1. Introduction
Nasotracheal intubation (NTI) is one of the most common techniques used in various maxillo-facial surgery procedures. During this type of intubation, a good and clear view in the oral cavity is possible. In most cases, a tracheal tube is inserted through the nose to enable a safe and accurate view of the oral cavity [
1,
2]. After achieving good ventilation during surgery, it is essential to enable a good, stable position of the tube. When clear visibility towards the oral cavity is necessary, NTI remains the approach of choice. There are a lot of methods of tube positioning, which are related not only to its safe position in the nasal cavity but also to reducing its bending, perforation or cuff leak, or possible extubation and avoiding any nasal cavity injury from its compression towards the nasal septum, ala, conchae, or nasal tip [
3,
4,
5,
6]. Secondly, a good position of the NTI might greatly impact the time of surgery, mostly because of accurate patient oxidation and evaluation of the value of the capnometry.
In some special cases, with a difficult airway, either endoscopic-guided assisted intubation or videolaryngoscopy or other methods may be helpful. Still, tracheostomy remains the choice of last resort if no adequate intubation and support of adequate airways conditions can be met [
1,
2,
3,
7]. Despite either nasal or orotracheal intubation techniques, the main principle is still focused on proper tube positioning in a safe and accurate position to maintain both patient safety and adequate cooperation between the anesthesiologists and surgeons.
In NTI, a dedicated northern NTI tube can be used, with the same result as a normal NTI tube; however, too much tube bending and flexing might cause some problems with maintaining good patient ventilation. In this case, the authors quite often use, and highly recommend, the usage of the northern tube for maintaining its proper shape and decreasing the possibility of inadequate patient ventilation. In order to reduce this fact, the nasotracheal cuff should remain in the symmetry line of the patient’s body midline on the forehead. This position is granted with the adequate support of a sponge under it. Many different sponges, foams, or other elastic devices can be used to support a passive nasotracheal tube position on the patient’s forehead, including medical cloth plaster to fix both the sponge and the tube onto the desired position on the patient’s forehead. The authors use a heel anti-bedsore prophylactic sponge.
The authors would like to present their own modified positioning of the NTI tube for various maxillo-facial surgeries, with a particular focus here on mandibular asymmetry correction when a detailed view of the surrounding anatomical landmarks is necessary to visualize the scope of the asymmetry correction and the adequate titanium plate and screw fixation.
2. Case Description
During preparation for surgery, the patient’s position on the operating table should be comfortable, especially for long-lasting procedures. Anti-bedsore prophylaxis is mandatory. Various equipment is used in the operating rooms. In the author’s operating room, anti-bedsore round discs are used with a good outcome to stabilize the safe position and comfort of the heels. Their second usage, with the authors’ modification, is used for tube stabilization. Halcamp
® 15 × 5 cm diameter polyurethane foam (Halcamp, Kąty-Wrocławskie, Poland) in a terry cover is used (
Figure 1). After removal of the cover, the foam is cut in half, and a “crown-like” shaped stabilizer is placed on the patient’s forehead, 1 cm above the horizontal line from the superior aspect of each scaphoid fossa ear lobe.
