
In Vitro Evaluation of the Strength of Dentin Replacement in Complex Posterior Tooth Restoration

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
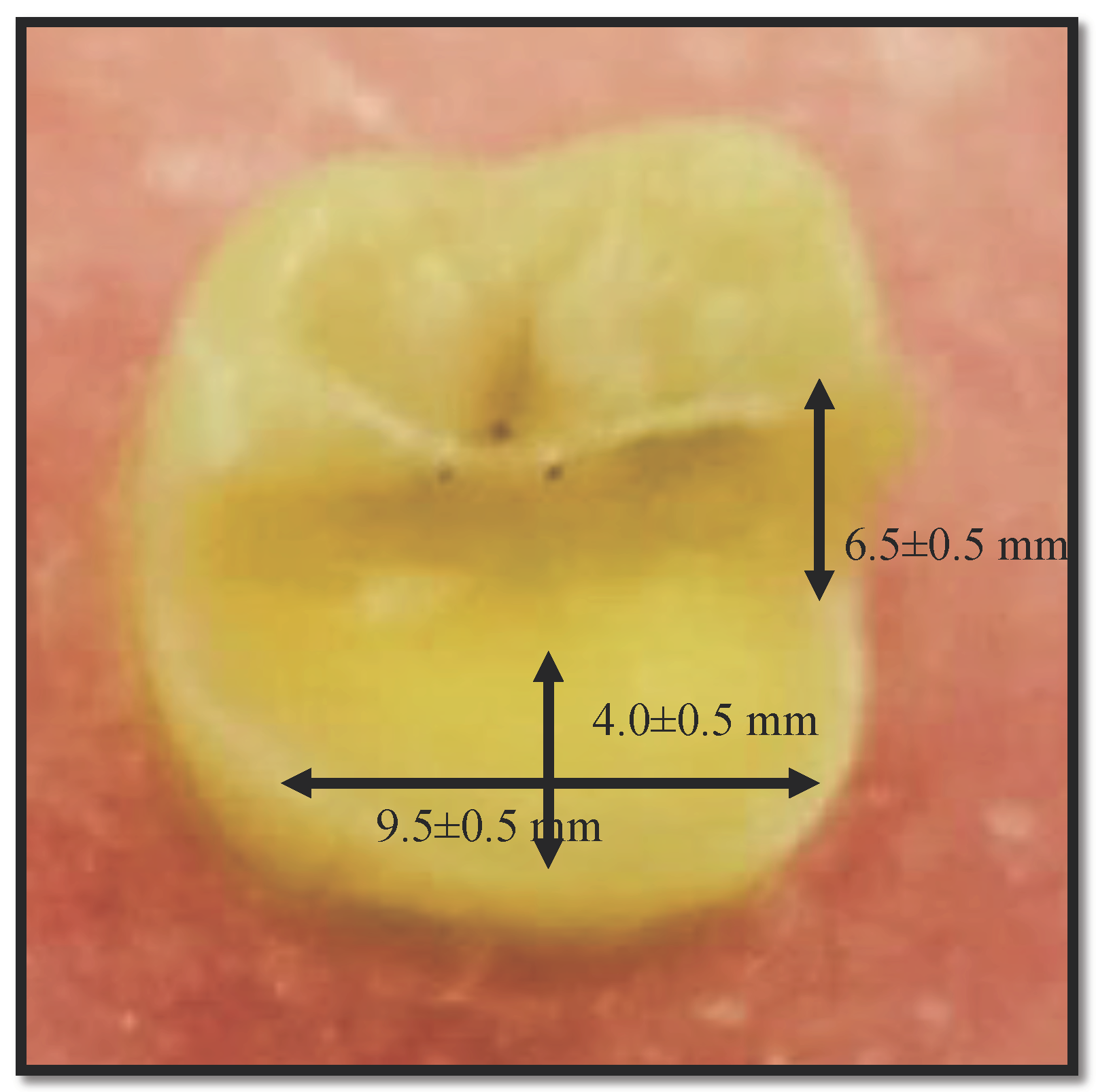
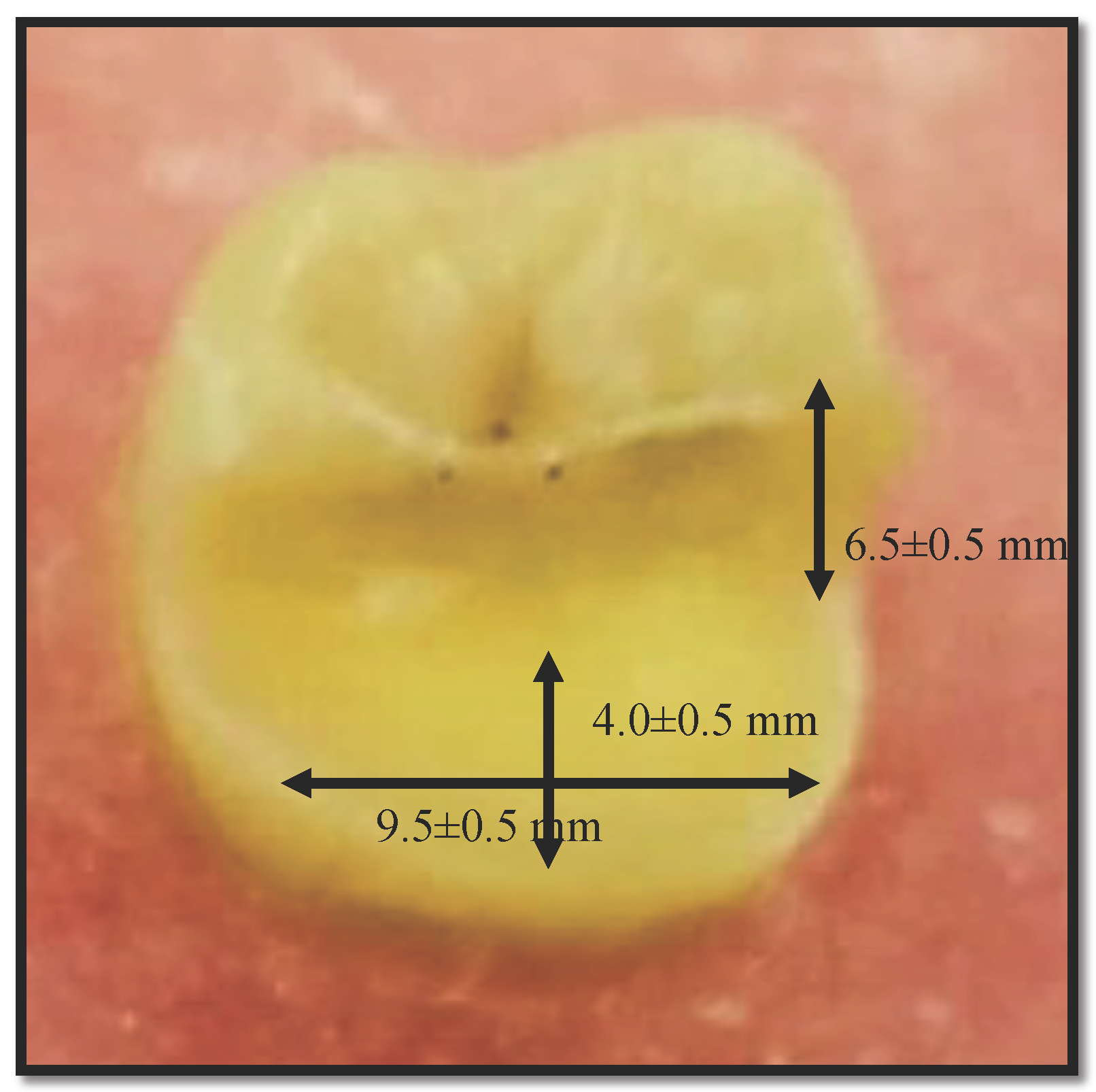
2.1. Teeth Preparation
2.2. Teeth Restoration
2.3. Tensile Strength Analysis
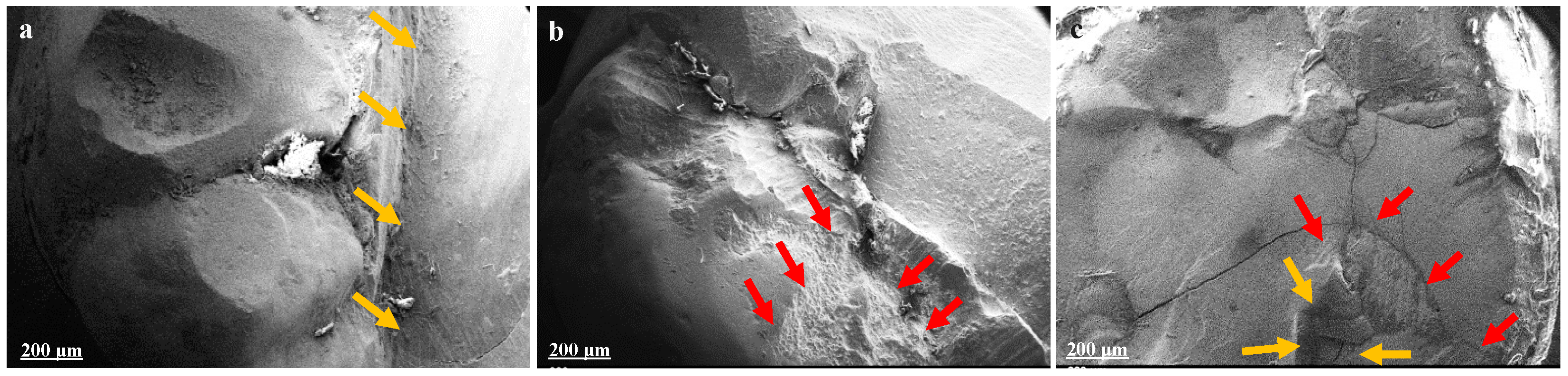
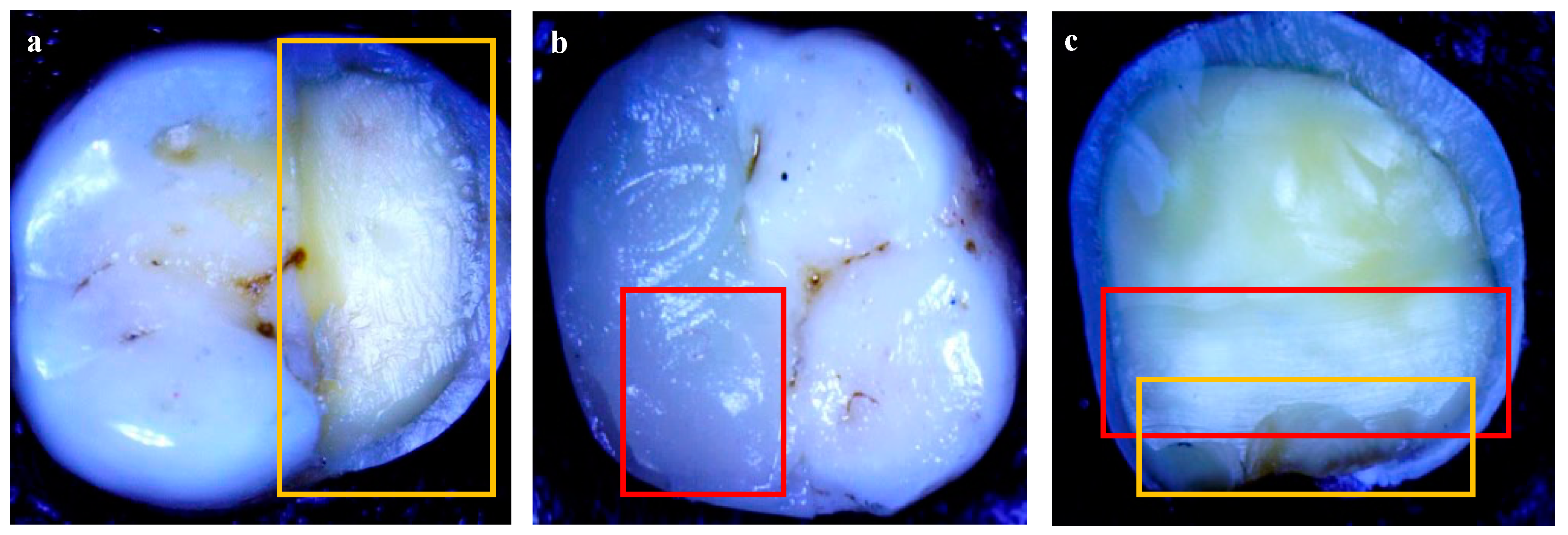
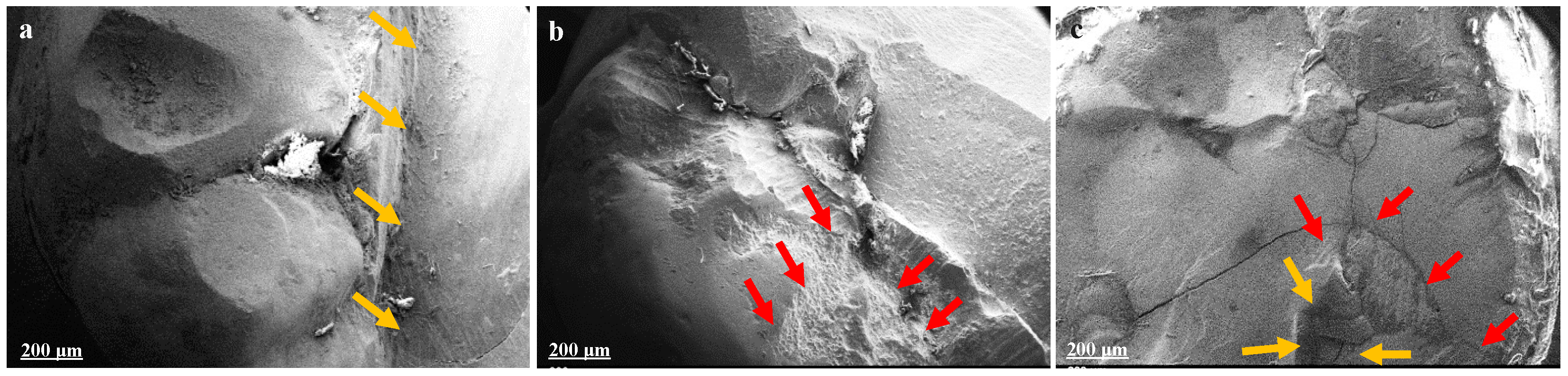
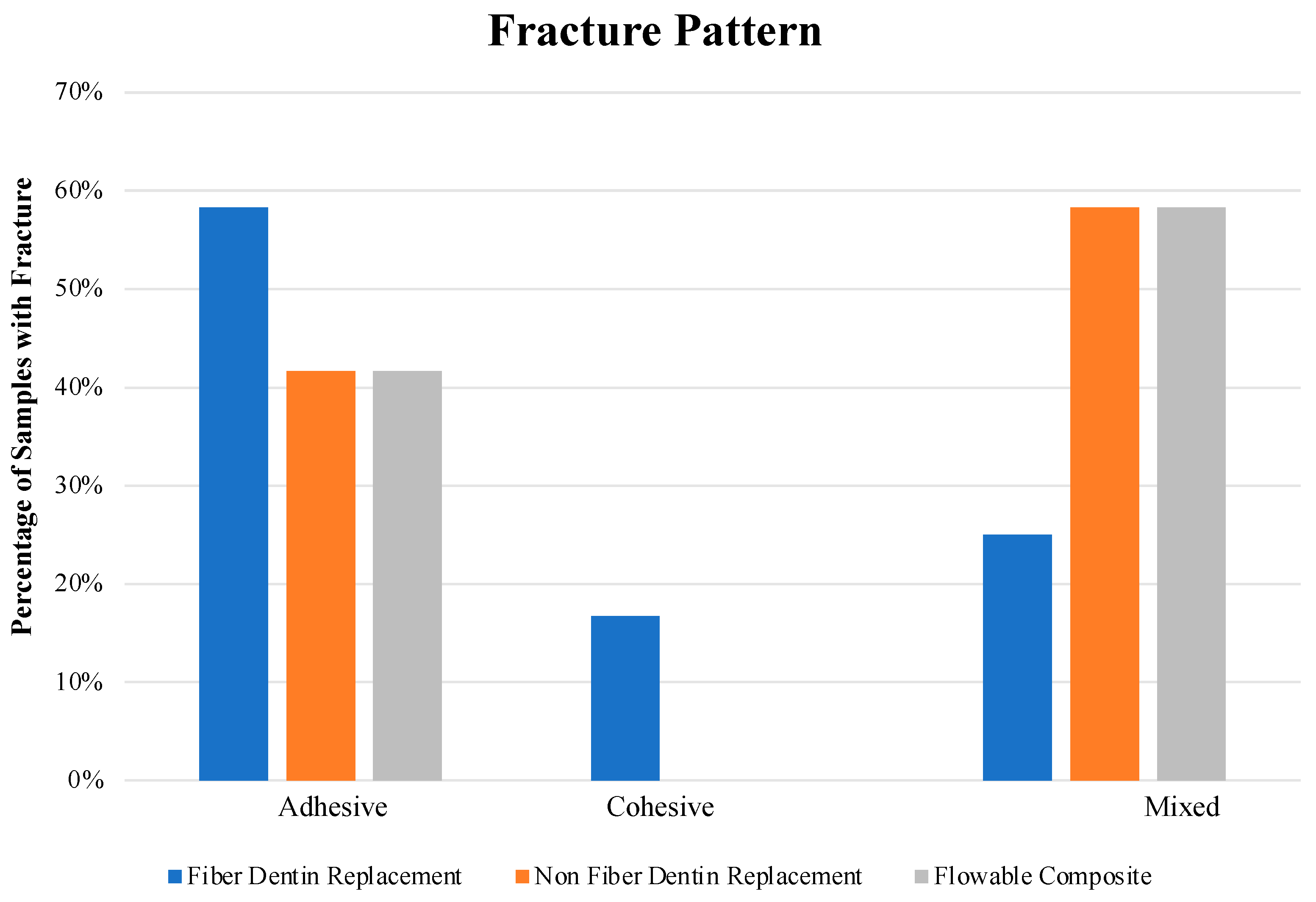
2.4. Fracture Pattern Evaluation
2.5. Statistical Analysis
3. Results
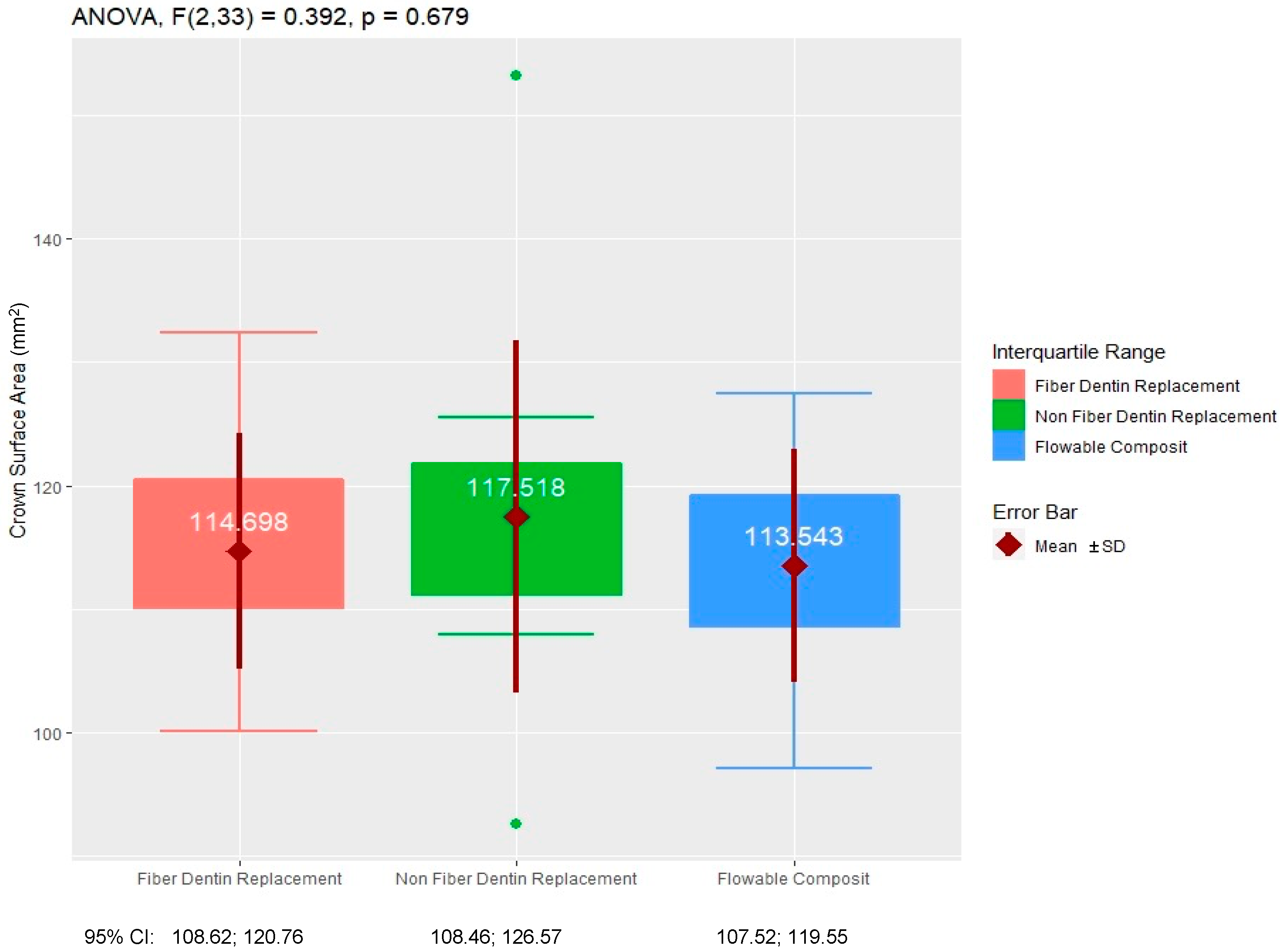
3.1. Sample Distribution
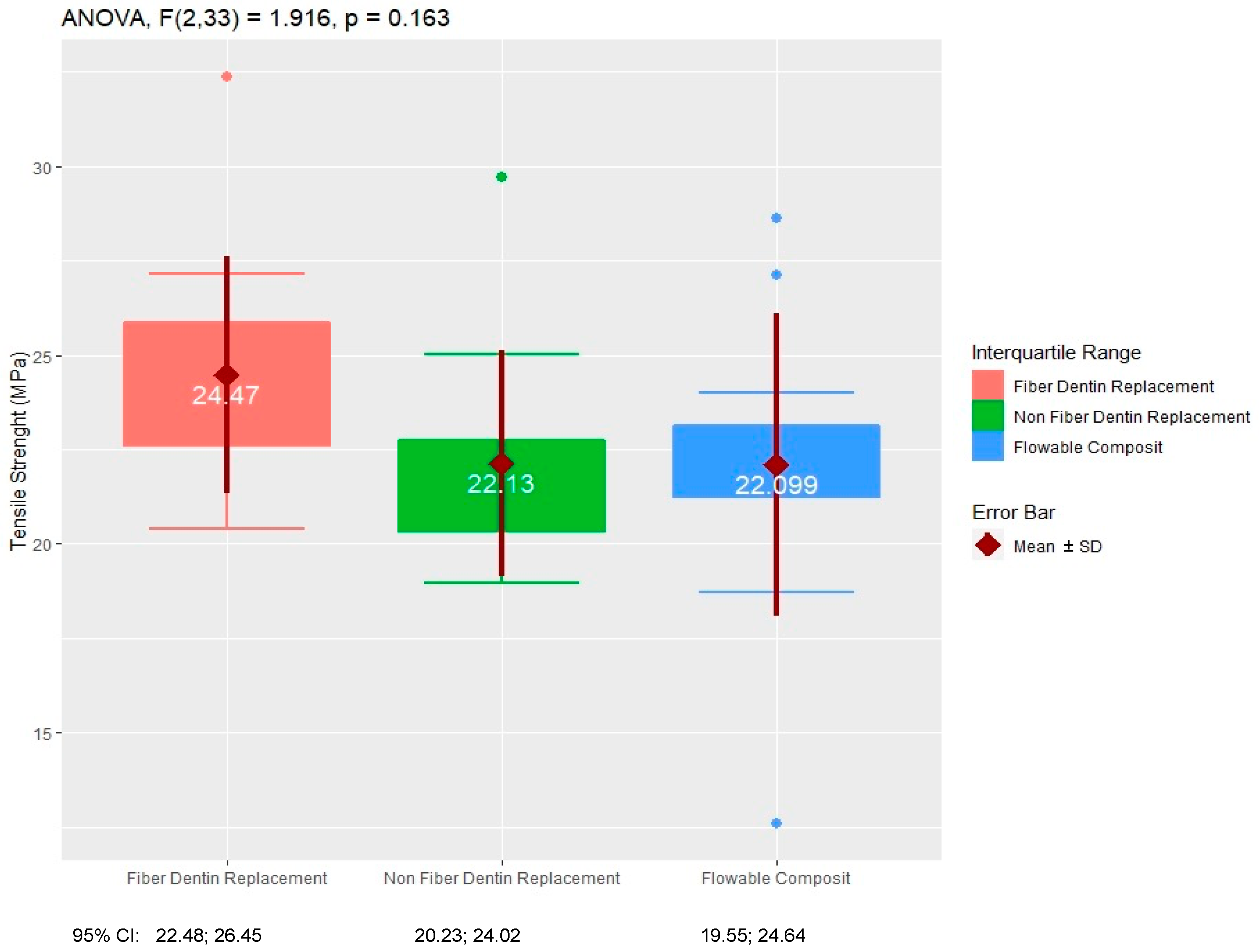
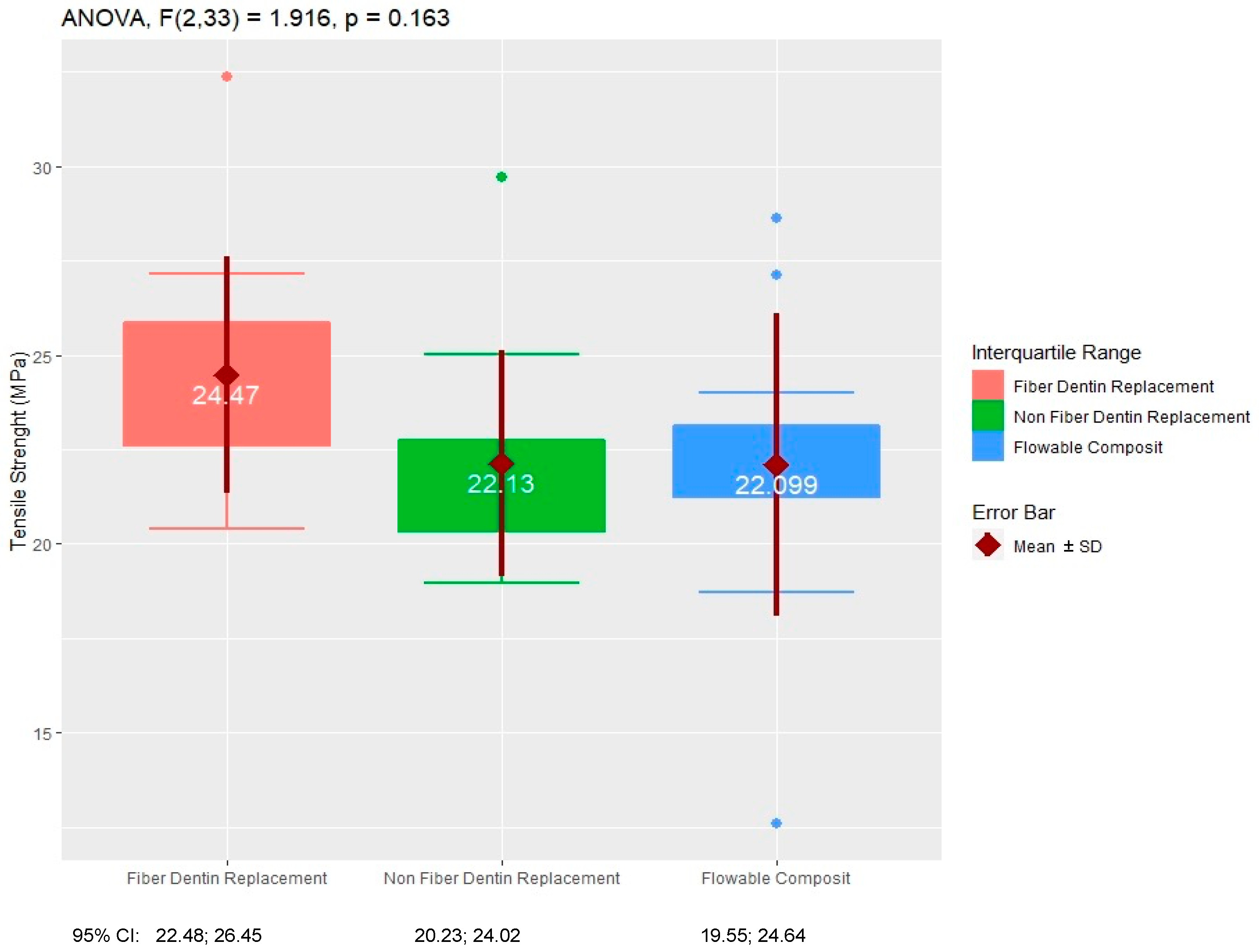
3.2. Tensile Strength Analysis
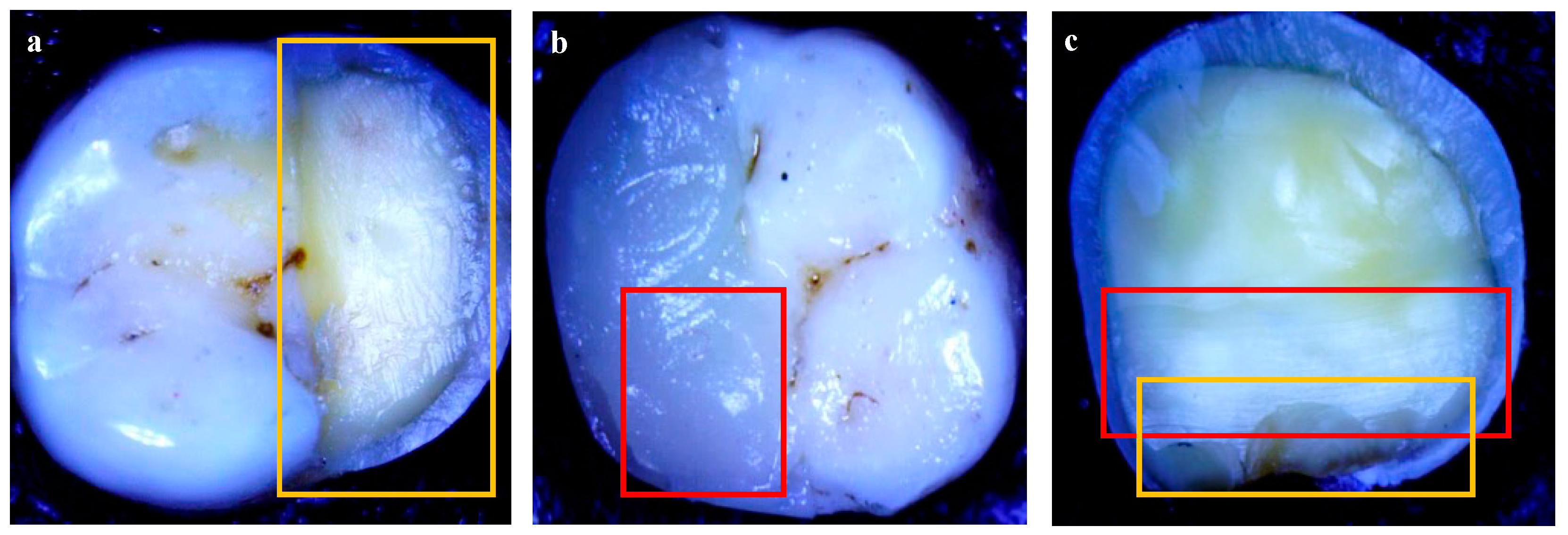
3.3. Fracture Pattern Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alani, A.; Austin, R.; Djemal, S. Contemporary management of tooth replacement in the traumatized dentition. Dent. Traumatol. 2012, 28, 183–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, I.R.; Lynch, C.D. Repair versus replacement of defective direct dental restorations in posterior teeth of adults. Prim. Dent. J. 2014, 3, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, L.; Banerjee, A. Minimally invasive direct restorations: A practical guide. Br. Dent. J. 2017, 223, 163–171. [Google Scholar] [CrossRef]
- Zarow, M.; Ramırez-Sebastia, A.; Paolone, G.; de Ribot Porta, J.; Mora, J.; Espona, J.; Duran-Sindreu, F.; Roig, M. A new classification system for the restoration of root filled teeth. Int. Endod. J. 2018, 51, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallesen, U.; van