
Rethinking Healthcare Teams’ Practices Using Network Science: Implications, Challenges, and Benefits



Abstract
:1. Introduction
2. Complexity and Teamwork
2.1. Complexity and Complex Systems
2.2. Networks: Mapping the Connected Worlds
2.3. Teamwork: An Interconnected World
3. The Implications, Challenges, and Benefits of Network Science for Health Teamworking
4. Case Study
4.1. Case Study Context and Analysis
4.2. Case Study Findings
4.3. Managerial Implications
5. Discussions on Network Science for Teamwork
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Measure | Definition | Meaning |
|---|---|---|
| Degree centrality (ki) | The number of links incident upon a node, which can be interpreted as the neighbourhood size of each member within the network. | This highlights the immediate risk of a node catching, whatever is flowing through the network. It quantifies how well it is connected to the other elements of the graph. The degree centrality is an indicator of the spread of node connectivity along the graph and is a crucial gauge in defining the network organisation. |
| Transitivity (Ci) | For any node i is the fraction of the connected neighbours of i. | It determines the capacity of link creations among neighbours, i.e., the tendency in the network to create stable groups. |
| Closeness centrality (CC) | The natural distance between all pairs of nodes is defined by the length of their shortest paths. Thus, the more central a node is, the lower its distance is to all other nodes. | This value measures how long it takes to spread information from a member to all others sequentially. |
| Betweenness centrality (CB) | The number of times a node acts as a bridge along the shortest path between two other nodes. | This measure reveals the intermediary members that are essential for connecting different regions of the network. |
| Eigenvector centrality (CE) | The influence of a node in a network according to the number and the quality of its connections. | Indeed, a node with a smaller number of high-quality links has more power than one with a larger number of mediocre contacts. |
| Pagerank | A node has high rank if the sum of the ranks of its in-edges is high. | It quantifies the overall importance of a component based on the relative importance of the components it is part of. |
| Bonacich index (CBP) | The power of a node is recursively defined by the sum of the power of its alters. | Positive values imply that members become more powerful as their alters, i.e., neighbours, come to be more powerful, while negative values imply that members are more powerful only as their alters become weaker, as occurs in competitive or antagonistic relations. |
