
An In Vitro Study of the Reproducibility of the Drilling Access of Digitalized Surgical Guides Generated via Three Different Implant Planning Software Programs

Abstract
1. Introduction
2. Materials and Methods
2.1. Model Preparation
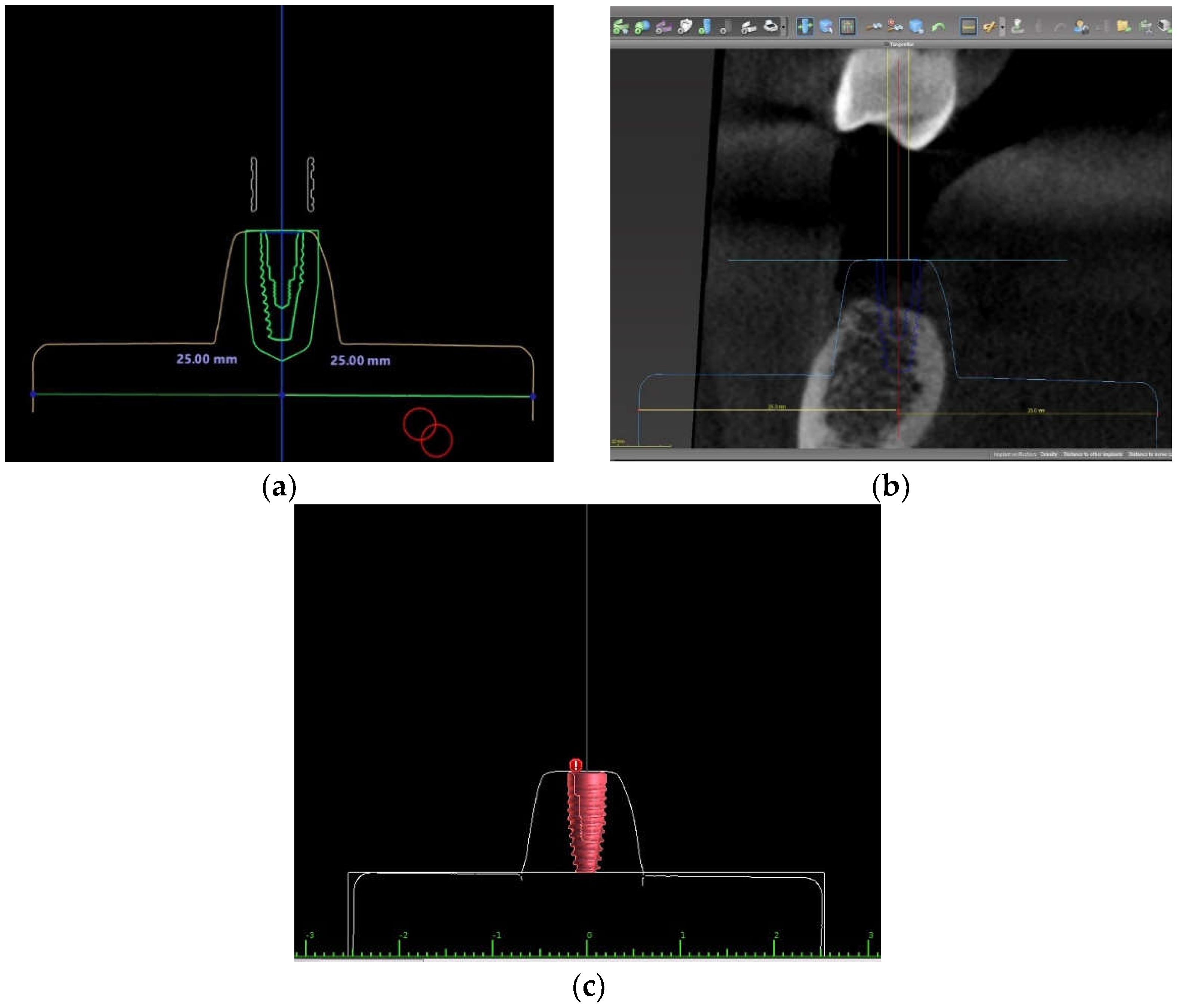
2.2. Implant Position Planning Procedure in Three Different Software Programs
2.3. Surgical Guide Design and Fabrication in Three Different Software Programs
2.4. Osteotomy and Implant Placement in the Study Model Process
2.5. Implant Position Accuracy Measurement
- Linear deviation from the implant platform: the linear displacement in mm between the planned and placed implants, measured at the center of the implant platform.
