
Environmental Efficiency Indices in the Public Hospital Sector: A Proposal

 , ,
, ,  ,
,  ,
, 
Abstract
:Featured Application
Abstract
1. Introduction
2. Methodology
2.1. Research Context
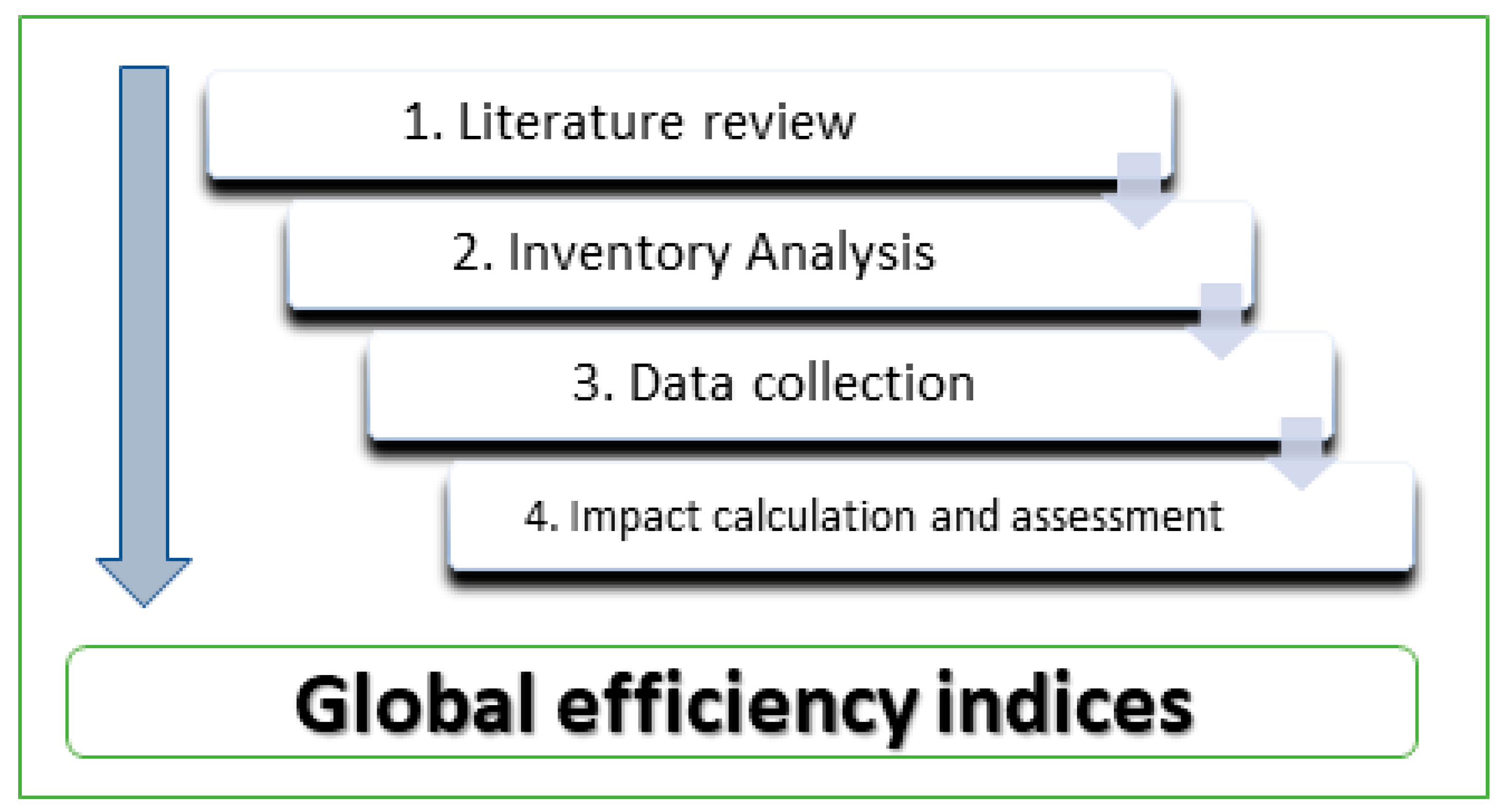
2.2. Methodology
2.2.1. Literature Review
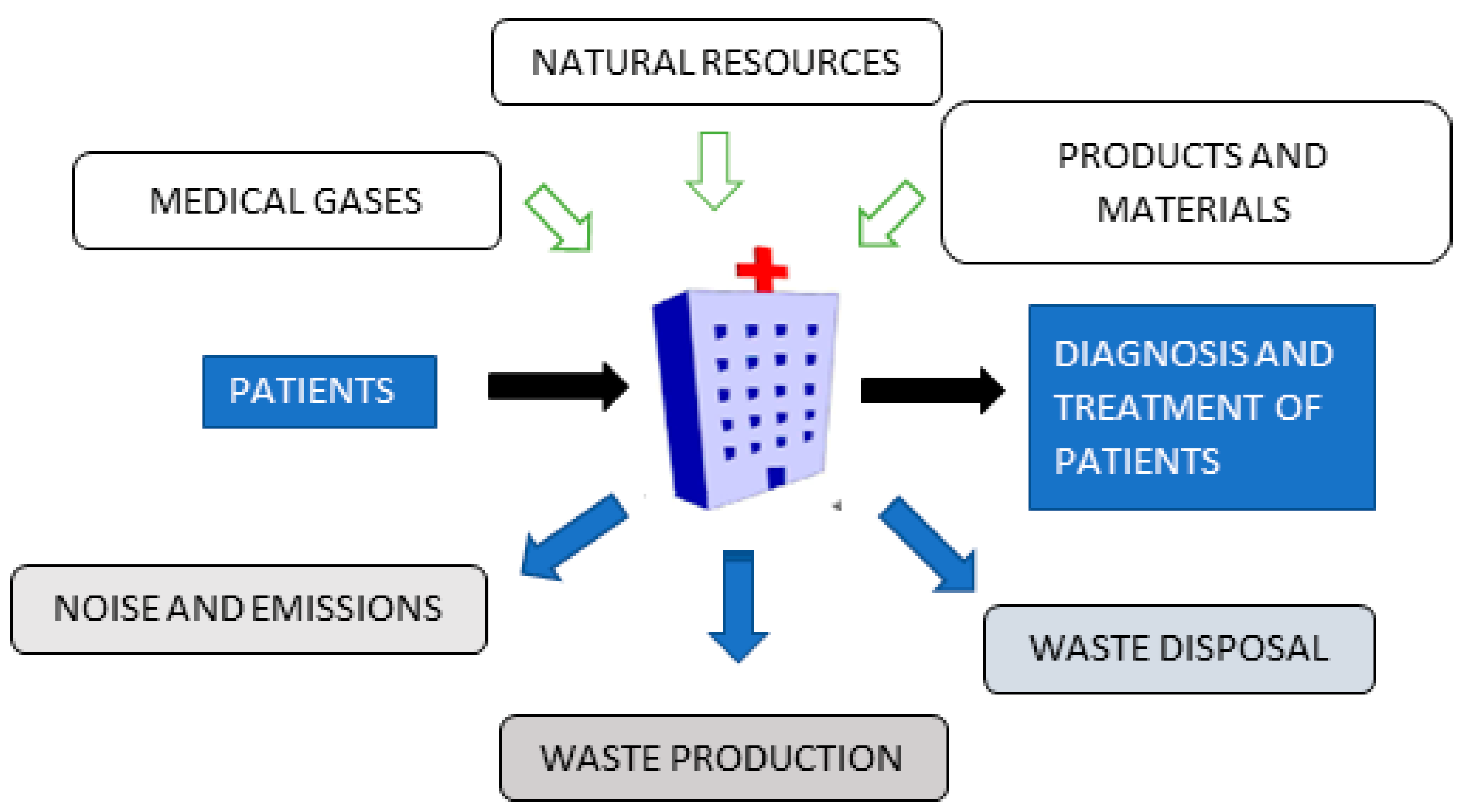
2.2.2. Inventory Analysis
2.2.3. Data Collection
2.2.4. Impact Calculation and Assessment
2.2.5. Calculation of the Environmental Efficiency Index (EEI)
3. Results and Discussion
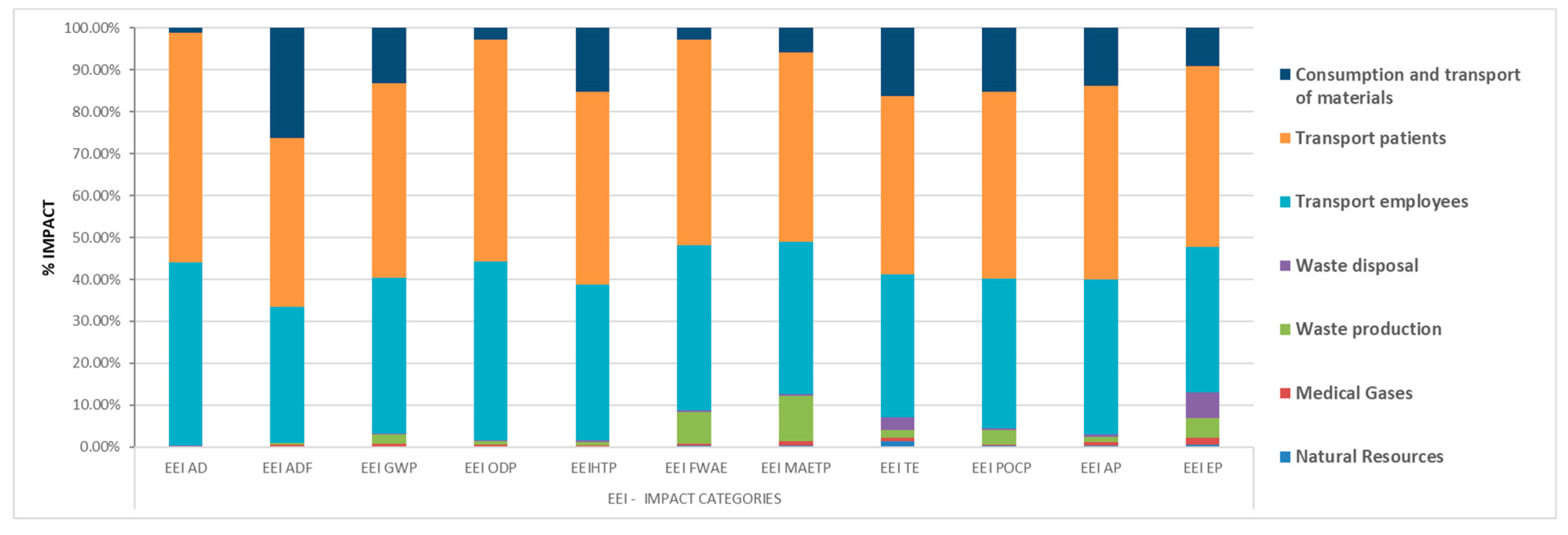
3.1. Global Efficiency Indices
3.1.1. Single-Value Global Environmental Efficiency Index
3.1.2. Environmental Efficiency Index per Category
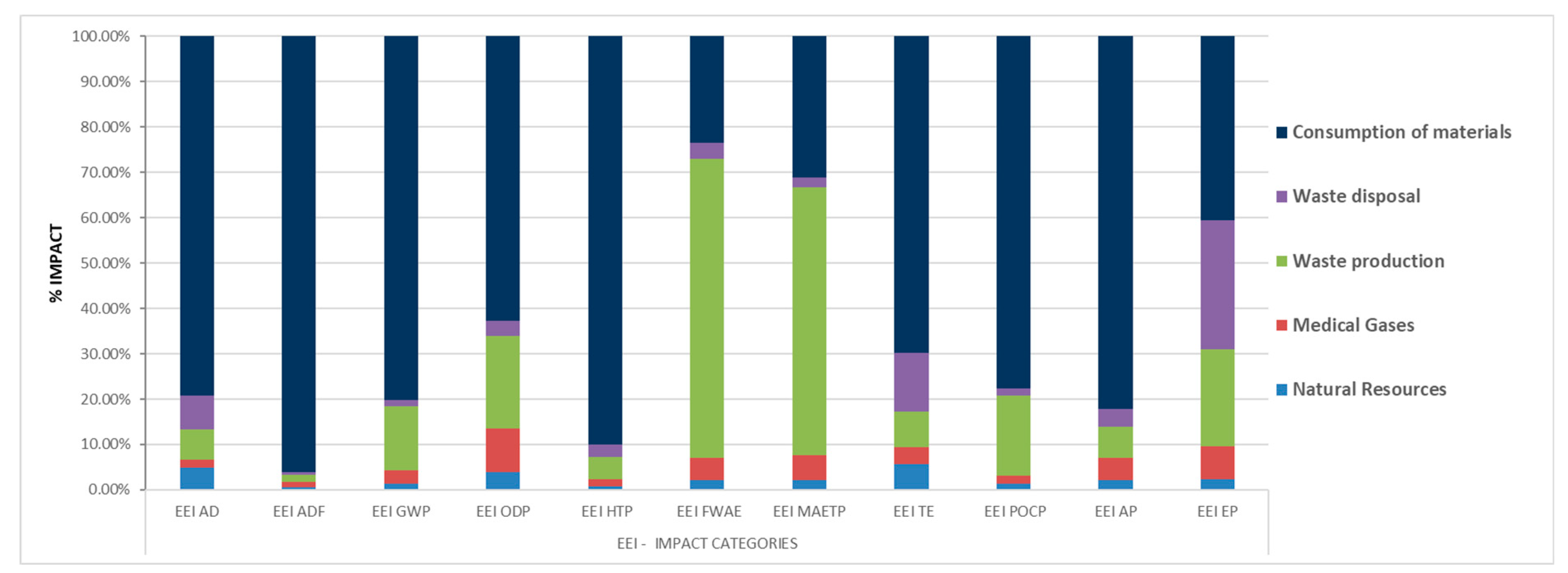
3.2. Study of Environmental Efficiency Indices of “Hospital Activity”
3.2.1. Single-Value Environmental Efficiency Index: “Hospital Activity”
3.2.2. Environmental Efficiency Index: “Hospital Activity” per Impact Categories
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LCA | Life cycle analysis |
| GDP | Gross domestic product |
| OECD | Organisation for Economic and Cooperation Development |
| WHO | World Health Organization |
| EMAS | Eco-Management and Audit Scheme |
| INSALUD | National Health Institute (Spanish) |
| HCU | Hospital complexity unit |
| DRG | Diagnosis-related group |
| AD | Abiotic depletion |
| ADF | Fossil depletion |
| GWP | Global warming potential for a 100-year time horizon |
| ODP | Ozone layer depletion |
| HTP | Human toxicity potential |
| FWAE | Fresh water aquatic ecotoxicity |
| MAETP | Marine aquatic ecotoxicity |
| TETP | Terrestrial ecotoxicity |
| POCP | Photochemical oxidant creation potential |
| AP | Acidification potential |
| EP | Eutrophication potential |
| EEI | Environmental Efficiency Index |
| GEEI | Global Environmental Efficiency Index |
References
