Abstract
The purpose of this report is to evaluate the applicability of a novel Print and Try technique in the presence of aberrant endodontic anatomies and to achieve a predictable treatment with improved outcome. According to guidelines, cone beam computed tomography (CBCT) is recommended in the presence of complex anatomies. The volumes were utilized to produce a stereo lithographic (STL) file, from which a 3D-plastic tooth model including a hollow root canal system was obtained. The 3D-patient-specific model facilitates the treatment planning and the trial of therapeutic approaches. Using a transparent material, all the treatment steps could be directly visualized. Subsequently, endodontic therapy could be performed in vivo with reduced operating time and with a better overview. Clinicians benefit from the Print and Try technique when facing a complicated root canal system with reduced stress and higher chances of success. In aberrant endodontic anatomies, the use of a transparent 3D plastic model, derived from the CBCT dicom, provides an exact preview of clinical challenges that will be met intra-operatively. A patient centered tailored approach to shaping, cleaning, and filling strategies can be applied.
1. Introduction
The main steps of root canal treatment are the shaping, cleaning, and filling of the root canal system. Shaping, including mechanical debridement, allows the creation of the space for medicament delivery and optimized canal geometries for adequate obturation [1,2,3]. Irrigation reduces friction between instruments and dentine, improves cutting effectiveness of the files, dissolves tissue, cools files and teeth, and, above all, it provides an antimicrobial/antibiofilm effect [3,4,5]. Obturation allows the sealing of all portals of exit in order to prevent leakage that may lead to a recurrent bacterial colonization [6].
The knowledge of the canal morphology and its frequent variations is a basic requirement to correctly perform the three steps above and to reach endodontic success. Missed canals, short obturation and iatrogenic errors are among the major factors leading to unsuccessful outcome [7,8,9]. Furthermore, the inability to effectively shape and clean complex anatomies leads to many efforts to systematically describe the diversity of canal configurations [10,11,12,13]. The use of operative microscopy, cone beam computed tomography (CBCT) and microcomputed tomography have increased the number of reports on complex root canal anatomies previously ignored. Variations in root canal system configuration have also been analyzed between genders and in patients belonging to distinct age groups and ethnicities [14,15,16,17,18,19,20,21,22].
The difficulties in interpreting three-dimensional anatomy with conventional intra-oral radiography have been overcome with the use of CBCT. Indeed, the appreciation of complex root canal systems (e.g., dens invaginatus) is a suggested criterion for CBCT and related software use in Endodontics [23,24,25,26,27]. CBCT imaging is often utilized clinically by manually exploring the three axial planes (axial/frontal/sagittal), although the use of a 3D reconstruction has been demonstrated to improve the diagnosis and understanding of the clinical case and to reduce the stress of the operator before the clinical procedure [28]. Moreover, CBCT with reduced field of view (FOV) and a reasonable exposure dosage limits scattering phenomena and increases resolution, maintaining the principle as low as reasonably achievable (ALARA) [23]. However, despite knowing the anatomy, determining the appropriate cleaning and shaping instrument sequence may represent a challenge.
Recently, 3D-printing starting from CBCT data has been introduced, for both soft and hard tissues [29]. When single extracted human teeth are digitalized by a CBCT and reproduced by a stereolithographic printer, replicas with values of precision ranging from 43.5 to 68.2 μm, very comparable (60%) or rather comparable (34%) to real teeth were obtained [30]. Furthermore, patient-specific complete tooth analogues—with their endodontic system—could be produced directly from the CBCT scan, eventually with their supporting bone, obtaining a very high degree of similarity between 3D-printed replicas and original elements [31]. Therefore, the creation of a low-cost environment for enabling design and fabrication of patient-specific 3D-models in dental facilities becomes an extremely interesting possibility [32].
Some applications have been already proposed, such as the development of tooth replicas for students training [30,33] and of individualized reamer drills for allogenic tooth transplantation [34].
A novel approach that could blend the educational and operative planning strategies is being developed: a Print and Try technique could be very useful in the daily dental practice of an Endodontist, consisting of a simulation method on a customized 3D-printed model that let clinicians try a specific clinical treatment before reproduce it on patient. Clinician can train on a 3D-printed tooth which replicates the same anatomical peculiarities of the real one and find the best approach to be more confident during the real treatment. A transparent material allows us to see through the root thickness during each step, and find the more conservative way not only to locate the root canal orifice but also to choose the best shaping, irrigation and filling technique, becoming at the same time an exact pre-view of the future situation into the oral cavity.
The purpose of this paper is to describe two cases: a dens invaginatus type3a (Section 2.1) and a molar with extremely curved and long canals (Section 2.2), where the Print and Try technique allowed a comfortable management of the clinical procedure.
2. Case Description
2.1. Case 1
History and physical examination: A 35-year-old healthy female, without any history of dental trauma, was referred to the endodontist for assessment of her upper right maxillary lateral incisor: she presented complaining of pain on the element 12, especially when chewing, lingering for several days.
An extraoral examination did not reveal abnormalities. An intraoral examination showed an aberrant coronal anatomy of element 12: the crown was wider mesially, with a slight irregularity of the incisal edge, hence a dens invaginatus was suspected (Figure 1a); no caries or restoration were detected.
