
Machine Learning in Chronic Pain Research: A Scoping Review

 , , ,
, , , 
Abstract
1. Introduction
- RQ1: Which ML methods have been used?
- RQ2: Which data have been used?
- RQ3: Were patient-generated data used?
- RQ4: Which chronic pain conditions were applied with ML algorithms?
- RQ5: Which stages (e.g., assessment/diagnosis or treatment) of chronic pain care were addressed?
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria
- The paper must be written in English.
- The reported trials must be done on humans.
- The trials must include patients with chronic pain.
- The study must have been completed.
- This review focused on chronic pain studies where the source of the pain was not known, such as fibromyalgia (FM) and chronic low back pain (CLBP).
2.3. Exclusion Criteria
- Review papers were excluded.
- Studies on acute pain were excluded.
- Headache, migraine, and chest pain were excluded.
- Postoperative pain and cancer-related pain were excluded.
- Studies with only healthy research participants were excluded.
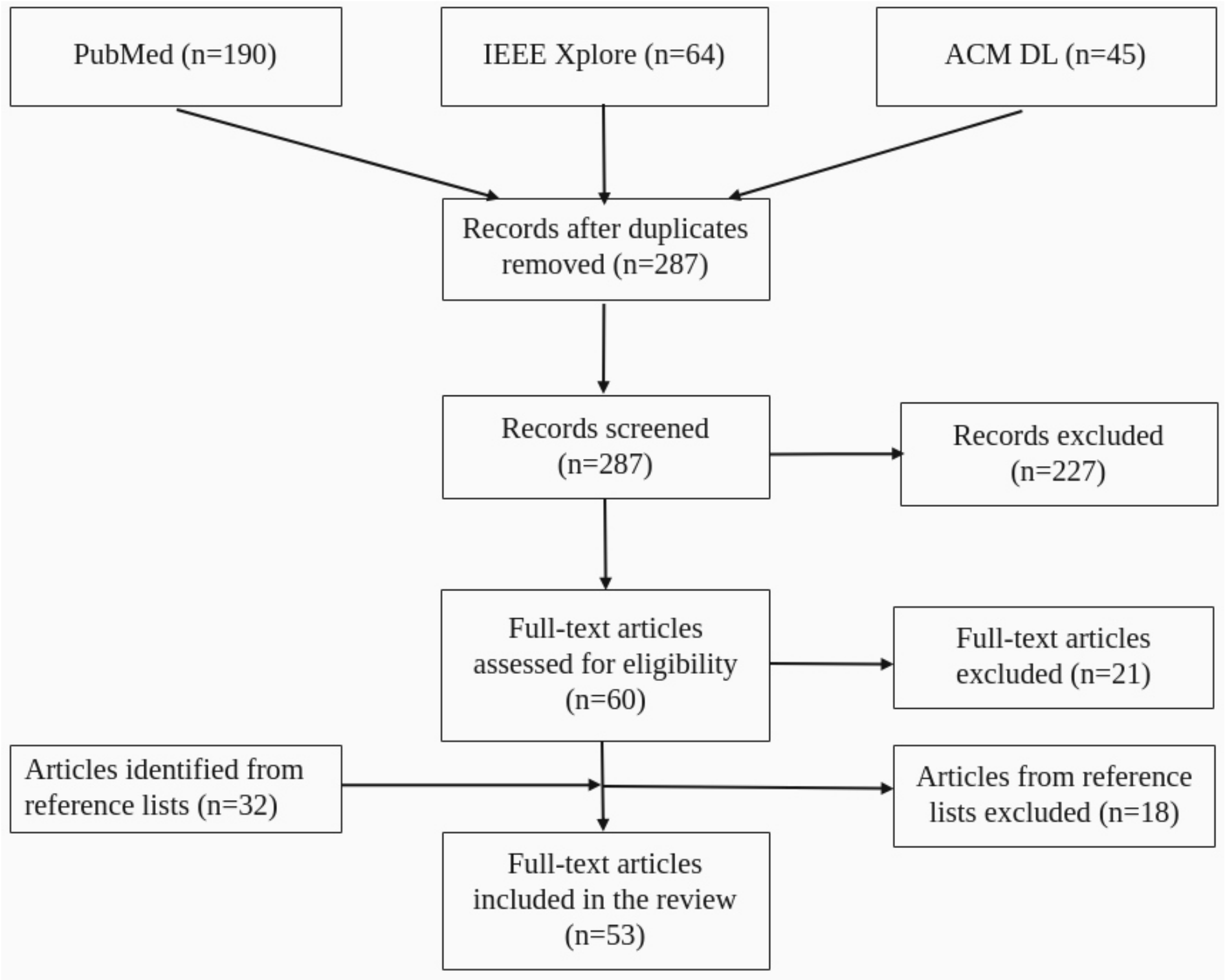
2.4. Screening and Full-Text Reading
- Wrong population (only healthy participants included in trials, no patients with chronic pain): twelve papers (all from the original search)
- Wrong publication type: nine papers (five from the original search and four from the references)
- Wrong study design: twelve papers (seven from the original search and five from the references)
- Studies not using ML: ten papers (all from the papers found in the reference lists)
3. Results
3.1. Applications of Machine Learning in Chronic Pain Research
- Classification/diagnosis of patients with chronic pain using structured health data
- Classification/diagnosis of patients with chronic pain using text and images
- Genomics approaches and pain biomarker identification
- Treatment
- Self-management
- Measurement of pain intensity
3.2. Machine Learning Algorithms
3.2.1. Supervised Algorithms
3.2.2. Unsupervised Algorithms
3.3. Data
3.4. Types of Chronic Pain That May Benefit from ML Research
4. Discussion
4.1. Important Findings
4.2. Recent Research
4.3. Potential Limitations of This Review
4.4. Future Research Directions
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | analysis of variance |
| AS | ankylosing spondylitis |
| CFS | chronic fatigue syndrome |
| CLBP | chronic low back pain |
| CNN | convolutional neural network |
| CPP | chronic pelvic pain |
| CRPS | complex regional pain syndrome |
| DT | decision tree |
| EHR | electronic health record |
| EMG | electromyography |
| FM | fibromyalgia |
| fMRI | functional magnetic resonance imaging |
| IBS | irritable bowel syndrome |
| IC | interstitial cystitis/bladder pain syndrome |
| kNN | k-nearest neighbours |
| LBP | low back pain |
| LDA | linear discriminant analysis |
| LUCCK | learning using concave and convex kernels |
| ML | machine learning |
| MLP | multilayer perceptron |
| MPS | myofascial pain syndrome |
| MRI | magnetic resonance imaging |
| MVPA | multivariate pattern analysis |
| PROM | patient reported outcome measures |
| PRoNTo | pattern recognition for neuroimaging toolbox |
| RA | rheumatoid arthritis |
| RF | random forest |
| RL | reinforcement learning |
| RQ | research question |
| SEMG | surface electromyography |
| sMRI | structural magnetic resonance imaging |
| SVM | support vector machine |
| SVR | support vector regression |
| TN | trigeminal neuralgia |
| VAS | visual analogue scale |
References
- Mills, S.; Torrance, N.; Smith, B.H. Identification and Management of Chronic Pain in Primary Care: A Review. Curr. Psychiatry Rep. 2016, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Landmark, T.; Romundstad, P.; Dale, O.; Borchgrevink, P.C.; Kaasa, S. Estimating the prevalence of chronic pain: Validation of recall against longitudinal reporting (the HUNT pain study). Pain 2012, 153, 1368–1373. [Google Scholar] [CrossRef]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: A systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef]
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef]
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef]
- Hadi, M.A.; McHugh, G.A.; Closs, S.J. Impact of Chronic Pain on Patients’ Quality of Life: A Comparative Mixed-Methods Study. J. Patient Exp. 2019, 6, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef]