- Davis, P.; Milne, B.; Parker, K.; Hider, P.; Lay-Yee, R.; Cumming, J.; Graham, P. Efficiency, effectiveness, equity (E3). Evaluating hospital performance in three dimensions. Health Policy 2013, 112, 19–27. [Google Scholar] [CrossRef]
- OECD. Health Spending; Organisation for Economic Cooperation and Development (OECD): Paris, France, 2019. [Google Scholar] [CrossRef]
- Villar, C.A.; Guadaño, M.d.B. Catalogo Nacional de Hospitales 2020; Ministry of Health: Madrid, Spain, 2020.
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K. Huella Climática del Sector de la Salud; Salud sin Daño: Buenos Aires, Argentina, 2019. [Google Scholar]
- Lalonde, M. A New Perspective on the Health of Canadians. 1974. Available online: www.phac-aspc.gc.ca/ph-sp/phdd/pdf/perspective.pdf (accessed on 18 January 2022).
- Amunjela, A.S.; De Kock, I.H.; Brent, A. Developing objective normalised metrics for comparing the energy use of hospitals. In Proceedings of the 26th International Association for Management of Technology Conference—IAMOT 2017, Vienna, Austria, 14–18 May 2017. [Google Scholar]
- Jain, N.; Burman, E.; Stamp, S.; Shrubsole, C.; Bunn, R.; Oberman, T.; Barrett, E.; Aletta, F.; Kang, J.; Raynham, P.; et al. Building performance evaluation of a new hospital building in the uk: Balancing indoor environmental quality and energy performance. Atmosphere 2021, 12, 115. [Google Scholar] [CrossRef]
- Bambarén-Alatrista, C. Environmental impact of a public hospital in the city of Lima, Peru. Rev. Peru. Med. Exp. Salud Publica 2014, 31, 712–715. [Google Scholar] [CrossRef]
- Rodríguez-Miranda, J.P.; García-Ubaque, C.A.; García-Vaca, M.C. Environmental management in public hospitals: Environmental management in Colombia. Rev. Fac. Med. 2016, 64, 621–624. [Google Scholar] [CrossRef]
- Pencheon, D. Developing a sustainable health care system: The United Kingdom experience. Med. J. Aust. 2018, 208, 284–285. [Google Scholar] [CrossRef]
