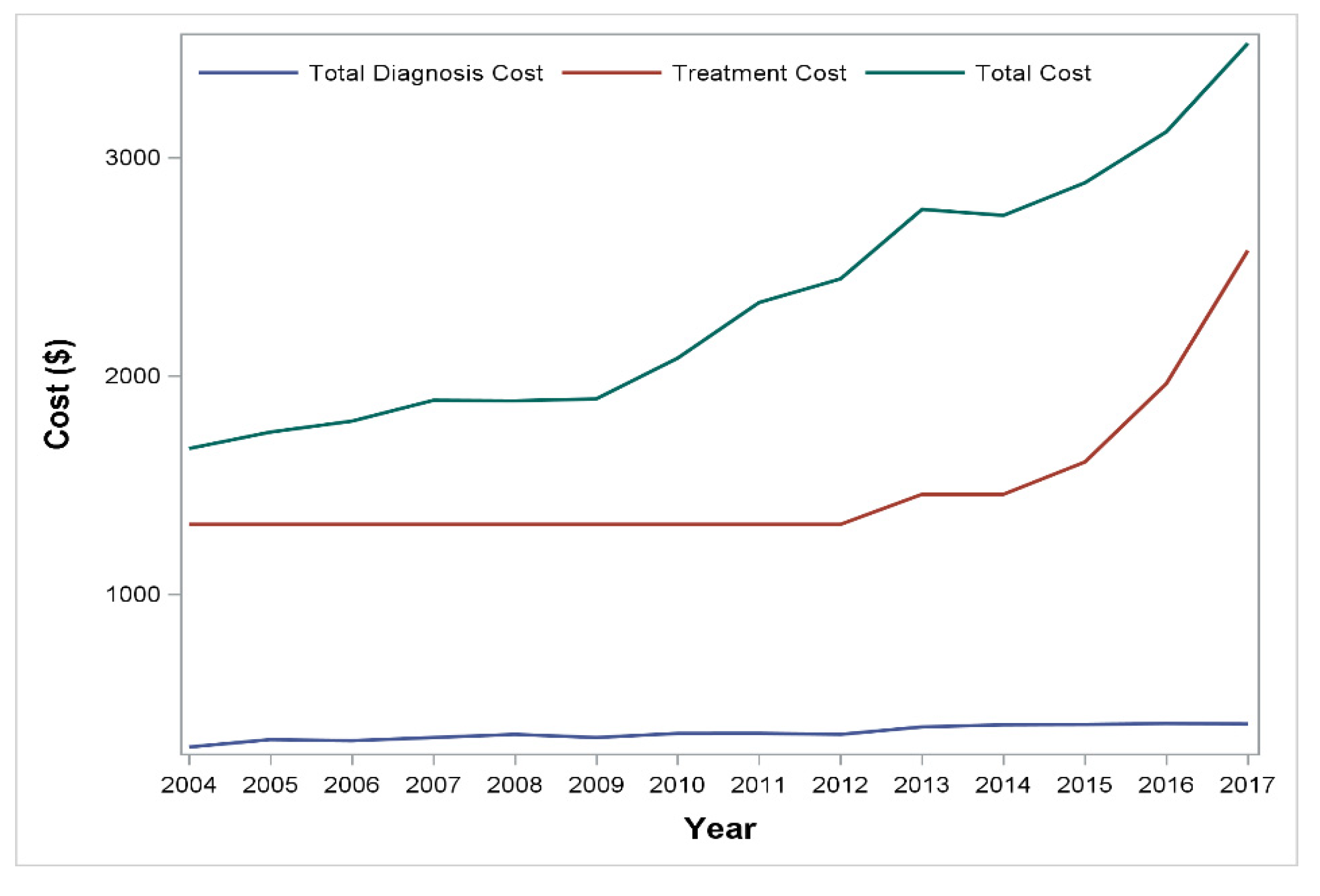
| Number of patients (n) | 770 | 1306 | 1762 | 2212 | 2942 | 3741 | 3920 | 4057 | 4305 | 4818 | 4344 | 4873 | 5827 | 6571 |
| Total cost, median (IQR) | 1668 (1350–2982) | 1743 (1379–4615) | 1794 (1380–4616) | 1889 (1459–4636) | 1887 (1457–4411) | 1895 (1416–4383) | 2082 (1490–4819) | 2337 (1589–5405) | 2445 (1576–5446) | 2763 (1609–6107) | 2735 (1610–6032) | 2885 (1643–6073) | 3118 (1738–6145) | 3523 (1799–6898) |
| Cost of treatment, median (IQR) | 1321 (1321–2635) | 1321 (1321–3267) | 1321 (1321–3895) | 1321 (1321–3812) | 1321 (1321–3507) | 1321 (1321–3542) | 1321 (1321–3678) | 1321 (1321–4283) | 1321 (1321–4372) | 1459 (1285–4879) | 1459 (1286–4929) | 1607 (1286–4861) | 1966 (1286–4994) | 2575 (1459–5665) |
| Cost of diagnosis, median (IQR) | 302 (88–484) | 336 (239–592) | 331 (224–630) | 345 (259–617) | 360 (268–651) | 345 (224–640) | 364 (242–846) | 364 (259–864) | 360 (220–902) | 394 (227–1013) | 403 (228–959) | 405 (244–1034) | 409 (279–962) | 407 (266–936) |
| Number of diagnoses | 615 | 1071 | 1468 | 1851 | 2397 | 3155 | 3334 | 3506 | 3769 | 4270 | 3893 | 4360 | 5192 | 5939 |
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients (n) | 57 | 92 | 91 | 16 | <11 | 12 | 20 | 26 | 29 | 191 | 239 | 263 | 310 | 341 |
| PSA (ng/mL), median (IQR) | 2.5 (1.1–5.2) | 1.8 (0.9–4.4) | 2.4 (1–5.1) | 3 (1.3–6) | 3.5 (1.1–5.8) | 3.2 (2.3–7) | 2.9 (1.5–5.5) | 1.6 (0.7–3.9) | 2.9 (1.7–5.6) | 2.4 (1.2–5) | 2.6 (1.4–5.5) | 2.6 (1.1–5.4) | 2.5 (1.2–4.9) | 2.7 (1.3–5.4) |
| Number of cancer detections | 16 | 14 | 18 | <11 | <11 | 0 | <11 | <11 | <11 | 21 | 34 | 21 | 30 | 15 |