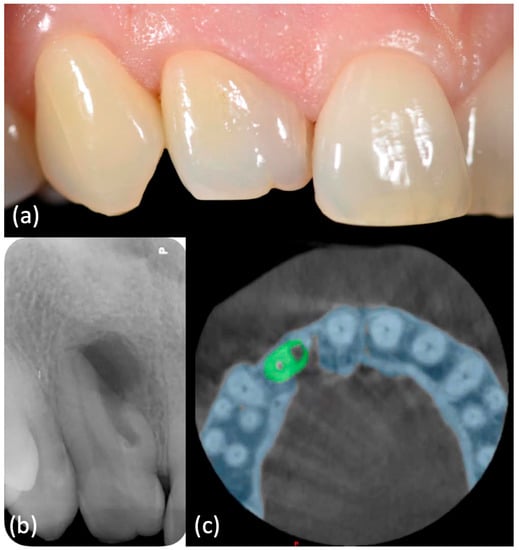
Figure 1.
(a) Intraoral examination showed a wide crown of element 1.2, typical anatomy of a dens invaginatus. (b) Periapical X-ray showed a mesial invagination separated from the main distal canal (dens invaginatus type3a), with an apical radiolucent area. (c) CBCT confirmed these findings.
The tooth was negative to cold and heat sensitivity testing, percussion and palpation tests were both positives, whereas the adjacent teeth responded normally. Electric pulp testing confirmed pulpal necrosis. There was no swelling in the apical mucosa area. Probing values, in absence of bleeding and suppuration, revealed a healthy periodontal status.
Imaging examination and diagnosis: A long cone periapical (LCPA) X-ray (Figure 1b) was taken (X-minD™ Unity, ACTEON® IMAGING, Merignac, France). Dens invaginatus type3a anatomy [35] was confirmed and chronic apical periodontitis was diagnosed, with a radiolucent area on the mesial aspect of the root, laterally to the main canal, where the invagination was communicating with the periodontal ligament through a pseudo-foramen; a large periapical radiolucency surrounded the periapex.
A small-FOV CBCT (Orthophos XG 3D, Dentsply Sirona, Charlotte, VA, USA) (Figure 1c–Movie 1) was taken as a supporting examination. The axial slices confirmed that the main root canal, developing from a small distal chamber, was separated from the invagination at all levels; furthermore, it showed that the invagination was limited to the root, not involving the clinical crown of the tooth, the periapical lesion was present both at the main and the pseudo-foramina and that it had perforated both the buccal and the palatal cortical plate.
Print and Try technique and treatment planning: The CBCT file was transformed in an STL one. On the STL file the bone structure was previewed with and without the tooth (Figure 2a–d–Movie 2) and tooth dimensions, including the invagination size, were measured (Figure 2e–g).
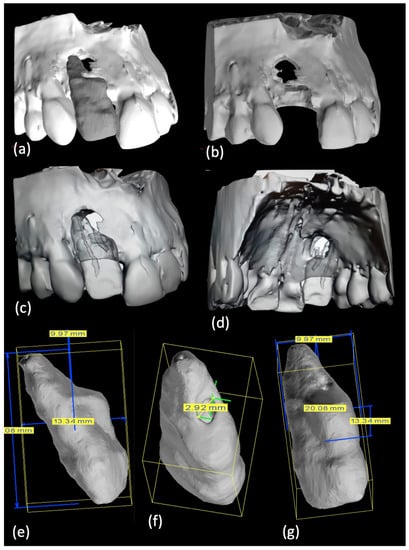
Figure 2.
(a–d) An STL of bone structure with and without element 1.2 was produced and (e–g) dimensions of element 1.2 were achieved.
Afterwards alveolar bone with and without the tooth was printed using the 3DSlicer software and a Formlabs printer (Figure 3a,b); a specific tooth model was obtained through a Meshmixer software and a Stratasys printer (Figure 3c).
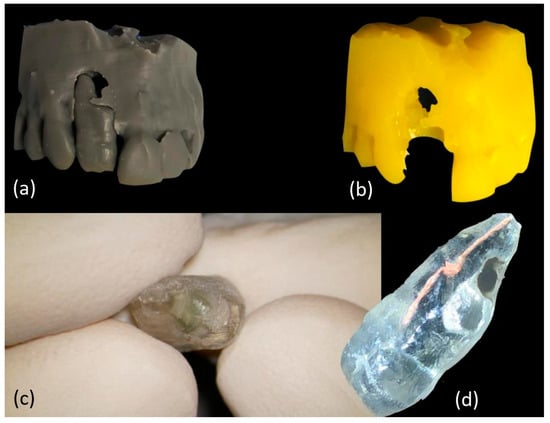
Figure 3.
(a,b) Customized bone and (c) tooth 3D-models were printed. (d) Main root canal therapy and invagination retrograde filling were performed on 3D-tooth model.
A clear material was chosen for the single tooth model (VeroClear, Stratasys, Eden Prairie, MI, USA), thus enabling visualization of both the root canal system and the instruments used at the different negotiation stages. Working on the 3D-printed models it was possible to determine the best treatment option which would have comprise of a primary orthograde endodontic treatment for the main canal, immediately followed by a surgical approach to achieve an adequate sealing of the invagination (Figure 3d). On the transparent tooth model, an occlusal distal conservative access cavity was centered on the main canal and then flexible rotary instruments were tried in to negotiate the canal lumen. A flexible irrigation plastic needle was confirmed to reach within 1 to 2 mm from the working length, even in the presence of a significant curvature between the middle and last third of the canal; also, the obturation stage was rehearsed and it was confirmed that a 3D-filling with warm gutta-percha was achievable. Finally, a complete infill of the invagination was practiced in a mock surgery with a putty bioceramic material. All these steps are reported in Movie 3.