- Jausovec, M.; Korpnik, N.; Gabrovec, B.; Klemencic, V.S. Siting of Healthcare Care Facilities Based on the Purpose of Their Operation, Demographic Changes, Environmental Characteristics, and the Impact on Public Health. Appl. Sci. 2022, 12, 379. [Google Scholar] [CrossRef]
- Organisation, U.N. Conferencia de las Naciones Unidas Sobre el Medio Ambiente y el Desarrollo; United Nations: New York, NY, USA, 1992. [Google Scholar]
- European Commission. Regulation (EC) No 1221/2009 of the European Parliament and of the Council of 25 November 2009 on the Voluntary Participation by Organisations in a Community Eco-Management and Audit Scheme (EMAS), Repealing Regulation (EC) No 761/2001 and Commission Decisions 2001/681/EC and 2006/193/EC; European Commission: Brussels, Belgium, 2009. [Google Scholar]
- Bambarén-Alatrista, C.; Alatrista-Gutiérrez, M.d.S. Huella de Carbono en Cinco Establecimientos de Salud del Tercer Nivel de Atención de Perú, 2013. Rev. Peru. Med. Exp. Salud Publica 2016, 33, 274–277. [Google Scholar] [CrossRef]
- Connor, A.; Lillywhite, R.; Cooke, M. The carbon footprint of a renal service in the United Kingdom. QJM Int. J. Med. 2010, 103, 965–975. [Google Scholar]
- Esmaeili, A.; McGuire, C.; Overcash, M.; Ali, K.; Soltani, S.; Twomey, J. Environmental impact reduction as a new dimension for quality measurement of healthcare services: The case of magnetic resonance imaging. Int. J. Health Care Qual. Assur. 2018, 31, 910–922. [Google Scholar] [CrossRef]
- Campion, N.; Thiel, C.L.; DeBlois, J.; Woods, N.C.; Landis, A.E.; Bilec, M.M. Life cycle assessment perspectives on delivering an infant in the US. Sci. Total Environ. 2012, 425, 191–198. [Google Scholar] [CrossRef]
- McAlister, S.; Grant, T.; McGain, F. An LCA of hospital pathology testing. Int. J. Life Cycle Assess. 2021, 26, 1753–1763. [Google Scholar] [CrossRef]
