
Heart Diseases Diagnose via Mobile Application


Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Set
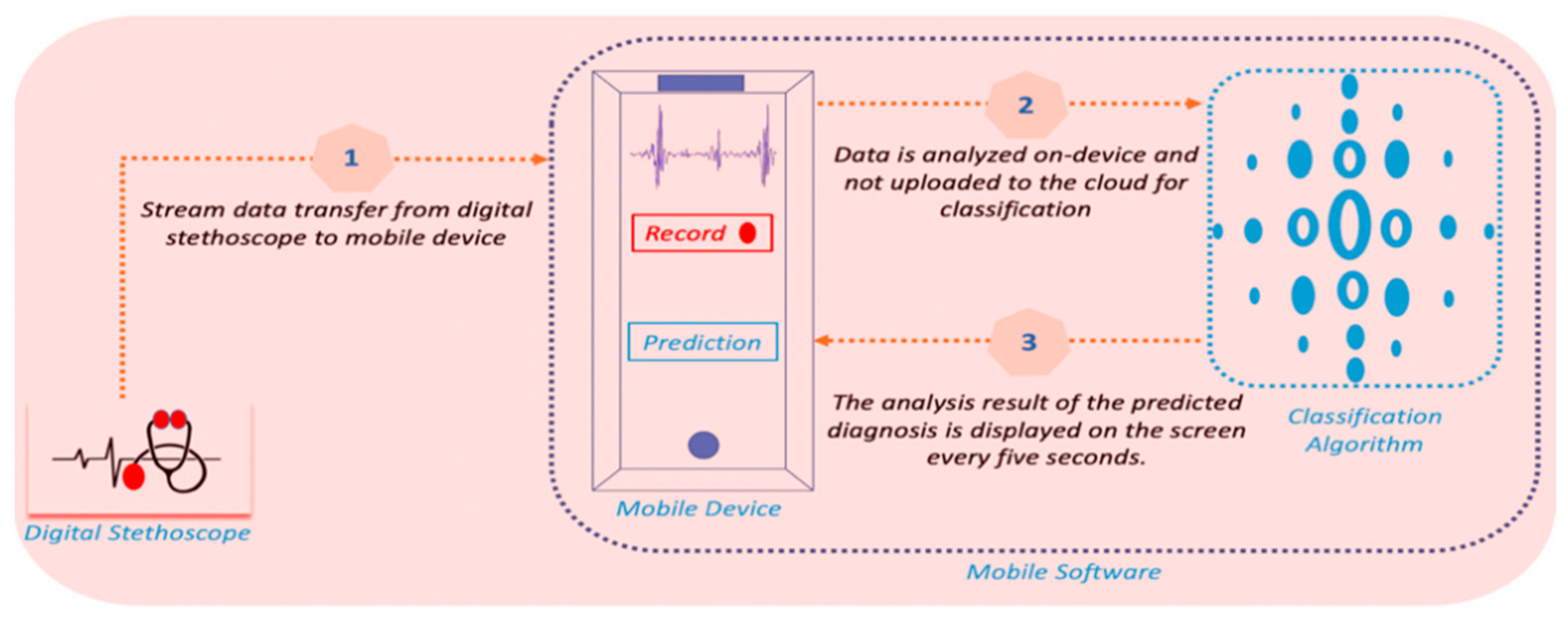
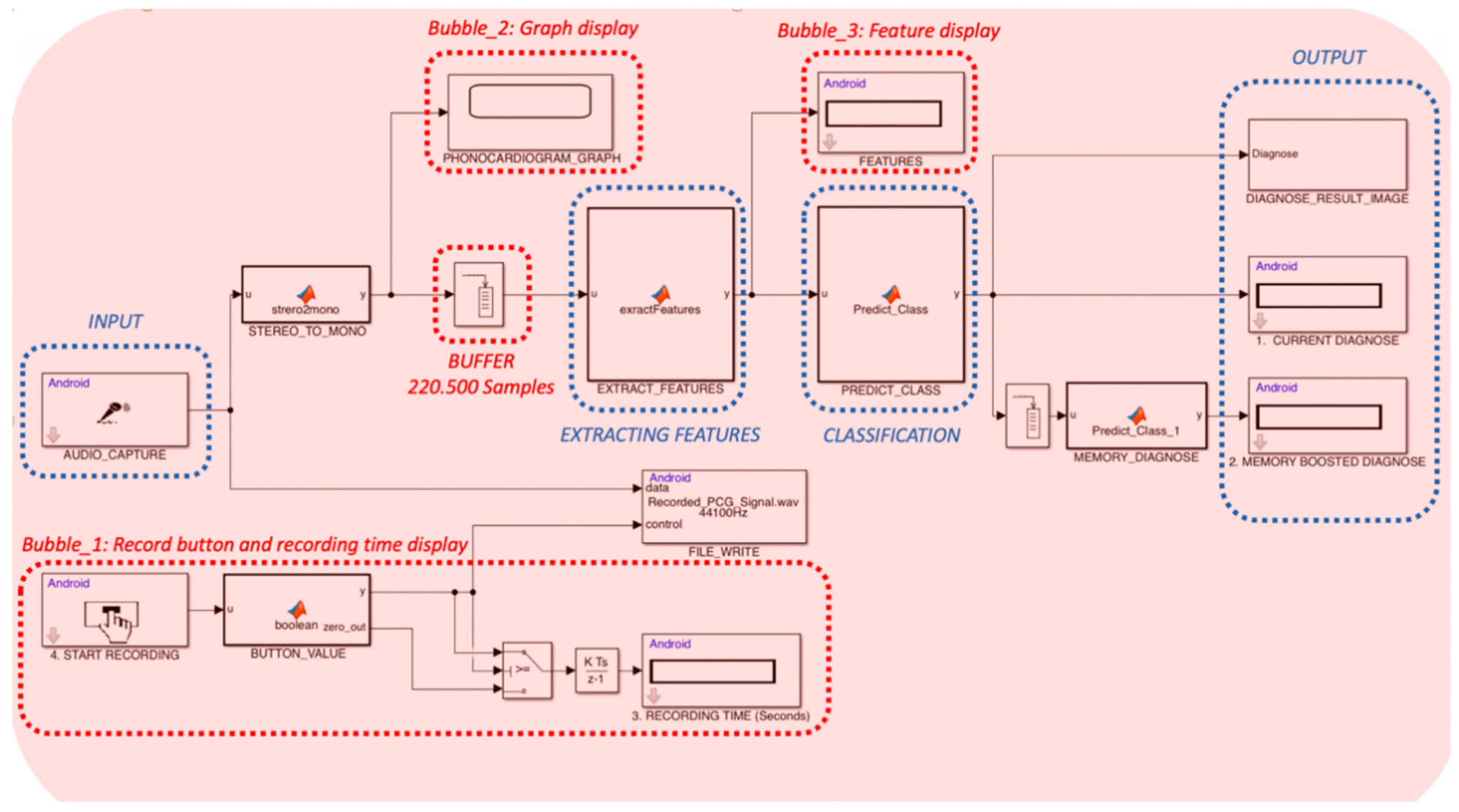
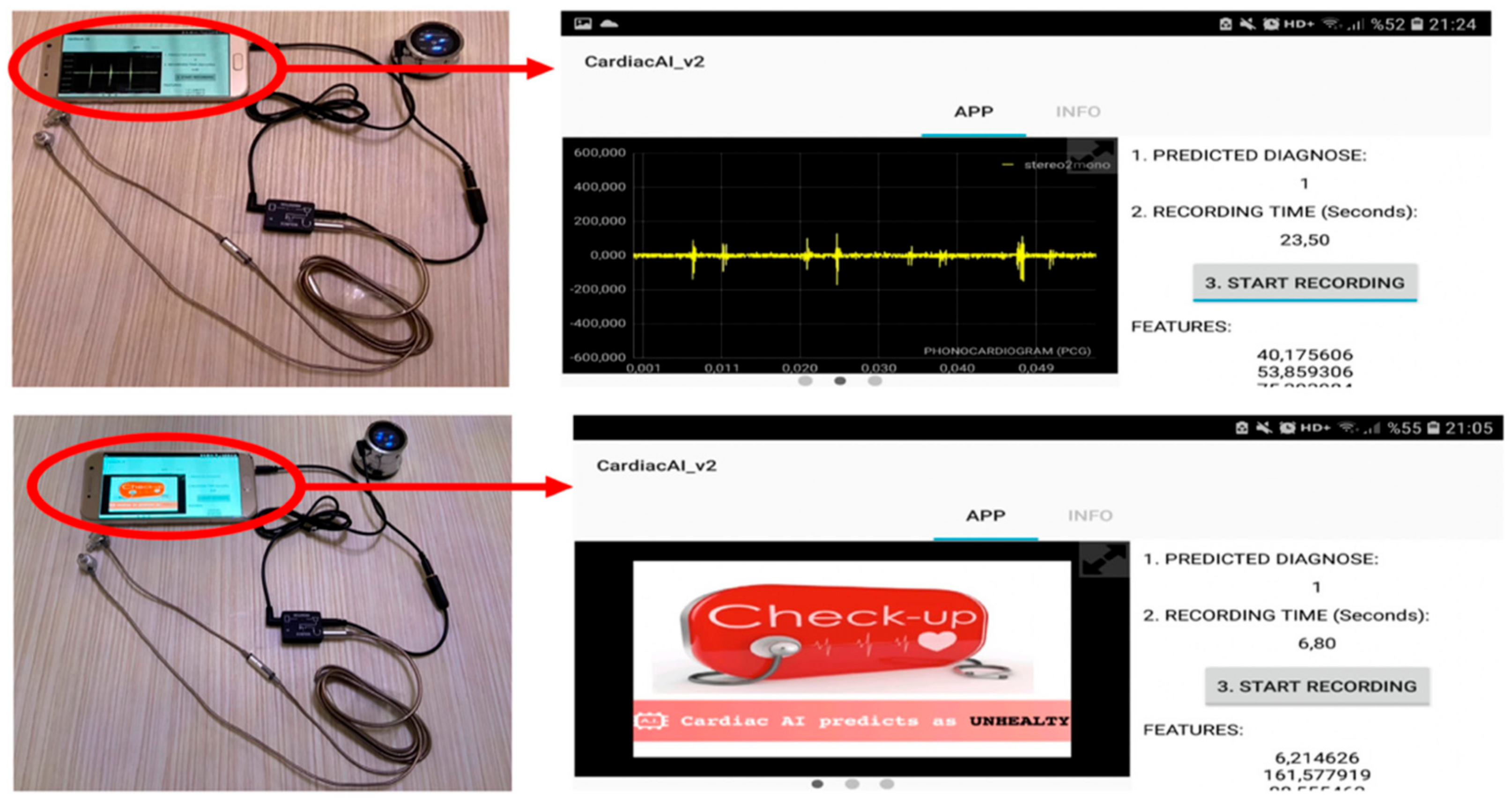
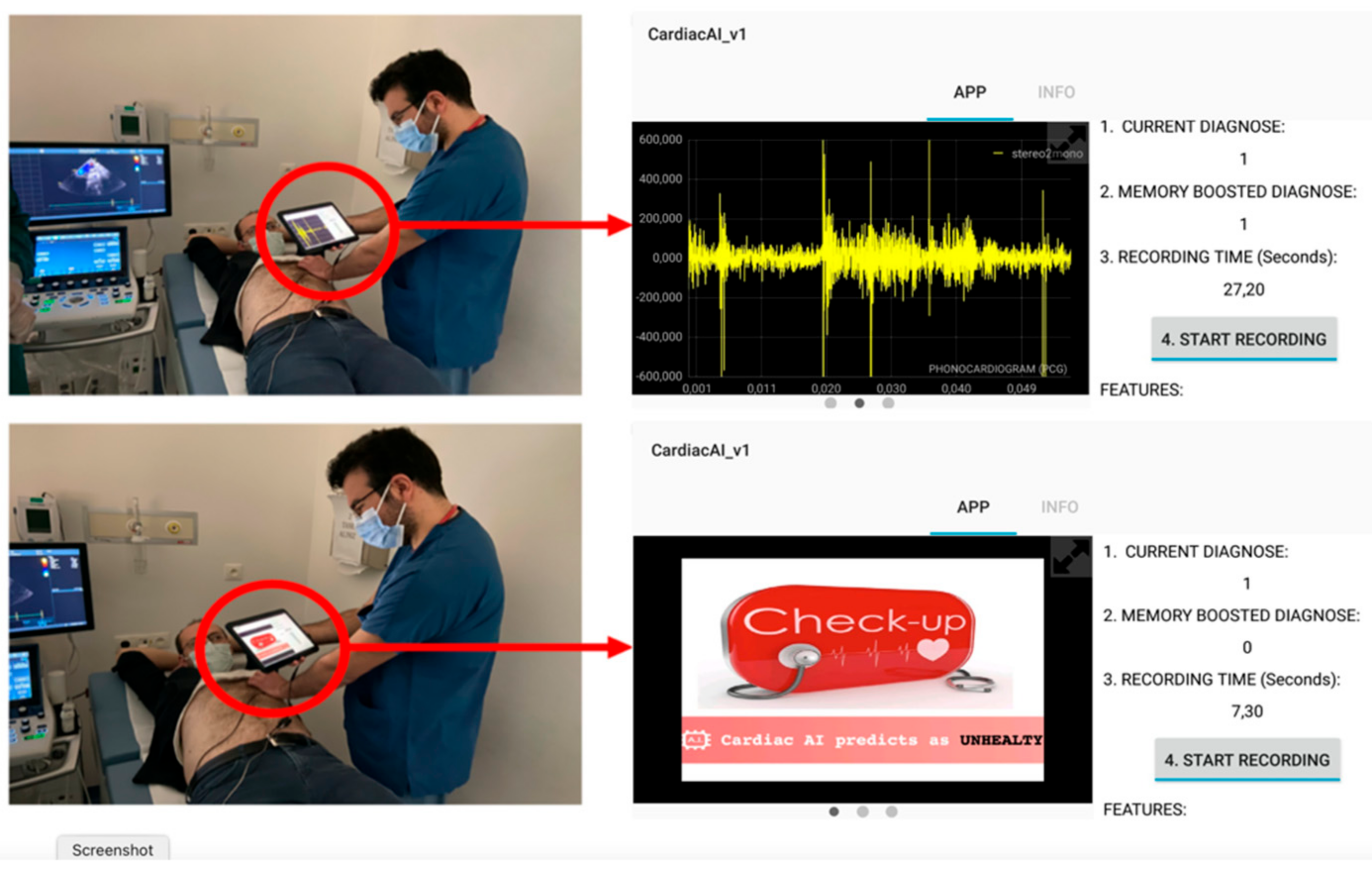
2.2. Software Description
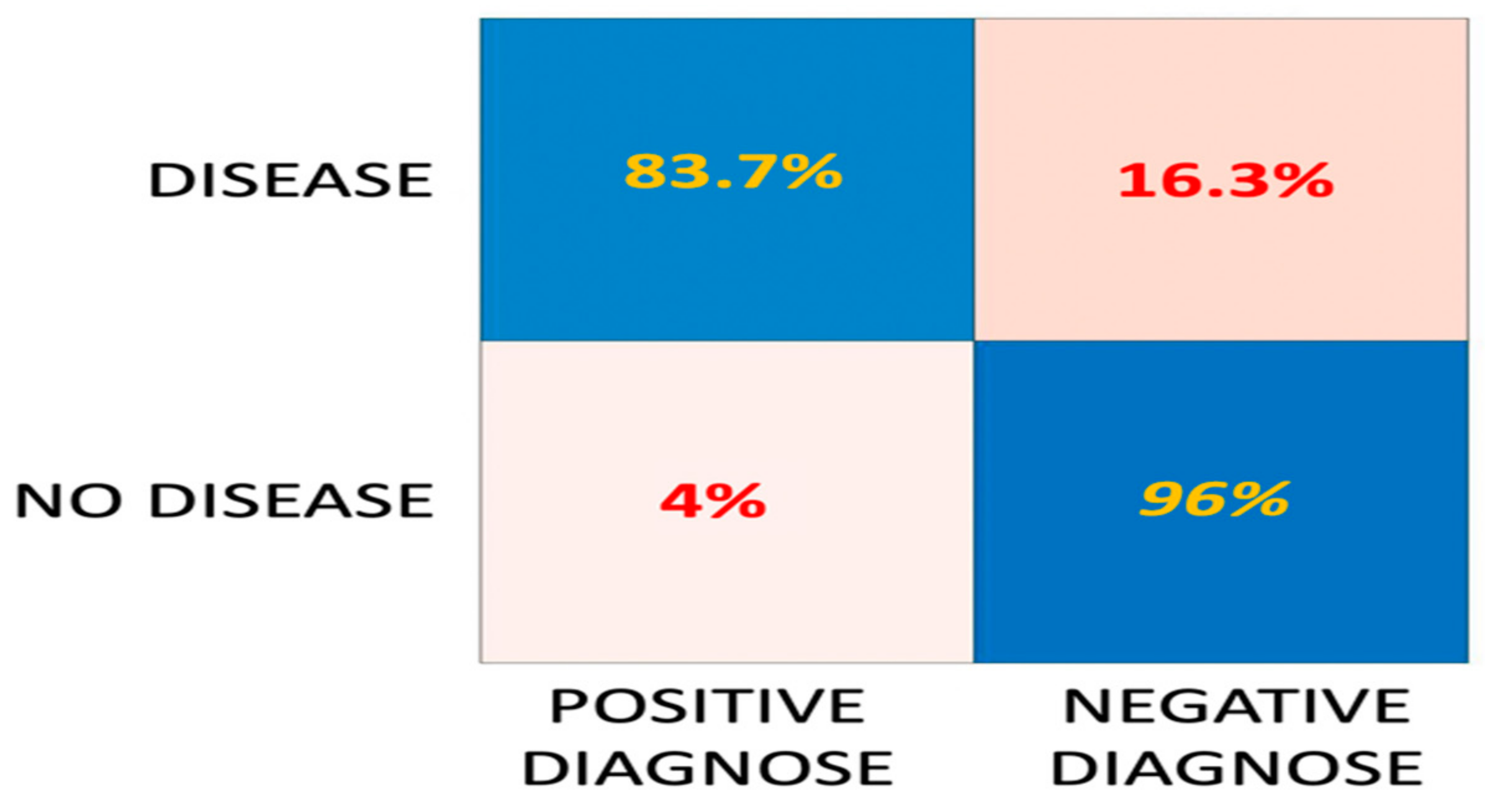
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Logistic Regression Classifiers | 80.3% | 42.7% | 92.4% |