| Authority (Kleinberg centrality scores) (CA) | A node is an authority if it is linked by hubs; it is a hub if it links to authorities. | A node is important if it receives many links from other important sources. |
| Coreness | The k-core of the graph is a maximal subgraph in which each vertex has at least degree k. The coreness of a vertex is k if it belongs to the k-core but not to the (k + 1)-core. | It helps identify tightly interlinked core areas in a network. |

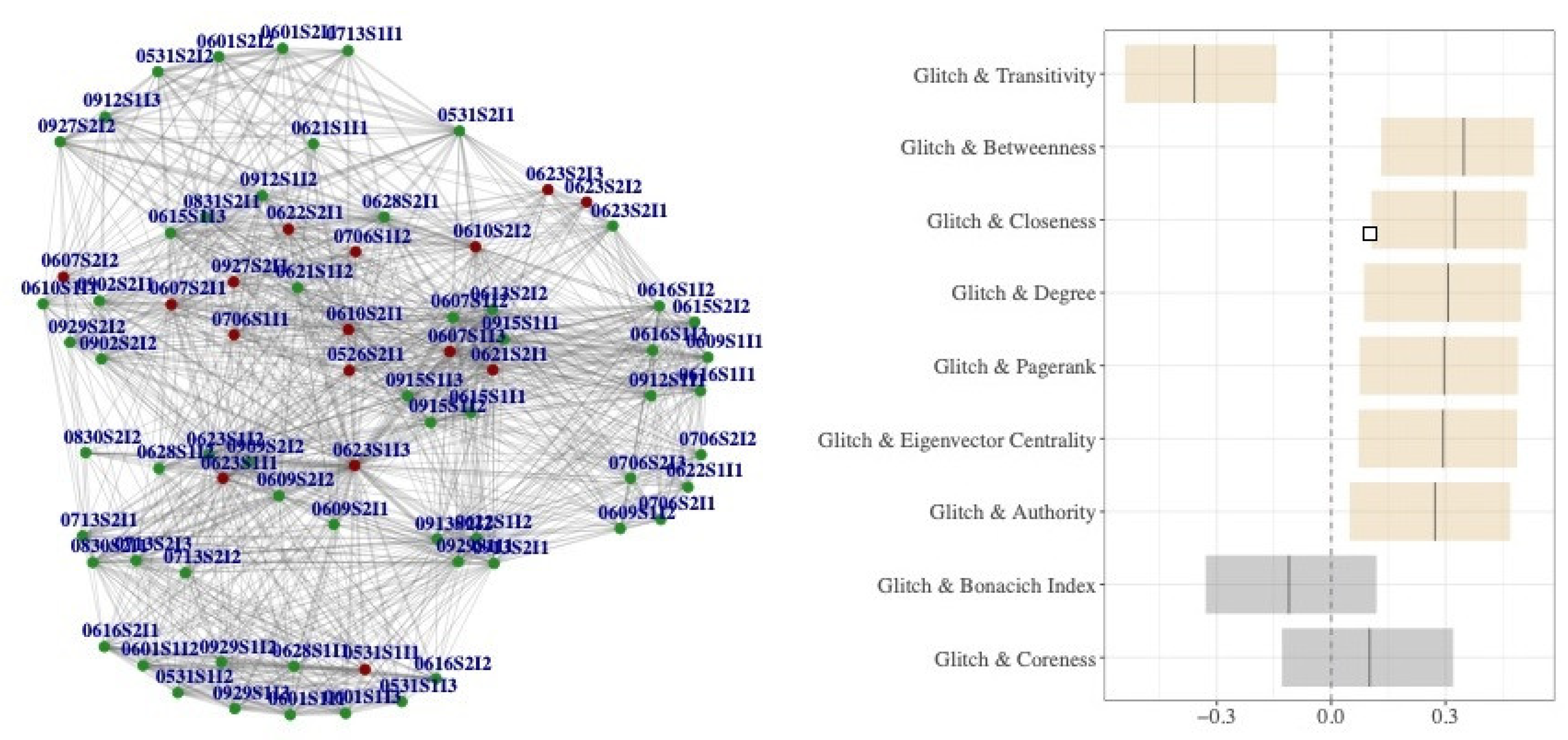
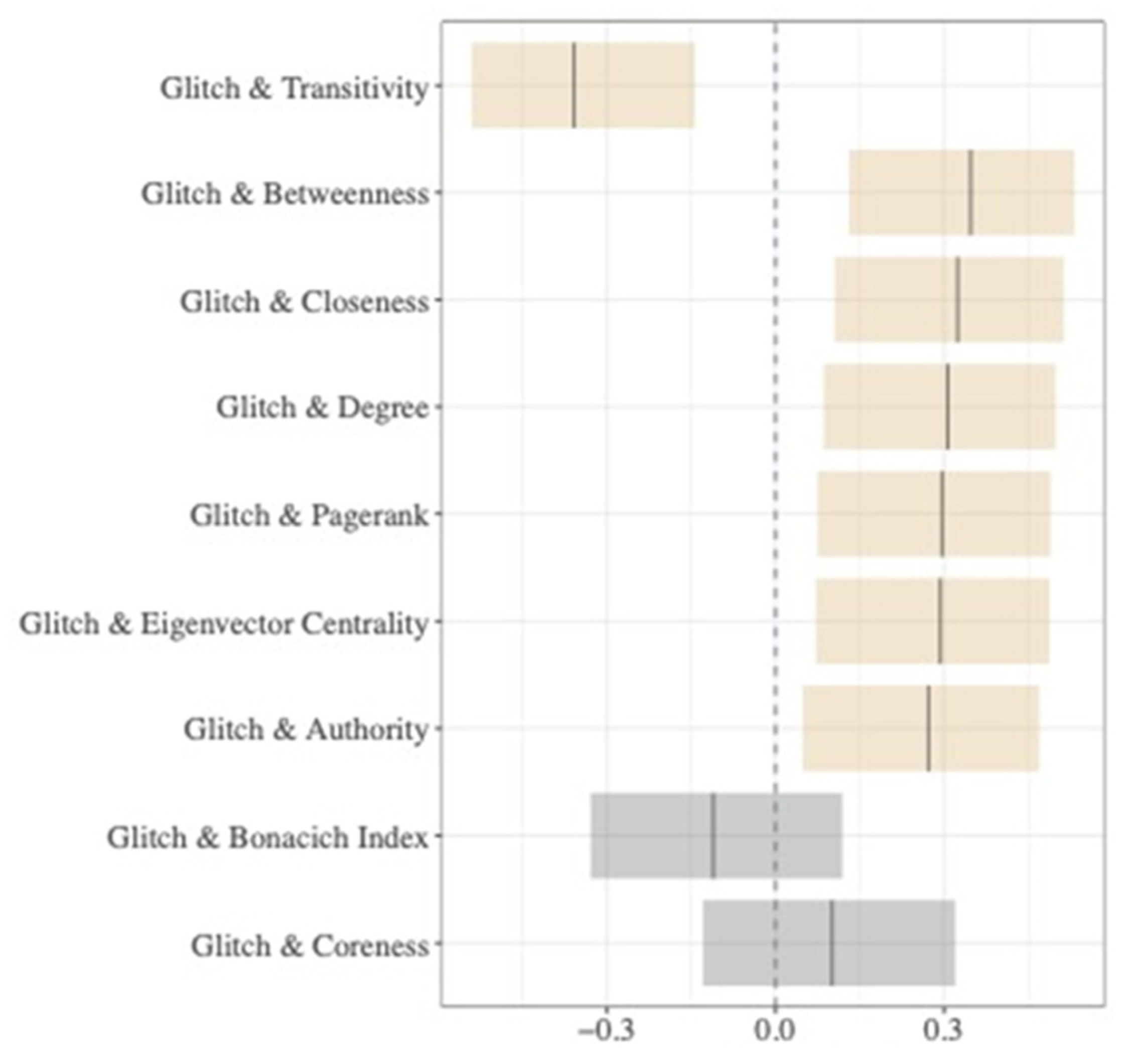
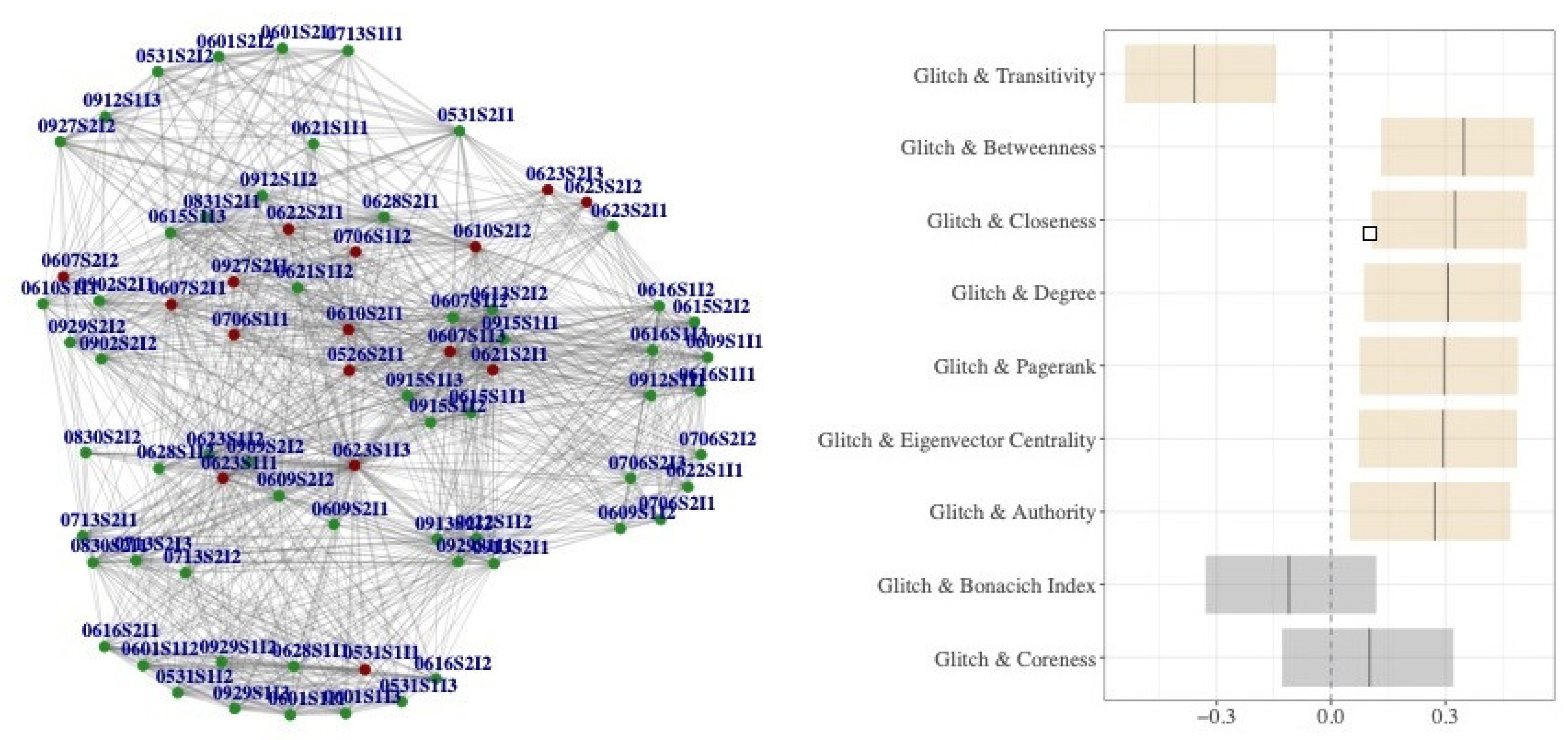
| Glitch vs. Centrality | Corr | p-Value | Lower | Upper | p | |
|---|---|---|---|---|---|---|
| 1 | Glitch–transitivity | −0.359 | 0.00158 | −0.542 | −0.143 | 0/1000 |
| 2 | Glitch–betweenness | 0.348 | 0.00224 | 0.131 | 0.533 | 67/1000 |
| 3 | Glitch–closeness | 0.324 | 0.00453 | 0.105 | 0.513 | 0/1000 |
| 4 | Glitch–degree | 0.307 | 0.00744 | 0.0857 | 0.499 | 0/1000 |
| 5 | Glitch–pagerank | 0.296 | 0.00985 | 0.0743 | 0.490 | 1000/1000 |
| 6 | Glitch–eigenvector centrality | 0.294 | 0.0106 | 0.0714 | 0.488 | 770/1000 |
| 7 | Glitch–authority | 0.272 | 0.0181 | 0.0483 | 0.470 | 994/1000 |
| 8 | Glitch–Bonacich index | −0.111 | 0.344 | −0.330 | 0.119 | 276/1000 |
| 9 | Glitch–coreness | 0.101 | 0.390 | −0.129 | 0.320 | 995/1000 |
References
- Wheelock, A.; Suliman, A.; Wharton, R.; Babu, E.D.; Hull, L.; Vincent, C.; Sevdalis, N.; Arora, S. The impact of operating room distractions on stress, workload, and teamwork. Ann. Surg. 2015, 261, 1079–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.T.; Lin, C.C.; Chen, C.H.; Ho, Y.H. Explicit and implicit team coordination: Development of a multidimensional scale. Soc. Behav. Personal. Int. J. 2017, 45, 915–929. [Google Scholar] [CrossRef]
- Brubakk, K.; Svendsen, M.V.; Deilkås, E.T.; Hofoss, D.; Barach, P.; Tjomsland, O. Hospital work environments affect the patient safety climate: A longitudinal follow-up using a logistic regression analysis model. PLoS ONE 2021, 16, e0258471. [Google Scholar] [CrossRef] [PubMed]
- Manser, T. Teamwork and patient safety in dynamic domains of healthcare: A review of the literature. Acta Anaesthesiol. Scand. 2009, 53, 143–151. [Google Scholar] [CrossRef]