Dijken, J.W.; Halken, J.; Hallonsten, A.L.; Höigaard, R. Longevity of posterior resin composite restorations in permanent teeth in Public Dental Health Service: A prospective 8 years follow up. J. Dent. 2013, 41, 297–306. [Google Scholar] [CrossRef]
- da Veiga, A.M.; Cunha, A.C.; Ferreira, D.M.; da Silva Fidalgo, T.K.; Chianca, T.K.; Reis, K.R.; Maia, L.C. Longevity of direct and indirect resin composite restorations in permanent posterior teeth: A systematic review and meta-analysis. J. Dent. 2016, 54, 1–12. [Google Scholar] [CrossRef]
- Huang, N.C.; Bottino, M.C.; Levon, J.A.; Chu, T.G. The Effect of Polymerization Methods and Fiber Types on the Mechanical Behavior of Fiber-Reinforced Resin-Based Composites. J. Prosthodont. 2017, 26, 230–237. [Google Scholar] [CrossRef] [Green Version]
- Abouelleil, H.; Pradelle, N.; Villat, C.; Attik, N.; Colon, P.; Grosgogeat, B. Comparison of mechanical properties of a new fiber reinforced composite and bulk filling composites. Restor. Dent. Endod. 2015, 40, 262–270. [Google Scholar] [CrossRef]
- Angeletaki, F.; Gkogkos, A.; Papazoglou, E.; Kloukos, D. Direct versus indirect inlay/onlay composite restorations in posterior teeth. A systematic review and meta-analysis. J. Dent. 2016, 53, 12–21. [Google Scholar] [CrossRef]
- Garoushi, S.; Mangoush, E.; Vallittu, M.; Lassila, L. Short fiber reinforced composite: A new alternative for direct onlay restorations. Open Dent. J. 2013, 7, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Barceleiro, M.; Soares, G.; Espindola, O.; Kahn, S.; Poiate, I.; Sampaio-filho, H. Low-shrinkage composites: An in vitro evaluation of sealing ability after occlusal loading. Gen. Dent. 2015, 63, e36–e40. [Google Scholar] [PubMed]