- Willskytt, S.; Tillman, A.M. Resource efficiency of consumables—Life cycle assessment of incontinence products. Resour. Conserv. Recycl. 2019, 144, 13–23. [Google Scholar] [CrossRef]
- Abd El-Salam, M.M. Hospital waste management in El-Beheira governorate, Egypt. J. Environ. Manag. 2010, 91, 618–629. [Google Scholar] [CrossRef]
- Ahmad, R.; Liu, G.; Santagata, R.; Casazza, M.; Xue, J.; Khan, K.; Nawab, J.; Ulgiati, S.; Lega, M. LCA of hospital solid waste treatment alternatives in a developing country: The case of district Swat, Pakistan. Sustainability 2019, 11, 3501. [Google Scholar] [CrossRef]
- Carino, S.; Porter, J.; Malekpour, S.; Collins, J. Environmental Sustainability of Hospital Foodservices across the Food Supply Chain: A Systematic Review. J. Acad. Nutr. Diet. 2020, 120, 825–873. [Google Scholar] [CrossRef] [PubMed]
- Eckelman, M.J.; Sherman, J. Environmental impacts of the U.S. health care system and effects on public health. PLoS ONE 2016, 11, e0157014. [Google Scholar] [CrossRef]
- Van Straten, B.; Ligtelijn, S.; Droog, L.; Putman, E.; Dankelman, J.; Weiland, N.H.S.; Horeman, T. A life cycle assessment of reprocessing face masks during the Covid-19 pandemic. Sci. Rep. 2021, 11, 17680. [Google Scholar] [CrossRef]
- Bałys, M.; Brodawka, E.; Korzeniewska, A.; Szczurowski, J.; Zarębska, K. LCA and economic study on the local oxygen supply in Central Europe during the COVID-19 pandemic. Sci. Total Environ. 2021, 786, 147401. [Google Scholar] [CrossRef]
- Zhao, H.; Liu, H.; Wei, G.; Wang, H.; Zhu, Y.; Zhang, R.; Yang, Y. Comparative life cycle assessment of emergency disposal scenarios for medical waste during the COVID-19 pandemic in China. Waste Manag. 2021, 126, 388–399. [Google Scholar] [CrossRef]
