
Pulpal Response to the Combined Use of Mineral Trioxide Aggregate and Iloprost for Direct Pulp Capping

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Estimation
2.2. Sample Selection, Animal Preparation, Randomization, and Grouping
2.3. Surgical Procedures
2.4. Sample Preparation
2.5. Histological Examination
2.6. Statistical Analysis
3. Results
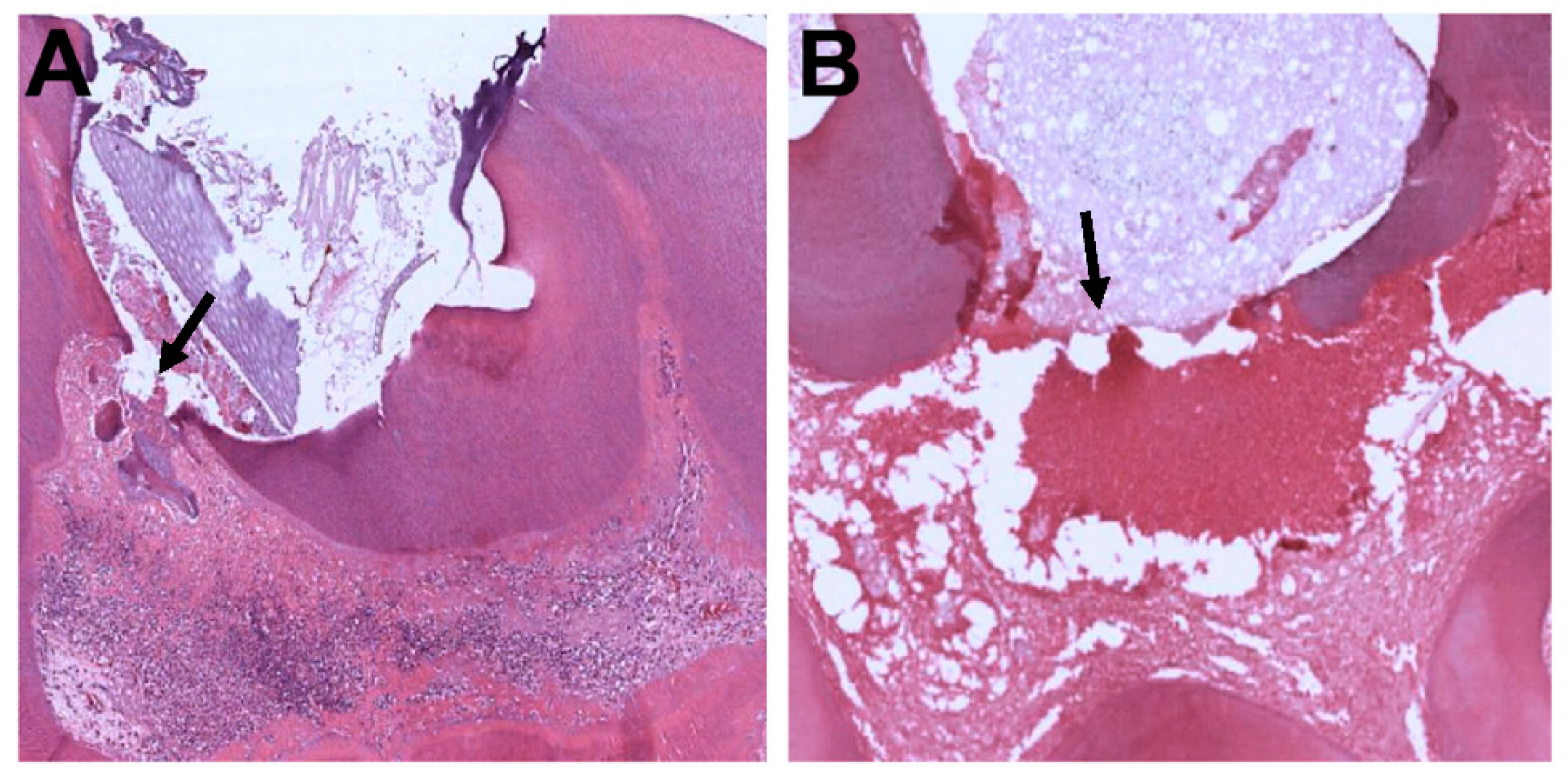
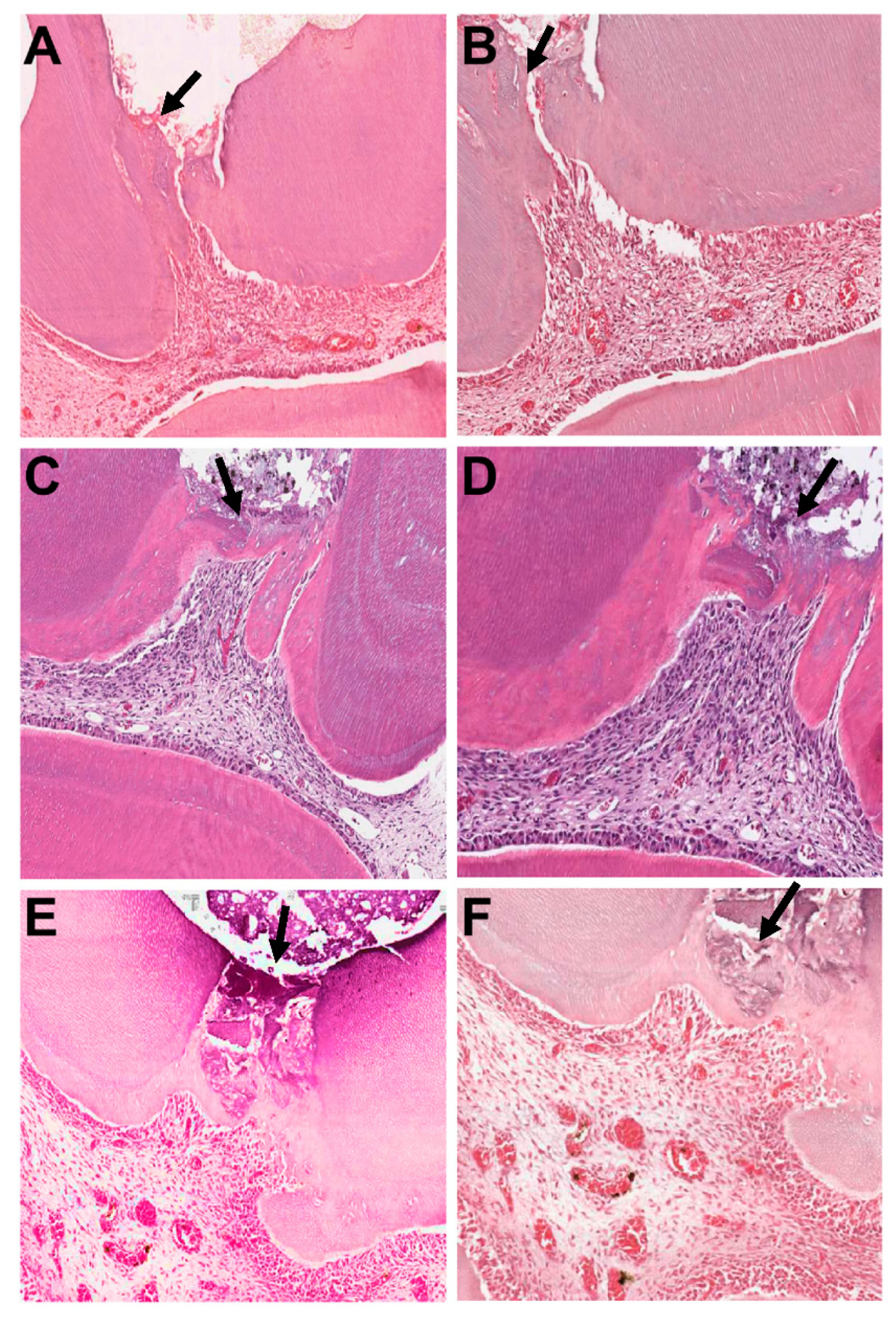
3.1. First Week of Observation
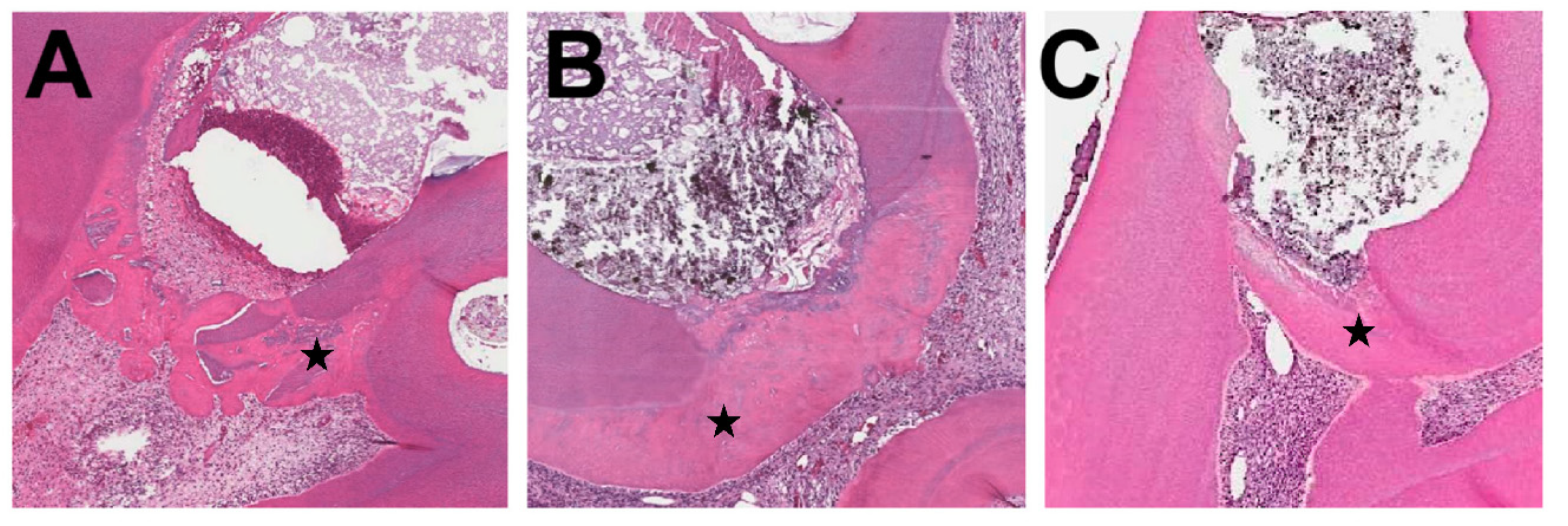
3.2. Four-Week Observation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aguilar, P.; Linsuwanont, P. Vital Pulp Therapy in Vital Permanent Teeth with Cariously Exposed Pulp: A Systematic Review. J. Endod. 2011, 37, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Saghiri, M.A.; Asatourian, A.; Sorenson, C.M.; Sheibani, N. Role of Angiogenesis in Endodontics: Contributions of Stem Cells and Proangiogenic and Antiangiogenic Factors to Dental Pulp Regeneration. J. Endod. 2015, 41, 797–803. [Google Scholar] [CrossRef]
- Zhang, W.; Yelick, P.C. Vital Pulp Therapy—Current Progress of Dental Pulp Regeneration and Revascularization. Int. J. Dent. 2010, 2010, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Limjeerajarus, C.N.; Osathanon, T.; Manokawinchoke, J.; Pavasant, P. Iloprost Up-regulates Vascular Endothelial Growth Factor Expression in Human Dental Pulp Cells In Vitro and Enhances Pulpal Blood Flow In Vivo. J. Endod. 2014, 40, 925–930. [Google Scholar] [CrossRef]
- Loureiro, M.J.; Cotrim, C.; Simões, O.; Miranda, R.; Cordeiro, P.; Carrageta, M. Acute hemodynamic effect of inhaled iloprost in pulmonary artery hypertension evaluated with echocardiography. Cardiovasc. Ultrasound 2007, 5, 41–43. [Google Scholar] [CrossRef] [PubMed]
- McHugh, N.J.; Csuka, M.; Watson, H.; Belcher, G.; Amadi, A.; Ring, E.F.; Black, C.M.; Maddison, P.J. Infusion of iloprost, a prostacyclin analogue, for treatment of Raynaud’s phenomenon in systemic sclerosis. Ann. Rheum. Dis. 1988, 47, 43–47. [Google Scholar] [CrossRef]
