1. Introduction
It is common for third molars to fail, erupt, and remain impacted. Impacted teeth are partially erupted or impacted teeth that cannot establish a proper relationship with other teeth and tissues in the arch despite the expiration of the eruption time. The most frequently impacted teeth in the lower and upper jaws are the third molars, and their frequency of impaction has been reported to vary between 18% and 32% [
1,
2,
3].
There are many theories to explain the frequency of impaction of third molars. Some of these are the Mendelian theory, the phylogenic theory, and the orthodontic theory. Most of these theories emphasize the relationship between changes in dietary habits and the mismatch between jaw size and tooth size [
4].
The prevalence and distribution of impacted teeth in different parts of the jaw differ in many studies. The prevalence of impacted teeth, age, eruption time of teeth, radiological tooth development, and eruption criteria are determined [
4]. Many studies show that there are no gender differences in impacted third molars. However, other studies have reported a higher frequency of molars being impacted in females than in males [
1,
2,
5,
6].
Although impacted third molars are mostly asymptomatic, they can sometimes cause complications. Some of these complications can include pain, infection, cyst and tumor formation, root resorption in permanent teeth, fracture in the jaw, crowding in the mandibular anterior teeth, and bone loss in adjacent teeth [
5,
7,
8,
9,
10,
11,
12,
13,
14].
Surgical removal of impacted third molars is the most common treatment method in oral surgery. However, various complications may occur during and after surgical extraction. The most common complications are pain, edema, trismus, bleeding, infection, alveolar nerve injury, displacement of the extracted tooth into neighbor spaces, and mandible fractures [
15,
16].
Many methods are used in the classification of impacted teeth. These classifications are made according to the level of impaction, the angle of the third molar, and its relationship with the anterior border of the mandibular ramus [
8]. According to the Pell and Gregory classification system, third molars can be classified by their depth or level according to the occlusal surface (OS) of the adjacent second molar tooth [
9].
There have been previous studies in Caucasian [
3,
10,
11,
13,
17,
18], Arab [
19,
20], African [
21,
22], and Chinese [
5,
12] populations regarding the impaction of mandibular third molars. However, no study has been done on the North Cyprus population. Hence, it was considered worthwhile to assess the prevalence of impacted third molars using a panoramic radiograph with the associated pathologies according to the age, gender, and type of impaction in a sample of patients living in North Cyprus.
2. Materials and Methods
This retrospective study was carried out utilizing a review of clinical records of North Cyprus patients who were referred to Dr. Burhan Nalbantoğlu State Hospital, Department of Oral and Maxillofacial Surgery clinic for a period of one year (December 2012–December 2013). Dr. Burhan Nalbantoğlu State Hospital is the only hospital that has an oral and maxillofacial surgery department among the state hospitals in North Cyprus. A total of 1752 third molars in 550 patients were included in the study.
The study started with the approval of the Turkish Republic of Northern Cyprus Ministry of Health inpatient treatment institutions (Ref: YTK0,000-6000-14/446/Approval/2014). This study was based on the retrospective evaluation of radiographs. Only archived data were used for the study. However, before taking any radiograph examinations, patients gave their informed consent before any application according to the principles of the Helsinki Declaration, including all amendments and revisions. Collected data was only accessible to the researchers.
All panoramic radiographs were taken with standardized equipment and specifications. Data regarding age, gender, number of erupted and impacted third molars, the location (mandible or maxilla), sides (left/right), and type of impaction were obtained from patients’ records, and panoramic radiographs were retrospectively assessed by a single oral and maxillofacial surgeon on a transparency projector under constant lighting conditions.
The third molars were divided into three groups: erupted, partially erupted third molars, and completely impacted third molars [
3,
10,
11,
12,
13].