- Linear deviation from the implant apex: the linear displacement in mm between the planned and placed implants as measured at the center of the implant apex.
- Linear deviation of the implant depth: the depth deviation in mm between the planned and placed implants.
- Deviation of the implant axis or an angular deviation: the deviation in degrees (°) between the center axis line of the planned and placed implants.
2.6. Statistical Analysis
3. Results
3.1. The Deviation of the Placed Implant Related to the Planned Implant
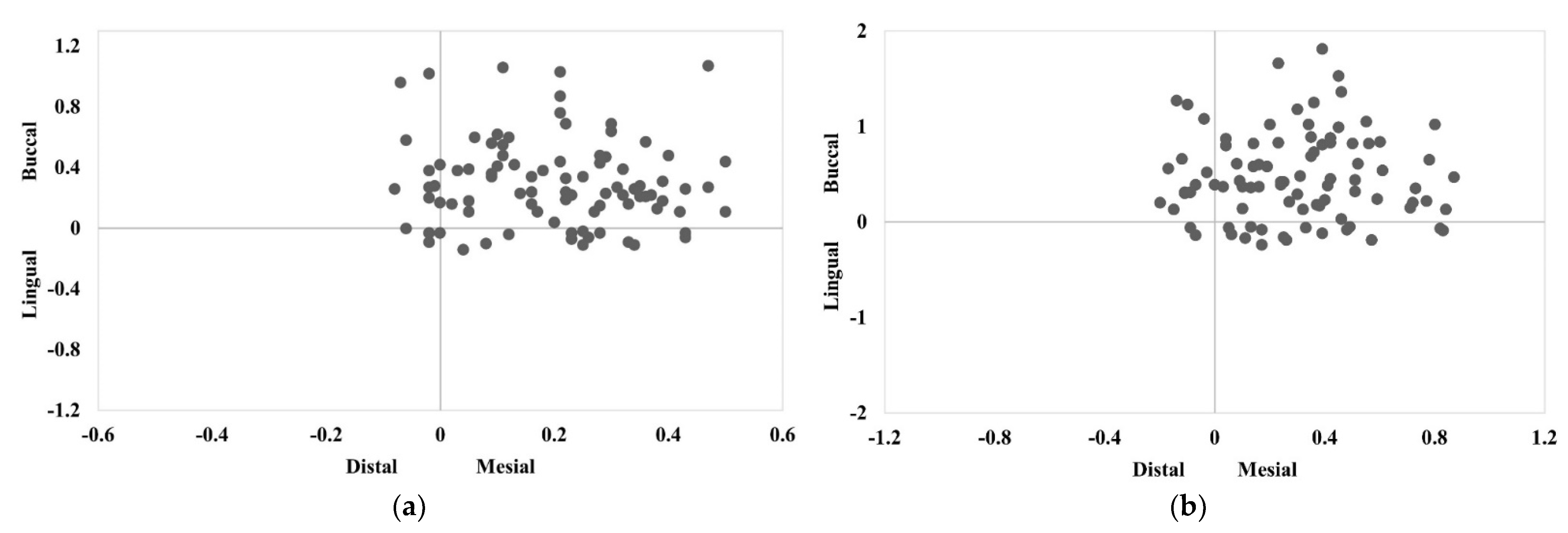
3.2. The Direction of the Buccolingual and Mesio-Distal Deviations of the Implant Position at the Implant Platform and Apex
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fortin, T.; Loup Coudert, J.; Champleboux, G.; Sautot, P.; Lavallée, S. Computer-assisted dental implant surgery using computed tomography. Comput. Aided Surg. 1995, 1, 53–58. [Google Scholar] [CrossRef]
- Katsoulis, J.; Pazera, P.; Mericske-Stern, R. Prosthetically driven, computer-guided implant planning for the edentulous maxilla: A model study. Clin. Implant. Dent. Relat. Res. 2008, 11, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Betensky, R.; Gianneschi, G.; Gallucci, G. Accuracy of digital versus conventional implant impressions. Clin. Oral Implant. Res. 2014, 26, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Somogyi-Ganss, E.; Holmes, H.; Jokstad, A. Accuracy of a novel prototype dynamic computer-assisted surgery system. Clin. Oral Implant. Res. 2015, 26, 882–890. [Google Scholar] [CrossRef]
- Widmann, G.; Bale, R. Accuracy in computer-aided implant surgery-A review. Int. J. Oral Maxillofac. Implant. 2006, 21, 305–313. [Google Scholar]
- Block, M.; Emery, R.; Lank, K.; Ryan, J. Implant placement accuracy using dynamic navigation. Int. J. Oral Maxillofac. Implant. 2016, 32, 92–99. [Google Scholar] [CrossRef]
- Brief, J.; Edinger, D.; Hassfeld, S.; Eggers, G. Accuracy of image-guided implantology. Clin. Oral Implant. Res. 2005, 16, 495–501. [Google Scholar] [CrossRef]
- Buser, D.; Janner, S.; Wittneben, J.; Brägger, U.; Ramseier, C.; Salvi, G. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: A retrospective study in 303 partially edentulous patients. Clin. Implant. Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral Maxillofac. Implant. 2004, 19, 43–61. [Google Scholar]
- Garber, D.A. The esthetic dental implant: Letting restoration be the guide. J. Am. Dent. Assoc. 1995, 126, 319–325. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29 (Suppl. 2014), 25–42. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, R.; Gherlone, E.F.; Calesini, G.; Zarone, F. Effect of implant angulation, connection length, and impression material on the dimensional accuracy of implant impressions: An in vitro comparative study. Clin. Implant. Dent. Relat. Res. 2010, 12 (Suppl. S1), e63–e76. [Google Scholar] [CrossRef] [PubMed]