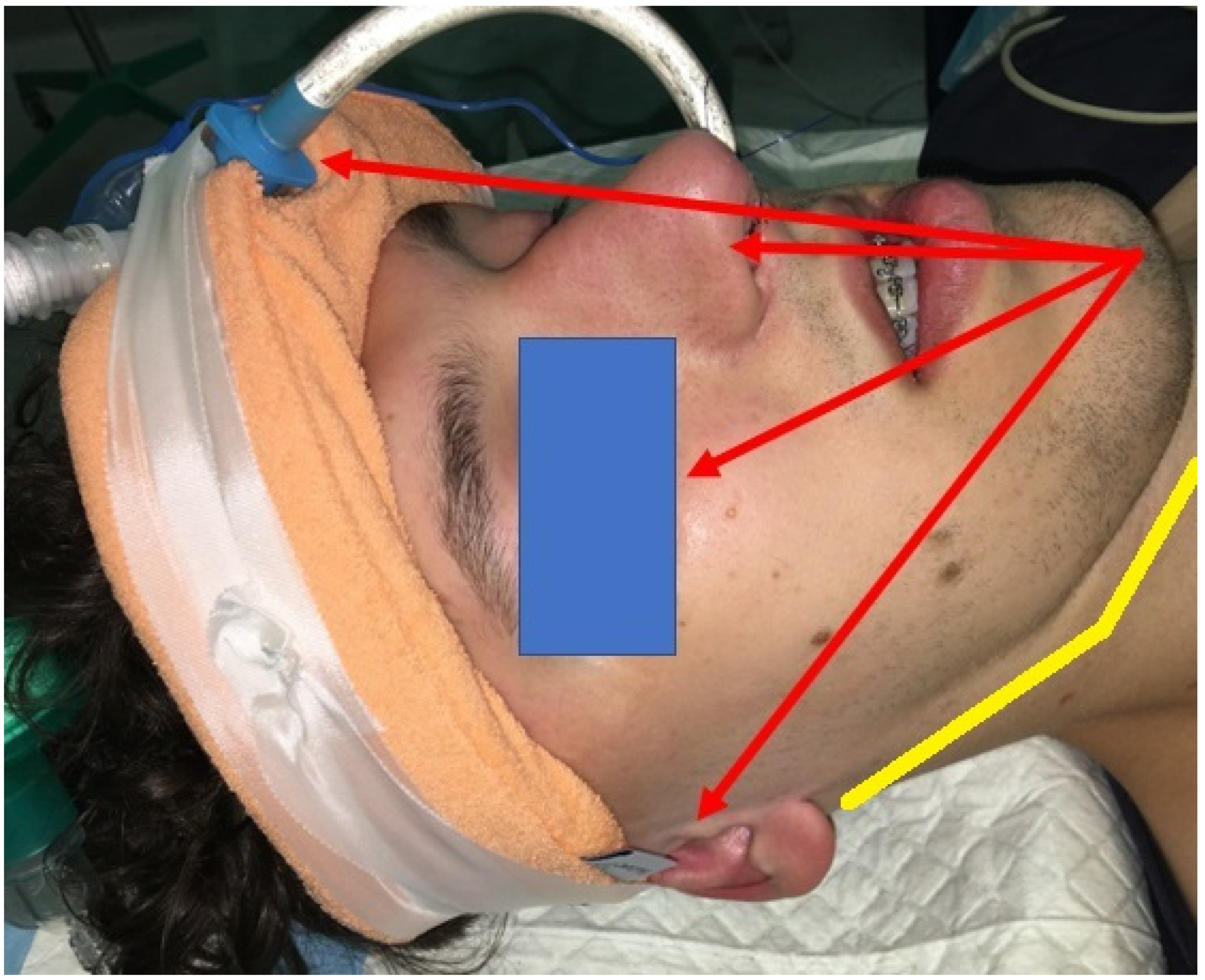
When the foam is situated on the patient’s forehead, about 1 cm superior to the eyebrow level, a medical cloth plaster is taped twice around the patient’s head just above the superior part of the ear, but inferiorly from the external occipital protuberance. After the following, the NTI tube can be either sutured with 2.0 nylon vertical mattress suture onto the nasal columella or just simply plastered; however, the authors advise suturing the tube with two vertical mattresses sutures. Later on, the tube cuff is placed directly on the sponge in the patient’s midline, and is, later on, taped again two times around the patient’s head. During the operation, a 6.0 nylon tarsorrhaphy is performed. This passive position of the tube is granted firstly by mattress sutures and then secondly by its taped position on the forehead foam (
Figure 2). With this, detailed visualization of the operating field is possible, especially in mandibular asymmetry correction. The main aim of this method is focused on full visualization of the important structures, as follows: (1) both ears with external auditory canals; (2) the inferior margins of the orbits; (3) the patient’s midline, which is not shifted because of the stable NTI tube position in the midline; (4) easy accessible pupils, to evaluate their shape and alignment (even after tarsorrhaphy, when the sutures are placed on surgical reins); (5) the nasal septum, which remains not shifted, and both mattress sutures stablize the NTI tube in the midline of the nasal columella without any traction of the nasal alae or deforming of the tip of the nose, and (6) at least 1 cm of the forehead above the eyebrows to estimate the vertical position of the asymmetrical mandible and also the maxillary bone.