- Girardi, A.; Curran, M.S. The comorbidity of chronic pain and depression. Nurs. Made Incred. Easy 2019, 17, 50–54. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Barnish, M.S.; Jones, G.T. Persons with chronic widespread pain experience excess mortality: Longitudinal results from UK Biobank and meta-analysis. Ann. Rheum. Dis. 2017, 76, 1815–1822. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Pain as a public health challenge. In Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research; National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Nachemson, A. Chronic pain–the end of the welfare state? Qual. Life Res. 1994, 3, S11–S17. [Google Scholar] [CrossRef]
- Landmark, T.; Romundstad, P.; Dale, O.; Borchgrevink, P.C.; Vatten, L.; Kaasa, S. Chronic pain: One year prevalence and associated characteristics (the HUNT pain study). Scand. J. Pain 2013, 4, 182–187. [Google Scholar] [CrossRef]
- Merskey, H.; Bogduk, N. (Eds.) Classification of Chronic Pain: Task Force on Taxonomy of the International Association for the Study of Pain (IASP), 2nd ed.; IASP Press: Seattle, WA, USA, 1994. [Google Scholar]
- Ashburn, M.A.; Staats, P.S. Management of chronic pain. Lancet 1999, 353, 1865–1869. [Google Scholar] [CrossRef]
- Grichnik, K.P.; Ferrante, F.M. The difference between acute and chronic pain. Mt. Sinai J. Med. 1991, 58, 217–220. [Google Scholar] [PubMed]
- Paster, R.Z. Chronic Pain Management Issues in the Primary Care Setting and the Utility of Long-Acting Opioids. Expert Opin. Pharmacother. 2010, 11, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Theodoridis, S.; Koutroumbas, K. Pattern Recognition, Fourth Edition, 4th ed.; Academic Press, Inc.: Cambridge, MA, USA, 2008. [Google Scholar]
- Smith, A.; López-Solà, M.; McMahon, K.; Pedler, A.; Sterling, M. Multivariate pattern analysis utilizing structural or functional MRI-In individuals with musculoskeletal pain and healthy controls: A systematic review. Semin. Arthritis Rheum. 2017, 47, 418–431. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pombo, N.; Araújo, P.; Viana, J. Knowledge discovery in clinical decision support systems for pain management: A systematic review. Artif. Intell. Med. 2014, 60, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Cheng, D.; Houle, T.T.; Chen, L.; Zhang, W.; Deng, H. Machine learning methods for automatic pain assessment using facial expression information: Protocol for a systematic review and meta-analysis. Medicine 2018, 97, e13421. [Google Scholar] [CrossRef]
- Lötsch, J.; Ultsch, A. Machine learning in pain research. Pain 2018, 159, 623. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005. [Google Scholar] [CrossRef]
- Liang, Z.; Zhang, G.; Xu, S.; Ou, A.; Fang, J.; Xu, N.; Fu, W. A kernel-decision tree based algorithm for outcome prediction on acupuncture for neck pain: A new method for interim analysis. In Proceedings of the 2011 IEEE International Conference on Bioinformatics and Biomedicine Workshops (BIBMW), Atlanta, GA, USA, 12–15 November 2011; pp. 760–764. [Google Scholar] [CrossRef]
- Zhang, G.; Liang, Z.; Yin, J.; Fu, W.; Li, G.Z. A similarity based learning framework for interim analysis of outcome prediction of acupuncture for neck pain. Int. J. Data Min. Bioinform. 2013, 8, 381–395. [Google Scholar] [CrossRef]
- Melidis, C.; Denham, S.L.; Hyland, M.E. A test of the adaptive network explanation of functional disorders using a machine learning analysis of symptoms. Biosystems 2018, 165, 22–30. [Google Scholar] [CrossRef]
- Davis, F.; Gostine, M.; Roberts, B.; Risko, R.; Cappelleri, J.C.; Sadosky, A. Characterizing classes of fibromyalgia within the continuum of central sensitization syndrome. J. Pain Res. 2018, 11, 2551–2560. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Yu, N.Y.; Jiang, C.F.; Chang, S.H. Characterizing the SEMG patterns with myofascial pain using a multi-scale wavelet model through machine learning approaches. J. Electromyogr. Kinesiol. 2018, 41, 147–153. [Google Scholar] [CrossRef]
- Oliverio, V.; Poli-Neto, O.B. Case study: Classification algorithms comparison for the multi-label problem of chronic pelvic pain diagnosing. In Proceedings of the 2017 IEEE 33rd International Conference on Data Engineering (ICDE), San Diego, CA, USA, 19–22 April 2017; pp. 1507–1509. [Google Scholar] [CrossRef]
- Hall, M.; Frank, E.; Holmes, G.; Pfahringer, B.; Reutemann, P.; Witten, I.H. The WEKA data mining software: An update. ACM SIGKDD Explor. Newsl. 2009, 11, 10–18. [Google Scholar] [CrossRef]