Treatment procedure: The actual endodontic treatment of the main canal was performed under local anestesia, articaine hydrochloride with 1:100.000 articaine (Septodont, Saint-Maur-des-Fossés, France) and rubber dam (VISION rubber dam, ASA DENTAL, Bozzano, Italy) isolation. The access cavity was opened mimicking the preliminary conservative design on the 3D-model. Operative microscope (Leica, Hamburg, Germany) and small-sized diamond burs (Komet, Lemgo, Germany) were used at this stage.
The shaping was performed following the ProtaperGoldTM sequence (Dentsply Maillefer, Charlotte, VA, USA), to size F1 20/.08, to minimize root canal transportation (Figure 4a). The working length was 19 mm confirmed by an electronic apex locator (Dentsply Sirona, Charlotte, VA, USA). Irrigation was performed through a flexible plastic 30-gauge needle (IrriFlex®, Produits Dentaires, Vevey, Switzerland) using 5% sodium hypochlorite solution (Niclor 5, OGNA, Pavia, Italy), followed by 17% ethylenediaminetetraacetic acid (EDTA 17%, OGNA, Pavia, Italy) (Figure 4b). Passive ultrasonic irrigation was carried out using a cordless ultrasonic unit with a flexible tip (EndoUltraTM, MICRO-MEGA®, Besançon Cedex, France). Finally, the canal was filled with warm gutta-percha vertical technique using cordless units (Fast Pack and Fast Fill, Eighteeth, Shangai, China) (Figure 4c). The access cavity was restored with an adhesive composite restoration (Figure 4d). A final post-operative LCPA X-ray was taken (Figure 4e) (Movie 4). At the same appointment, a flap was opened (Figure 4f) and the granulomatous tissue extending above the invagination and the main canal foramen was surgically removed (Figure 4g,h).
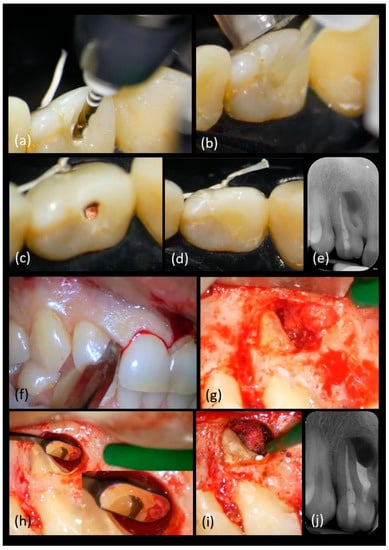
Figure 4.
Main clinical steps of case 1. Orthograde approach: (a) shaping with rotary files, (b) irrigation with a plastic needle, (c) gutta-percha filling, (d) conservative coronal restoration and (e) periapical X-ray. Surgical approach: (f) Surgical flap design, (g) granulomatous tissue removal, (h) resulting invagination access exposure which was prepared with ultrasonic tips and irrigated with a plastic needle, (i) 3D-invagination filling with a putty bioceramic sealer and (j) periapical X-ray after palatal and buccal membrane positioning.
The invagination was prepared with ultrasonic tips (KiS, Obtura Spartan Endodontics, Algonquin, IL, USA) and irrigated with a sterile saline solution (Sodium Chloride 0.9%, Fresenius Kabi, Bad Homburg, Germany) carried by a plastic needle. For the retrograde filling, a bioceramic sealer (EndoSequence BC RRM Fast Set Putty, Brasseler USA®, Savannah, GA, USA) was delivered with a syringe (Figure 4i). A microsurgical mirror (BLACK ULTRAmicro B6183, Hahnenkratt, Koginbach Stein, Germany) (Figure 4h) was used to confirm under microscope magnification the retro-preparation and plugging stages. Palatal and buccal absorbable collagen membranes (Ossix® Plus, Sweden&Martina, Padova, Italy) were positioned prior to flap reapproximation and closure with an absorbable 5-0 suture (Movie 5). A post-surgical LCPA X-ray was taken (Figure 4j).
One week later, no discomfort has been reported and primary tissue healing had been achieved, allowing sutures removal (Figure 5a). Clinical (Figure 5b) and radiographic follow-up (Figure 5c,d) showed a positive outcome, with soft tissue and bone healing progression.

Figure 5.
Tissue healing after (a) one week and (b) six months and (c) six-months and (d) twelve-months radiographic follow-up.
2.2. Case 2
History and physical examination: A 16-year-old otherwise healthy female was seen in emergency because of pain in her right maxillary region. An extraoral examination did not reveal swelling or other abnormalities. An intraoral examination showed immediately the presence of a lump on the buccal aspect of the tooth 26, which appeared not to be completely erupted and with a typical aspect of dilacerated root morphology on 2D radiographic imaging. A carious lesion was present on the same tooth and element 27 was not erupted (Figure 6a–Movie 6).