- Berry, J.C.; Davis, J.T.; Bartman, T.; Hafer, C.C.; Lieb, L.M.; Khan, N.; Brilli, R.J. Improved safety culture and teamwork climate are associated with decreases in patient harm and hospital mortality across a hospital system. J. Patient Saf. 2016, 16, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Dinh, J.V.; Schweissing, E.J.; Venkatesh, A.; Traylor, A.M.; Kilcullen, M.P.; Perez, J.A.; Salas, E. The Study of Teamwork Processes within the Dynamic Domains of Healthcare: A Systematic and Taxonomic Review. Front. Commun. 2021, 6, 3. [Google Scholar] [CrossRef]
- Antonacopoulou, E.; Chiva, R. The social complexity of organizational learning: The dynamics of learning and organizing. Manag. Learn. 2007, 38, 277–295. [Google Scholar] [CrossRef]
- Andersson, C.; Törnberg, P. Wickedness and the anatomy of complexity. Futures 2018, 95, 118–138. [Google Scholar] [CrossRef]
- Brešan, M.; Erčulj, V.; Lajovic, J.; Ravljen, M.; Sermeus, W.; Grosek, Š. The relationship between the nurses’ work environment and the quality and safe nursing care: Slovenian study using the RN4CAST questionnaire. PLoS ONE 2021, 16, e0261466. [Google Scholar] [CrossRef]
- Turner, J.R.; Baker, R.M.; Romine, K. Complex Adaptive Team Systems (CATS): Scaling of a Team Leadership Development Model. In Leadership; IntechOpen: London, UK, 2019. [Google Scholar]
- Funtowicz, S.; Ravetz, J.R. Emergent complex systems. Futures 1994, 26, 568–582. [Google Scholar] [CrossRef]
- Thurner, S.; Hanel, R.; Klimek, P. Introduction to the Theory of Complex Systems; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Barabási, A.-L. Network Science; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Newman, M. Networks; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Russell, M.G.; Smorodinskaya, N.V. Leveraging complexity for ecosystemic innovation. Technol. Forecast. Soc. Chang. 2018, 136, 114–131. [Google Scholar] [CrossRef]
- Hassanien, A.E.; Azar, A.T.; Snasael, V.; Kacprzyk, J.; Abawajy, J.H. Big Data in Complex Systems; Springer International Publishing: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Bokeno, M. Complexity: An alternative paradigm for teamwork development. Dev. Learn. Organ. Int. J. 2008, 22, 7–10. [Google Scholar] [CrossRef]
- Vasileiadou, E.; Safarzyńska, K. Transitions: Taking complexity seriously. Futures 2010, 42, 1176–1186. [Google Scholar] [CrossRef]
- Cilliers, P.; Nicolescu, B. Complexity and transdisciplinarity–Discontinuity, levels of Reality and the Hidden Third. Futures 2012, 44, 711–718. [Google Scholar] [CrossRef]
- Cilliers, P. Knowledge, limits and boundaries. Futures 2015, 37, 605–613. [Google Scholar] [CrossRef]