- Dionysopoulos, D.; Gerasimidou, O. Wear of contemporary dental composite resin restorations: A literature review. Restor. Dent. Endod. 2021, 46, e18. [Google Scholar] [CrossRef] [PubMed]
- Lotfy, M.; Mahmoud, N.A.; Riad, M.I. Effect of preheating on polymerization shrinkage strain of BIS-GMA free and containing resin composite restorative materials (in vitro study). Bull. Natl. Res. Cent. 2022, 46, 74. [Google Scholar] [CrossRef]
- Giachetti, L.; Scaminaci Russo, D.; Bambi, C.; Grandini, R. A Review of Polymerization Shrinkage Stress: Current Techniques for Posterior Direct Resin Restorations. J. Contemp. Dent. Pract. 2006, 7, 79–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkhudhairy, F.I. The effect of curing intensity on mechanical properties of different bulk-fill composite resins. Clin. Cosmet. Investig. Dent. 2017, 9, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Cramer, N.B.; Stansbury, J.W.; Bowman, C.N. Recent advances and developments in composite dental restorative materials. J. Dent. Res. 2011, 90, 402–416. [Google Scholar] [CrossRef] [Green Version]
- Sakaguchi, R.L.; Powers, J.M. Craig’s Restorative Dental Materials, 13th ed.; Elsevier Mosby: Philadelphia, PA, USA, 2012; p. 21. [Google Scholar]
- Choudhury, W.R.; Nekkanti, S. Mechanical Properties of SDR™ and Biodentine™ as Dentin Replacement Materials: An In Vitro Study. J. Contemp. Dent. Pract. 2022, 23, 43–48. [Google Scholar] [CrossRef]