- Yim, Y.R.; Lee, K.E.; Park, D.J.; Kim, S.H.; Nah, S.S.; Lee, J.; Kim, S.K.; Lee, Y.A.; Hong, S.J.; Kim, H.S.; et al. Identifying fibromyalgia subgroups using cluster analysis: Relationships with clinical variables. Eur. J. Pain 2017, 21, 374–384. [Google Scholar] [CrossRef]
- Emir, B.; Masters, E.T.; Mardekian, J.; Clair, A.; Kuhn, M.; Silverman, S.L. Identification of a Potential Fibromyalgia Diagnosis Using Random Forest Modeling Applied to Electronic Medical Records. J. Pain Res. 2015, 8, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Zapirain, B.; Garcia-Chimeno, Y.; Rogers, H. Machine learning techniques for automatic classification of patients with fibromyalgia and arthritis. Int. J. Comput. Trends Technol. (IJCTT) 2015, 25, 149–152. [Google Scholar] [CrossRef]
- Olugbade, T.A.; Aung, M.H.; Bianchi-Berthouze, N.; Marquardt, N.; Williams, A.C. Bi-modal detection of painful reaching for chronic pain rehabilitation systems. In Proceedings of the ICMI ’14 16th International Conference on Multimodal Interaction, Istanbul, Turkey, 12–16 November 2014; ACM: New York, NY, USA, 2014; pp. 455–458. [Google Scholar] [CrossRef]
- Chan, H.; Zheng, H.; Wang, H.; Sterritt, R.; Newell, D. Smart mobile phone based gait assessment of patients with low back pain. In Proceedings of the 2013 Ninth International Conference on Natural Computation (ICNC), Shenyang, China, 23–25 July 2013; pp. 1062–1066. [Google Scholar] [CrossRef]
- Yang, M.; Zheng, H.; Wang, H.; McClean, S.; Hall, J.; Harris, N. A machine learning approach to assessing gait patterns for Complex Regional Pain Syndrome. Med. Eng. Phys. 2012, 34, 740–746. [Google Scholar] [CrossRef]
- Goertzel, B.N.; Pennachin, C.; de Souza Coelho, L.; Maloney, E.M.; Jones, J.F.; Gurbaxani, B. Allostatic load is associated with symptoms in chronic fatigue syndrome patients. Pharmacogenomics 2006, 7, 485–494. [Google Scholar] [CrossRef]
- Fodeh, S.J.; Finch, D.; Bouayad, L.; Luther, S.L.; Ling, H.; Kerns, R.D.; Brandt, C. Classifying clinical notes with pain assessment using machine learning. Med. Biol. Eng. Comput. 2018, 56, 1285–1292. [Google Scholar] [CrossRef]
- Tan, W.K.; Hassanpour, S.; Heagerty, P.J.; Rundell, S.D.; Suri, P.; Huhdanpaa, H.T.; James, K.; Carrell, D.S.; Langlotz, C.P.; Organ, N.L.; et al. Comparison of Natural Language Processing Rules-based and Machine-learning Systems to Identify Lumbar Spine Imaging Findings Related to Low Back Pain. Acad. Radiol. 2018, 25, 1422–1432. [Google Scholar] [CrossRef]
- Zhong, J.; Chen, D.Q.; Hung, P.S.P.; Hayes, D.J.; Liang, K.E.; Davis, K.D.; Hodaie, M. Multivariate pattern classification of brain white matter connectivity predicts classic trigeminal neuralgia. Pain 2018, 159, 2076–2087. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.C.; Rogachov, A.; Hemington, K.S.; Kucyi, A.; Bosma, R.L.; Lindquist, M.A.; Inman, R.D.; Davis, K.D. Multivariate machine learning distinguishes cross-network dynamic functional connectivity patterns in state and trait neuropathic pain. Pain 2018, 159, 1764–1776. [Google Scholar] [CrossRef]
- Rogachov, A.; Cheng, J.C.; Hemington, K.S.; Bosma, R.L.; Kim, J.A.; Osborne, N.R.; Inman, R.D.; Davis, K.D. Abnormal Low-Frequency Oscillations Reflect Trait-Like Pain Ratings in Chronic Pain Patients Revealed through a Machine Learning Approach. J. Neurosci. 2018, 38, 7293–7302. [Google Scholar] [CrossRef] [PubMed]
- Schrouff, J.; Rosa, M.J.; Rondina, J.; Marquand, A.F.; Chu, C.; Richiardi, J.; Phillips, C.; Mourão-Miranda, J. Pattern Recognition for Neuroimaging Toolbox. Neuroinformatics 2013, 11, 319–337. [Google Scholar] [CrossRef]
- Mano, H.; Kotecha, G.; Leibnitz, K.; Matsubara, T.; Sprenger, C.; Nakae, A.; Shenker, N.; Shibata, M.; Voon, V.; Yoshida, W.; et al. Classification and characterisation of brain network changes in chronic back pain: A multicenter study. Wellcome Open Res. 2018, 3. [Google Scholar] [CrossRef]
- Sevel, L.S.; Boissoneault, J.; Letzen, J.E.; Robinson, M.E.; Staud, R. Structural brain changes versus self-report: Machine-learning classification of chronic fatigue syndrome patients. Exp. Brain Res. 2018, 236, 2245–2253. [Google Scholar] [CrossRef] [PubMed]
- López-Solà, M.; Woo, C.W.; Pujol, J.; Deus, J.; Harrison, B.J.; Monfort, J.; Wager, T.D. Towards a neurophysiological signature for fibromyalgia. Pain 2017, 158, 34–47. [Google Scholar] [CrossRef]