- Derbyshire, J. The implications, challenges and benefits of a complexity-oriented Futures Studies. Futures 2016, 77, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Corning, P.A. The Re-Emergence of “Emergence”: A Venerable Concept in Search of a Theory. Complexity 2002, 7, 18–30. [Google Scholar] [CrossRef]
- Börner, K.; Sanyal, S.; Vespignani, A. Network Science. Annu. Rev. Inf. Sci. Technol. 2007, 41, 537–607. [Google Scholar] [CrossRef]
- Lewis, T.G. Network Science: Theory and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Cerqueti, R.; Ferraro, G.; Iovanella, A. A new measure for community structure through indirect social connections. Expert Syst. Appl. 2018, 114, 196–209. [Google Scholar] [CrossRef] [Green Version]
- Brannick, M.T.; Prince, C. An overview of team performance measurement. In Team Performance Assessment and Measurement; Psychology Press: London, UK, 1997; pp. 15–28. [Google Scholar]
- Mathieu, J.; Maynard, M.T.; Rapp, T.; Gilson, L. Team effectiveness 1997–2007: A review of recent advancements and a glimpse into the future. J. Manag. 2008, 34, 410–476. [Google Scholar] [CrossRef] [Green Version]
- McGrath, J.E. Social Psychology: A Brief Introduction; Holt, Rinehart & Winston: New York, NY, USA, 1964. [Google Scholar]
- Cohen, S.G.; Bailey, D.E. What makes teams work: Group effectiveness research from the shop floor to the executive suite. J. Manag. 1997, 23, 239–290. [Google Scholar] [CrossRef]
- Ilgen, D.R.; Hollenbeck, J.R.; Johnson, M.; Jundt, D. Teams in organizations: From input-process-output models to IMOI models. Annu. Rev. Psychol. 2005, 56, 517–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozlowski, S.W.; Ilgen, D.R. Enhancing the effectiveness of work groups and teams. Psychol. Sci. Public Interest 2006, 7, 77–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmutz, J.; Manser, T.D. Do team processes really have an effect on clinical performance? A systematic literature review. Br. J. Anaesth. 2013, 110, 529–544. [Google Scholar] [CrossRef] [Green Version]
- Chaffin, D.; Heidl, R.; Hollenbeck, J.R.; Howe, M.; Yu, A.; Voorhees, C.; Calantone, R. The promise and perils of wearable sensors in organizational research. Organ. Res. Methods 2017, 20, 3–31. [Google Scholar] [CrossRef]
- Rosen, M.A.; Dietz, A.S.; Yang, T.; Priebe, C.E.; Pronovost, P.J. An integrative framework for sensor-based measurement of teamwork in healthcare. J. Am. Med. Inform. Assoc. 2014, 22, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Cooke, N.J.; Gorman, J.C.; Myers, C.W.; Duran, J.L. Interactive team cognition. Cogn. Sci. 2013, 37, 255–285. [Google Scholar] [CrossRef]