- Limjeerajarus, C.N.; Chanarattanubol, T.; Trongkij, P.; Rujiwanichkul, M.; Pavasant, P. Iloprost Induces Tertiary Dentin Formation. J. Endod. 2014, 40, 1784–1790. [Google Scholar] [CrossRef]
- Seang, S.; Pavasant, P.; Limjeerajarus, C.N. Iloprost Induces Dental Pulp Angiogenesis in a Growth Factor–free 3-Dimensional Organ Culture System. J. Endod. 2018, 44, 759–764.e2. [Google Scholar] [CrossRef] [PubMed]
- Linsuwanont, P.; Wimonsutthikul, K.; Pothimoke, U.; Santiwong, B. Treatment Outcomes of Mineral Trioxide Aggregate Pulpotomy in Vital Permanent Teeth with Carious Pulp Exposure: The Retrospective Study. J. Endod. 2017, 43, 225–230. [Google Scholar] [CrossRef]
- Parinyaprom, N.; Nirunsittirat, A.; Chuveera, P.; Na Lampang, S.; Srisuwan, T.; Sastraruji, T.; Bua-On, P.; Simprasert, S.; Khoipanich, I.; Sutharaphan, T.; et al. Outcomes of Direct Pulp Capping by Using Either ProRoot Mineral Trioxide Aggregate or Biodentine in Permanent Teeth with Carious Pulp Exposure in 6- to 18-Year-Old Patients: A Randomized Controlled Trial. J. Endod. 2018, 44, 341–348. [Google Scholar] [CrossRef]
- Cervino, G.; Laino, L.; D’Amico, C.; Russo, D.; Nucci, L.; Amoroso, G.; Gorassini, F.; Tepedino, M.; Terranova, A.; Gambino, D.; et al. Mineral Trioxide Aggregate Applications in Endodontics: A Review. Eur. J. Dent. 2020, 14, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.R.P.; Torabinejad, M.; Abedi, H.R.; Bakland, L.K.; Kariyawasam, S.P. Using Mineral Trioxide Aggregate as a Pulp-Capping Material. J. Am. Dent. Assoc. 1996, 127, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.-M.; Chang, S.-W.; Park, K.-R.; Herr, L.; Kim, E.-C. Combined Effects of Growth Hormone and Mineral Trioxide Aggregate on Growth, Differentiation, and Angiogenesis in Human Dental Pulp Cells. J. Endod. 2016, 42, 269–275. [Google Scholar] [CrossRef]