- Qin, R.; Meng, H.; Li, M. Continuous pain related behavior recognition from muscle activity and body movements. In Proceedings of the 2016 12th International Conference on Natural Computation, Fuzzy Systems and Knowledge Discovery (ICNC-FSKD), Changsha, China, 13–15 August 2016; pp. 1710–1715. [Google Scholar] [CrossRef]
- Olugbade, T.A.; Bianchi-Berthouze, N.; Marquardt, N.; Williams, A.C. Pain level recognition using kinematics and muscle activity for physical rehabilitation in chronic pain. In Proceedings of the 2015 International Conference on Affective Computing and Intelligent Interaction (ACII), Xi’an, China, 21–24 September 2015; pp. 243–249. [Google Scholar] [CrossRef]
- Labus, J.S.; Van Horn, J.D.; Gupta, A.; Alaverdyan, M.; Torgerson, C.; Ashe-McNalley, C.; Irimia, A.; Hong, J.Y.; Naliboff, B.; Tillisch, K.; et al. Multivariate morphological brain signatures predict chronic abdominal pain patients from healthy control subjects. Pain 2015, 156, 1545–1554. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; O’Shea, A.M.; Craggs, J.G.; Price, D.D.; Letzen, J.E.; Staud, R. Comparison of machine classification algorithms for fibromyalgia: Neuroimages versus self-report. J. Pain 2015, 16, 472–477. [Google Scholar] [CrossRef]
- Sundermann, B.; Burgmer, M.; Pogatzki-Zahn, E.; Gaubitz, M.; Stüber, C.; Wessolleck, E.; Heuft, G.; Pfleiderer, B. Diagnostic classification based on functional connectivity in chronic pain: Model optimization in fibromyalgia and rheumatoid arthritis. Acad. Radiol. 2014, 21, 369–377. [Google Scholar] [CrossRef]
- Callan, D.; Mills, L.; Nott, C.; England, R.; England, S. A tool for classifying individuals with chronic back pain: Using multivariate pattern analysis with functional magnetic resonance imaging data. PLoS ONE 2014, 9, e98007. [Google Scholar] [CrossRef] [PubMed]
- Bagarinao, E.; Johnson, K.A.; Martucci, K.T.; Ichesco, E.; Farmer, M.A.; Labus, J.; Ness, T.J.; Harris, R.; Deutsch, G.; Apkarian, A.V.; et al. Preliminary structural MRI based brain classification of chronic pelvic pain: A MAPP network study. Pain 2014, 155, 2502–2509. [Google Scholar] [CrossRef]
- Ung, H.; Brown, J.E.; Johnson, K.A.; Younger, J.; Hush, J.; Mackey, S. Multivariate classification of structural MRI data detects chronic low back pain. Cereb. Cortex 2012, 24, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Lukkahatai, N.; Walitt, B.; Deandrés-Galiana, E.J.; Fernández-Martínez, J.L.; Saligan, L.N. A predictive algorithm to identify genes that discriminate individuals with fibromyalgia syndrome diagnosis from healthy controls. J. Pain Res. 2018, 11, 2981–2990. [Google Scholar] [CrossRef]
- Chancellor, M.B.; Bartolone, S.N.; Veerecke, A.; Lamb, L.E. Crowdsourcing Disease Biomarker Discovery Research: The IP4IC Study. J. Urol. 2018, 199, 1344–1350. [Google Scholar] [CrossRef]
- Ultsch, A.; Kringel, D.; Kalso, E.; Mogil, J.S.; Lötsch, J. A data science approach to candidate gene selection of pain regarded as a process of learning and neural plasticity. Pain 2016, 157, 2747–2757. [Google Scholar] [CrossRef] [PubMed]
- Braundmeier-Fleming, A.; Russell, N.T.; Yang, W.; Nas, M.Y.; Yaggie, R.E.; Berry, M.; Bachrach, L.; Flury, S.C.; Marko, D.S.; Bushell, C.B.; et al. Stool-based biomarkers of interstitial cystitis/bladder pain syndrome. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef]
- Golabchi, F.N.; Sapienza, S.; Severini, G.; Reaston, P.; Tomecek, F.; Demarchi, D.; Reaston, M.; Bonato, P. Assessing aberrant muscle activity patterns via the analysis of surface EMG data collected during a functional evaluation. BMC Musculoskelet. Disord. 2019, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Sabeti, E.; Gryak, J.; Derksen, H.; Biwer, C.; Ansari, S.; Isenstein, H.; Kratz, A.; Najarian, K. Learning Using Concave and Convex Kernels: Applications in Predicting Quality of Sleep and Level of Fatigue in Fibromyalgia. Entropy 2019, 21, 442. [Google Scholar] [CrossRef]
- Nijeweme-d’Hollosy, W.O.; van Velsen, L.; Poel, M.; Groothuis-Oudshoorn, C.G.M.; Soer, R.; Hermens, H. Evaluation of three machine learning models for self-referral decision support on low back pain in primary care. Int. J. Med. Inform. 2018, 110, 31–41. [Google Scholar] [CrossRef] [PubMed]
- McKernan, L.C.; Lenert, M.C.; Crofford, L.J.; Walsh, C.G. Outpatient Engagement Lowers Predicted Risk of Suicide Attempts in Fibromyalgia. Arthritis Care Res. 2019, 71, 1255–1263. [Google Scholar] [CrossRef]