- Ausiello, P.; Dal Piva, A.M.d.O.; Borges, A.L.S.; Lanzotti, A.; Zamparini, F.; Epifania, E.; Mendes Tribst, J.P. Effect of Shrinking and No Shrinking Dentine and Enamel Replacing Materials in Posterior Restoration: A 3D-FEA Study. Appl. Sci. 2021, 11, 2215. [Google Scholar] [CrossRef]
- Orłowski, M.; Tarczydło, B.; Chałas, R. Evaluation of marginal integrity of four bulk-fill dental composite materials: In vitro study. Sci. World J. 2015, 2015, 701262. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, N.; Bahuguna, N.; Anand, S. Influence of composite insertion technique on gap formation. J. Conserv. Dent. 2016, 19, 77–81. [Google Scholar] [CrossRef] [Green Version]
- Jaganath, B.; Krishnegowda, S.; Rudranaik, S.; Madanan, S.; Kurup, N.; Manjula, C.G. Influence of Composite Insertion Techniques (Bulk-fill and Incremental Nanofilled Composites) on Adaptability to the Pulpal Floor and Interfacial Gap Formation. Int. J. Prev. Clin. Dent. Res. 2017, 4, 225–231. [Google Scholar] [CrossRef]
- Arslan, S.; Demirbuga, S.; Ustun, Y.; Dincer, A.N.; Canakci, B.C.; Zorba, Y.O. The effect of a new-generation flowable composite resin on microleakage in Class V composite restorations as an intermediate layer. J. Conserv. Dent. 2013, 16, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lokhande, N.A.; Padmai, A.S.; Rathore, V.P.; Shingane, S.; Jayashankar, D.N.; Sharma, U. Effectiveness of flowable resin composite in reducing microleakage—An in vitro study. J. Int. Oral Health 2014, 6, 111–114. [Google Scholar]
