
A Novel Digital Technique to Quantify the Area and Volume of Enamel Removal after Interproximal Enamel Reduction


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedure
2.3. Alignment Procedure
2.4. Measurement Procedure
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jarjoura, K.; Gagnon, G.; Nieberg, L. Caries risk after interproximal enamel reduction. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Aasen, T.O.; Espeland, L. An approach to maintain orthodontic alignment of lower incisors without the use of retainers. Eur. J. Orthod. 2005, 27, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Lapenaite, E.; Lopatiene, K. Interproximal enamel reduction as a part of orthodontic treatment. Stomatologija 2014, 16, 19–24. [Google Scholar] [PubMed]
- Kaaouara, Y.; Mohind HBen Azaroual, M.F.; Zaoui, F.; Bahije, L.; Benyahia, H. In vivo enamel stripping: A macroscopic and microscopic analytical study. Int. Orthod. 2019, 17, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, P.E.; Tortorella, A. Enamel reduction procedures in orthodontic treatment. J. Can. Dent. Assoc. 2003, 69, 378–383. [Google Scholar] [PubMed]
- Chudasama, D.; Sheridan, J.J. Guidelines for contemporary air-rotor stripping. J. Clin. Orthod. 2007, 41, 315–320. [Google Scholar]
- Zachrisson, B.U. Interdental papilla reconstruction in adult orthodontics. World J. Orthod. 2004, 5, 67–73. [Google Scholar] [PubMed]
- Zachrisson, B.U.; Minster, L.; Øgaard, B.; Birkhed, D. Dental health assessed after interproximal enamel reduction: Caries risk in posterior teeth. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 90–98. [Google Scholar] [CrossRef]
- Arman, A.; Cehreli, S.B.; Ozel, E.; Arhun, N.; Cetinsahin, A.; Soyman, M. Qualitative and quantitative evaluation of enamel after various stripping methods. Am. J. Orthod. Dentofac. Orthop. 2006, 130, e7–e14. [Google Scholar] [CrossRef]
- Keim, R.G.; Gottlieb, E.L.; Nelson, A.H.; Vogels, D.S., 3rd. 2008 JCO study of orthodontic diagnosis and treatment procedures, part 1: Results and trends. J. Clin. Orthod. 2008, 42, 625–640. [Google Scholar]
- Zachrisson, B.U.; Nyøygaard, L.; Mobarak, K. Dental health assessed more than 10 years after interproximal enamel reduction of mandibular anterior teeth. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Grippaudo, C.; Cancellieri, D.; Grecolini, M.E.; Deli, R. Comparison between different interdental stripping methods and evaluation of abrasive strips: SEM analysis. Prog. Orthod. 