- Barth, S.; Schraagen, J.M.; Schmettow, M. Network measures for characterising team adaptation processes. Ergonomics 2015, 58, 1287–1302. [Google Scholar] [CrossRef]
- Houghton, R.J.; Baber, C.; Mcmaster, R.; Stanton, N.A.; Salmon, P.; Stewart, R.; Walker, G. Command and control in emergency services operations: A social network analysis. Ergonomics 2006, 49, 1204–1225. [Google Scholar] [CrossRef] [Green Version]
- Antonacci, G.; Fronzetti Colladon, A.; Stefanini, A.; Gloor, P. It is rotating leaders who build the swarm: Social network determinants of growth for healthcare virtual communities of practice. J. Knowl. Manag. 2017, 21, 1218–1239. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; McFee, E.; Olguin, D.O.; Waber, B.; Pentland, A. Sociometric badges: Using sensor technology to capture new forms of collaboration. J. Organ. Behav. 2012, 33, 412–427. [Google Scholar] [CrossRef]
- Aloini, D.; Covucci, C.; Stefanini, A. Collaboration Dynamics in Healthcare Knowledge Intensive Processes: A State of the Art on Sociometric Badges. In Digital Technology and Organizational Change; Springer: Cham, Switzerland, 2018; pp. 213–225. [Google Scholar]
- Leonard, M.; Graham, S.; Bonacum, D. The human factor: The critical importance of effective teamwork and communication in providing safe care. BMJ Qual. Saf. 2014, 13, i85–i90. [Google Scholar] [CrossRef] [Green Version]
- Burtscher, M.J.; Manser, T. Team mental models and their potential to improve teamwork and safety: A review and implications for future research in healthcare. Saf. Sci. 2012, 50, 1344–1354. [Google Scholar] [CrossRef]
- Rosen, M.A.; DiazGranados, D.; Dietz, A.S.; Benishek, L.E.; Thompson, D.; Pronovost, P.J.; Weaver, S.J. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. Am. Psychol. 2018, 73, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Valentine, M.A.; Nembhard, I.M.; Edmondson, A.C. Measuring teamwork in health care settings: A review of survey instruments. Med. Care 2015, 53, e16–e30. [Google Scholar] [CrossRef] [PubMed]
- Ansoff, H.I. Managing strategic surprise by response to weak signals. Calif. Manag. Rev. 1975, 18, 21–33. [Google Scholar] [CrossRef]
- Stroebel, C.K.; McDaniel, R.R., Jr.; Crabtree, B.F.; Miller, W.L.; Nutting, P.A.; Stange, K.C. How complexity science can inform a reflective process for improvement in primary care practices. Jt. Comm. J. Qual. Patient Saf. 2005, 31, 438–446. [Google Scholar] [CrossRef]