- Jiang, N.; Luk, K.D.K.; Hu, Y. A Machine Learning-based Surface Electromyography Topography Evaluation for Prognostic Prediction of Functional Restoration Rehabilitation in Chronic Low Back Pain. Spine 2017, 42, 1635–1642. [Google Scholar] [CrossRef]
- Aung, M.S.; Kaltwang, S.; Romera-Paredes, B.; Martinez, B.; Singh, A.; Cella, M.; Valstar, M.; Meng, H.; Kemp, A.; Shafizadeh, M.; et al. The automatic detection of chronic pain-related expression: Requirements, challenges and the multimodal EmoPain dataset. IEEE Trans. Affective Comput. 2015, 7, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Aung, M.H.; Bianchi-Berthouze, N.; Watson, P.; Williams, A.C.D.C. Automatic recognition of fear-avoidance behavior in chronic pain physical rehabilitation. In Proceedings of the 8th International Conference on Pervasive Computing Technologies for Healthcare, Oldenburg, Germany, 20–23 May 2014; pp. 158–161. [Google Scholar] [CrossRef]
- Aung, M.S.; Singh, A.; Lim, S.; Williams, A.C.d.C.; Watson, P.; Bianchi-Berthouze, N. Automatic recognition of protective behaviour in chronic pain rehabilitation. In Proceedings of the Workshop on Ubiquitous Games and Gamification for Promoting Behavior Change and Wellbeing, Trento, Italy, 16 September 2013; ACM: Trento, Italy, 2013; pp. 25–28. [Google Scholar]
- Ghosh, S.; Malgireddy, M.R.; Chaudhary, V.; Dhillon, G. A new approach to automatic disc localization in clinical lumbar MRI: Combining machine learning with heuristics. In Proceedings of the 2012 9th IEEE International Symposium on Biomedical Imaging (ISBI), IEEE, Barcelona, Spain, 2–5 May 2012; pp. 114–117. [Google Scholar] [CrossRef]
- Dickey, J.P.; Pierrynowski, M.R.; Bednar, D.A.; Yang, S.X. Relationship between pain and vertebral motion in chronic low-back pain subjects. Clin. Biomech. 2002, 17, 345–352. [Google Scholar] [CrossRef]
- Jamison, R.N.; Xu, X.; Wan, L.; Edwards, R.R.; Ross, E.L. Determining Pain Catastrophizing From Daily Pain App Assessment Data: Role of Computer-Based Classification. J. Pain 2019, 20, 278–287. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S.; Roeder, K. A SAS procedure based on mixture models for estimating developmental trajectories. Sociol. Methods Res. 2001, 29, 374–393. [Google Scholar] [CrossRef]
- Meier, M.L.; Vrana, A.; Humphreys, B.K.; Seifritz, E.; Stämpfli, P.; Schweinhardt, P. Pain-Related Fear-Dissociable Neural Sources of Different Fear Constructs. eNeuro 2018, 5. [Google Scholar] [CrossRef]
- Rahman, Q.A.; Janmohamed, T.; Pirbaglou, M.; Clarke, H.; Ritvo, P.; Heffernan, J.M.; Katz, J. Defining and Predicting Pain Volatility in Users of the Manage My Pain App: Analysis Using Data Mining and Machine Learning Methods. J. Med. Internet Res. 2018, 20, e12001. [Google Scholar] [CrossRef]
- Rabbi, M.; Aung, M.S.; Gay, G.; Reid, M.C.; Choudhury, T. Feasibility and Acceptability of Mobile Phone-Based Auto-Personalized Physical Activity Recommendations for Chronic Pain Self-Management: Pilot Study on Adults. J. Med. Internet Res. 2018, 20, e10147. [Google Scholar] [CrossRef]
- Huang, Y.; Zheng, H.; Nugent, C.; McCullagh, P.; Black, N.; Vowles, K.E.; McCracken, L. Feature selection and classification in supporting report-based self-management for people with chronic pain. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Vowles, K.E.; McCracken, L.M. Acceptance and values-based action in chronic pain: A study of treatment effectiveness and process. J. Consult. Clin. Psychol. 2008, 76, 397–407. [Google Scholar] [CrossRef]
- Huang, Y.; Zheng, H.; Nugent, C.; McCullagh, P.; Black, N.; Vowles, K.; McCracken, L. Classification of health level from chronic pain self reporting. In Proceedings of the IADIS International Conference e-Health 2009, IADIS, Algarve, Portugal, 21–23 June 2009; pp. 43–50. [Google Scholar]
- Lee, J.; Mawla, I.; Kim, J.; Loggia, M.L.; Ortiz, A.; Jung, C.; Chan, S.T.; Gerber, J.; Schmithorst, V.J.; Edwards, R.R.; et al. Machine learning-based prediction of clinical pain using multimodal neuroimaging and autonomic metrics. Pain 2019, 160, 550–560. [Google Scholar] [CrossRef]
- Jaiswal, S.; Egede, J.; Valstar, M. Deep learned cumulative attribute regression. In Proceedings of the 2018 13th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2018), Xi’an, China, 15–19 May 2018; pp. 715–722. [Google Scholar] [CrossRef]