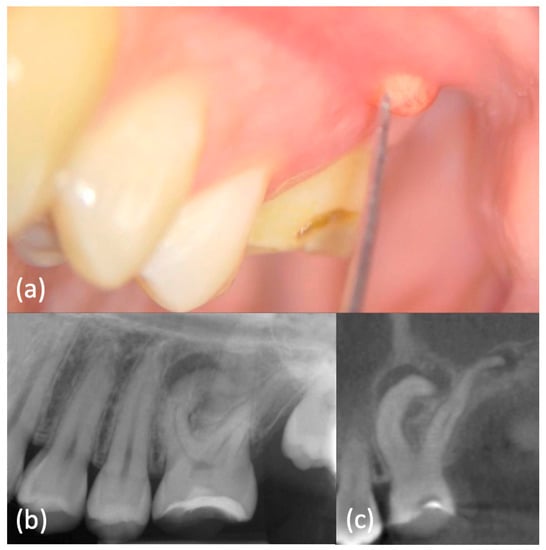
Figure 6.
(a) Intraoral examination showed a lump on buccal side of element 2.6, which appeared not to be completely erupted and with a carious lesion. Element 2.7 was clinically absent. (b) Periapical X-ray showed dilacerated roots of element 2.6, with a periapical lesion on the mesial-buccal one. Element 2.7 was not erupted, but present. (c) CBCT confirmed these findings and highlighted a periapical lesion also on the other roots.
Tooth 26 did not respond to sensitivity testing and it was tender to percussion and palpation, whereas the other elements responded normally. The electric pulp vitality test confirmed the pulpal necrosis of 26. Periodontal pocket values were between 1 mm up to 3 mm, without bleeding on probing.
Imaging examination and diagnosis: A pre-operative periapical image (Figure 6b) was carried out by long-cone paralleling technique (CS 2200, Carestream Dental, Rochester, NY, USA). It confirmed the presence of dilacerated mesio- and disto-buccal roots and the diagnosis of chronic periapical periodontitis. The tooth 27 was not erupted because of aberrant root morphology of the mesial element.
This radiography had an important role in the preliminary assessment of the irregular morphology of the root canal system, but it provided only a 2D-representation of the complex anatomy. Therefore, a small-FOV CBCT (Figure 6c–Movie 7) was indicated based on the current ESE guidelines. It provided a 3D image of the dilacerated tooth and its surrounding tissues and helped to determine the exact position and angulation of the dilaceration abnormality, which was found to also affect the palatal root. Apical radiolucencies were detected within the woven bone surrounding the apices of all roots. These diagnostic findings could be obtained only with CBCT imaging. An orthograde primary root canal treatment was recommended to the patient.
Print and Try technique and treatment planning: From the CBCT dicom file, an STL file was converted to generate a whole image of the teeth and supporting bone in three planes, thus allowing a better three-dimensional understanding of the structure involved (Figure 7a–l); subsequently a 3D plastic model was obtained with a Stratasys printer, using a clear material (Figure 7m) (Movie 8).
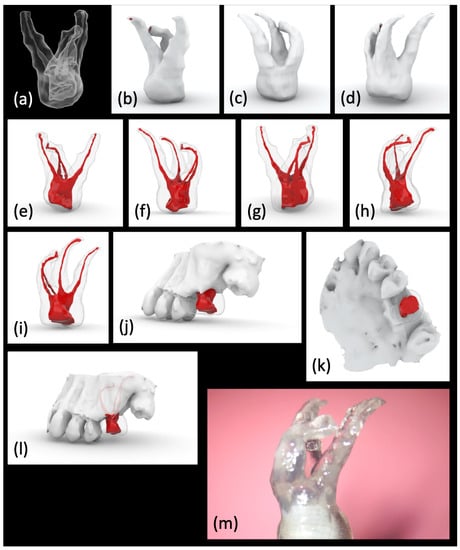
Figure 7.
(a–l) CBCT data were uploaded to an STL software and (m) a transparent plastic model was three-dimensionally printed.
The 3D model, inclusive of its hollow root canal system, was used to carry out a mock orthograde endodontic therapy, in particular the best access cavity was determined to localize the position of each orifice in anticipation of the actual treatment. The canals were negotiated with a preliminary rotary scout instrument: the clear roots allowed to understand where the instruments were likely to stop or create an inappropriate path. Rotary files with reduced taper were then used and it was possible to reach the full working length and gauge the apical foramen. An irrigation plastic needle could reach within 1 to 2 mm from the working length. Finally, a single cone filling technique, combined with a bioceramic sealer, was tried in the model tooth.
Treatment procedure: Root canal treatment was performed under local anestesia, articaine hydrochloride with 1:100,000 articaine (Septodont, Saint-Maur-des-Fossés, France) and rubber dam (VISION rubber dam, ASA DENTAL, Bozzano, Italy) isolation. The access cavity was opened mimicking the preliminary design on 3D-model, under operative microscope. Ultrasonic tips were used to remove pulp calcifications and to finish the access cavity (Figure 8a).
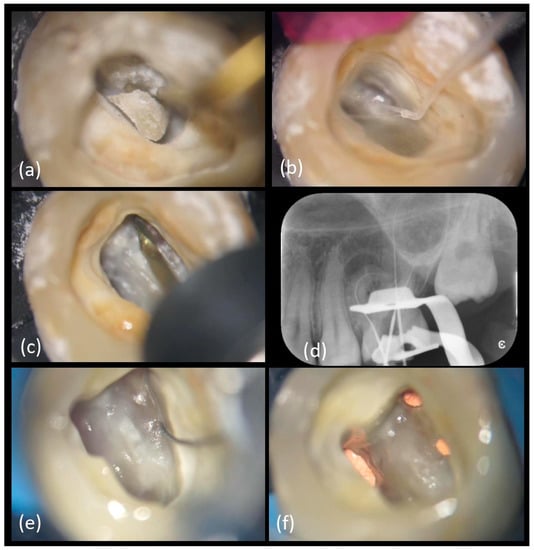
Figure 8.