- Bae, S.H.; Nikolaev, A.; Seo, J.Y.; Castner, J. Health care provider social network analysis: A systematic review. Nurs. Outlook 2015, 63, 566–584. [Google Scholar] [CrossRef]
- Kukk, P.; Moors, E.H.M.; Hekkert, M.P. The complexities in system building strategies—The case of personalized cancer medicines in England. Technol. Forecast. Soc. Chang. 2015, 98, 47–59. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.; Carrington, P.J. The SAGE Handbook of Social Network Analysis; SAGE Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Cinelli, M.; Ferraro, G.; Iovanella, A. Network processes for collaborative innovation. Int. J. Entrep. Small Bus. 2019, 36, 430–452. [Google Scholar]
- Murdoch, T.B.; Detsky, A.S. The inevitable application of big data to health care. JAMA 2013, 309, 1351–1352. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.W.; Saria, S.; Ohno-Machado, L.; Shah, A.; Escobar, G. Big data in health care: Using analytics to identify and manage high-risk and high-cost patients. Health Aff. 2014, 33, 1123–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, S.A. Surgical management of the breast: Breast conservation therapy and mastectomy. Surg. Clin. 2013, 93, 411–428. [Google Scholar]
- Leach, L.S.; Myrtle, R.C.; Weaver, F.A.; Dasu, S. Assessing the performance of surgical teams. Health Care Manag. Rev. 2009, 34, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, S.; Sevdalis, N.; Nestel, D.; Woloshynowych, M.; Darzi, A.; Kneebone, R. The impact of stress on surgical performance: A systematic review of the literature. Surgery 2010, 147, 318–330. [Google Scholar] [CrossRef]
- Cox, C.E.; Salud, C.J.; Cantor, A.; Bass, S.S.; Peltz, E.S.; Ebert, M.D.; Reintgen, D.S. Learning curves for breast cancer sentinel lymph node mapping based on surgical volume analysis. J. Am. Col. Surg. 2001, 193, 593–600. [Google Scholar] [CrossRef]
- Mansel, R.E.; MacNeill, F.; Horgan, K.; Goyal, A.; Britten, A.; Townson, J.; Senior Guildford Breast Surgeons, On Behalf of the New Start Training Group. Results of a national training programme in sentinel lymph node biopsy for breast cancer. Br. J. Surg. 2013, 100, 654–661. [Google Scholar]
- Paige, J.T. Surgical team training: Promoting high reliability with nontechnical skills. Surg. Clin. 2010, 90, 569–581. [Google Scholar] [CrossRef]
- Gardner, A.K.; Scott, D.J.; Pedowitz, R.A.; Sweet, R.M.; Feins, R.H.; Deutsch, E.S.; Sachdeva, A.K. Best practices across surgical specialties relating to simulation-based training. Surgery 2015, 158, 1395–1402. [Google Scholar] [CrossRef]