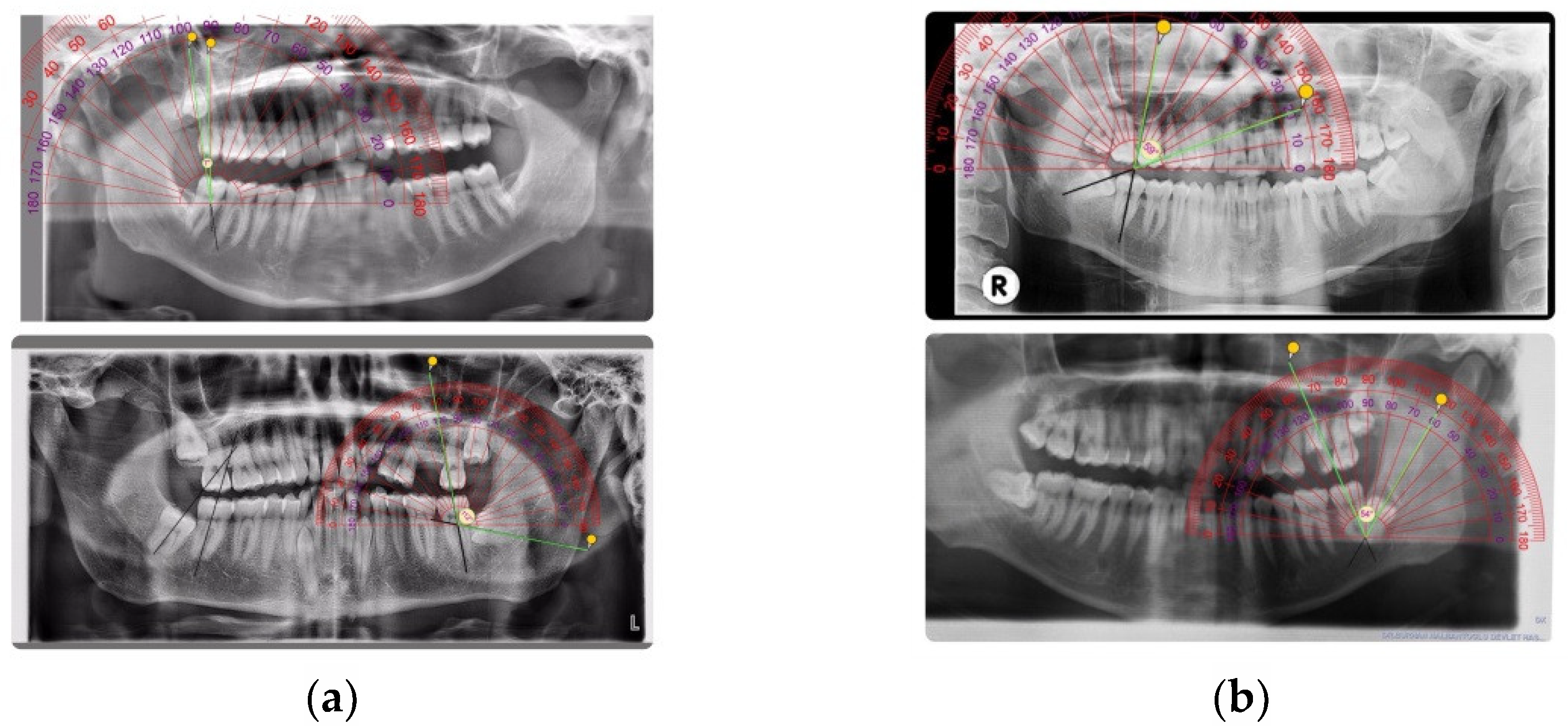
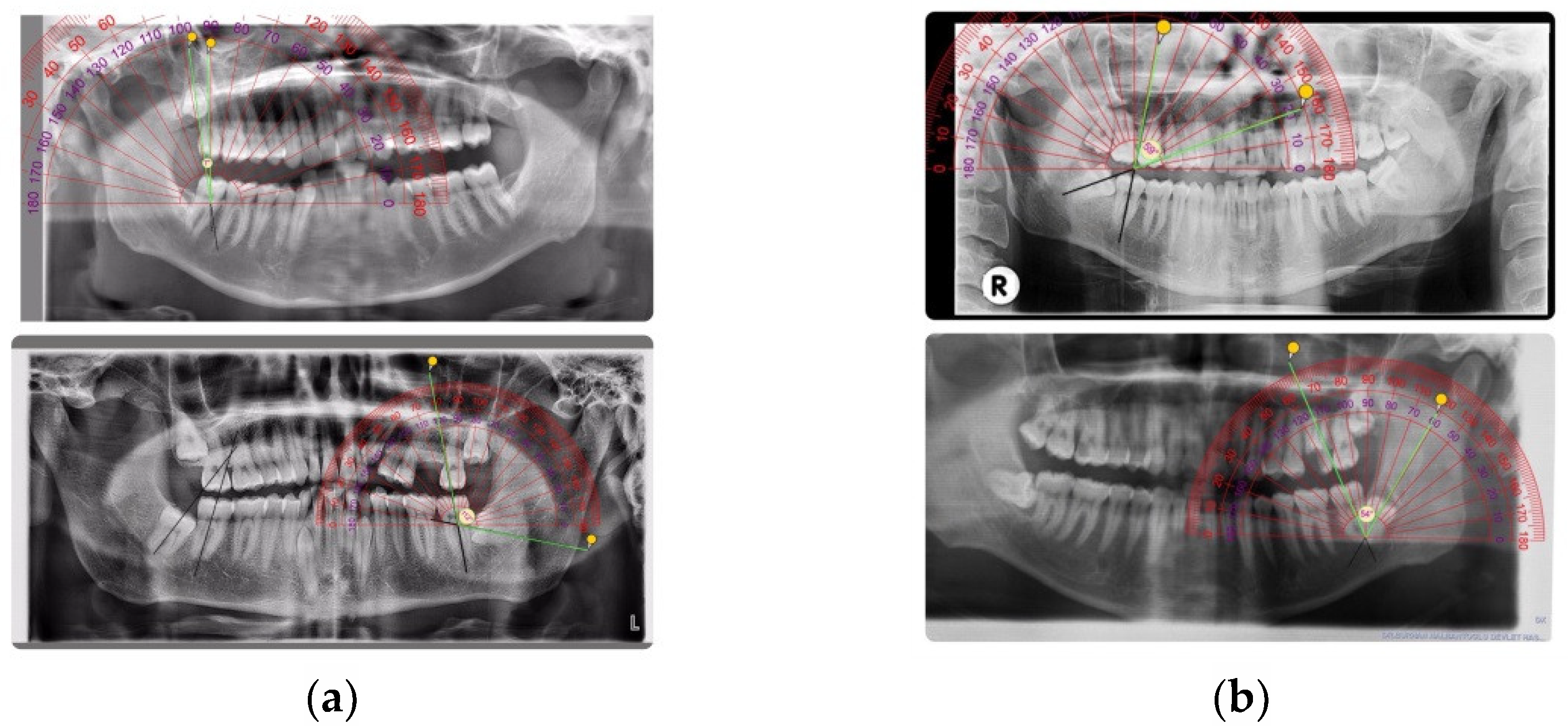
The angulation of the impacted third molar was documented based on Winter’s classification regarding the angle formed between the intersected longitudinal axes of the second and third molars, namely vertical impaction (10° to −10°), mesioangular impaction (11° to 79°), horizontal impaction (80° to 100°), distoangular impaction (−11° to −79°), others (111° to −80°), and buccolingual impaction (any tooth oriented in a buccolingual direction with crown overlapping the roots) [
17]. The axis of the teeth was measured on panoramic radiographs obtained from the patients by using a ruler and compass (
Figure 1a,b).