2010, 11, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, S.; Iliadi, A.; Eliades, T.; Eliades, G. An in vitro study on the effect of an oscillating stripping method on enamel roughness. Prog. Orthod. 2015, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Guarneri, M.P.; D’Amico, P.; Molinari, C.; Meddis, V.; Carlucci, A.; Siciliani, G. Orthofile(R): A new approach for mechanical interproximal reduction: A scanning electron micro- scopic enamel evaluation. J. Orofac. Orthop. 2014, 75, 203–212. [Google Scholar] [CrossRef]
- Danesh, G.; Podstawa, P.K.K.; Schwartz, C.E.; Kirschneck, C.; Bizhang, M.; Arnold, W.H. Depth of acid penetration and enamel surface roughness associated with different methods of interproximal enamel reduction. PLoS ONE 2020, 15, e0229595. [Google Scholar] [CrossRef]
- Johner, A.M.; Pandis, N.; Dudic, A.; Kiliaridis, S. Quantitative comparison of 3 enamel-stripping devices in vitro: How precisely can we strip teeth? Am. J. Orthod. Dentofac. Orthop. 2013, 143, 468–472. [Google Scholar] [CrossRef]
- De Felipe, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog. Orthod. 2020, 21, 1–7. [Google Scholar] [CrossRef]
- Abduo, J.; Elseyoufi, M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar]
- Lee, K.C.; Park, S.-J. Digital Intraoral Scanners and Alginate Impressions in Reproducing Full Dental Arches: A Comparative 3D Assessment. Appl. Sci. 2020, 10, 7637. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Gandini, P.; Malfatto, M.; Di Corato, F.; Trovati, F.; Scribante, A. Computerized Casts for Orthodontic Purpose Using Powder-Free Intraoral Scanners: Accuracy, Execution Time, and Patient Feedback. Biomed. Res. Int. 2018, 23, 4103232. [Google Scholar] [CrossRef]
- Lecocq, G. Digital impression-taking: Fundamentals and benefits in orthodontics. Int. Orthod. 2016, 14, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Duvert, R.; Gebeile-Chauty, S. La précision des empreintes numériques intra-orales en orthodontie est-elle suffisante? Orthod. Fr. 2017, 88, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef] [PubMed]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, A.I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef]
- Sugsompian, K.; Tansalarak, R.; Piyapattamin, T. Comparison of the Enamel Surface Roughness from Different Polishing Methods: Scanning Electron Microscopy and Atomic Force Microscopy Investigation. Eur. J. Dent. 2020, 14, 299–305. [Google Scholar] [CrossRef]
- Mhatre, A.C.; Tandur, A.P.; Reddy, S.S.; Karunakara, B.C.; Baswaraj, H. Enamel Surface Evaluation after Removal of Orthodontic Composite Remnants by Intraoral Sandblasting Technique and Carbide Bur Technique: A Three-Dimensional Surface Profilometry and Scanning Electron Microscopic Study. J. Int. Oral Health 2015, 7, 34–39. [Google Scholar]