- Han, J.-W.; Lee, B.-N.; Kim, S.-M.; Koh, J.-T.; Min, K.-S.; Hwang, Y.-C. Odontogenic Potential of Parathyroid Hormone–related Protein (107-111) Alone or in Combination with Mineral Trioxide Aggregate in Human Dental Pulp Cells. J. Endod. 2017, 43, 2054–2060. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.-M.; Kim, W.-J.; Lim, H.-S.; Choi, N.-K.; Kim, S.-H.; Kim, S.-M.; Jung, J.-Y. Combination of Mineral Trioxide Aggregate and Platelet-rich Fibrin Promotes the Odontoblastic Differentiation and Mineralization of Human Dental Pulp Cells via BMP/Smad Signaling Pathway. J. Endod. 2016, 42, 82–88. [Google Scholar] [CrossRef]
- Chang, S.-W.; Kim, J.-Y.; Kim, M.-J.; Kim, G.-H.; Yi, J.-K.; Lee, D.-W.; Kum, K.-Y.; Kim, E.-C. Combined effects of mineral trioxide aggregate and human placental extract on rat pulp tissue and growth, differentiation and angiogenesis in human dental pulp cells. Acta Odontol. Scand. 2015, 74, 298–306. [Google Scholar] [CrossRef]
- Chen, J.; Cui, C.; Qiao, X.; Yang, B.; Yu, M.; Guo, W.; Tian, W. Treated dentin matrix paste as a novel pulp capping agent for dentin regeneration. J. Tissue Eng. Regen. Med. 2017, 11, 3428–3436. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Wang, S.; Dong, Y. Evaluation of a Bioceramic as a Pulp Capping Agent In Vitro and In Vivo. J. Endod. 2015, 41, 652–657. [Google Scholar] [CrossRef]
- Kim, D.-H.; Jang, J.-H.; Lee, B.-N.; Chang, H.-S.; Hwang, I.-N.; Oh, W.-M.; Kim, S.-H.; Min, K.-S.; Koh, J.-T.; Hwang, Y.-C. Anti-inflammatory and Mineralization Effects of ProRoot MTA and Endocem MTA in Studies of Human and Rat Dental Pulps In Vitro and In Vivo. J. Endod. 2018, 44, 1534–1541. [Google Scholar] [CrossRef]
- Long, Y.; Liu, S.; Zhu, L.; Liang, Q.; Chen, X.; Dong, Y. Evaluation of Pulp Response to Novel Bioactive Glass Pulp Capping Materials. J. Endod. 2017, 43, 1647–1650. [Google Scholar] [CrossRef]
- McNamara, R.P.; Henry, M.A.; Schindler, W.G.; Hargreaves, K.M. Biocompatibility of Accelerated Mineral Trioxide Aggregate in a Rat Model. J. Endod. 2010, 36, 1851–1855. [Google Scholar] [CrossRef]
- Watts, A.; Paterson, R.C.; Cohen, B.D.; Combe, E.C. Pulp response to a novel adhesive calcium hydroxide based cement. Eur. J. Prosthodont. Restor. Dent. 1994, 3, 27–33. [Google Scholar]