The pathologies and diagnoses of these pathologies associated with impacted teeth were defined in Dogan et al.’s study [
3]: pericoronitis, infection of the soft tissue surrounding a partially erupted tooth; caries, a clinical cavity or radiographic lesion reaching at least to the amelodentinal junction; periodontitis, bone loss of the adjacent tooth of more than 5 mm below the cementoenamel junction that is diagnosed both radiographically and by probing the gingival pocket; abscess-cyst, lesions with a pericoronal space of the dental follicle of more than 4 mm that is verified radiographically or surgically; caries on the second molar and root resorption of the adjacent teeth, clear loss of substance in the root surface revealed radiographically.
Data collected were entered into a spreadsheet (Excel 2000; Microsoft, Redmond, DC, USA) and analyzed subsequently using Statistical Package for Social Sciences (SPSS) version 16.0. The prevalence of impacted third molars according to age, gender, and type was assessed and displayed by frequency and percentage. A p-value less than 0.05 among gender, age, and sides was considered statistically significant through the Pearson Chi-square test.
3. Results
This study included 550 patients. Of these, 248 (46%) were female and 302 (54%) were male, and a total of 1752 third molar teeth were investigated (
Table 1).
The age of the patients who were the subjects of this study ranged from 16 to 65 years, with a mean age of 29 years. The highest prevalence of third molars included in this study were observed in patients belonging to the 20–29 years of age group. The total number of third molars in this group is 1050 (60%). The number of third molars included in this study decreased with increasing age (
Table 2).
Among all of the 1752 third molars included in this study, 716 (40%) of them erupted, while 1036 (60%) were impacted third molar teeth. The rest of the third molars were congenitally missing or already extracted and were not seen in panoramic radiographs. Impacted teeth were divided into two groups. The first group consisted of 487 (47%) partially impacted third molars, and the second group consisted of completely impacted 549 (53%) third molar teeth. Partially and completely impacted mandibular third molars displayed a significant difference between the left and right sides (
p < 0.05), whereas partially and completely impacted maxillary third molars did not display a significant difference between the left and right sides (
p > 0.05). Data analysis showed that third molars had approximately the same rate of occurrence in the mandible and maxilla (932 and 820 molars). The left side of the mandible had a greater number of impactions than the right side in our study group (
Table 3).
The distribution of erupted, partially impacted, and completely impacted third molars according to gender is shown in
Table 4. There was no statistically significant difference between genders according to the maxillary and mandibular right and left sides (
p > 0.05) (
Table 4).
The patients’ data showed that 383 (21%) teeth were associated with the following pathologies: pericoronitis, caries, periodontitis, abscess or cysts, caries on the second molar, and root resorption of the adjacent teeth. Pericoronitis was observed as the most frequent pathology in both the completely impacted and partially impacted groups, with 76 (14%) and 102 (21%) cases, respectively. Caries was not diagnosed with completely impacted teeth. The number of observed caries was low, with 73 cases observed in partially erupted teeth (representing 7% of all observed pathologies) (
Table 5).
Considering the distribution of pathologies by age, while pericoronitis, caries, and caries on the second molar were most common in the 30–39 age group; periodontitis, abscess-cyst, and root resorption of the adjacent teeth were most common in the 40–49 age group (
Table 6).
Among the impacted mandibular third molars, the majority of the patients had mesioangular impaction (42%), and only 4% of the patients had distoangular impaction. Contrary vertical impaction was the most common type in the maxillary arch (62%), and horizontal impaction was the least prevalent type (3%) (
Table 7).
While symptoms were observed in 144 (26%) of the completely impacted third molars, symptoms were observed in 239 (49%) of the partially impacted third molars. When we compare the completely impacted and partially impacted teeth with each other in terms of symptoms, we see that the number of asymptomatic teeth is higher in both groups (
Table 8).
4. Discussion
Impacted teeth are teeth that cannot be found in the normal position in the mouth, have not erupted, usually cause pathology, and need to be treated. All permanent teeth may remain impacted in the dental arch. The most impacted are mandibular and maxillary third molars, maxillary canine, and mandibular and maxillary second premolar and maxillary central incisors [
4]. Since mandibular third molars are the most frequently impacted teeth, their operations are also the most common procedure in maxillofacial surgery [
15,
16,
23,
24,
25].