After careful positioning of the NTI tube, the entire surgical field is rinsed and scrubbed with betadine solution. Sterile draping covers firstly the inferior field from the hyoid bone, then laterally behind both mandibular angles and both ear lobes. The third part of the draping covers the foam and is situated on the visible forehead. A fourth small part of the draping covers the superior part of the tube from the cuff towards half the diameter of the visible nasotracheal tube. Because of that, the entire surgical field is very much visible, which enables good surgical mandibular asymmetry correction.
Additional biomaterials and supportive devices might include sterile tapes, Steri-Stip wound dressings, eye ointments, nasal catheters, or others, which are greatly related to the surgeons’ preferences and usage in the pre-operative settings.
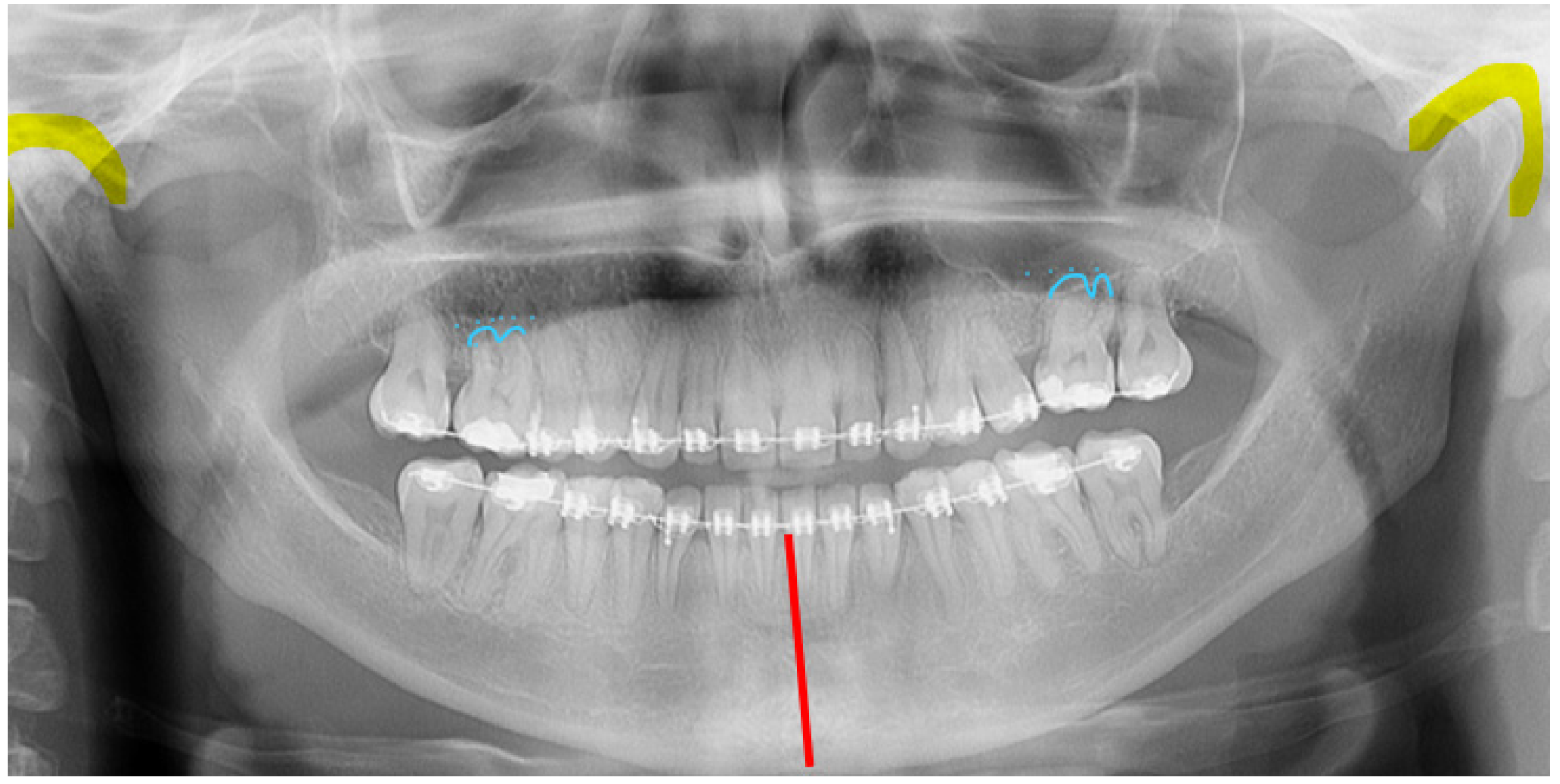