- Maurice, C.G.; Schour, I. Experimental Cavity Preparations in the Molar of the Rat. J. Dent. Res. 1955, 34, 429–434. [Google Scholar] [CrossRef]
- Berman, D.S.; Massler, M. Experimental Pulpotomies in Rat Molars. J. Dent. Res. 1958, 37, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Vallés, M.; Mercadé, M.; Duran-Sindreu, F.; Bourdelande, J.L.; Roig, M. Influence of Light and Oxygen on the Color Stability of Five Calcium Silicate–based Materials. J. Endod. 2013, 39, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Rouhani, A.; Samiee, S.; Jafarzadeh, H. Effect of Dentin Bonding Agent on the Prevention of Tooth Discoloration Produced by Mineral Trioxide Aggregate. Int. J. Dent. 2011, 2012, 1–3. [Google Scholar] [CrossRef]
- Namazikhah, M.S.; Nekoofar, M.H.; Sheykhrezae, M.S.; Salariyeh, S.; Hayes, S.J.; Bryant, S.T.; Mohammadi, M.M.; Dummer, P.M.H. The effect of pH on surface hardness and microstructure of mineral trioxide aggregate. Int. Endod. J. 2007, 41, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Borna, Z.; Rahimi, S.; Shahi, S.; Valizadeh, H.; Ghojazadeh, M.; Yavari, H.R. Placement in an acidic environment increase the solubility of white mineral trioxide aggregate. J. Conserv. Dent. 2013, 16, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Lan, W.-H.; Lan, W.-C.; Wang, T.-M.; Lee, Y.-L.; Tseng, W.-Y.; Lin, C.-P.; Jeng, J.-H.; Chang, M.-C. Cytotoxicity of conventional and modified glass ionomer cements. Oper. Dent. 2003, 28, 251–259. [Google Scholar]
- Alhadainy, H.A.; Himel, V.T. Evaluation of the sealing ability of amalgam, Cavit, and glass ionomer cement in the repair of furcation perforations. Oral Surg. Oral Med. Oral Pathol. 1993, 75, 362–366. [Google Scholar] [CrossRef]
- Kakehashi, S.; Stanley, H.; Fitzgerald, R. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg. Oral Med. Oral Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef]
- Goldberg, M.; Njeh, A.; Uzunoglu, E. Is Pulp Inflammation a Prerequisite for Pulp Healing and Regeneration? Mediat. Inflamm. 2015, 2015, 1–11. [Google Scholar] [CrossRef]