- Canay, S.; Hersek, N.; Akpinar, I.; Aşik, Z. Comparison of stress distribution around vertical and angled implants with finite-element analysis. Quintessence Int. 1996, 27, 591–598. [Google Scholar] [PubMed]
- Lin, C.L.; Wang, J.C.; Ramp, L.C.; Liu, P.R. Biomechanical response of implant systems placed in the maxillary posterior region under various conditions of angulation, bone density, and loading. Int. J. Oral. Maxillofac. Implant. 2008, 23, 57–64. [Google Scholar]
- Saab, X.E.; Griggs, J.A.; Powers, J.M.; Engelmeier, R.L. Effect of abutment angulation on the strain on the bone around an implant in the anterior maxilla: A finite element study. J. Prosthet. Dent. 2007, 97, 85–92. [Google Scholar] [CrossRef]
- Rodrigues, V.; Tribst, J.; Santis, L.; Lima, D.; Nishioka, R. Influence of angulation and vertical misfit in the evaluation of micro-deformations around implants. Braz. Dent. Sci. 2017, 20, 32. [Google Scholar] [CrossRef]
- Rodrigues, V.; Tribst, J.; Santis, L.; Borges, A.; Nishioka, R. Biomechanical effect of inclined implants in fixed prosthesis: Strain and stress analysis. Rev. Odontol. UNESP 2018, 47, 237–243. [Google Scholar] [CrossRef][Green Version]
- Tahmaseb, A.; Weijden, J.; Mercelis, P.; De Clerck, R.; Wismeijer, D. Parameters of passive fit using a new technique to mill implant-supported superstructures: An in vitro study of a novel three-dimensional force measurement-misfit method. Int. J. Oral Maxillofac. Implant. 2010, 25, 247–257. [Google Scholar]
- Vercruyssen, M.; Laleman, I.; Jacobs, R.; Quirynen, M. Computer-supported implant planning and guided surgery: A narrative review. Clin. Oral Implant. Res. 2015, 26, 69–76. [Google Scholar] [CrossRef]
- Bencharit, S.; Staffen, A.; Yeung, M.; Whitley, D., III; Laskin, D.M.; Deeb, G.R. In vivo tooth-supported implant surgical guides fabricated with desktop stereolithographic printers: Fully guided surgery is more accurate than partially guided surgery. J. Oral Maxillofac. Surg. 2018, 76, 1431–1439. [Google Scholar] [CrossRef]
- Deeb, G.R.; Allen, R.K.; Hall, V.P.; Whitley, D., III; Laskin, D.M.; Bencharit, S. How accurate are implant surgical guides produced with desktop stereolithographic 3-dimentional printers? J. Oral Maxillofac. Surg. 2017, 75, 2559.e1–2559.e8. [Google Scholar] [CrossRef] [PubMed]
- Hinckfuss, S.; Conrad, H.J.; Lin, L.; Lunos, S.; Seong, W.J. Effect of surgical guide design and surgeon’s experience on the accuracy of implant placement. J. Oral Implantol. 2012, 38, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C.; Clement, J.G. Immediate implant placement postextraction without flap elevation. J. Periodontol. 2009, 80, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.D.; Chen, S.T. Esthetic outcomes of immediate implant placements. Clin. Oral Implant. Res. 2008, 19, 73–80. [Google Scholar] [CrossRef]