- Ahrari, F.; Akbari, M.; Akbari, J.; Dabiri, G. Enamel surface roughness after debonding of orthodontic brackets and various clean-up techniques. J. Dent. 2013, 10, 82–93. [Google Scholar]
- Kubínek, R.; Zapletalová, Z.; Vůjtek, M.; Novotný, R.; Kolářová, H.; Chmelíčková, H.; Peřina, J., Jr. Sealing of open dentinal tubules by laser irradiation: AFM and SEM observations of dentine surfaces. J. Mol. Recognit. 2007, 20, 476–482. [Google Scholar] [CrossRef]
- García Vargas, M.C.; Montoya Toro, F.A.; Salamanca Mojica, I.P.; Figueroa Valbuena, E.; Castro Figueroa, M.E.; Delgado Perdomo, L.P.; Quintero, L.C. Efectos sobre el esmalte dental con la utilización de tres diferentes métodos de reducción interproximal. Rev. Nac. Odontol. 2011, 7, 9–17. [Google Scholar]
- Kilinc, D.D.; Hamamci, O. Enamel surfaces with sem after the application of different in vivo stripping methods. J. Int. Dent. Med. Res. 2009, 2, 71–76. [Google Scholar]
- Meredith, L.; Farella, M.; Lowrey, S.; Cannon, R.D.; Mei, L. Atomic force microscopy analysis of enamel nanotopography after interproximal reduction. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Zubizarreta-Macho, Á.; Triduo, M.; Alonso Pérez-Barquero, J.; Guinot Barona, C.; Albaladejo Martínez, A. Novel Digital Technique to Quantify the Area and Volume of Cement Remaining and Enamel Removed after Fixed Multibracket Appliance Therapy Debonding: An In Vitro Study. J. Clin. Med. 2020, 9, 1098. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef]
- Sason, G.K.; Mistry, G.; Tabassum, R.; Shetty, O. A comparative evaluation of intraoral and extraoral digital impressions: An in vivo study. J. Indian Prosthodont. Soc. 2018, 18, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.; Att, W.; Metzger, M.; Nelson, K. Precision of Dental Implant Digitization Using Intraoral Scanners. Int. J. Prosthodont. 2016, 29, 277–283. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Full arch scans: Conventional versus digital impressions--an in-vitro study. Int. J. Comput. Dent. 2011, 14, 11–21. [Google Scholar]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef]
- Kuhr, F.; Schmidt, A.; Rehmann, P.; Wöstmann, B. A new method for assessing the accuracy of full arch impressions in patients. J. Dent. 2016, 55, 68–74. [Google Scholar] [CrossRef]
- Guth, J.; Runkel, C.; Beuer, F.; Stimmelmayr, M.; Edelhoff, D.; Keul, C. Accuracy of five intraoral scanners compared to indirect digitalization. Clin. Oral Investig. 2017, 21, 1445–1455. [Google Scholar] [CrossRef]