This retrospective study to assess the prevalence of impacted third molars among the North Cyprus population included 550 patients. In this study, standard clinical radiographic findings were used from patients during a routine examination. A total of 1752 third molars were found in 550 patients. Of all teeth, 740 of the teeth were from female patients, while 1012 were teeth from male patients. Males tend to have a higher incidence of impacted third molars (
p > 0.05). The male to female ratio was 302:248 (1.21:1), with a
p-value of 0.897, which is not statistically significant. Our male to female ratio of impacted molars is similar to the other studies [
3,
26,
27].
The age group in which the third molars were impacted the most was the 20–29 years age group (62%), with the rate of impacted molars decreasing as the age increases. This is similar to other studies and is widely seen when the literature is searched [
4,
26,
28]. The reason for this may be that the third molars tend to cause problems in an earlier period of life, and therefore the related teeth are often surgically extracted in an earlier period of life.
Observed impacted third molars were more impacted in the mandibular arch than in the maxillary arch in both genders. The ratio of mandibular third molar (n = 932) to maxillary third molar (n = 820) was 1.13:1. The greater incidence of impaction in the lower jaw may be due to the more compactness of the bone structure in the mandible.
Third molar impaction is a common problem affecting a large proportion of the population throughout the world. In this study, the incidence of impacted third molars in the North Cyprus population was estimated at 59% (1036/1752). The reported incidence in the present research is higher than published research in the Southeast region [
20,
29,
30]; on the other hand, it is less than published research in the United States of America and Singapore [
5,
31,
32]. This difference may be due to genetic and racial differences, which are two important factors in tooth impaction.
Impacted mandibular third molar teeth were mostly found in the mesioangular position (42%) and were least observed in the distoangular (4%) position. In the maxillary arch, the most common type was vertical impaction (62%), and the least common type was horizontal impaction (3%). According to reports from Pakistan, the USA, Nigeria, China, Thailand, Spain, and Malaysia, the most common impaction type is mesioangular in the maxilla. However, other studies have shown that vertical impaction is the most common impaction type in maxilla, similar to our findings [
1,
5].
It is controversial whether impacted teeth can cause root resorption of the adjacent teeth. In our study, we found that 21 teeth (2%) showed root resorption of the adjacent teeth. This value was lower than the study of Nitzan [
23] but higher than the study of Yamaoka [
18].
Findings in this study indicated that pericoronitis was the most common symptom for the third molars. However, a significant portion of the partially impacted (60%) and completely impacted (73%) third molars appear to be asymptomatic.
A limitation of this study is that it only considered one health center. The wide age range of the people included in the study may suggest that the results of the study are not representative of the general population. However, the primary aim of this study was to investigate the frequency of impacted teeth in patients attending our department. It should also be noted that a large sample population should be considered for further studies with additional parameters such as symptoms of third molars.
5. Conclusions
A huge proportion of third molars are impacted in the North Cyprus population. The degree of impaction of wisdom teeth and the problems they cause should be well evaluated, and the surgical approach should be considered according to the baseline of this data. Such a study has never been done in North Cyprus before. Therefore, this study helps in revealing the impact rate on the population and will be of further use in guiding larger subsequent studies.