- Singer, S.J.; Molina, G.; Li, Z.; Jiang, W.; Nurudeen, S.; Kite, J.G.; Berry, W.R. Relationship between operating room teamwork, contextual factors, and safety checklist performance. J. Am. Coll. Surg. 2016, 223, 568–580. [Google Scholar] [CrossRef]
- Son, Y.J.; Lee, E.K.; Ko, Y. Association of working hours and patient safety competencies with adverse nurse outcomes: A cross-sectional study. Int. J. Environ. Res. Public Health 2019, 16, 4083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, S.; Tschan, F.; Beldi, G.; Kurmann, A.; Candinas, D.; Semmer, N.K. Noise peaks influence communication in the operating room. An observational study. Ergonomics 2016, 59, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Allard, M.A.; Blanie, A.; Brouquet, A.; Benhamou, D. Learning non-technical skills in surgery. J. Visc. Surg. 2020, 157, S131–S136. [Google Scholar] [CrossRef]
- Rasoulkhani, K.; Mostafavi, A. Resilience as an emergent property of human-infrastructure dynamics: A multi-agent simulation model for characterizing regime shifts and tipping point behaviors in infrastructure systems. PLoS ONE 2018, 13, e0207674. [Google Scholar]
- Soto-Rubio, A.; Giménez-Espert, M.D.C.; Prado-Gascó, V. Effect of emotional intelligence and psychosocial risks on burnout, job satisfaction, and nurses’ health during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7998. [Google Scholar] [CrossRef]
- Goñi, J.; Avena-Koenigsberger, A.; Velez de Mendizabal, N.; van den Heuvel, M.P.; Betzel, R.F.; Sporns, O. Exploring the morphospace of communication efficiency in complex networks. PLoS ONE 2013, 8, e58070. [Google Scholar] [CrossRef] [PubMed]
- Tröster, C.; Mehra, A.; van Knippenberg, D. Structuring for team success: The interactive effects of network structure and cultural diversity on team potency and performance. Organ. Behav. Hum. Decis. Processes 2014, 124, 245–255. [Google Scholar] [CrossRef] [Green Version]
- West, D.B. Introduction to Graph Theory; Prentice Hall: Hoboken, NJ, USA, 2001. [Google Scholar]
- White, D.R.; Harary, F. The Cohesiveness of Blocks in Social Networks: Node Connectivity and Conditional Density. Sociol. Methodol. 2002, 31, 305–359. [Google Scholar] [CrossRef] [Green Version]
- Borgatti, S.P.; Everett, M.G. A Graph-theoretic perspective on centrality. Soc. Netw. 2006, 28, 466–484. [Google Scholar] [CrossRef]