Main clinical steps of case 2. (a) Access cavity with US tips, (b) chamber irrigation with IrriFlex®, (c) orifices enlargement with TruNatomy™ Orifice Modifier followed by the TruNatomyTM series, (d) working lengths X-ray control, (e) MB2 location and (f) filling with bioceramic sealer and single cone gutta-percha technique.
After the Micro-Opener 10.04 use andchamber irrigation, (Figure 8b) the orifices were enlarged with a TruNatomy™ Orifice Modifier 20.08 (TOM) (TruNatomy™, Dentsply Maillefer, Charlotte, VA, USA) (Figure 8c) (Movie 9). A temporary filling (Fuji IX, GC Italia, Milan, Italy) was placed following dressing with calcium hydroxide.
At the second appointment a viscous chelator (GLYDE File Prep Intro Package, Dentsply Sirona, Charlotte, VA, USA) was employed to facilitate the negotiations of the canals and the displacement of the dentinal shaving to minimize the risk of blockages.
The canal was progressively negotiated to full patency with a 10/.02 K-file. Working lengths were confirmed with an electronic apex locator (Root ZX mini, Morita, Tokyo, Japan) and a periapical X-ray (Figure 8d) as follows: MB1 was 27 mm long, MB2 merged with MB1 (Figure 8e), distal and palatal canals were respectively 30 and 28 mm long.
TruNatomy™ Glider 17/0.02 was used to obtain a rotary reproducible glide path with a mini-invasive approach, followed by TruNatomy™ Small 20/.04, as recommended for small canals. Afterwards, all the canals were prepared up to TruNatomy™ Prime 26/.04.
The irrigation protocol consisted of the following:10 mL of 5% sodium hypochlorite, used between each file of the TruNatomy™ series with sonic activation through a cordless unit with a flexible tip; 2 mL of 17% ethylenediaminetetraacetic acid (EDTA 17%, OGNA) for 60 min with sonic activation (EndoActivator®, Simit Dental, Maillefer, Charlotte, VA, USA) and a final rinse for 90 min with 5% sodium hypochlorite and 60 min of sonic activation (EndoActivator®, Simit Dental, Maillefer, Charlotte, VA, USA). Between each solution change and at the end of the irrigation protocol a sterile saline solution, Sodium Chloride 0.9%, was used.
Considering the anatomical complexity, the minimal preparation and the good result obtained with the mock obturation on the 3D-model, a single cone technique with TruNatomy™ Conform Fit™ Gutta-Percha Prime 26/.04 was chosen and combined with a bioceramic sealer (EndoSequence BC Sealer HiFlow, Brasseler USA®, Savannah, GA, USA) which is flowable and can fill any irregularities or voids (Figure 8f) (Movie 10). The coronal anatomy was restored with a build-up, followed by an indirect composite overlay. A post-operative LCPA X-ray was taken (Figure 9a). Clinical and radiographic follow-up was scheduled at 6 months: the patient confirmed that the tooth had been clinically asymptomatic and periapical X-ray showed a smaller radiolucent area around the mesial buccal root (Figure 9b); closure of the existing sinus tract was observed too. The next follow-up has been planned at one year.
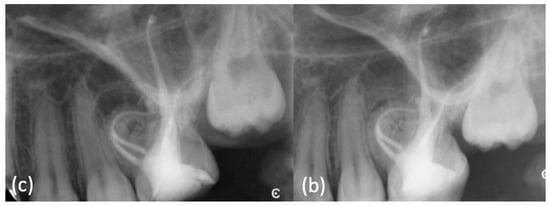
Figure 9.
(a) Post-operative X-ray was taken. (b) At 6 months review the periapical X-ray showed a smaller radiolucent area around the mesial buccal root.
3. Discussion
Shaping, cleaning, and filling are the basis of a successful endodontic therapy [1,2,3,4,5,6], and they must be performed to the current standards even when the root canal anatomy is extremely complicated. CBCT imaging is recommended by the ESE guidelines in cases of anatomical complexities because it improves diagnosis and treatment planning [23,24,27]. However, the choice of the best procedure and combination of materials could still be a challenge, and treatment outcome could be questionable in case anatomy is only partially dealt with. Fortunately, technology can support clinicians not only at the diagnostic but also at the planning stages: the Print and Try technique could represent a useful method to simulate the clinical treatment that will be carried out subsequently. Using CBCT scan images, it is possible to extrapolate files that can be transformed in STL models and then printed with a high-definition 3D-printer which deposes material in layers [30,31,36]. Clinicians can train on 3D-printed teeth and find the best approach in order to be more confident during the real treatment. This approach does not disrupt the current clinical approaches and steps as it does not require additional intra-operative lithographic stent or specific tools.