- Hammal, Z.; Cohn, J.F. Automatic detection of pain intensity. In Proceedings of the 14th ACM International Conference on Multimodal Interaction, ACM, Santa Monica, CA, USA, 22–26 October 2012; pp. 47–52. [Google Scholar] [CrossRef]
- Kaltwang, S.; Rudovic, O.; Pantic, M. Continuous pain intensity estimation from facial expressions. In Proceedings of the International Symposium on Visual Computing, Crete, Greece, 16–18 July 2012; Springer: Berlin/Heidelberg, Germany, 2012; pp. 368–377. [Google Scholar] [CrossRef]
- Lucey, P.; Cohn, J.F.; Prkachin, K.M.; Solomon, P.E.; Matthews, I. Painful data: The UNBC-McMaster shoulder pain expression archive database. In Proceedings of the IEEE International Conference on Automatic Face and Gesture Recognition and Workshops (FG 2011), IEEE, Santa Barbara, CA, USA, 21–25 March 2011; pp. 57–64. [Google Scholar] [CrossRef]
- Fillingim, R.B.; Loeser, J.D.; Baron, R.; Edwards, R.R. Assessment of Chronic Pain: Domains, Methods, and Mechanisms. J. Pain Off. J. Am. Pain Soc. 2016, 17, T10–T20. [Google Scholar] [CrossRef] [PubMed]
- Wallace, P.J.; Shah, N.D.; Dennen, T.; Bleicher, P.A.; Bleicher, P.D.; Crown, W.H. Optum Labs: Building a novel node in the learning health care system. Health Aff. 2014, 33, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Rev. Saúde Pública 2015, 49, 73. [Google Scholar] [CrossRef]
- Koes, B.W.; van Tulder, M.W.; Thomas, S. Diagnosis and treatment of low back pain. BMJ 2006, 332, 1430–1434. [Google Scholar] [CrossRef]
- Cimmino, M.A.; Ferrone, C.; Cutolo, M. Epidemiology of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2011, 25, 173–183. [Google Scholar] [CrossRef]
- Hunter, T.M.; Boytsov, N.N.; Zhang, X.; Schroeder, K.; Michaud, K.; Araujo, A.B. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol. Int. 2017, 37, 1551–1557. [Google Scholar] [CrossRef]
- Pribicevic, M. The epidemiology of shoulder pain: A narrative review of the literature. In Pain in Perspective; Ghosh, S., Ed.; InTechOpen: London, UK, 2012; pp. 147–186. [Google Scholar] [CrossRef]
- De Toledo, I.P.; Réus, J.C.; Fernandes, M.; Porporatti, A.L.; Peres, M.A.; Takaschima, A.; Linhares, M.N.; Guerra, E.; Canto, G.D.L. Prevalence of trigeminal neuralgia. J. Am. Dent. Assoc. 2016, 147. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.P.; Freburger, J.; Carey, T. Prevalence, practice patterns, and evidence for chronic neck pain. Arthritis Care Res. 2010, 62, 1594–1601. [Google Scholar] [CrossRef]
- Gerwin, R. Myofascial Pain Syndrome. In Pain Medicine: An Interdisciplinary Case-Based Approach; Hayek, S.M., Shah, B.J., Desai, M.J., Chelimsky, T.C., Eds.; Oxford University Press: New York, NY, USA, 2015; pp. 69–88. ISBN 978-0-19-939082-3. Available online: https://oxfordmedicine.com/view/10.1093/med/9780199931484.001.0001/med-9780199931484 (accessed on 2 April 2021). [CrossRef]
- Clauw, D.J.; Arnold, L.M.; McCarberg, B.H. The science of fibromyalgia. Mayo Clin. Proc. 2011, 86, 907–911. [Google Scholar] [CrossRef]
- Wolfe, F.; Brähler, E.; Hinz, A.; Häuser, W. Fibromyalgia Prevalence, Somatic Symptom Reporting, and the Dimensionality of Polysymptomatic Distress: Results From a Survey of the General Population. Arthritis Care Res. 2013, 65, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Neumann, L.; Buskila, D. Epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2003, 7, 362–368. [Google Scholar] [CrossRef]
- Zhu, W.; He, X.; Cheng, K.; Zhang, L.; Chen, D.; Wang, X.; Qiu, G.; Cao, X.; Weng, X. Ankylosing spondylitis: Etiology, pathogenesis, and treatments. Bone Res. 2019, 7, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Goh, E.L.; Chidambaram, S.; Ma, D. Complex regional pain syndrome: A recent update. Burns Trauma 2017, 5. [Google Scholar] [CrossRef]
- Lamichhane, B.; Jayasekera, D.; Jakes, R.; Glasser, M.F.; Zhang, J.; Yang, C.; Grimes, D.; Frank, T.L.; Ray, W.Z.; Leuthardt, E.C.; et al. Multi-modal biomarkers of low back pain: A machine learning approach. NeuroImage Clin. 2021, 29, 102530. [Google Scholar] [CrossRef]
- Santana, A.N.; de Santana, C.N.; Montoya, P. Chronic Pain Diagnosis Using Machine Learning, Questionnaires, and QST: A Sensitivity Experiment. Diagnostics 2020, 10, 958. [Google Scholar] [CrossRef]
- Santana, A.N.; Cifre, I.; De Santana, C.N.; Montoya, P. Using Deep Learning and Resting-State fMRI to Classify Chronic Pain Conditions. Front. Neurosci. 2019, 13, 1313. [Google Scholar] [CrossRef]