- Sisinno, C.; Moreira, J.C. Ecoefficiency: A tool to reduce solid waste production and waste of materials in health care units. Cad. Saude Publica 2005, 21, 1893–1900. [Google Scholar] [CrossRef]
- Silva, A.; Bernardes, R.S.; Moraes, L.; Reis, J. Criteria for definition of environmental contamination indicators related to solid waste from health care facilities: A proposal for evaluation. Cad. Saude Publica 2002, 18, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Andeobu, L.; Wibowo, S.; Grandhi, S. Medical Waste from COVID-19 Pandemic—A Systematic Review of Management and Environmental Impacts in Australia. Int. J. Environ. Res. Public Health 2022, 19, 1381. [Google Scholar] [CrossRef]
- Talibi, S.S.; Scott, T.; Hussain, R.A. The Environmental Footprint of Neurosurgery Operations: An Assessment of Waste Streams and the Carbon Footprint. Int. J. Environ. Res. Public Health 2022, 19, 5995. [Google Scholar] [CrossRef]
- European Commission. EMAS Statistics & Graphs. Available online: http://ec.europa.eu/environment/emas/emas_registrations/statistics_graphs_en.htm (accessed on 13 April 2022).
- Sanyé-Mengual, E.; Sala, S. Life Cycle Assessment support to environmental ambitions of EU policies and the Sustainable Development Goals. Integr. Environ. Assess. Manag. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gulcimen, S.; Aydogan, E.K.; Uzal, N. Life cycle sustainability assessment of a light rail transit system: Integration of environmental, economic, and social impacts. Integr. Environ. Assess. Manag. 2021, 17, 1070–1082. [Google Scholar] [CrossRef]
- Seifert, C.; Koep, L.; Wolf, P.; Guenther, E. Life cycle assessment as decision support tool for environmental management in hospitals: A literature review. Health Care Manag. Rev. 2021, 46, 12–24. [Google Scholar] [CrossRef]
- Observatory, N.R.S. Anuario Estadístico 2019; Directorate General for Traffic: Madrid, Spain, 2020.