| Percentage of cancer detection | 28.07 | 15.22 | 19.78 | 0 | 10.99 | 14.23 | 7.98 | 9.68 | 4.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Giudice, F.; Oh, J.K.; Basran, S.; Nicaise, E.; Song, P.H.; Kim, W.; Kim, S.Y.; Min, G.E.; Yoo, K.H.; Cho, H.J.; et al. Recent Trends in the Diagnostic and Surgical Management of Benign Prostatic Hyperplasia in the U.S. from 2004 to 2017: Annual Changes in the Selection of Treatment Options and Medical Costs. Appl. Sci. 2022, 12, 8697. https://doi.org/10.3390/app12178697
Del Giudice F, Oh JK, Basran S, Nicaise E, Song PH, Kim W, Kim SY, Min GE, Yoo KH, Cho HJ, et al. Recent Trends in the Diagnostic and Surgical Management of Benign Prostatic Hyperplasia in the U.S. from 2004 to 2017: Annual Changes in the Selection of Treatment Options and Medical Costs. Applied Sciences. 2022; 12(17):8697. https://doi.org/10.3390/app12178697
Chicago/Turabian StyleDel Giudice, Francesco, Jin Kyu Oh, Satvir Basran, Edouard Nicaise, Phil Hyun Song, Wansuk Kim, Sang Youn Kim, Gyeong Eun Min, Koo Han Yoo, Hyuk Jin Cho, and et al. 2022. "Recent Trends in the Diagnostic and Surgical Management of Benign Prostatic Hyperplasia in the U.S. from 2004 to 2017: Annual Changes in the Selection of Treatment Options and Medical Costs" Applied Sciences 12, no. 17: 8697. https://doi.org/10.3390/app12178697
APA StyleDel Giudice, F., Oh, J. K., Basran, S., Nicaise, E., Song, P. H., Kim, W., Kim, S. Y., Min, G. E., Yoo, K. H., Cho, H. J., Lee, S., Sciarra, A., Salciccia, S., De Berardinis, E., Asero, V., Scornajenghi, C. M., Pradere, B., Krajewski, W., Gallioli, A., ... Chung, B. I. (2022). Recent Trends in the Diagnostic and Surgical Management of Benign Prostatic Hyperplasia in the U.S. from 2004 to 2017: Annual Changes in the Selection of Treatment Options and Medical Costs. Applied Sciences, 12(17), 8697. https://doi.org/10.3390/app12178697