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Gaussian Naïve Bayes Classifiers | 80.8% | 64% | 86.2% |
| Kernel Naïve Bayes Classifiers | 80.7% | 72.2% | 83.5% |
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Linear Discriminant | 80.7% | 44.6% | 92.2% |
| Quadratic Discriminant | 82.1% | 48.8% | 92.8% |
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Fine Tree | 86.6% | 68.3% | 92.4% |
| Medium Tree | 84.9% | 64.4% | 91.4% |
| Coarse Tree | 81.5% | 37.4% | 95.6% |
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Linear SVM | 80.7% | 43% | 92.7% |
| Quadratic SVM | 87.7% | 69.9% | 93.4% |
| Cubic SVM | 89.7% | 78% | 93.5% |
| Fine Gaussian SVM | 85.4% | 43.2% | 98.9% |
| Medium Gaussian SVM | 89.5% | 73.7% | 94.6% |
| Coarse Gaussian SVM | 85.6% | 58.6% | 94.2% |
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Fine KNN | 92.8% | 85.9% | 95% |
| Medium KNN | 90.9% | 82.7% | 93.5% |
| Coarse KNN | 87.1% | 64.5% | 94.3% |
| Cosine KNN | 89.2% | 75.7% | 93.5% |
| Cubic KNN | 90.4% | 81.8% | 93.1% |
| Weighted KNN | 92.1% | 83% | 95% |
| Algorithms | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Boosted Trees | 87.7% | 68.7% | 93.8% |
| Bagged Trees | 90.9% | 79.5% | 94.5% |
| Subspace Discriminant | 76.3% | 18.1% | 94.9% |
| Subspace k-nearest neighbor | 93% | 84.6% | 95.6% |
| RUSBoosted Trees | 83.6% | 89.4% | 81.7% |
References
- WHO. Statistics On Cardiovascular Disease. Available online: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(CVDs) (accessed on 10 January 2021).