- Goldberg, D.S.; McGee, S.J. Pain as a global public health priority. BMC Public Health 2011, 11, 770. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Year | Condition | Data Size | Data Sources | ML Methods |
|---|---|---|---|---|---|
| Classifying patients using structured health data | |||||
| Melidis [26] | 2018 | IBS, FM, CFS | 1751 | Symptom frequency questionnaire | Adaptive network model, k-means clustering, NN |
| Davis et al. [27] | 2018 | FM | 2529 | De-identified clinic-level data | K-means clustering, principal component analysis, discriminant analysis |
| Lin et al. [28] | 2018 | MPS | 56 | SEMG | Template matching, k-means clustering |
| Oliviero and Poli-Neto [29] | 2017 | CPP | 346 | A database of diagnosed cases containing the full history of the patient. Seven different conditions related to pelvic pain were included in the data. | Naive Bayes, C4.5, SVM, AdaBoost, kNN, Weka software [30] |
| Yim et al. [31] | 2017 | FM | 313 | Demographic characteristics | Clustering |
| Emir et al. [32] | 2015 | FM | 587,960 | Structured EHR data (Humedica database) | RF |
| Garcia-Zapirain et al. [33] | 2015 | FM | 127 | Psychopathological and medical-social features, VAS | AdaBoost |
| Olugbade et al. [34] | 2014 | CLBP | 31 | Movements, muscle activity characteristics, SEMG (EmoPaindataset) | One-way ANOVA, SVM |
| Chan [35] | 2013 | CLBP | 40 | Gait data | kStar, SVM, MLP, DT |
| Yang et al. [36] | 2012 | CRPS | 20 | Gait data | MLP, SVM, RF, LDA, KStar |
| Goertzel et al. [37] | 2006 | CFS | 103 | Clinical data | Nonlinear regression |
| Classifying patients using text and images | |||||
| Fodeh [38] | 2018 | Musculoskeletal pain | 92 | Clinical notes from EHR | kNN, DT, SVM, RF |
| Tan [39] | 2018 | CLBP | 871 | Lumbar spine imaging, radiology reports | Natural language processing |
| Zhong [40] | 2018 | TN | 46 | sMRI | SVM |
| Cheng [41] | 2018 | AS | 133 | Questionnaire, fMRI | Multiple linear regression |
| Rogachov et al. [42] | 2018 | AS | 133 | fMRI | PRoNTo [43] |
| Mano [44] | 2018 | CLBP | 97 | fMRI (+test data from OpenPain project) | SVM, conditional variational autoencoder |
| Sevel [45] | 2018 | CFS | 33 | sMRI and PROM | SVM |
| Lopez-Sola [46] | 2017 | FM | 72 | fMRI | SVM |
| Qin et al. [47] | 2016 | CLBP | 22 | Body movement and EMG (EmoPain dataset) | RF, kNN, hidden Markov model |
| Olugbade et al. [48] | 2015 | CLBP | 53 | Motion capture, EMG, video, audio, and Hospital Anxiety and Depression Scale (EmoPain dataset) | SVM, RF |
| Labus [49] | 2015 | IBS | 212 | sMRI | MVPA |
| Robinson et al. [50] | 2015 | FM | 26 | sMRI, PROM (mood and pain intensity) | Naive Bayes, logistic regression, kNN, MLP, SVM, DT |
| Sundermann [51] | 2014 | FM, RA | 50 | fMRI, VAS | MVPA, SVM, DT, RF, naive Bayes, LDA, MLP |
| Callan et al. [52] | 2014 | CLBP | 26 | fMRI | Sparse logistic regression |
| Bagarinao [53] | 2014 | CPP | 66 | sMRI | SVM |
| Ung [54] | 2012 | CLBP | 94 | sMRI | SVM |
| Genomics approaches and biomarker identification | |||||
| Lukkahatai et al. [55] | 2018 | FM | 47 | Gene expression data | Fisher’s ratio |
| Chancellor et al. [56] | 2018 | IC | 448 | Urine samples, questionnaires | Supervised learning |
| Ultsch et al. [57] | 2016 | Chronic pain | 535 genes | Pain genes | ctional genomics analysis |
| Braundmeier-Fleming et al. [58] | 2016 | IC | 34 | DNA from stool and vaginal samples | extended random forest |
| Treatment | |||||
| Golabchi [59] | 2019 | CLBP | 62 | SEMG, VAS | RF, linear regression |
| Sabeti [60] | 2019 | FM | 20 | PROM and patient-generated data (wristband sensors) | kNN, AdaBoost, SVM, RF, LDA, LUCCK |
| Nijeweme-d’Hollosy [61] | 2018 | CLBP | 1326 | Age, well-being, pain description | DT, RF, and boosted tree |
| McKernan [62] | 2018 | FM | 15,945 | EHR | Penalized regression |
| Jiang [63] | 2017 | CLBP | 78 | SEMG | SVM |
| Aung et al. [64] | 2015 | CLBP | 22 | The EmoPain dataset (anthropometric measurements, facial expressions, movement behaviours) | SVM, RF |
| Aung et al. [65] | 2014 | CLBP | 21 | Sit-to-stand and one-leg stand | RF |
| Aung et al. [66] | 2013 | CLBP | 21 | The EmoPain dataset | RF |
| Zhang [25] | 2013 | Chronic neck pain | 794 | Patients records | DT, non-dominated sort |
| Ghosh [67] | 2012 | CLBP | 53 | MRI | SVM |
| Dickey [68] | 2002 | CLBP | 9 | 3D vertebral motion | LDA and NN |
| Self-management | |||||