- Rowley, T.J. Moving beyond dyadic ties: A network theory of stakeholder influences. Acad. Manag. Rev. 1997, 22, 887–910. [Google Scholar] [CrossRef]
- Jäntschi, L. A Test Detecting the Outliers for Continuous Distributions Based on the Cumulative Distribution Function of the Data Being Tested. Symmetry 2019, 11, 835. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- Csardi, G.; Nepusz, T. The igraph software package for complex network research. InterJ. Complex Syst. 2006, 1695, 1–9. [Google Scholar]
- Wasserman, S.; Faust, K. Social Network Analysis-Methods and Applications; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Diudea, M.V.; Gutman, I.; Jantschi, L. Molecular Topology; Nova Science Publishers: New York, NY, USA, 2001. [Google Scholar]
- Newman, M.E.J. Assortative mixing in networks. Phys. Rev. Lett. 2002, 89, 208701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslov, S.; Sneppen, K. Specificity and stability in topology of protein networks. Science 2002, 296, 910–913. [Google Scholar] [CrossRef] [Green Version]
| Concept | Implications | Challenges | Benefits |
|---|---|---|---|
| Irreversibility of time |
|
|
|
| Path dependence |
|
|
|
| Sensitivity to initial condition |
|
|
|
| Emergence and systemness |
|
|
|
| Attractor states |
|
|
|
| Complex causation |
|
|
|
| Concept | Implications | Challenges | Benefits |
|---|---|---|---|
| Irreversibility of time |
|
|
|
| Path dependence |
|
|
|
| Sensitivity to initial condition |
|
|
|
| Emergence and systemness |
|
|
|
| Attractor states |
|
|
|
| Complex causation |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aloini, D.; Ferraro, G.; Iovanella, A.; Stefanini, A. Rethinking Healthcare Teams’ Practices Using Network Science: Implications, Challenges, and Benefits. Appl. Sci. 2022, 12, 5841. https://doi.org/10.3390/app12125841
Aloini D, Ferraro G, Iovanella A, Stefanini A. Rethinking Healthcare Teams’ Practices Using Network Science: Implications, Challenges, and Benefits. Applied Sciences. 2022; 12(12):5841. https://doi.org/10.3390/app12125841
Chicago/Turabian StyleAloini, Davide, Giovanna Ferraro, Antonio Iovanella, and Alessandro Stefanini. 2022. "Rethinking Healthcare Teams’ Practices Using Network Science: Implications, Challenges, and Benefits" Applied Sciences 12, no. 12: 5841. https://doi.org/10.3390/app12125841
APA StyleAloini, D., Ferraro, G., Iovanella, A., & Stefanini, A. (2022). Rethinking Healthcare Teams’ Practices Using Network Science: Implications, Challenges, and Benefits. Applied Sciences, 12(12), 5841. https://doi.org/10.3390/app12125841