- Farges, J.-C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental Pulp Defence and Repair Mechanisms in Dental Caries. Mediat. Inflamm. 2015, 2015, 1–16. [Google Scholar] [CrossRef]
- Limjeerajarus, C.N.; Sonntana, S.; Pajaree, L.; Kansurang, C.; Pitt, S.; Saowapa, T.; Prasit, P. Prolonged release of iloprost enhances pulpal blood flow and dentin bridge formation in a rat model of mechanical tooth pulp exposure. J. Oral Sci. 2019, 61, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Um, S.; Jang, J.-H.; Seo, B.M. Effects of VEGF and FGF-2 on proliferation and differentiation of human periodontal ligament stem cells. Cell Tissue Res. 2012, 348, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Okiji, T.; Yoshiba, K. Reparative Dentinogenesis Induced by Mineral Trioxide Aggregate: A Review from the Biological and Physicochemical Points of View. Int. J. Dent. 2009, 2009, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Decup, F.; Six, N.; Palmier, B.; Buch, D.; Lasfargues, J.J.; Salih, E.; Goldberg, M. Bone sialoprotein-induced reparative dentinogenesis in the pulp of rat’s molar. Clin. Oral Investig. 2000, 4, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Kuratate, M.; Yoshiba, K.; Shigetani, Y.; Yoshiba, N.; Ohshima, H.; Okiji, T. Immunohistochemical Analysis of Nestin, Osteopontin, and Proliferating Cells in the Reparative Process of Exposed Dental Pulp Capped with Mineral Trioxide Aggregate. J. Endod. 2008, 34, 970–974. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Inflammatory Cell Response | Hard Tissue Formation | Quality of Dentin Formation in the Bridge |
|---|---|---|---|
| 1 | Absent or few inflammatory cells | Heavy: hard tissue deposition as complete and continuous dentin bridge | Regular pattern of tubules |
| 2 | Mild: inflammatory cells only next to dentin bridge or area of pulp exposition | Moderate: hard tissue formation as incomplete and discontinuous dentin bridge | Irregular pattern of tubules |
| 3 | Moderate: inflammatory cells are observed in the part of coronal pulp | Slight: a layer of scattered and foggy hard tissue deposition | No tubules present |