Author Contributions
B.G.Ç.G. was a principal investigator and a major contributor to data collection, data entry, manuscript writing, and literature search. K.O. was a co-investigator and supervisor of the study. E.H. was a co-investigator and a major contributor to statistics. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki, and approved by the Institutional Review Board of the TRNC Ministry of Health inpatient treatment institutions (Ref: YTK0,000-6000-14/446/Approval/2014).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank all the participants who cooperated with us and contributed to the creation of the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hashemipour, M.A.; Tahmasbi-Arashlow, M.; Fahimi-Hanzaei, F. Incidence of impacted mandibular and maxillary third molars: A radiographic study in a Southeast Iran population. Med. Oral Patol. Oral Cir. Bucal 2013, 18, 140–145. [Google Scholar] [CrossRef]
- Kaya, G.S.; Aslan, M.; Ömezli, M.M.; Dayi, E. Some morphological features related to mandibular third molar impaction. J. Clin. Exp. Dent. 2010, 2, 12–17. [Google Scholar] [CrossRef]
- Doğan, N.; Orhan, K.; Günaydin, Y.; Köymen, R.; Okçu, K.; Uçok, O. Unerupted mandibular third molars: Symptoms, associated pathologies, and indications for removal in a Turkish population. Quintessence Int. 2007, 38, 497–505. [Google Scholar]
- Syed, K.B.; Zaheer, K.B.; Ibrahim, M.; Bagi, M.A.; Assiri, M.A. Prevalence of Impacted Molar Teeth among Saudi Population in Asir Region, Saudi Arabia—A Retrospective Study of 3 Years. J. Int. Oral Health 2013, 5, 43–47. [Google Scholar] [PubMed]
- Quek, S.L.; Tay, C.K.; Tay, K.H.; Toh, S.L.; Lim, K.C. Pattern of third molar impaction in a Singapore Chinese population: A retrospective radiographic survey. Int. J. Oral Maxillafac. Surg. 2003, 32, 548–552. [Google Scholar] [CrossRef]
- Hugoson, A.; Kugelberg, C.F. The prevalence of third molars in a Swedish population. An epidemiological study. Community Dent. Health 1988, 5, 121–138. [Google Scholar]
- Ma’aita, J.; Alwrikat, A. Is the mandibular third molar a risk factor for mandibular angle fracture? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 143–146. [Google Scholar] [CrossRef]
- Almendros-Marqués, N.; Alaejos-Algarra, E.; Quinteros-Borgarello, M.; Berini-Aytés, L.; Gay-Escoda, C. Factors influencing the prophylactic removal of asymptomatic impacted lower third molars. Int. J. Oral Maxillofac. Surg. 2008, 37, 29–35. [Google Scholar] [CrossRef]
- Breik, O.; Grubor, D. The incidence of mandibular third molar impactions in different skeletal face types. Aust. Dent. J. 2008, 53, 320–324. [Google Scholar] [CrossRef]
- Sağlam, A.A.; Tüzüm, Ş. Clinical and radiographic investigation of the incidence, complications, and suitable removal times for fully impacted teeth in the Turkish population. Quintessence Int. 2003, 34, 53–59. [Google Scholar]
- Ventä, I.; Ylipaavalniemi, P.; Turtola, L. Clinical outcome of third molars in adults followed during 18 years. J Oral Maxillofac. Surg. 2004, 62, 182–185. [Google Scholar] [CrossRef]
- Chu, F.C.S.; Li, T.K.L.; Lui, V.K.B.; Newsome, P.R.H.; Chow, R.L.K.; Cheung, L.K. Prevalence of impacted teeth and associated pathologies-a radiographic study of the Hong Kong Chinese population. Hong Kong Med. J. 2003, 9, 158–163. [Google Scholar]
- Ventä, I.; Turtola, P.; Ylipaavalniemi, P. Radiographic follow-up of impacted third molars from age 20 to 32 years. Int. J. Oral Maxillofac. Surg. 2001, 30, 54–57. [Google Scholar] [CrossRef]
- Lima, C.J.; Silva, L.C.; Melo, M.R.; Santos, J.A.; Santos, T.S. Evaluation of the agreement by examiners according to classifications of third molars. Med. Oral Patol. Oral Cir. Bucal 2012, 17, 216–281. [Google Scholar] [CrossRef]