- Garoushi, S.K.; Hatem, M.; Lassila, L.V.J.; Vallittu, P.K. The effect of short fiber composite base on microleakage and load-bearing capacity of posterior restorations. Acta Biomater. Odontol. Scand. 2015, 1, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Tsujimoto, A.; Barkmeier, W.W.; Takamizawa, T.; Latta, M.A.; Miyazaki, M. Mechanical properties, volumetric shrinkage and depth of cure of short fiber-reinforced resin composite. Dent. Mater. J. 2016, 35, 418–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukarcanin, J.; Sadıkoğlu, İ.S.; Yaşa, B.; Türkün, L.Ş.; Türkün, M. Comparison of Different Restoration Techniques for Endodontically Treated Teeth. Int. J. Biomater. 2022, 2022, 6643825. [Google Scholar] [CrossRef] [PubMed]
- Didem, A.; Gözde, Y.; Nurhan, Ö. Comparative Mechanical Properties of Bulk-Fill Resins. Open J. Compos. Mater. 2014, 4, 117–121. [Google Scholar] [CrossRef] [Green Version]
- Atalay, C.; Yazici, A.R.; Horuztepe, A.; Nagas, E.; Ertan, A.; Ozgunaltay, G. Fracture Resistance of Endodontically Treated Teeth Restored With Bulk Fill, Bulk Fill Flowable, Fiber-reinforced, and Conventional Resin Composite. Oper Dent. 2016, 41, E131–E140. [Google Scholar] [CrossRef]
- Aminoroaya, A.; Neisiany, R.E.; Khorasani, S.N.; Panahi, P.; Das, O.; Madry, H.; Cucchiarini, M.; Ramakrishna, S. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Compos. Part B Eng. 2021, 216, 108852. [Google Scholar] [CrossRef]
- Ramdas, R.; Kumar, R.; Balan, P.; Rajeesh, M.G.; Palottil, A.S. Comparative Evaluation of Compressive And Flexural Strength of Newer Nanocomposite Materials with Conventional Hybrid Composites—An Invitro Study. IOSR-JDMS 2017, 16, 65–69. [Google Scholar]