- Alshqaqeeq, F.; Amin Esmaeili, M.; Overcash, M.; Twomey, J. Quantifying hospital services by carbon footprint: A systematic literature review of patient care alternatives. Resour. Conserv. Recycl. 2020, 154, 104560. [Google Scholar] [CrossRef]
- Huijbregts, M.A.J.; Steinmann, Z.J.N.; Elshout, P.M.F.; Stam, G.; Verones, F.; Vieira, M.; Zijp, M.; Hollander, A.; van Zelm, R. ReCiPe2016: A harmonised life cycle impact assessment method at midpoint and endpoint level. Int. J. Life Cycle Assess. 2017, 22, 138–147. [Google Scholar] [CrossRef]
- Malik, A.; Padget, M.; Carter, S.; Wakiyama, T.; Maitland-Scott, I.; Vyas, A.; Boylan, S.; Mulcahy, G.; Li, M.; Lenzen, M.; et al. Environmental impacts of Australia’s largest health system. Resour. Conserv. Recycl. 2021, 169, 105556. [Google Scholar] [CrossRef]
- Nicolet, J.; Mueller, Y.; Paruta, P.; Boucher, J.; Senn, N. What is the carbon footprint of primary care practices? A retrospective life-cycle analysis in Switzerland. Environ. Health Glob. Access Sci. Source 2022, 21, 3. [Google Scholar] [CrossRef]
- Zhao, W.; van der Voet, E.; Huppes, G.; Zhang, Y. Comparative life cycle assessments of incineration and non-incineration treatments for medical waste. Int. J. Life Cycle Assess. 2009, 14, 114–121. [Google Scholar] [CrossRef]
- IDAE. Estudio Sobre Hábitos y Actitudes de Los No Usuarios Habituales Hacia el Transporte Público Urbano Colectivo; IDAE: Madrid, Spain, 2017.
- Weisz, U.; Pichler, P.P.; Jaccard, I.S.; Haas, W.; Matej, S.; Bachner, F.; Nowak, P.; Weisz, H. Carbon emission trends and sustainability options in Austrian health care. Resour. Conserv. Recycl. 2020, 160, 104862. [Google Scholar] [CrossRef]
- Keller, R.L.; Muir, K.; Roth, F.; Jattke, M.; Stucki, M. From bandages to buildings: Identifying the environmental hotspots of hospitals. J. Clean. Prod. 2021, 319, 128479. [Google Scholar] [CrossRef]
- Martini, M.; Chiavaro Da Fonseca, R.; Voigt Severiano, L.; Garbin, H.I.; Flôres Da Rosa, T.; Klück, M. Hospital waste: Can we reduce the environmental impact of a large university hospital? Clin. Biomed. Res. 2017, 37, 288–294. [Google Scholar] [CrossRef]
- Schoen, J.; Chopra, V. The Harm We Do: The Environmental Impact of Medicine. J. Hosp. Med. 2018, 13, 353–355. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Unit | Quantity | |
|---|---|---|---|
| Natural Resources | Water | m3 | 29,917 |
| Electricity | MWh | 2865.29 | |
| Natural gas | MWh | 2767.35 | |
| Medical Gases | Oxygen | m3 | 28,432 |
| Medical air | m3 | 31,005 | |
| Nitrogen | m3 | 686 | |
| Waste Production | Waste | kg | 179,991.49 |
| Waste Disposal | Water | m3 | 29,038 |
| Transport | Employees | km | 6,648,422.4 |
| Patients | km | 8,274,345.4 | |
| Materials | km | 7101.6 | |
| Products and Materials | Disinfectants | kg | 2146.6 |
| Reagents | kg | 1323.2 | |
| Batteries | kg | 106.56 | |
| Paper | kg | 15,033 | |
| Toner | kg | 244.8 | |
| Plastic bags | kg | 5483 | |
| Gloves | kg | 11,275.5 | |
| Masks | kg | 456 | |
| Head and shoe covers | kg | 524 | |
| Gowns | kg | 8 | |
| Protection goggles | kg | 456 |
| Waste Production | Item |