- Castillo, M.; Conte, B.; Hinkes, S.; Mathew, M.; Na, C.J.; Norindr, A.; Serota, D.P.; Forrest, D.W.; Deshpande, A.R.; Bartholomew, T.S.; et al. Implementation of a medical student-run telemedicine program for medications for opioid use disorder during the COVID-19 pandemic. Harm Reduct. J. 2020, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, F. Role of Telemedicine and Telegenetics Framework for the Management of Cancer Patients During the COVID-19 Pandemic. Biointerface Res. Appl. Chem. 2021, 11, 8773–8779. [Google Scholar] [CrossRef]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.F.; de Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.; Vinhoza, T.T.V.; Mattos, S.S.; Coimbra, M.T. Heart Sound Segmentation of Pediatric Auscultations Using Wavelet Analysis. In Proceedings of the 2013 35th Annual International Conference of the Ieee Engineering in Medicine and Biology Society, Osaka, Japan, 3–7 July 2013; pp. 3909–3912. [Google Scholar]
- Liu, C.Y.; Springer, D.; Li, Q.; Moody, B.; Juan, R.A.; Chorro, F.J.; Castells, F.; Roig, J.M.; Silva, I.; Johnson, A.E.W.; et al. An open access database for the evaluation of heart sound algorithms. Physiol. Meas. 2016, 37, 2181–2213. [Google Scholar] [CrossRef] [PubMed]
- Leatham, A. Auscultation of the Heart and Phonocardiography; Churchill Livingstone: London, UK, 1970. [Google Scholar]
- Gharehbaghi, A.; Ekman, I.; Ask, P.; Nylander, E.; Janerot-Sjoberg, B. Assessment of aortic valve stenosis severity using intelligent phonocardiography. Int. J. Cardiol. 2015, 198, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Maglogiannis, I.; Loukis, E.; Zafiropoulos, E.; Stasis, A. Support vectors machine-based identification of heart valve diseases using heart sounds. Comput. Methods Programs Biomed. 2009, 95, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Lim, C.S.; Chauhan, S.; Foo, J.Y.A.; Anantharaman, V. Phonocardiographic signal analysis method using a modified hidden Markov model. Ann. Biomed. Eng. 2007, 35, 367–374. [Google Scholar] [CrossRef] [PubMed]
- KardiaMobile, ECG Based Analyze. Available online: https://www.alivecor.com/kardiamobile (accessed on 10 January 2021).
- Stethee, AI Boosted Digital Stethescopes. Available online: https://www.stethee.com/ (accessed on 10 January 2021).
- Eko Devices, Eko Core Digital Stethoscope. Available online: https://ekodevices.com/ (accessed on 10 January 2021).
- Sensicardiac, a Way to Provide Quantitative Heart Screenings. Available online: https://sensicardiac.com/ (accessed on 10 January 2021).
- Kleyko, D.; Osipov, E.; Wiklund, U. A Comprehensive Study of Complexity and Performance of Automatic Detection of Atrial Fibrillation: Classification of Long ECG Recordings Based on the PhysioNet Computing in Cardiology Challenge 2017. Biomed. Phys. Eng. Express 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Kucharski, D.; Grochala, D.; Kajor, M.; Kańtoch, E. A Deep Learning Approach for Valve Defect Recognition in Heart Acoustic Signal; Springer: Cham, Switzerland, 2017; pp. 3–14. [Google Scholar]
- Chen, Y.; Wei, S.; Zhang, Y. Classification of heart sounds based on the combination of the modified frequency wavelet transform and convolutional neural network. Med. Biol. Eng. Comput. 2020, 58, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Ma, K.; Liu, M. Temporal Convolutional Network Connected with an Anti-Arrhythmia Hidden Semi-Markov Model for Heart Sound Segmentation. Appl. Sci. 2020, 10, 22. [Google Scholar] [CrossRef]
- Android Support from Simulink. Available online: https://www.mathworks.com/hardware-support/android-programming-simulink.html (accessed on 10 January 2021).
- Introduction to Simulink Hardware Support for Android and iOS Mobile Devices. Available online: https://www.mathworks.com/videos/introduction-to-simulink-hardware-support-for-android-and-ios-mobile-devices-1487797862580.html (accessed on 10 January 2021).
- Getting Started with Android Devices. Available online: https://www.mathworks.com/help/supportpkg/android/ref/getting-started-with-android-devices.html (accessed on 10 January 2021).
- Getting Started with iOS Devices. Available online: https://www.mathworks.com/help/supportpkg/appleios/ug/getting-started-with-apple-ios-devices.html (accessed on 10 January 2021).
- Generate C/C++ Code for the Object Functions. Available online: https://www.mathworks.com/help/stats/savelearnerforcoder.html (accessed on 10 January 2021).