- Braga, S.; Oliveira, L.; Rodrigues, R.B.; Bicalho, A.A.; Novais, V.R.; Armstrong, S.; Soares, C.J. The Effects of Cavity Preparation and Composite Resin on Bond Strength and Stress Distribution Using the Microtensile Bond Test. Oper. Dent. 2018, 43, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Karatas, O. Effect of fiber reinforcement on color stability and degree of polymerization of different composite resins. J. Oral Res. Rev. 2021, 13, 25–30. [Google Scholar] [CrossRef]
- Garlapati, T.G.; Krithikadatta, J.; Natanasabapathy, V. Fracture resistance of endodontically treated teeth restored with short fiber composite used as a core material-An in vitro study. J. Prosthodont. Res. 2017, 61, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Safwat, E.M.; Khater, A.G.A.; Abd-Elsatar, A.G.; Khater, G.A. Glass fiber-reinforced composites in dentistry. Bull. Natl. Res. Cent. 2021, 45, 190. [Google Scholar] [CrossRef]
- Chandrasekhar, V.; Rudrapati, L.; Badami, V.; Tummala, M. Incremental techniques in direct composite restoration. J. Conserv. Dent. 2017, 20, 386. [Google Scholar] [CrossRef]
- Alrahlah, A. Diametral Tensile Strength, Flexural Strength, and Surface Microhardness of Bioactive Bulk Fill Restorative. J. Contemp. Dent. Pract. 2018, 19, 13–19. [Google Scholar] [CrossRef]
- Vignesh, S.; Kandaswamy, D.; Lakshmi, B. Comparative evaluation of fracture resistance of endodontically treated teeth restored with bulk fill, packable and fiber reinforced composites. IJCR 2018, 10, 5. [Google Scholar]
- Rosatto, C.M.; Bicalho, A.A.; Veríssimo, C.; Bragança, G.F.; Rodrigues, M.P.; Tantbirojn, D.; Versluis, A.; Soares, C.J. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J. Dent. 2015, 43, 1519–1528. [Google Scholar] [CrossRef]