|---|---|
| Group I—Urban assimilable wastes | Organic waste Glass Cardboard Paper Debris/wood/metal |
| Group II—Non-specific healthcare wastes | |
| Group III—Biohazardous healthcare wastes | Hospital waste Cytostatics |
| Group IV—Special healthcare wastes | Expired drugs Halogenated solvents Plates Contaminated packaging Electronic equipment Batteries Formaldehyde wastes |
| GEEI | |
|---|---|
| Natural Resources | 1.39 × 102 |
| Medicinal Gases | 2.91 × 102 |
| Wastes | 2.99 × 103 |
| Discharges | 1.69 × 102 |
| Means of Transport Used | 2.21 × 104 |
| Transport of Patients | 3.48 × 104 |
| Consumption of Materials | 1.57 × 101 |
| Indices | Total | Natural Resources | Medical Gases | Waste Production | Waste Disposal | Transport Employees | Transport Patients | Consumption Transport Mat. |
|---|---|---|---|---|---|---|---|---|
| EEIAD | 6.12 × 10−3 | 4.42 × 10−6 | 1.71 × 10−6 | 6.06 × 10−6 | 6.73 × 10−6 | 2.69 × 10−3 | 3.34 × 10−3 | 7.52 × 10−5 |
| EEIADF | 9.80 × 103 | 1.48 × 101 | 3.30 × 101 | 4.15 × 101 | 1.39 × 101 | 3.17 × 103 | 3.95 × 103 | 2.58 × 103 |
| EEIGWP100a | 6.22 × 102 | 1.35 × 10 | 3.11 × 10 | 1.43 × 101 | 1.51 × 10 | 2.31 × 102 | 2.88 × 102 | 8.25 × 101 |
| EEIODP | 8.16 × 10−5 | 1.30 × 10−7 | 3.14 × 10−7 | 6.70 × 10−7 | 1.07 × 10−7 | 3.48 × 10−5 | 4.33 × 10−5 | 2.18 × 10−6 |
| EEIHTP | 5.46 × 102 | 7.08 × 10−1 | 1.37 × 10 | 4.57 × 10 | 2.48 × 10 | 2.02 × 102 | 2.51 × 102 | 8.32 × 101 |
| EEIFWAE | 3.31 × 102 | 8.15 × 10−1 | 1.86 × 10 | 2.51 × 101 | 1.33 × 10 | 1.30 × 102 | 1.62 × 102 | 9.14 × 10 |
| EEIMAETP | 5.46 × 105 | 2.08 × 103 | 5.48 × 103 | 5.92 × 104 | 2.14 × 103 | 1.98 × 105 | 2.47 × 105 | 3.18 × 104 |
| EEITE | 1.05 × 10 | 1.39 × 10−2 | 8.77 × 10−3 | 1.90 × 10−2 | 3.18 × 10−2 | 3.57 × 10−1 | 4.45 × 10−1 | 1.71 × 10−1 |
| EEIPOCP | 1.64 × 10−1 | 4.06 × 10−4 | 5.92 × 10−4 | 5.66 × 10−3 | 5.02 × 10−4 | 5.88 × 10−2 | 7.32 × 10−2 | 2.52 × 10−2 |
| EEIAP | 1.99 × 10 | 6.93 × 10−3 | 1.62 × 10−2 | 2.26 × 10−2 | 1.30 × 10−2 | 7.37 × 10−1 | 9.18 × 10−1 | 2.72 × 10−1 |
| EEIEP | 6.51 × 10−1 | 3.26 × 10−3 | 1.04 × 10−2 | 3.09 × 10−2 | 4.05 × 10−2 | 2.26 × 10−1 | 2.81 × 10−1 | 5.93 × 10−2 |
| Indices | Transport of Patients (100% Private Vehicles) | Transport of Patients (45.7% Private Vehicles and 54.3% Public Transport) | Impact Reduction | Transport of Employees (100% Private Vehicles) | Transport of Employees (45.7% Private Vehicles and 54.3% Public Transport) | Impact Reduction | Transport of Employees (97.9% Private Vehicles and 2.1% Bicycles) | Impact Reduction |
|---|---|---|---|---|---|---|---|---|
| EEIAD | 3.34 × 10−3 | 1.97 × 10−3 | 41.02% | 2.69 × 10−3 | 1.58 × 10−3 | 41.26% | 2.63 × 10−3 | 2.23% |
| EEIADF | 3.95 × 103 | 2.54 × 103 | 35.70% | 3.17 × 103 | 2.04 × 103 | 35.65% | 3.11 × 103 | 1.89% |
| EEIGWP100a | 2.88 × 102 | 1.83 × 102 | 36.46% | 2.31 × 102 | 1.47 × 102 | 36.36% | 2.27 × 102 | 1.73% |
| EEIODP | 4.33 × 10−5 | 2.88 × 10−5 | 33.49% | 3.48 × 10−5 | 2.31 × 10−5 | 33.62% | 3.41 × 10−5 | 2.01% |
| EEIHTP | 2.51 × 102 | 1.28 × 102 | 49.00% | 2.02 × 102 | 1.03 × 102 | 49.01% | 1.98 × 102 | 1.98% |