The first case in which the Print and Try technique was adopted was a symptomatic dens invaginatus type3a, with a suspected diagnosis hinted by the unusual crown morphology confirmed by both periapical X-ray and small FOV [35,37]. Different methods had been already proposed or already applied to remove necrotic tissue and bacteria in a tooth with a severe dens invaginatus type3a with periapical lesion [38]: the invagination which separately communicates with the periodontal ligament space could undergo an orthograde approach, usually managing the apical third with MTA or other hydraulic; if the periapical lesion does not heal, a secondary surgical management should follow if not planned at the outset. Alternatively, the invagination could be directly and completely filled with hydraulic cements through a contemporary or immediate surgical access. The main canal could be treated conventionally and completely sealed with gutta-percha. The last options are replantation and even extraction. The customized 3D-model of the specific tooth has been decisive in this case: through the transparent tooth the clinician realized that a solely orthograde approach for both the main canal and the invagination would have been unsuccessful because a direct access to the invagination was difficult and excessive removal of dental tissue would ensue, especially on the mesial aspect. Therefore, a contemporary nonsurgical/surgical treatment was planned: an orthograde approach for the main canal and an immediate surgical one for the invagination using a bioceramic putty material to allow an easier application with a larger volume of material due to its inherent flowability when dispensed from a syringe [39].
The second case was an upper left first molar affected by dilacerations, as the roots showed a sudden change in the axial inclination in both the X-ray and small-FOV CBCT [40,41]. Dilacerations treatment is known to be complicated and the failure to maintain the root canal curvature can result in iatrogenic errors including ledging, apical transportation and zipping, perforation and instrument separation [40]. Some clinical advices have been published: for instance, the access cavity should give a direct access to the apical foramen and a scout file may provide critical information and facilitate the preliminary canal negotiation [42]. In this specific clinical case, the endodontic steps were rehearsed; especially the shaping phase where the movement of each file into the system was tried to prevent any potential error during the actual treatment, which would have been extremely difficult or impossible to rectify. Mini-invasive files allowed a limited but complete and effective shaping of the root canal system [43,44].
In both cases the clinician felt more confident and less stressed during the clinical stages; the appointments were also more comfortable for the patient being shorter. On the other hand, the clinician spent time to learn to use 3D programs (which are free of charge) and to plan the specific cases. However, the successful outcome with lack of clinical symptoms and progressing radiographic periapical healing, even in the presence of complex anatomies, support the usage of the Pritn&Try approach.
A clear 3D-plastic tooth model including its root canal system represents an ideal training ground for both the expert clinician facing a complex endodontic case and an undergraduate student learning the basic stages of endodontic treatment. A Print and Try approach has a clinical and educational value as it allows to decide the best treatment plan and to practice each operative stage.
4. Conclusions
In complex endodontic anatomies, patient-specific 3D-models seem to facilitate treatment planning and, subsequently, they seem to make the actual therapy extremely precise, increasing the comfort for clinicians and patients and positively influencing the outcome. However, further studies dealing with a higher number of cases with long-term follow-up are needed to evaluate if a statistically significant difference could be found in the treatment outcomes using the Print and Try Technique.
Supplementary Materials
The following supplementary materials are available online:
Movie 1. CASE 1–The consecutive axial CBCT slices are compiled as a movie.
Movie 2. CASE 1–3D-STL file view is scrolled through.
Movie 3. CASE 1–The main steps of the treatment on 3D-tooth model are here reported: access cavity, shaping with rotary files, irrigation, root canal filling with warm gutta-percha of the main root canal and apical putty bioceramic location into the invagination.
Movie 4. CASE 1–The main steps of the main root canal treatment under operating microscope are here reported: access cavity, shaping with rotary files, irrigation with a plastic needle, ultrasonic activation, gutta-percha cone introduction with endodontic sealer, back-filling and conservative coronal restoration.
Movie 5. CASE 1–The main steps of the surgical invagination treatment under operating mi-croscope are here reported: surgical flap design, granulomatous tissue removal, preparation with ultrasonic tips, irrigation with a plastic needle, 3D-invagination filling with a putty bioceramic sealer and both palatal and buccal membrane positioning.
Movie 6. CASE 2–Intraoral examination showed a lump on buccal side of element 2.6.
Movie 7. CASE 2–The consecutive sagittal CBCT slices are compiled as a movie.
Movie 8. CASE 2–3D-STL file views and transparent tooth are scrolled through.
Movie 9. CASE 2–The main steps of the first appointment of root canal treatment under operating microscope are here reported: access cavity with US tips, orifices location through Micro-Opener 10/.04, chamber irrigation with IrriFlex® and orifices enlargement with TruNatomy™ Orifice Modifier.
Movie 10. CASE 2–The main steps of the second appointment of root canal treatment under op-erating microscope are here reported: use of a viscous chelator, working lengths measurement, shaping with TruNatomy™ Glider 17/.02, TruNatomy™ Small 20/.04 and TruNatomy™ Prime 26/.04 and filling with bioceramic sealer and single cone gutta-percha technique.