When the proper surgical field preparation is completed, and the safety of the intubation tube is secure, a surgical correction of the asymmetric mandible can be conducted. At first, after detailed planning, each patient is individually scheduled for one of the known and possible osteotomy protocols, which is greatly focused not only on full symmetry restoration but always on gaining a more balanced profile, an improved bite, occlusion, and a more symmetric facial contour. In the presented case of unilateral condylar hyperplasia (UCH), at first the patient had been scheduled for a corrective condylectomy because of active prolonged growth in the condyle. After that procedure, the patient was further treated orthodontically for orthognathic surgery (
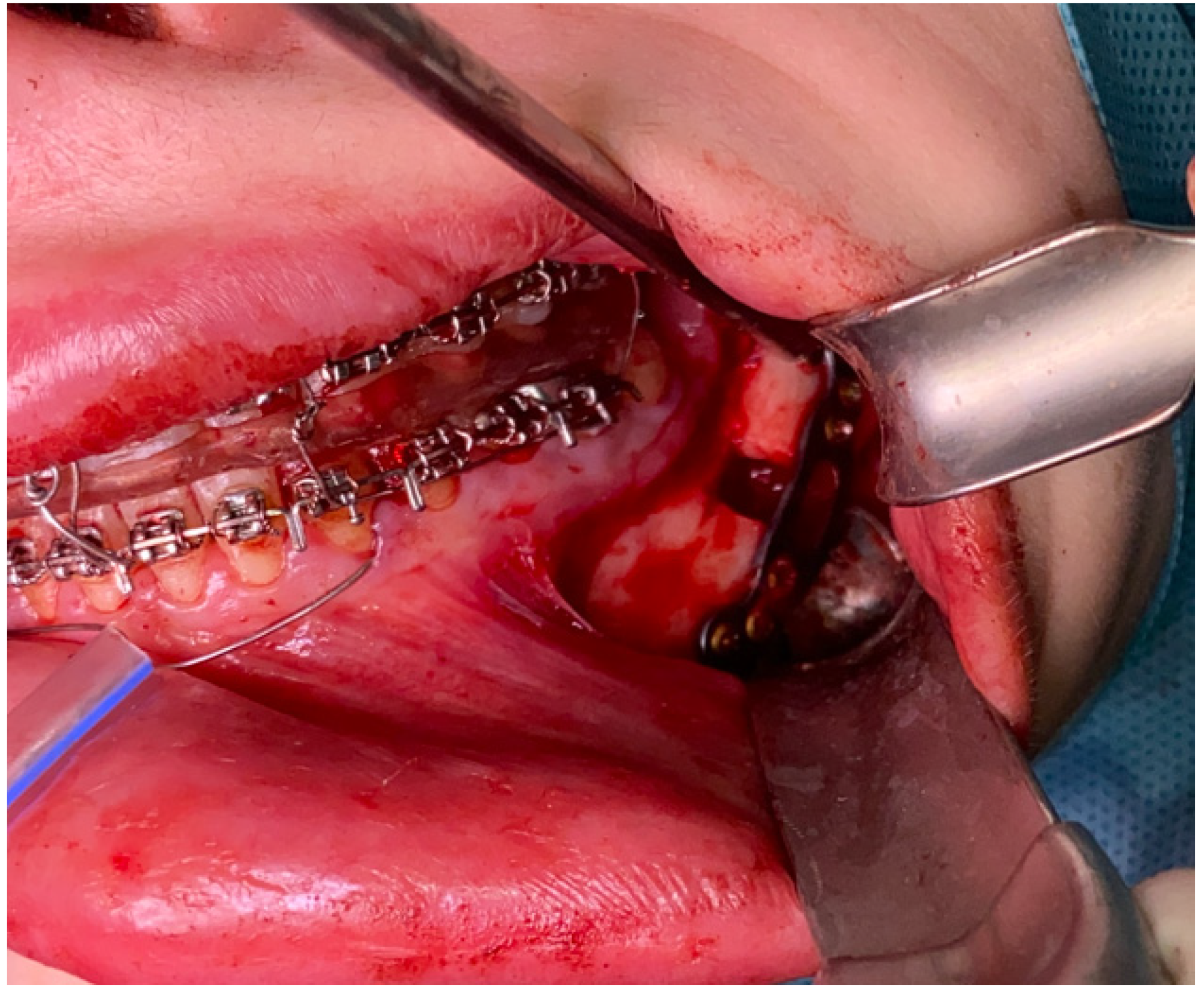