- Kan, J.Y.; Rungcharassaeng, K.; Sclar, A.; Lozada, J.L. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J. Oral Maxillofac. Surg. 2007, 65, 13–19. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontology 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Rungcharassaeng, K.; Caruso, J.M.; Kan, J.Y.K.; Schutyser, F.; Boumans, T. Accuracy of computer-guided surgery: A comparison of operator experience. J. Prosthet. Dent. 2015, 114, 407–413. [Google Scholar] [CrossRef]
- Al Yafi, F.; Camenisch, B.; Al-Sabbagh, M. Is digital guided implant surgery accurate and reliable? Dent. Clin. N. Am. 2019, 63, 381–397. [Google Scholar] [CrossRef]
- Behneke, A.; Burwinkel, M.; Behneke, N. Factors influencing transfer accuracy of cone beam CT-derived template-based implant placement. Clin. Oral Implant. Res. 2011, 23, 416–423. [Google Scholar] [CrossRef]
- Di Giacomo, G.A.; Cury, P.R.; de Araujo, N.S.; Sendyk, W.R.; Sendyk, C.L. Clinical application of stereolithographic surgical guides for implant placement: Preliminary results. J. Periodontol. 2005, 76, 503–507. [Google Scholar] [CrossRef]
- Fokas, G.; Vaughn, V.M.; Scarfe, W.C.; Bornstein, M.M. Accuracy of linear measurements on CBCT images related to presurgical implant treatment planning: A systematic review. Clin. Oral Implant. Res. 2018, 29, 393–415. [Google Scholar] [CrossRef] [PubMed]
- Bover-Ramos, F.; Viña-Almunia, J.; Cervera-Ballester, J.; Penarrocha, M.; Mira, B. Accuracy of implant placement with computer-guided surgery: A systematic review and meta-analysis comparing cadaver, clinical, and in vitro studies. Int. J. Oral Maxillofac. Implant. 2017, 33, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Polizzi, G.; Moy, P. Guided surgery with tooth-supported templates for single missing teeth: A critical review. Eur. J. Oral Implantol. 2016, 9, 135–153. [Google Scholar]
- El Kholy, K.; Lazarin, R.; Janner, S.; Faerber, K.; Buser, R.; Buser, D. Influence of surgical-guide support and implant site location on accuracy of static computer assisted implant surgery. Clin. Oral Implant. Res. 2019, 30, 1067–1075. [Google Scholar] [CrossRef]
- Henprasert, P.; Dawson, D.; El-Kerdani, T.; Song, X.; Couso-Queiruga, E.; Holloway, J. Comparison of the accuracy of implant position using surgical guides fabricated by additive and subtractive techniques. J. Prosthodont. 2020, 29, 534–541. [Google Scholar] [CrossRef]
- El Kholy, K.; Ebenezer, S.; Wittneben, J.-G.; Lazarin, R.; Rousson, D.; Buser, D. Influence of implant macrodesign and insertion connection technology on the accuracy of static computer-assisted implant surgery. Clin. Implant. Dent. Relat. Res. 2019, 21, 1073–1079. [Google Scholar] [CrossRef]