Author Contributions
Conceptualization, R.T. and M.G.; methodology, R.T. and M.G.; software, R.T. and M.G.; clinical case, R.T. and M.G.; writing—original draft preparation, G.B. and F.F.; writing—review and editing, G.B. and M.S.; visualization, G.B. and M.S.; supervision, E.X., A.A.-A., G.G., L.T., L.P. and A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Peters, O.A. Current challenges and concepts in the preparation of root canal systems: A review. J. Endod. 2004, 30, 559–567. [Google Scholar] [CrossRef]
- Schäfer, E.; Bürklein, S. Impact of nickel-titanium instrumentation of the root canal on clinical outcomes: A focused review. Odontology 2012, 100, 130–136. [Google Scholar] [CrossRef]
- Tomson, P.L.; Simon, S.R. Contemporary Cleaning and Shaping of the Root Canal System. Prim. Dent. J. 2016, 5, 46–53. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr. Strategies to treat infected root canals. J. Calif. Dent. Assoc. 2001, 29, 825–837. [Google Scholar]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Veríssimo, D.M.; do Vale, M.S. Methodologies for assessment of apical and coronal leakage of endodontic filling materials: A critical review. J. Oral. Sci. 2006, 48, 93–98. [Google Scholar] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1: Periapical health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 2: Tooth survival. Int. Endod. J. 2011, 44, 610–625. [Google Scholar] [CrossRef] [PubMed]
- Vertucci, F.J. Root canal anatomy of the human permanent teeth. Oral. Surg. Oral. Med. Oral. Pathol. 1984, 58, 589–599. [Google Scholar] [CrossRef]
- Weine, F.S.; Healey, H.J.; Gerstein, H.; Evanson, L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral. Surg. Oral. Med. Oral. Pathol. 1969, 28, 419–425. [Google Scholar] [CrossRef]
- Park, J.W.; Lee, J.K.; Ha, B.H.; Choi, J.H.; Perinpanayagam, H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using micro-computed tomography. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2009, 108, 437–442. [Google Scholar] [CrossRef]
- Kim, Y.; Chang, S.W.; Lee, J.K.; Chen, I.P.; Kaufman, B.; Jiang, J.; Cha, B.Y.; Zhu, Q.; Safavi, K.E.; Kum, K.Y. A micro-computed tomography study of canal configuration of multiple-canalled mesiobuccal root of maxillary first molar. Clin. Oral. Investig. 2013, 17, 1541–1546. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.N.R.; Marques, D.; Francisco, H.; Caramês, J. Gender influence on the number of roots and root canal system configuration in human permanent teeth of a Portuguese subpopulation. Quintessence Int. 2018, 49, 103–111. [Google Scholar]
- Martins, J.N.R.; Ordinola-Zapata, R.; Marques, D.; Francisco, H.; Caramês, J. Differences in root canal system configuration in human permanent teeth within different age groups. Int. Endod. J. 2018, 51, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.N.R.; Marques, D.; Silva, E.; Caramês, J.; Versiani, M.A. Prevalence Studies on Root Canal Anatomy Using Cone-beam Computed Tomographic Imaging: A Systematic Review. J. Endod. 2019, 45, 372–386. [Google Scholar] [CrossRef]
- Valenti-Obino, F.; Di Nardo, D.; Quero, L.; Miccoli, G.; Gambarini, G.; Testarelli, L.; Galli, M. Symmetry of root and root canal morphology of mandibular incisors: A cone-beam computed tomography study in vivo. J. Clin. Exp. Dent. 2019, 11, e527–e533. [Google Scholar] [CrossRef]
- Mashyakhy, M.; Gambarini, G. Root and Root Canal Morphology Differences Between Genders: A Comprehensive in-vivo CBCT Study in a Saudi Population. Acta Stomatol. Croat. 2019, 53, 213–246. [Google Scholar] [CrossRef]
- Ratanajirasut, R.; Panichuttra, A.; Panmekiate, S. A Cone-beam Computed Tomographic Study of Root and Canal Morphology of Maxillary First and Second Permanent Molars in a Thai Population. J. Endod. 2018, 44, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.C.; Cheng, W.C.; Chung, M.P.; Su, C.C.; Weng, P.W.; Cathy Tsai, Y.W.; Chiang, H.S.; Yeh, H.W.; Chung, C.H.; Shieh, Y.S.; et al. Complicated Root Canal Morphology of Mandibular Lateral Incisors Is Associated with the Presence of Distolingual Root in Mandibular First Molars: A Cone-beam Computed Tomographic Study in a Taiwanese Population. J. Endod. 2018, 44, 73–79. [Google Scholar] [CrossRef]
- Alfawaz, H.; Alqedairi, A.; Alkhayyal, A.K.; Almobarak, A.A.; Alhusain, M.F.; Martins, J.N.R. Prevalence of C-shaped canal system in mandibular first and second molars in a Saudi population assessed via cone beam computed tomography: A retrospective study. Clin. Oral. Investig. 2019, 23, 107–112. [Google Scholar] [CrossRef]
- Gambarini, G.; Piasecki, L.; Ropini, P.; Miccoli, G.; Di Nardo, D.; Testarelli, L. Cone-beam computed tomographic analysis on root and canal morphology of mandibular first permanent molar among multiracial population in Western European population. Eur. J. Dent. 2018, 12, 434–438. [Google Scholar] [CrossRef][Green Version]