Figure 3). Because of a deviated maxillary plane and a downward position of the maxilla towards the affected right side of the asymmetric condylar overgrowth and a deviated mandibular midline towards the left healthy side, the patient was scheduled for a combined LeFort I and bilateral sagittal split osteotomy of the mandible (BSSO) osteotomy protocol. Under general anesthesia and NTI, the maxilla was advanced and rotated towards a new position. Secondly, the asymmetric mandible was rotated towards the right asymmetric overgrowth side and advanced. A new suitable position of the jaw bones was secured with titanium Modus 2.0 Orthognathic Plates from Medartis (Medartis, Basel, Switzerland) (
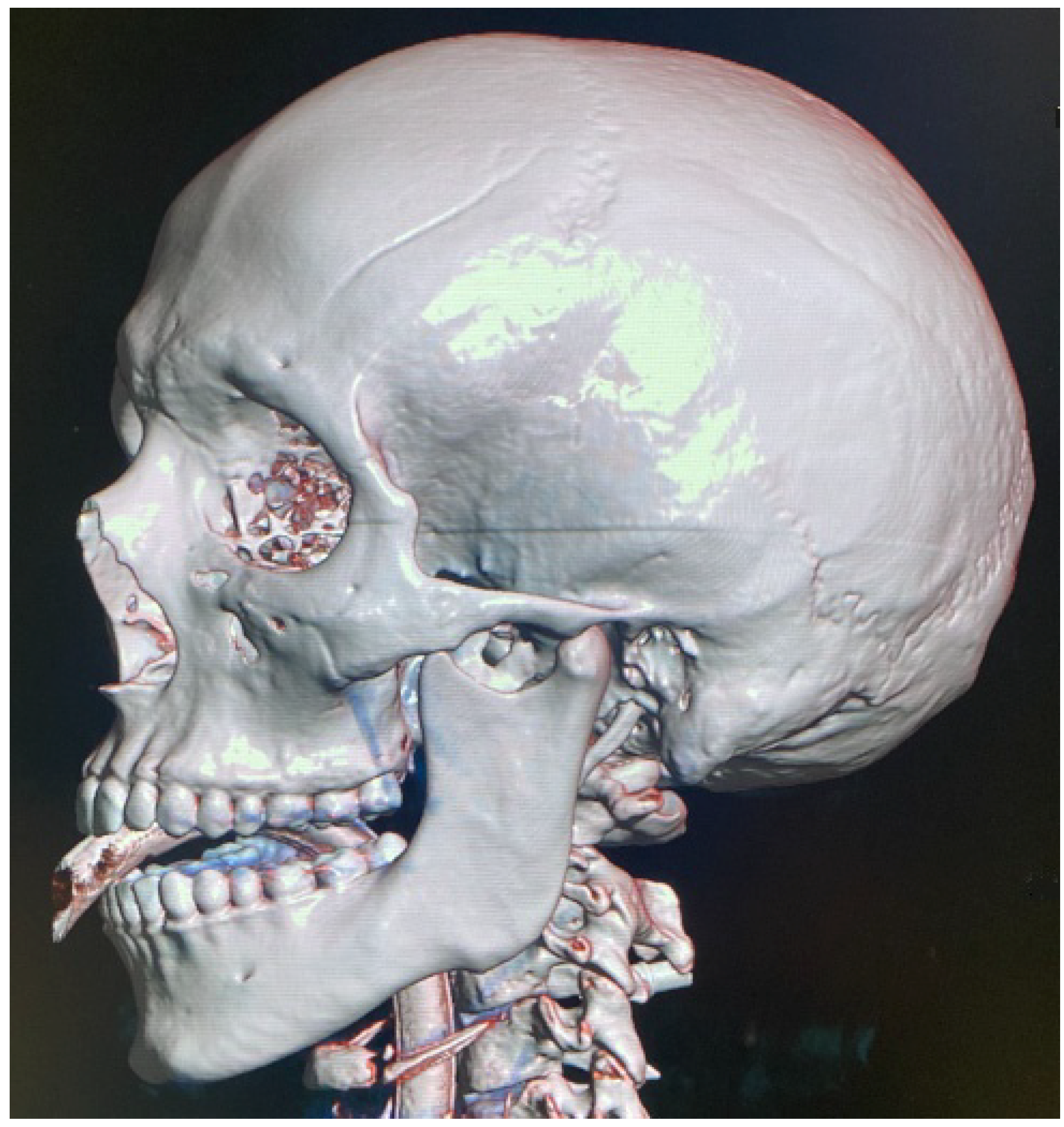
Figure 4). An additional bicortical 15 mm screw was used to secure the left mandibular basis because of its advancement and rotation (visible in the radiograph as an enlarged bone gap) (
Figure 5).