| Jamison et al. [69] | 2019 | Chronic pain | 144 | Pain Catastrophizing Scale, Pain Disability Index, Hospital Anxiety and Depression Scale, VAS | Multilevel AR (1) modelling, SAS procedure [70], -test, logistic regression |
| Meier [71] | 2018 | CLBP | 20 | MRI, PROM (pain-related fear) | MVPA, PRoNTo [43] |
| Rahman [72] | 2018 | Chronic pain | 28,952 | Patient-generated data (mobile app: pain data) | Logistic regression, RF, SVM, k-means clustering |
| Rabbi et al. [73] | 2018 | CLBP | 10 | Patient-generated data (mobile app: sensor-based and self-reported physical activity, and self-reported pain | RL |
| Huang et al. [74] | 2011 | Chronic pain | 187 [75] | PROM | SVM |
| Huang [76] | 2009 | Chronic pain | 187 [75] | PROM | DT, naive Bayes, SVM, MLP |
| Measuring pain intensity | |||||
| Lee et al. [77] | 2019 | CLBP | 71 | Exacerbation manoeuvres, fMRI | SVM, SVR |
| Jaiswal et al. [78] | 2018 | Shoulder pain | 25 | Facial expression videos | CNN |
| Hammal and Cohn [79] | 2012 | Shoulder pain | 129 | Facial expression videos, PROM | SVM, active appearance model |
| Kaltwang et al. [80] | 2012 | Shoulder pain | 25 | Facial expression videos | Relevance vector regression, active appearance model |
| Lucey [81] | 2011 | Shoulder pain | 129 | Facial expression videos | SVM |
| Title | Participants | Data Types |
|---|---|---|
| UNBC-McMaster Shoulder Pain Expression Archive Database [81] | 129 patients with shoulder pain (66 female and 63 male) | Video of facial expressions while performing range-of-motion tests. Frames are coded with self-reported and observer-reported ratings of pain. |
| EmoPain dataset [64] | 22 patients with CLBP (15 female, 7 male) and 28 healthy controls | A fully labelled multimodal dataset containing face videos, 3D motion capture, and EMG signals from back muscles. Pain-related facial expressions and body movement behaviours were elicited from people with chronic pain performing physical exercises. |
| OpenPain dataset [44] | fMRI data of patients with CLBP | |
| Optum Humedica database [83] | >150 million people | De-identified EHR data and claims data, including diagnoses, treatments, pharmacy and over-the-counter prescriptions, text notes, etc. |
| Condition | Prevalence | Diagnosis | Clinical Decision Support | Rehabilitation | Self-Management |
|---|---|---|---|---|---|
| Myofascial Pain Syndrome (MPS) | 9%–20% | [28] | |||
| Chronic Musculoskeletal Pain | 11.4%–24% | [38] | |||
| Chronic Pelvic Pain (CPP) | 4%–24% | [29,53] | |||
| Chronic Low Back Pain (CLBP) | 5%–20% | [39,44,52,54,77] | [59,61,67,68] | [34,35,48,63,64,65,66] | [47,71,73] |
| Chronic Shoulder Pain | 15.1% | [78,79,80,81] | |||
| Irritable Bowel Syndrome (IBS) | 11% | [26,49] | |||
| Interstitial Cystitis/Bladder Pain Syndrome (IC) | 2.7%–6.53% | [56,58] | |||
| Fibromyalgia (FM) | 2%–5% | [26,27,31,32,33,46,50,51,55] | [27,60,62] | ||
| Chronic Fatigue Syndrome (CFS) | 0.76%–3.28 % | [26,37,45] | |||
| Chronic Neck Pain | 2.2% | [25] | |||
| Rheumatoid Arthritis (RA) | 0.41%–0.54% | [51] | |||
| Ankylosing Spondylitis (AS) | 0.07%–0.32% | [41,42] | |||
| Trigeminal Neuralgia (TN) | 0.03%–0.3% | [40] | |||
| Complex Regional Pain Syndrome (CRPS) | 0.025% | [36] | |||
| Unspecified Chronic Pain | [57] | [69,72,74,76] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jenssen, M.D.K.; Bakkevoll, P.A.; Ngo, P.D.; Budrionis, A.; Fagerlund, A.J.; Tayefi, M.; Bellika, J.G.; Godtliebsen, F. Machine Learning in Chronic Pain Research: A Scoping Review. Appl. Sci. 2021, 11, 3205. https://doi.org/10.3390/app11073205
Jenssen MDK, Bakkevoll PA, Ngo PD, Budrionis A, Fagerlund AJ, Tayefi M, Bellika JG, Godtliebsen F. Machine Learning in Chronic Pain Research: A Scoping Review. Applied Sciences. 2021; 11(7):3205. https://doi.org/10.3390/app11073205
Chicago/Turabian StyleJenssen, Marit Dagny Kristine, Per Atle Bakkevoll, Phuong Dinh Ngo, Andrius Budrionis, Asbjørn Johansen Fagerlund, Maryam Tayefi, Johan Gustav Bellika, and Fred Godtliebsen. 2021. "Machine Learning in Chronic Pain Research: A Scoping Review" Applied Sciences 11, no. 7: 3205. https://doi.org/10.3390/app11073205
APA StyleJenssen, M. D. K., Bakkevoll, P. A., Ngo, P. D., Budrionis, A., Fagerlund, A. J., Tayefi, M., Bellika, J. G., & Godtliebsen, F. (2021). Machine Learning in Chronic Pain Research: A Scoping Review. Applied Sciences, 11(7), 3205. https://doi.org/10.3390/app11073205