- Atiyah, A.; Baban, L. Fracture resistance of endodontically treated premolars with extensive MOD cavities restored with different composite restorations (An In vitro study). J. Bagh. Coll. Dent. 2014, 26, 9. [Google Scholar] [CrossRef]
- Kumagai, R.Y.; Zeidan, L.C.; Rodrigues, J.A.; Reis, A.F.; Roulet, J.F. Bond Strength of a Flowable Bulk-fill Resin Composite in Class II MOD Cavities. J. Adhes. Dent. 2015, 17, 427–432. [Google Scholar] [CrossRef]
- Nadig, A.; Usha, G.; Karthik, J.; Rao, R.; Vedhavathi, B. Effect of Four Different Placement Techniques on Marginal Microleakage in Class II Composite Restorations: An in vitro Study. World J. Dent. 2011, 2, 111–116. [Google Scholar] [CrossRef]
- Ibrahim, B.; Al-Azzawi, H. Fracture Resistance of Endodontically Treated Premolar Teeth with Extensive MOD Cavities Restored with Different Bulk Fill Composite Restorations (An In vitro Study). J. Bagh. Coll. Dent. 2017, 29, 7. [Google Scholar] [CrossRef]
- Geerts, S.O.; Seidel, L.; Albert, A.I.; Gueders, A.M. Microleakage after Thermocycling of Three Self-Etch Adhesives under Resin-Modified Glass-Ionomer Cement Restorations. Int. J. Dent. 2010, 2010, 728453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, R.O.; Ozcan, M.; Michida, S.M.; de Melo, R.M.; Pavanelli, C.A.; Bottino, M.A.; Soares, L.E.; Martin, A.A. Conversion degree of indirect resin composites and effect of thermocycling on their physical properties. J. Prosthodont. 2010, 19, 218–225. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptives | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tensile Strength (MPa) | ||||||||