Similar approaches to an asymmetric mandible are quite known and common; however, because of various degrees of asymmetry, bone overgrowth, and the individuality of each case, the degree of the osteotomy protocols might be different. Maintaining a good view in the surgical field is mandatory. Good visualization of key features, such as the entire architecture of the mandible, the ear lobes, the nasal floor, and the inferior orbital rim, grants each surgeon some greater visualization, which helps in good planning for osteotomies and for accurate plate and screw fixation to enable a good final position. This approach helps to more clearly identify facial symmetry and to avoid any relapse or inadequate bite position.
3. Discussion
The necessity of adequate NTI tube placement and its secure positioning was modified over time when the advancement of various craniofacial surgeries developed [
3,
4,
5,
6]. Nowadays, the necessity of the NTI safe position is mostly related to not only long-lasting surgeries but also those relying on nasal tip symmetry, visualized maxillary and jaw bones, easy access to facial bones in trauma or tumor cases, and reducing possible complications from long surgeries, such as skin irritations, bedsores, nasal disfigurement, bleeding, or others [
7,
8,
9]. The usage of bandages, plasters, or other devices is helpful but also has its limitations, which are related to a wet environment, blood, the presence of hair, and the scope of the surgical field. Plasters of various sizes and fabrics are non-invasive methods, while additional tube suturing is considered an invasive approach [
10,
11]. It seems that classic orotracheal intubation is less demanding than NTI, especially in cases of its positioning (
Figure 6). Particularly in classical orotracheal intubation, the proper occlusion and bite cannot be evaluated and established properly [
10,
11,
12].
In cases that do not include orthognathic surgery, correction of skeletal malocclusion, or temporomandibular surgeries or those not requiring nasal intubation, classic orotracheal intubation can be used [
4,
5,
6,
7,
8,
9,
10,
11,
12]. Other methods of airway management might be troublesome and require some special devices and skills to perform them; however, they are also used either in surgical wards or in anesthesiology departments [
7,
8]. In cases of severe facial trauma, either submental intubation, presented first by Altemir et al. in 1986, or, alternatively, perhaps a classical surgical tracheostomy or percutaneous ones, presented by Griggs or Ciaglia, can be used [
7,
8,
9].
When successful nasotracheal intubation is achieved, in cases of long surgeries, with patients with difficult airways, or simply to maintain a good and stable position of the nasotracheal tube (without its flexion), many possibilities are known to stabilize the tube passively [
2,
3,
4,
5,
6,
7,
8,
9,
12]. Despite some plaster materials, bandages, special clamping devices, metal/plastic wires, splints, and others, there are many possibilities and alternatives for how to achieve a good and safe tube position [
8,
9,
10]. Furthermore, when a stable tube position is achieved, the better the view and the surgical field exposure that can be granted. This situation also influences the proper maxillo-mandibular complex bone cutting, titanium plate fixation, and overall orientation in a bigger field.