- Park, C.; Raigrodski, A.J.; Rosen, J.; Spiekerman, C.; London, R.M. Accuracy of implant placement using precision surgical guides with varying occlusogingival heights: An in vitro study. J. Prosthet. Dent. 2009, 101, 372–381. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Deviation | Program A (n = 30) | Program B (n = 30) | Program C (n = 30) | p-Value |
|---|---|---|---|---|
| 3D deviation at implant platform | ||||
| Mean ± SD (mm) Min–max (mm) | 0.55 ± 0.25 (0.39–0.71) | 0.52 ± 0.31 (0.38–0.57) | 0.56 ± 0.22 (0.43–0.62) | 0.84 |
| 3D deviation at implant apex | ||||
| Mean ± SD (mm) Min–max (mm) | 0.72 ± 0.37 (0.44–1.04) | 0.73 ± 0.40 (0.51–0.99) | 0.9 ± 0.46 (0.57–1) | 0.19 |
| Angular deviation | ||||
| Mean ± SD (degrees) Min–max (degrees) | 1.72 ± 0.88 (1.1–2.4) | 2.05 ± 1.24 (1.1–2.8) | 2.74 ± 1.81 (1.5–3.5) | 0.02 |
| Vertical depth deviation | ||||
| Mean ± SD (mm) Min–max (mm) | 0.19 ± 0.13 (0.09–0.27) | 0.31 ± 0.32 (0.11–0.35) | 0.31 ± 0.22 (0.13–0.44) | 0.11 |
| Direction | Program A (n = 30) | Program B (n = 30) | Program C (n = 30) | |
|---|---|---|---|---|
| The direction of implant platform deviation | ||||
| Buccolingual deviation | Buccal | 26 (86.67%) | 25 (83.33%) | 20 (66.67%) |
| Lingual | 4 (13.33%) | 5 (16.67%) | 10 (33.33%) | |
| Mesio-distal deviation | Mesial | 23 (76.67%) | 23 (76.67%) | 29 (96.67%) |
| Distal | 7 (23.33%) | 7 (23.33%) | 1 (3.33%) | |
| The direction of implant apex deviation | ||||
| Buccolingual deviation | Buccal | 24 (80.00%) | 25 (83.33%) | 20 (66.67%) |
| Lingual | 6 (20.00%) | 5 (16.67%) | 10 (33.33%) | |
| Mesio-distal deviation | Mesial | 23 (76.67%) | 23 (76.67%) | 29 (96.67%) |
| Distal | 7 (23.33%) | 7 (23.33%) | 1 (3.33%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visuttiwattanakorn, S.; Phatthanagowit, B. An In Vitro Study of the Reproducibility of the Drilling Access of Digitalized Surgical Guides Generated via Three Different Implant Planning Software Programs. Appl. Sci. 2022, 12, 7005. https://doi.org/10.3390/app12147005
Visuttiwattanakorn S, Phatthanagowit B. An In Vitro Study of the Reproducibility of the Drilling Access of Digitalized Surgical Guides Generated via Three Different Implant Planning Software Programs. Applied Sciences. 2022; 12(14):7005. https://doi.org/10.3390/app12147005
Chicago/Turabian StyleVisuttiwattanakorn, Surakit, and Bongkoch Phatthanagowit. 2022. "An In Vitro Study of the Reproducibility of the Drilling Access of Digitalized Surgical Guides Generated via Three Different Implant Planning Software Programs" Applied Sciences 12, no. 14: 7005. https://doi.org/10.3390/app12147005
APA StyleVisuttiwattanakorn, S., & Phatthanagowit, B. (2022). An In Vitro Study of the Reproducibility of the Drilling Access of Digitalized Surgical Guides Generated via Three Different Implant Planning Software Programs. Applied Sciences, 12(14), 7005. https://doi.org/10.3390/app12147005