| EEIFWAE | 1.62 × 102 | 8.24 × 101 | 49.14% | 1.30 × 102 | 6.62 × 101 | 49.08% | 1.28 × 102 | 1.54% |
| EEIMAETP | 2.47 × 105 | 1.28 × 105 | 48.18% | 1.98 × 105 | 1.03 × 105 | 47.98% | 1.95 × 105 | 1.52% |
| EEITE | 4.45 × 10−1 | 2.50 × 10−1 | 43.82% | 3.57 × 10−1 | 2.01 × 10−1 | 43.70% | 3.51 × 10−1 | 1.68% |
| EEIPOCP | 7.32 × 10−2 | 4.36 × 10−2 | 40.44% | 5.88 × 10−2 | 3.50 × 10−2 | 40.48% | 5.77 × 10−2 | 1.87% |
| EEIAP | 9.18 × 10−1 | 7.45 × 10−1 | 18.85% | 7.37 × 10−1 | 5.98 × 10−1 | 18.86% | 7.23 × 10−1 | 1.90% |
| EEIEP | 2.81 × 10−1 | 2.08 × 10−1 | 25.98% | 2.26 × 10−1 | 1.67 × 10−1 | 26.11% | 2.21 × 10−1 | 2.21% |
| GEEI | |
|---|---|
| Natural Resources | 1.39 × 102 |
| Medicinal Gases | 2.91 × 102 |
| Wastes | 2.99 × 103 |
| Discharges | 1.69 × 102 |
| Consumption of Materials | 1.49 × 101 |
| Indices | Total | Natural Resources | Medical Gases | Waste Production | Waste Disposal | Consumption of Materials |
|---|---|---|---|---|---|---|
| EEIAD | 9.11 × 10−5 | 4.42 × 10−6 | 1.71 × 10−6 | 6.06 × 10−6 | 6.73 × 10−6 | 7.23 × 10−5 |
| EEIADF | 2.67 × 103 | 1.48 × 101 | 3.30 × 101 | 4.15 × 101 | 1.39 × 101 | 2.57 × 103 |
| EEIGWP100a | 1.02 × 102 | 1.35 × 10 | 3.11 × 10 | 1.43 × 101 | 1.51 × 10 | 8.17 × 101 |
| EEIODP | 3.28 × 10−6 | 1.30 × 10−7 | 3.14 × 10−7 | 6.70 × 10−7 | 1.07 × 10−7 | 2.06 × 10−6 |
| EEIHTP | 9.20 × 101 | 7.08 × 10−1 | 1.37 × 10 | 4.57 × 10 | 2.48 × 10 | 8.29 × 101 |
| EEIFWAE | 3.81 × 101 | 8.15 × 10−1 | 1.86 × 10 | 2.51 × 101 | 1.33 × 10 | 8.96 × 10 |
| EEIMAETP | 1.00 × 105 | 2.08 × 103 | 5.48 × 103 | 5.92 × 104 | 2.14 × 103 | 3.13 × 104 |
| EEITE | 2.43 × 10−1 | 1.39 × 10−2 | 8.77 × 10−3 | 1.90 × 10−2 | 3.18 × 10−2 | 1.70 × 10−1 |
| EEIPOCP | 3.21 × 10−2 | 4.06 × 10−4 | 5.92 × 10−4 | 5.66 × 10−3 | 5.02 × 10−4 | 2.49 × 10−2 |
| EEIAP | 3.28 × 10−1 | 6.93 × 10−3 | 1.62 × 10−2 | 2.26 × 10−2 | 1.30 × 10−2 | 2.69 × 10−1 |
| EEIEP | 1.43 × 10−1 | 3.26 × 10−3 | 1.04 × 10−2 | 3.09 × 10−2 | 4.05 × 10−2 | 5.83 × 10−2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Lacarra, V.; Martínez-Cámara, E.; Santamaría-Peña, J.; Jiménez-Macías, E.; Bruzzone, A.; Blanco-Fernández, J. Environmental Efficiency Indices in the Public Hospital Sector: A Proposal. Appl. Sci. 2022, 12, 8120. https://doi.org/10.3390/app12168120
Jiménez-Lacarra V, Martínez-Cámara E, Santamaría-Peña J, Jiménez-Macías E, Bruzzone A, Blanco-Fernández J. Environmental Efficiency Indices in the Public Hospital Sector: A Proposal. Applied Sciences. 2022; 12(16):8120. https://doi.org/10.3390/app12168120
Chicago/Turabian StyleJiménez-Lacarra, Vanesa, Eduardo Martínez-Cámara, Jacinto Santamaría-Peña, Emilio Jiménez-Macías, Agostino Bruzzone, and Julio Blanco-Fernández. 2022. "Environmental Efficiency Indices in the Public Hospital Sector: A Proposal" Applied Sciences 12, no. 16: 8120. https://doi.org/10.3390/app12168120
APA StyleJiménez-Lacarra, V., Martínez-Cámara, E., Santamaría-Peña, J., Jiménez-Macías, E., Bruzzone, A., & Blanco-Fernández, J. (2022). Environmental Efficiency Indices in the Public Hospital Sector: A Proposal. Applied Sciences, 12(16), 8120. https://doi.org/10.3390/app12168120