There are some interesting alternatives for intubation tube stabilization, especially those including NTI in craniofacial surgery procedures. Koshika et al. developed a 3D-printed fabricated device for proper nasotracheal tube placement [
6]. This method included a taping of the device onto the patient’s forehead while the surgical cap would remain safe and would not fall down or slide. A patient’s forehead remains a stable anatomical landmark. A study of 335 cases revealed good outcomes, with limited complications, which were related to small and local skin irritations, such as redness of the nasal ala caused by used plaster [
6]. On the other hand, Elias et al., in a 5-year observation study, investigated the usage of their own self-designed M-bent wire support form with additional U-shaped curved extremities [
10]. An additional turban-like cap and surgical compress with plasters helped to maintain safe NTI tube placement in maxilla-facial surgeries. The authors suggest that out of 197 cases in just 10 cases the escribed turban was loose and in just 6 cases the patients suffered from nasal hyperemia [
10]. Some authors suture the NTI tube onto the nasal septum with braided silk thread and use an additional rubber tube to help maintain proper anterior nares shape and oxygenation [
13]. Suturing the tube onto the nasal septum is a good and well-known method of tube supporting with a limited number of complications, which also is confirmed by the authors of the present study. Tube suturing might have various modifications with single, mattress, resorbable, or non-absorbable sutures of various sizes, and the nasal septum seems to be the best suitable place for this [
14]. It seems also that additional plasters are very much welcome and grant more suitable NTI placement than the standard endotracheal tube holders [
15]. Plasters alone are not sufficient to maintain safe NTI placement; so, as described here, an anti-bedsore heel disc combined with suturing towards the nasal septum and some additional plasters seems a reasonable proposal. Presented here are additional plasters, which are longer, wider, and set in more layers and are safer, which is also confirmed by other studies on adhesive plasters [
16,
17]. A study by Wagner et al. on extubation force evaluated seven different methods of fixation techniques and concluded that fixation devices should be designed in such detail as to reduce possible extubation [
16].
Some other special attention should be focused on the additional devices helpful in NTI tube stabilization. As described by Bhat et al., the usage of infant feeding tubes is quite interesting. A presented elastic feeding tube encircled the nasal septum and was sutured with a loose knot at the base of the nasal columella [
18]. Both fixations, with either plasters or bandages, are quite good; however, their usage is mostly related to surgeons’ and anesthesiologists’ comfort and preferences. Some authors, such as Seyedhosseini et al., compared the efficiency and differences between fixed bandages and adhesive tapes [
19]. A studied group of 72 patients revealed no significant differences in unplanned extubation in the emergency department. This finding might be related to the sedated and calm patients without any ongoing surgery in the craniofacial area. Firstly and most importantly, the used devices are mostly also used to improve visibility in the operating field. Because of the various degree of surgical maneuvers around patients’ heads and the presence of blood, saliva, sweat, and other factors, the humidity of the area might influence the condition of the used plasters and bandages. The second factor related to the used plasters and bandages includes possible hair loss, occipital or frontal bone pain, ear irritations, skin abrasions, or others [
20,
21,
22,
23,
24].
Maintaining a stable NTI tube position is very important to avoid any unexpected situations which might be related to tube instability, inadequate ventilation, disrupted anatomical landmarks with nasal disfigurement, and tube ejecting. Furthermore, tube instability and its movement might additionally pull sterile draping within its undesired position and cause an unnecessary non-sterile environment. The used heel disc is not only cheap, easy to use, and accessible, but also very common in every surgical field, because of its prophylactic anti-bedsore usage in most operating rooms. Some authors use sterile scrubbing brushes, while others use special foams for many other surgical purposes, even for abdominal surgeries, burn treatments, or others. The main goal of the authors is focused not only on a good tube placement but also on achieving a full view of the operating field, especially during asymmetry correction or even more complicated osteotomies such as LeFort II-III.
Furthermore, a sterile environment during long-lasting surgeries is also desirable. Instead of suturing some parts of the draping onto the patients’ skin, a good layer-by-layer cover seems more efficient. The key point of the stable position of the tube lies not only in the correct passive tube position. A second most important part is a good position of the pilot balloon, which should be gently twisted and then passively sutured by a separate shot plaster onto the heel pad presented here.


 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