- Nedelcu, R.G.; Persson, A.S. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. Prosthet. Dent. 2014, 112, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Akyalcin, S.; Cozad, B.; English, J.; Colville, C.; Laman, S. Diagnostic accuracy of impression-free digital models. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Kulczyk, T.; Rychlik, M.; Lorkiewicz-Muszyńska, D.; Abreu-Głowacka, M.; Czajka-Jakubowska, A.; Przystańska, A. Computed tomography versus optical scanning: A comparison of different methods of 3d data acquisition for tooth replication. Biomed. Res. Int. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
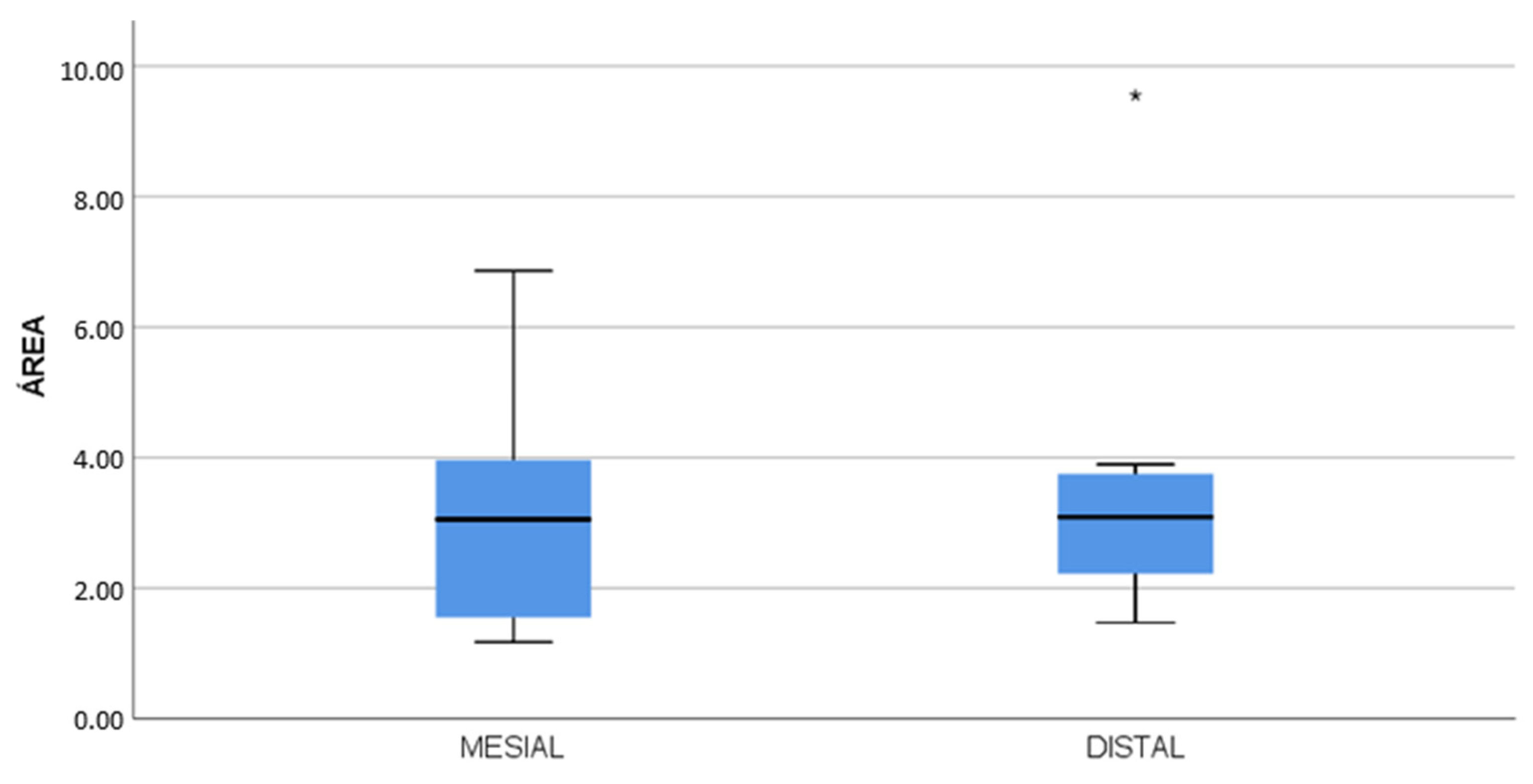
| Surface | n | Mean | Median | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Mesial | 14 | 2.97 | 3.05 | 1.78 | 1.17 | 6.86 |
| Distal | 12 | 3.53 | 3.08 | 2.25 | 1.47 | 9.55 |
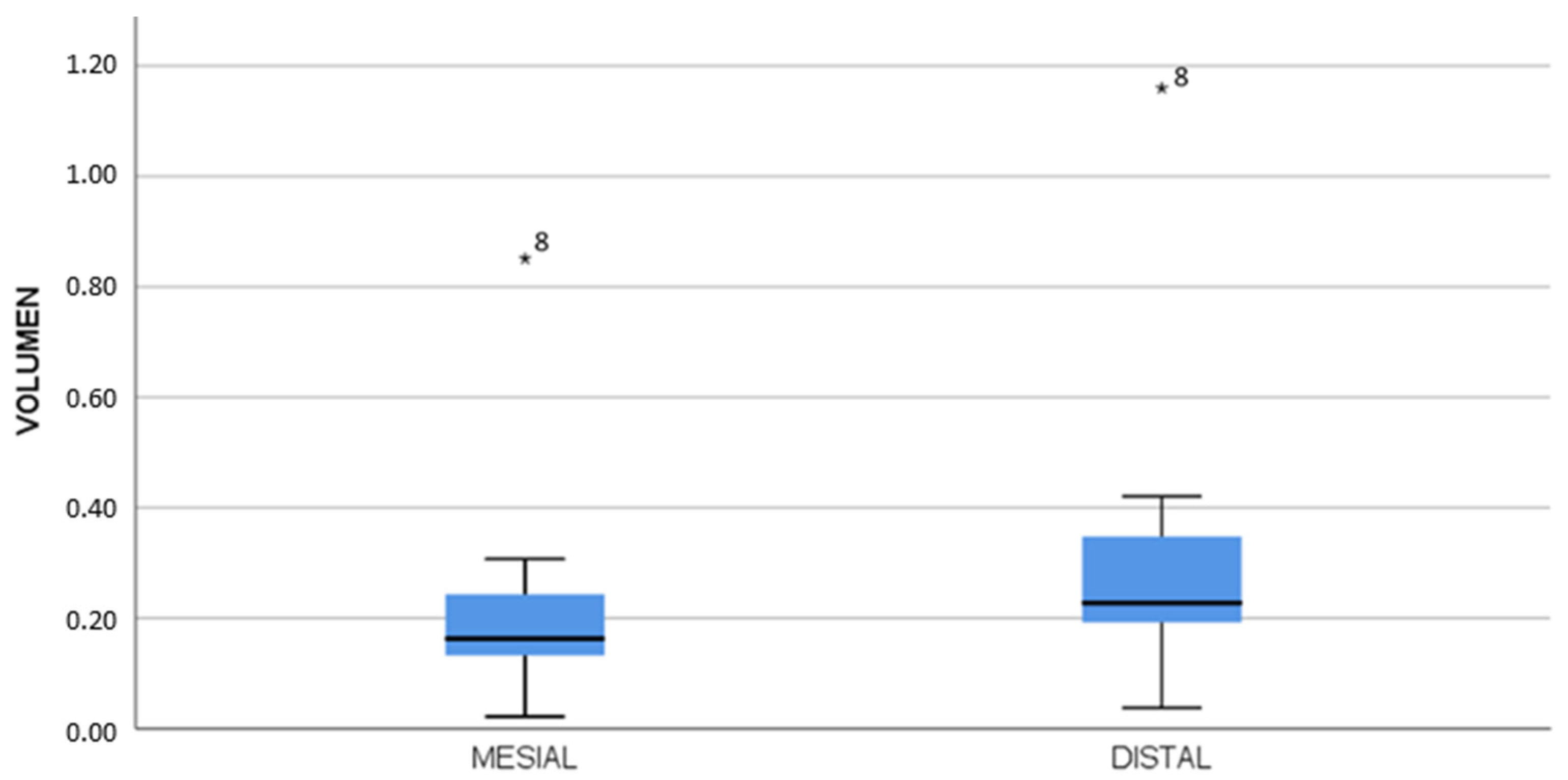
| Surface | n | Mean | Median | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Mesial | 14 | 0.22 | 0.16 | 0.22 | 0.02 | 0.85 |
| Distal | 12 | 0.32 | 0.22 | 0.31 | 0.04 | 1.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triduo, M.; Zubizarreta-Macho, Á.; Pérez-Barquero, J.A.; Guinot Barona, C.; Alvarado Lorenzo, A.; Vicente-Galindo, P.; Albaladejo Martínez, A. A Novel Digital Technique to Quantify the Area and Volume of Enamel Removal after Interproximal Enamel Reduction. Appl. Sci. 2021, 11, 1274. https://doi.org/10.3390/app11031274
Triduo M, Zubizarreta-Macho Á, Pérez-Barquero JA, Guinot Barona C, Alvarado Lorenzo A, Vicente-Galindo P, Albaladejo Martínez A. A Novel Digital Technique to Quantify the Area and Volume of Enamel Removal after Interproximal Enamel Reduction. Applied Sciences. 2021; 11(3):1274. https://doi.org/10.3390/app11031274
Chicago/Turabian StyleTriduo, Martina, Álvaro Zubizarreta-Macho, Jorge Alonso Pérez-Barquero, Clara Guinot Barona, Alfonso Alvarado Lorenzo, Purificación Vicente-Galindo, and Alberto Albaladejo Martínez. 2021. "A Novel Digital Technique to Quantify the Area and Volume of Enamel Removal after Interproximal Enamel Reduction" Applied Sciences 11, no. 3: 1274. https://doi.org/10.3390/app11031274
APA StyleTriduo, M., Zubizarreta-Macho, Á., Pérez-Barquero, J. A., Guinot Barona, C., Alvarado Lorenzo, A., Vicente-Galindo, P., & Albaladejo Martínez, A. (2021). A Novel Digital Technique to Quantify the Area and Volume of Enamel Removal after Interproximal Enamel Reduction. Applied Sciences, 11(3), 1274. https://doi.org/10.3390/app11031274