- Davis, S.; Mermelstein, P. Comparison of parametric representations for monosyllabic word recognition in continuously spoken sentences. IEEE Trans. Acoust. Speech Signal Process. 1980, 28, 357–366. [Google Scholar] [CrossRef]
- Zewoudie, A.W.; Luque, J.; Hernando, J. The use of long-term features for GMM- and i-vector-based speaker diarization systems. EURASIP J. Audio Speech Music Process. 2018, 2018, 14. [Google Scholar] [CrossRef]
- Haney, I.; Ipp, M.; Feldman, W.; McCrindle, B.W. Accuracy of clinical assessment of heart murmurs by office based (general practice) paediatricians. Arch. Dis. Child. 1999, 81, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Gardezi, S.K.M.; Myerson, S.G.; Prendergast, B.; Prothero, A.; Prendergast, A.; Loudon, M.; D’Arcy, J.; Ox, V.P.C.S. Cardiac auscultation in diagnosing valvular heart disease: A comparison between general practitioners and cardiologists. Eur. Heart J. 2017, 38, 1155. [Google Scholar]
- Rushmer, R.F.; Sparkman, D.R.; Polley, R.F.; Bryan, E.E.; Bruce, R.R.; Welch, G.B.; Bridges, W.C. Variability in detection and interpretation of heart murmurs; a comparison of auscultation and stethography. AMA Am. J. Dis. Child. 1952, 83, 740–754. [Google Scholar] [CrossRef] [PubMed]
- Leach, R.M.; McBrien, D.J. Brachioradial delay—A new clinical indicator of the severity of aortic-stenosis. Lancet 1990, 335, 1199–1201. [Google Scholar] [CrossRef]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Mant, J.; Fitzmaurice, D.A.; Hobbs, F.D.R.; Jowett, S.; Murray, E.T.; Holder, R.; Davies, M.; Lip, G.Y.H. Accuracy of diagnosing atrial fibrillation on electrocardiogram by primary care practitioners and interpretative diagnostic software: Analysis of data from screening for atrial fibrillation in the elderly (SAFE) trial. BMJ Br. Med. J. 2007, 335, 380B–382B. [Google Scholar] [CrossRef]
- Eko Devices White Paper. Available online: https://ekodevices.com/ (accessed on 10 January 2021).






| Index | Algorithms | ||||||
|---|---|---|---|---|---|---|---|
| LR | NB | DA | DT | SVM | KNN | Ensemble | |
| 1 | Logistic | Gaussian | Linear | Fine | Linear | Fine | Boosted Tree |
| 2 | Kernel | Quadratic | Medium | Quadratic | Medium | Bagged Tree | |
| 3 | Coarse | Cubic | Coarse | Subspace DC | |||
| 4 | Fine | Cosine | Subspace KNN | ||||
| 5 | Medium | Cubic | RUSBoosted Tree | ||||
| 6 | Coarse | Weighted | |||||
| Label | Auscultation Result | Confirmation Results | Length (Seconds) | Age (Years) | Recording Position | Sensor |
|---|---|---|---|---|---|---|
| Normal | 88 | - | 25–45 | 15–70 | Four Typical Position | ThinkLabs 44,100 Hz |
| Abnormal | 74 | 74 | 25–45 | 15–70 | Four Typical Position | ThinkLabs 44,100 Hz |
| Performance Metric | Against Validation Data | Against Verification Data | Trained Cardiologists | General Practitioners |
|---|---|---|---|---|
| Specificity | 96.0% | 92.0% | 98.2% | 81.0% |
| Sensitivity | 83.7% | 81.0% | 69.6% | 31.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Güven, M.; Hardalaç, F.; Özışık, K.; Tuna, F. Heart Diseases Diagnose via Mobile Application. Appl. Sci. 2021, 11, 2430. https://doi.org/10.3390/app11052430
Güven M, Hardalaç F, Özışık K, Tuna F. Heart Diseases Diagnose via Mobile Application. Applied Sciences. 2021; 11(5):2430. https://doi.org/10.3390/app11052430
Chicago/Turabian StyleGüven, Mesut, Fırat Hardalaç, Kanat Özışık, and Funda Tuna. 2021. "Heart Diseases Diagnose via Mobile Application" Applied Sciences 11, no. 5: 2430. https://doi.org/10.3390/app11052430
APA StyleGüven, M., Hardalaç, F., Özışık, K., & Tuna, F. (2021). Heart Diseases Diagnose via Mobile Application. Applied Sciences, 11(5), 2430. https://doi.org/10.3390/app11052430