- Guillaumet-Claure, M.A.; Juiz-Camps, A.M.; Gay-Escoda, C. Prevalence of intraoperative and postoperative iatrogenic mandibular fractures after lower third molar extraction: A systematic review. J. Clin. Exp. Dent. 2022, 14, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, A.; Molinero-Mourelle, P.; Ferrillo, M.; Cobo-Vázquez, C.; Sanchez-Labrador, L.; Ammendolia, A.; Migliario, M.; de Sire, A. Type I Collagen-Based Devices to Treat Nerve Injuries after Oral Surgery Procedures. A Systematic Review. Appl. Sci. 2021, 11, 3927. [Google Scholar] [CrossRef]
- Brann, C.R.; Brickley, M.R.; Shepherd, J.P. Factors influencing nerve damage during lower third molar surgery. Br. Dent. J. 1999, 186, 514–516. [Google Scholar] [CrossRef]
- Yamaoka, M.; Furusawa, K.; Ikeda, M.; Hasegawa, T. Root resorption of mandibular second molar teeth associated with the presence of the third molars. Aust. Dent. J. 1999, 44, 112–116. [Google Scholar] [CrossRef]
- Bataineh, B.A.; Albashaireh, S.Z.; Hazza’a, M.A. The surgical removal of mandibular third molars: A study in decision making. Quintessence Int. 2002, 33, 613–617. [Google Scholar]
- Hattab, F.N.; Fahmy, M.S.; Rawashdeh, M.A. Impaction status of third molars in Jordians students. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1995, 79, 24–29. [Google Scholar] [CrossRef]
- Obiechina, E.A.; Arotiba, T.J.; Fasola, O.A. Third molar impaction: Evaluation of the symptoms and pattern of impaction of mandibular third molar teeth in Nigerians. Odonto-Stomatol. Trop. 2001, 93, 22–25. [Google Scholar]
- Obiechina, E.A.; Oji, C.; Fasola, O.A. Impacted third molars: Depth of impaction and surgical methods of extraction among Nigerians. Odonto-Stomatol. Trop. 2001, 94, 33–36. [Google Scholar]
- Nitzan, D.W.; Tal, O.; Sela, M.N.; Shteyer, A. Pericoronitis: A reappraisal of its clinical and microbiologic aspects. J. Oral Maxillofac. Surg. 1985, 43, 510–516. [Google Scholar] [CrossRef]
- Othman, R. Impacted mandibular third molars among patients attending Hospital UniversitiSains Malaysia. Arch. Orofac. Sci. 2009, 4, 7–12. [Google Scholar]
- Stecker, S.S.; Beiraghi, S.; Hodges, J.S.; Peterson, V.S.; Myers, S.L. Prevalence of dental anomalies in a Southeast Asian population in the Minneapolis/Saint Paul metropolitan area. Northwest Dent. 2007, 86, 25–28. [Google Scholar]
- Ioannis, A. Prevalence of impacted teeth in a Greek population. J. Investig. Clin. Dent. 2011, 2, 1–8. [Google Scholar]
- Peterson, L.J. Principles of Management of Impacted Teeth. In Contemporary Oral and Maxillofacial Surgery; Ellis, E., Hupp, J.R., Tucker, M.R., Eds.; Mosby: St. Louis, MO, USA, 2003; pp. 184–213. [Google Scholar]
- Shetty, D.C. Epidemiological Status of 3rd Molars-Their Clinical Implications. J. Oral Health Comm. Dent. 2010, 4, 12–15. [Google Scholar] [CrossRef]
- Eliasson, S.; Heimdahl, A.; Nordenram, A. Pathological changes related to long-term impaction of third molars. A radiographic study. Int. J. Oral Maxillofac. Surg. 1989, 18, 10–12. [Google Scholar] [CrossRef]
- Rajasuo, A.; Murtomaa, H.; Meurman, J.H. Comparison of the clinical status of third molars of young men in 1949 and 1990. Oral Surg. Oral Med. Oral Pathol. 1993, 76, 694–698. [Google Scholar] [CrossRef]
- Morris, C.R.; Jerman, A.C. Panoramic radiographic survey: A study of embedded third molars. J. Oral Surg. 1971, 29, 122–125. [Google Scholar]
- Bishara, S.E. Impacted maxillary canines: A review. Am. J. Orthod. Dentofac. Ortho. 1992, 101, 159–171. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}