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ||
| Lower Bound | Upper Bound | |||||||
| Fiber Dentin Replacement | 12 | 24.47 | 3.12 | 0.90 | 22.48 | 26.45 | 20.39 | 32.36 |
| Non-Fiber Dentin Replacement | 12 | 22.13 | 2.98 | 0.86 | 20.23 | 24.02 | 18.96 | 29.70 |
| Flowable Composite | 12 | 22.10 | 4.00 | 1.15 | 19.55 | 24.64 | 12.60 | 28.62 |
| Total | 36 | 22.89 | 3.49 | 0.58 | 21.71 | 24.08 | 12.60 | 32.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natsir, N.; Rahim, F.; Nugroho, J.J.; Rovani, C.A.; Syam, S.; Ruslin, M.; Saito, T.; Ou, K.-L. In Vitro Evaluation of the Strength of Dentin Replacement in Complex Posterior Tooth Restoration. Appl. Sci. 2022, 12, 6877. https://doi.org/10.3390/app12146877
Natsir N, Rahim F, Nugroho JJ, Rovani CA, Syam S, Ruslin M, Saito T, Ou K-L. In Vitro Evaluation of the Strength of Dentin Replacement in Complex Posterior Tooth Restoration. Applied Sciences. 2022; 12(14):6877. https://doi.org/10.3390/app12146877
Chicago/Turabian StyleNatsir, Nurhayaty, Farida Rahim, Juni Jekti Nugroho, Christine Anastasia Rovani, Syamsiah Syam, Muhammad Ruslin, Takashi Saito, and Keng-Liang Ou. 2022. "In Vitro Evaluation of the Strength of Dentin Replacement in Complex Posterior Tooth Restoration" Applied Sciences 12, no. 14: 6877. https://doi.org/10.3390/app12146877
APA StyleNatsir, N., Rahim, F., Nugroho, J. J., Rovani, C. A., Syam, S., Ruslin, M., Saito, T., & Ou, K.-L. (2022). In Vitro Evaluation of the Strength of Dentin Replacement in Complex Posterior Tooth Restoration. Applied Sciences, 12(14), 6877. https://doi.org/10.3390/app12146877