| 4 | Severe: all coronal pulp | No hard tissue deposition |
| Time | Group | No. of Specimen | Inflammatory Cell Response Score (%) | Hard Tissue Formation Score (%) | Quality of Dentin Formation Score (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | |||
| Week 1 | Control | 9 | 0.0 | 0.0 | 33.3 | 66.7 | 0.0 | 0.0 | 55.6 | 44.4 | - | - | - |
| Iloprost | 9 | 44.4 | 55.6 | 0.0 | 0.0 | 0.0 | 44.4 | 44.4 | 11.1 | - | - | - | |
| MTA | 7 | 28.6 | 28.6 | 42.9 | 0.0 | 0.0 | 85.7 | 14.3 | 0.0 | - | - | - | |
| MTA- ILO | 8 | 37.5 | 50.0 | 12.5 | 0.0 | 12.5 | 62.5 | 25.0 | 0.0 | - | - | - | |
| Week 4 | Control | 7 | 57.1 | 28.6 | 14.3 | 0.0 | 0.0 | 28.6 | 42.8 | 28.6 | 0.0 | 28.5 | 71.5 |
| Iloprost | 10 | 50.0 | 40.0 | 10.0 | 0.0 | 50.0 | 30.0 | 20.0 | 0.0 | 10.0 | 70.0 | 20.0 | |
| MTA | 11 | 63.6 | 36.4 | 0.0 | 0.0 | 72.7 | 9.1 | 18.2 | 0.0 | 27.3 | 54.5 | 18.2 | |
| MTA- ILO | 9 | 77.8 | 22.2 | 0.0 | 0.0 | 77.8 | 0.0 | 22.2 | 0.0 | 55.6 | 22.2 | 22.2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeshari, A.; Khounganian, R.; Mahdi, W.; Aljarbou, F.; Bhandi, S.; Alsubait, S. Pulpal Response to the Combined Use of Mineral Trioxide Aggregate and Iloprost for Direct Pulp Capping. Appl. Sci. 2021, 11, 3702. https://doi.org/10.3390/app11083702
Almeshari A, Khounganian R, Mahdi W, Aljarbou F, Bhandi S, Alsubait S. Pulpal Response to the Combined Use of Mineral Trioxide Aggregate and Iloprost for Direct Pulp Capping. Applied Sciences. 2021; 11(8):3702. https://doi.org/10.3390/app11083702
Chicago/Turabian StyleAlmeshari, AlAnoud, Rita Khounganian, Wael Mahdi, Fahd Aljarbou, Shilpa Bhandi, and Sara Alsubait. 2021. "Pulpal Response to the Combined Use of Mineral Trioxide Aggregate and Iloprost for Direct Pulp Capping" Applied Sciences 11, no. 8: 3702. https://doi.org/10.3390/app11083702
APA StyleAlmeshari, A., Khounganian, R., Mahdi, W., Aljarbou, F., Bhandi, S., & Alsubait, S. (2021). Pulpal Response to the Combined Use of Mineral Trioxide Aggregate and Iloprost for Direct Pulp Capping. Applied Sciences, 11(8), 3702. https://doi.org/10.3390/app11083702