- Patel, S.; Brown, J.; Pimentel, T.; Kelly, R.D.; Abella, F.; Durack, C. Cone beam computed tomography in Endodontics—a review of the literature. Int. Endod. J. 2019, 52, 1138–1152. [Google Scholar] [CrossRef]
- European Society of Endodontology; Patel, S.; Durack, C.; Abella, F.; Roig, M.; Shemesh, H.; Lambrechts, P.; Lemberg, K. European Society of Endodontology position statement: The use of CBCT in endodontics. J. Endod. 2014, 47, 502–504. [Google Scholar] [CrossRef] [PubMed]
- Gambarini, G.; Galli, M.; Stefanelli, L.V.; Di Nardo, D.; Morese, A.; Seracchiani, M.; De Angelis, F.; Di Carlo, S.; Testarelli, L. Endodontic Microsurgery Using Dynamic Navigation System: A Case Report. J. Endod. 2019, 45, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- Gambarini, G.; Galli, M.; Morese, A.; Abduljabbar, F.; Seracchiani, M.; Stefanelli, L.V.; Giovarruscio, M.; Di Nardo, D.; Testarelli, L. Digital Design of Minimally Invasive Endodontic Access Cavity. Appl. Sci. 2020, 10, 3513. [Google Scholar] [CrossRef]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE) developed by. J. Endod. 2019, 52, 1675–1678. [Google Scholar] [CrossRef]
- Patel, S.; Patel, R.; Foschi, F.; Mannocci, F. The Impact of Different Diagnostic Imaging Modalities on the Evaluation of Root Canal Anatomy and Endodontic Residents’ Stress Levels: A Clinical Study. J. Endod. 2019, 45, 406–413. [Google Scholar] [CrossRef]
- Kim, G.B.; Lee, S.; Kim, H.; Yang, D.H.; Kim, Y.H.; Kyung, Y.S.; Kim, C.S.; Choi, S.H.; Kim, B.J.; Ha, H.; et al. Three-Dimensional Printing: Basic Principles and Applications in Medicine and Radiology. Korean J. Radiol. 2016, 17, 182–197. [Google Scholar] [CrossRef]
- Reymus, M.; Fotiadou, C.; Kessler, A.; Heck, K.; Hickel, R.; Diegritz, C. 3D printed replicas for endodontic education. Int. Endod. J. 2019, 52, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Sokolowski, A.A.; Sokolowski, A.A.; Kammerhofer, J.; Madreiter-Sokolowski, C.T.; Payer, M.; Koller, M.; Jakse, N.; Wegscheider, W.A. Accuracy assessment of 3D-printed tooth replicas. Int. J. Comput. Dent. 2019, 22, 321–329. [Google Scholar] [CrossRef]
- Kamio, T.; Hayashi, K.; Onda, T.; Takaki, T.; Shibahara, T.; Yakushiji, T.; Shibui, T.; Kato, H. Utilizing a low-cost desktop 3D printer to develop a “one-stop 3D printing lab” for oral and maxillofacial surgery and dentistry fields. 3D Print. Med. 2018, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hanafi, A.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Perception of a modular 3D print model in undergraduate endodontic education. Int. Endod. J. 2020, 53, 1007–1016. [Google Scholar] [CrossRef]
- Xu, H.D.; Miron, R.J.; Zhang, X.X.; Zhang, Y.F. Allogenic tooth transplantation using 3D printing: A case report and review of the literature. World J. Clin. Cases 2019, 7, 2587–2596. [Google Scholar] [CrossRef]
- Oehlers, F.A. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral. Surg. Oral. Med. Oral. Pathol. 1957, 10, 1204–1218. [Google Scholar] [CrossRef]
- Ventola, C.L. Medical Applications for 3D Printing: Current and Projected Uses. Pharm. Ther. 2014, 39, 704–711. [Google Scholar]
- Gallacher, A.; Ali, R.; Bhakta, S. Dens invaginatus: Diagnosis and management strategies. Br. Dent. J. 2016, 221, 383–387. [Google Scholar] [CrossRef]
- Zhu, J.; Wang, X.; Fang, Y.; Von den Hoff, J.W.; Meng, L. An update on the diagnosis and treatment of dens invaginatus. Aust. Dent. J. 2017, 62, 261–275. [Google Scholar] [CrossRef]
- Shokouhinejad, N.; Nekoofar, M.H.; Ashoftehyazdi, K.; Zahraee, S.; Khoshkhounejad, M. Marginal adaptation of new bioceramic materials and mineral trioxide aggregate: A scanning electron microscopy study. Iran. Endod. J. 2014, 9, 144–148. [Google Scholar]
- Malcić, A.; Jukić, S.; Brzović, V.; Miletić, I.; Pelivan, I.; Anić, I. Prevalence of root dilaceration in adult dental patients in Croatia. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2006, 102, 104–109. [Google Scholar] [CrossRef]
- Nabavizadeh, M.; Sedigh Shamsi, M.; Moazami, F.; Abbaszadegan, A. Prevalence of root dilaceration in adult patients referred to shiraz dental school (2005–2010). J. Dent. 2013, 14, 160–164. [Google Scholar]
- Jafarzadeh, H.; Abbott, P.V. Dilaceration: Review of an endodontic challenge. J. Endod. 2007, 33, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Elnaghy, A.M.; Elsaka, S.E.; Mandorah, A.O. In vitro comparison of cyclic fatigue resistance of TruNatomy in single and double curvature canals compared with different nickel-titanium rotary instruments. BMC Oral. Health 2020, 20, 38. [Google Scholar] [CrossRef] [PubMed]
- Riyahi, A.M.; Bashiri, A.; Alshahrani, K.; Alshahrani, S.; Alamri, H.M.; Al-Sudani, D. Cyclic Fatigue Comparison of TruNatomy, Twisted File, and ProTaper Next Rotary Systems. Int. J. Dent. 2020, 2020, 3190938. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).